Hyperreflective Material in Optical Coherence Tomography Images of Eyes with Myopic Choroidal Neovascularization May Affect the Visual Outcome


 ,
,  and
and 
Abstract
1. Introduction
2. Experimental Section
2.1. Subjects
2.2. Ocular Examinations
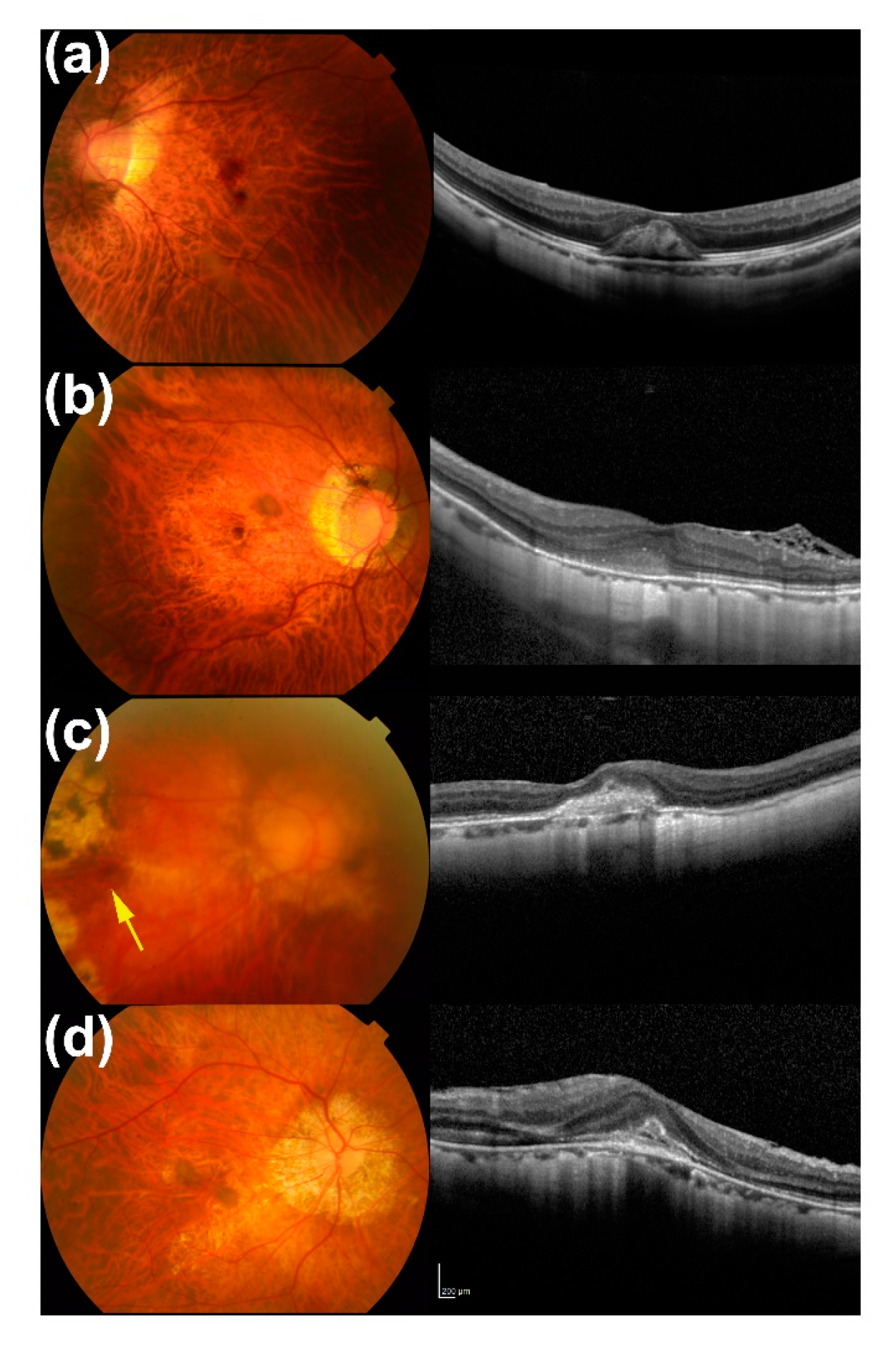
2.3. OCT
2.4. Intravitreal Injections
2.5. Statistical Analyses
3. Results
3.1. Participants’ Characteristics
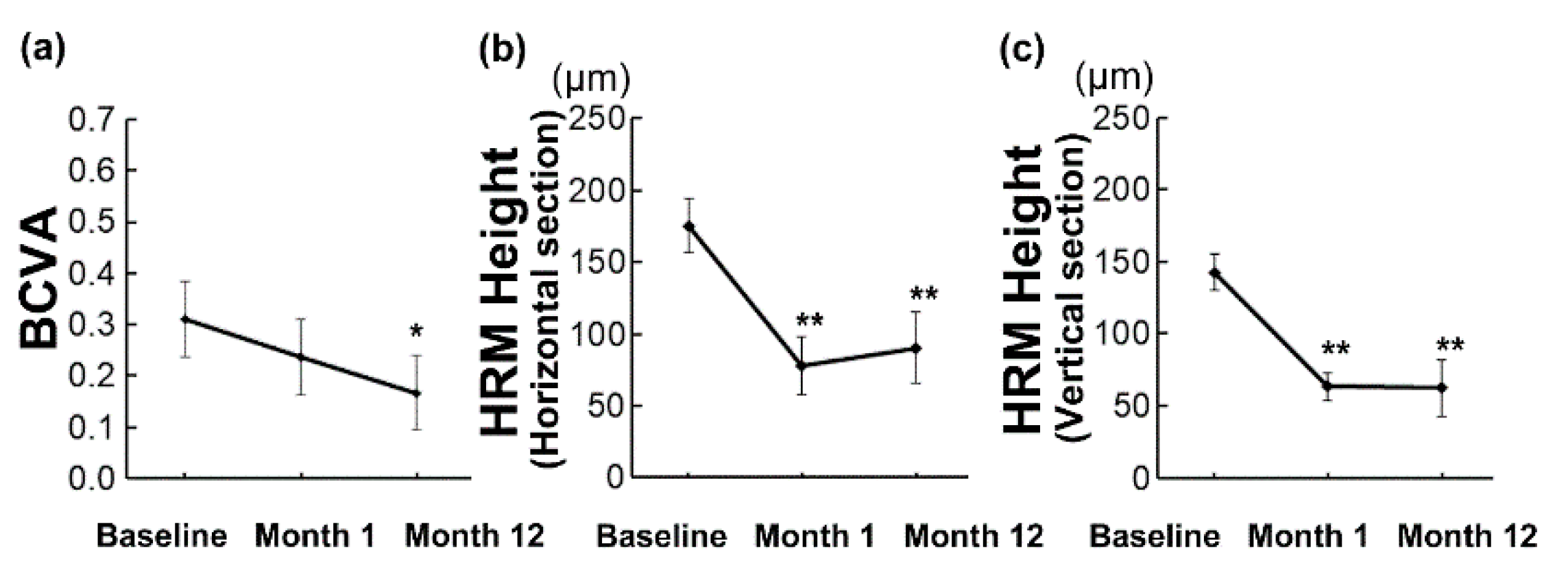
3.2. Overall Changes in BCVA and HRM Height during 12 Months
3.3. Characteristics of Initial HRM in Eyes with or without BCVA ≤ 0.10 at 12 Months After the Initial Treatment
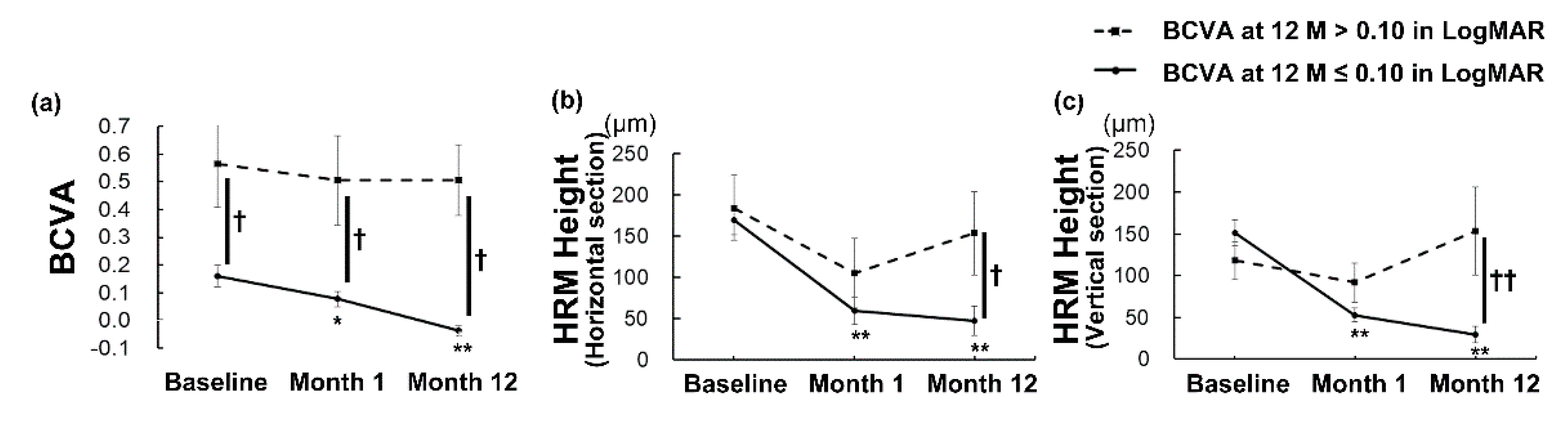
3.4. Differences in the Clinical Courses of Eyes with or without BCVA ≤ 0.10 at 12 Months After Initial Treatment
3.5. Impact of Initial BCVA and HRM in Predicting BCVA at 12 Months After the Initial Treatment
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ohno-Matsui, K.; Ikuno, Y.; Lai, T.Y.Y.; Gemmy Cheung, C.M. Diagnosis and treatment guideline for myopic choroidal neovascularization due to pathologic myopia. Prog. Retin. Eye Res. 2018, 63, 92–106. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.; Sperduto, R.D.; Ferris, F.L., 3rd. Increased prevalence of myopia in the United States between 1971–1972 and 1999–2004. Arch. Ophthalmol. 2009, 127, 1632–1639. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.M.; Bertelsen, G.; Cumberland, P.; Wolfram, C.; Verhoeven, V.J.; Anastasopoulos, E.; Buitendijk, G.H.; Cougnard-Gregoire, A.; Creuzot-Garcher, C.; Erke, M.G.; et al. Increasing Prevalence of Myopia in Europe and the Impact of Education. Ophthalmology 2015, 122, 1489–1497. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, K.; Ohno-Matsui, K.; Shimada, N.; Moriyama, M.; Kojima, A.; Hayashi, W.; Yasuzumi, K.; Nagaoka, N.; Saka, N.; Yoshida, T.; et al. Long-term pattern of progression of myopic maculopathy: A natural history study. Ophthalmology 2010, 117, 1595–1611. [Google Scholar] [CrossRef]
- Hsu, W.M.; Cheng, C.Y.; Liu, J.H.; Tsai, S.Y.; Chou, P. Prevalence and causes of visual impairment in an elderly Chinese population in Taiwan: The Shihpai Eye Study. Ophthalmology 2004, 111, 62–69. [Google Scholar] [CrossRef]
- Iwase, A.; Araie, M.; Tomidokoro, A.; Yamamoto, T.; Shimizu, H.; Kitazawa, Y.; Tajimi Study Group. Prevalence and causes of low vision and blindness in a Japanese adult population: The Tajimi study. Ophthalmology 2006, 113, 1354–1362. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Wang, Y.; Li, Y.; Wang, Y.; Cui, T.; Li, J.; Jonas, J.B. Causes of blindness and visual impairment in urban and rural areas in Beijing: The Beijing Eye study. Ophthalmology 2006, 113, 1134.e1–1134.e11. [Google Scholar] [CrossRef]
- Wolf, S.; Balciuniene, V.J.; Laganovska, G.; Menchini, U.; Ohno-Matsui, K.; Sharma, T.; Wong, T.Y.; Silva, R.; Pilz, S.; Gekkieva, M.; et al. RADIANCE: A randomized controlled study of ranibizumab in patients with choroidal neovascularization secondary to pathologic myopia. Ophthalmology 2014, 121, 682–692.e2. [Google Scholar] [CrossRef]
- Ikuno, Y.; Ohno-Matsui, K.; Wong, T.Y.; Korobelnik, J.F.; Vitti, R.; Li, T.; Stemper, B.; Asmus, F.; Zeitz, O.; Ishibashi, T.; et al. Intravitreal aflibercept injection in patients with myopic choroidal neovascularization: The MYRROR Study. Ophthalmology 2015, 122, 1220–1227. [Google Scholar] [CrossRef]
- Chen, Y.; Sharma, T.; Li, X.; Song, Y.; Chang, Q.; Lin, R.; Egger, A.; Foo, A.; Gekkieva, M.; Lai, T.Y.Y. Ranibizumab versus verteporfin photodynamic therapy in Asian patients with myopic choroidal neovascularization: BRILLIANCE, a 12-Month, Randomized, Double-Masked Study. Retina 2019, 39, 1985–1994. [Google Scholar] [CrossRef]
- Morgan, I.G.; French, A.N.; Ashby, R.S.; Guo, X.; Ding, X.; He, M.; Rose, K.A. The epidemics of myopia: Aetiology and prevention. Prog. Retin. Eye Res. 2018, 62, 134–149. [Google Scholar] [CrossRef]
- Cheung, C.M.G.; Arnold, J.J.; Holz, F.G.; Park, K.H.; Lai, T.Y.Y.; Larsen, M.; Mitchell, P.; Ohno-Matsui, K.; Chen, S.J.; Wolf, S.; et al. Myopic choroidal neovascularization: Review, guidance, and consensus statement on management. Ophthalmology 2017, 124, 1690–1711. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Xing, Y.Q.; Li, T.; Li, Y.; Song, X.S.; Li, J.Z. Meta-analysis of best corrected visual acuity after treatment for myopic choroidal neovascularisation. Int. J. Ophthalmol. 2014, 7, 720–725. [Google Scholar] [CrossRef] [PubMed]
- Moon, B.G.; Cho, A.R.; Lee, J.; Kim, Y.J.; Lee, J.Y.; Kim, J.G.; Yoon, Y.H. Improved visual outcome and low recurrence with early treatment with intravitreal anti-vascular endothelial growth factor in myopic choroidal neovascularization. Ophthalmologica 2017, 237, 128–138. [Google Scholar] [CrossRef]
- Suzuki, M.; Nagai, N.; Minami, S.; Kurihara, T.; Kamoshita, M.; Sonobe, H.; Watanabe, K.; Shinoda, H.; Tsubota, K.; Ozawa, Y. Predicting recurrences of macular edema due to branch retinal vein occlusion during anti-vascular endothelial growth factor therapy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Nagai, N.; Suzuki, M.; Uchida, A.; Kurihara, T.; Ban, N.; Minami, S.; Shinoda, H.; Tsubota, K.; Ozawa, Y. The area and number of intraretinal cystoid spaces predict the visual outcome after ranibizumab monotherapy in diabetic macular edema. J. Clin. Med. 2020, 9, 1391. [Google Scholar] [CrossRef]
- Suzuki, M.; Nagai, N.; Shinoda, H.; Uchida, A.; Kurihara, T.; Tomita, Y.; Kamoshita, M.; Iyama, C.; Tsubota, K.; Ozawa, Y. Distinct responsiveness to intravitreal ranibizumab therapy in polypoidal choroidal vasculopathy with single or multiple polyps. Am. J. Ophthalmol. 2016, 166, 52–59. [Google Scholar] [CrossRef]
- Tomita, Y.; Nagai, N.; Suzuki, M.; Shinoda, H.; Uchida, A.; Mochimaru, H.; Izumi-Nagai, K.; Sasaki, M.; Tsubota, K.; Ozawa, Y. Functional visual acuity in age-related macular degeneration. Optom. Vis. Sci 2016, 93, 70–76. [Google Scholar] [CrossRef]
- Nagai, N.; Suzuki, M.; Uchida, A.; Kurihara, T.; Kamoshita, M.; Minami, S.; Shinoda, H.; Tsubota, K.; Ozawa, Y. Non-responsiveness to intravitreal aflibercept treatment in neovascular age-related macular degeneration: Implications of serous pigment epithelial detachment. Sci. Rep. 2016, 6, 29619. [Google Scholar] [CrossRef]
- Ding, X.; Zhan, Z.; Sun, L.; Yang, Y.; Li, S.; Zhang, A.; Luo, X.; Lu, L. Retinal pigmental epithelium elevation and external limiting membrane interruption in myopic choroidal neovascularization: Correlation with activity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 1831–1837. [Google Scholar] [CrossRef]
- Battaglia Parodi, M.; Iacono, P.; Bandello, F. Correspondence of leakage on fluorescein angiography and optical coherence tomography parameters in diagnosis and monitoring of myopic choroidal neovascularization treated with bevacizumab. Retina 2016, 36, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Kang, H.G.; Lee, S.C.; Kim, M. Features of optical coherence tomography predictive of choroidal neovascularisation treatment response in pathological myopia in association with fluorescein angiography. Br. J. Ophthalmol. 2018, 102, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Kurihara, T.; Uchino, M.; Torii, H.; Kawashima, M.; Sasaki, M.; Ozawa, Y.; Yamagishi, K.; Iso, H.; Sawada, N.; et al. High myopia and its associated factors in JPHC-NEXT eye study: A cross-sectional observational study. J. Clin. Med. 2019, 8, 1788. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.C.; Chen, Y.P.; Tan, E.C.; Leteneux, C.; Chang, E.; Chu, C.H.; Lai, C.C. Epidemiology, treatment pattern and health care utilization of myopic choroidal neovascularization: A population based study. Jpn. J. Ophthalmol. 2017, 61, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.S.; Kim, J.G.; Kim, J.T.; Joe, S.G. Prognostic factors of eyes with naive subfoveal myopic choroidal neovascularization after intravitreal bevacizumab. Am. J. Ophthalmol. 2013, 156, 1201–1210.e2. [Google Scholar] [CrossRef] [PubMed]
- Casalino, G.; Bandello, F.; Chakravarthy, U. Changes in neovascular lesion hyperreflectivity after anti-vegf treatment in age-related macular degeneration: An integrated multimodal imaging analysis. Invest. Ophthalmol. Vis. Sci 2016, 57, OCT288–OCT298. [Google Scholar] [CrossRef] [PubMed]
- Iacono, P.; Battaglia Parodi, M.; Selvi, F.; Parravano, M.C.; Chiaravalloti, A.; Varano, M.; Bandello, F. Factors influencing visual acuity in patients receiving anti-vascular endothelial growth factor for myopic choroidal neovascularization. Retina 2017, 37, 1931–1941. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Age (years old) | 70.6 ± 2.1 (50 to 83) |
| Sex (female [%]) | 16 (66.7) |
| Baseline BCVA (LogMAR) | 0.31 ± 0.07 (−0.08 to 1.3) |
| Intraocular pressure (mmHg) | 13.5 ± 0.7 (7 to 20) |
| CNV location | |
| Subfoveal, (eyes [%]) | 17 [70.8] |
| Juxtafoveal, (eyes [%]) | 7 [29.2] |
| HRM height (μm) | |
| Horizontal section | 175.4 ± 18.8 (49 to 452) |
| Vertical section | 142.7 ± 12.7 (36 to 229) |
| HRM intensity | |
| Horizontal section | 65.6 ± 3.5 (35.1 to 105.4) |
| Vertical section | 66.1 ± 3.0 (48.2 to 90.9) |
| BCVA ≤ 0.10 in LogMAR | BCVA > 0.10 in LogMAR | p-Value | |
|---|---|---|---|
| Eyes (%) | 15 (62.5) | 9 (37.5) | - |
| Age | 68.9 ± 2.9 (53 to 86) | 73.4 ± 2.7 (55 to 80) | 0.299 |
| Sex (female) (eyes [%]) | 10 [66.7] | 6 [66.7] | 1.000 |
| Baseline BCVA | 0.16 ± 0.04 | 0.56 ± 0.15 | 0.015 * |
| Baseline HRM height (μm) | |||
| Horizontal section | 169.2 ± 17.6 (75 to 256) | 184.4 ± 39.0 (49 to 452) | 0.700 |
| Vertical section | 151.4 ± 15.1 (52 to 229) | 118.2 ± 22.4 (36 to 129) | 0.263 |
| Baseline HRM intensity | |||
| Horizontal section | 59.8 ± 4.0 (35.1 to 88.2) | 73.9 ± 5.4 (51.3 to 105.4) | 0.033 * |
| Vertical section | 63.0 ± 2.8 (48.2 to 88.2) | 75.0 ± 7.4 (54.1 to 90.8) | 0.075 |
| Injection Number | 2.00 ± 3.73 (1 to 7) | 2.27 ± 4.41 (1 to 4) | 0.861 |
| Variable | Adjusted R2 | Constant [95% CI] | Coefficient [95% CI] | p |
|---|---|---|---|---|
| Baseline BCVA (LogMAR) | 0.442 | −0.42 [−0.192, 0.108] | 0.673 [0.354, 0.991] | <0.001 ** |
| HRM intensity | ||||
| Horizontal section | 0.122 | −0.403 [−1.042, 0.236] | 0.009 [0.000, 0.018] | 0.062 |
| Vertical section | −0.047 | −0.061 [−1.032, 0.910] | 0.003 [−0.011, 0.017] | 0.673 |
| Unstandardized Coefficient | Standardized Coefficient | |||
|---|---|---|---|---|
| Model | B | Standard Error | Beta | p |
| (Constant) | −0.314 | 0.244 | 0.214 | |
| Baseline BCVA (logMAR) | 0.599 | 0.167 | 0.613 | 0.002 ** |
| HRM intensity, Horizontal section | 0.005 | 0.004 | 0.211 | 0.231 |
| Total adjusted R2 | 0.502 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mushiga, Y.; Minami, S.; Uchida, A.; Nagai, N.; Suzuki, M.; Kurihara, T.; Sonobe, H.; Ban, N.; Watanabe, K.; Shinoda, H.; et al. Hyperreflective Material in Optical Coherence Tomography Images of Eyes with Myopic Choroidal Neovascularization May Affect the Visual Outcome. J. Clin. Med. 2020, 9, 2394. https://doi.org/10.3390/jcm9082394
Mushiga Y, Minami S, Uchida A, Nagai N, Suzuki M, Kurihara T, Sonobe H, Ban N, Watanabe K, Shinoda H, et al. Hyperreflective Material in Optical Coherence Tomography Images of Eyes with Myopic Choroidal Neovascularization May Affect the Visual Outcome. Journal of Clinical Medicine. 2020; 9(8):2394. https://doi.org/10.3390/jcm9082394
Chicago/Turabian StyleMushiga, Yasuaki, Sakiko Minami, Atsuro Uchida, Norihiro Nagai, Misa Suzuki, Toshihide Kurihara, Hideki Sonobe, Norimitsu Ban, Kazuhiro Watanabe, Hajime Shinoda, and et al. 2020. "Hyperreflective Material in Optical Coherence Tomography Images of Eyes with Myopic Choroidal Neovascularization May Affect the Visual Outcome" Journal of Clinical Medicine 9, no. 8: 2394. https://doi.org/10.3390/jcm9082394
APA StyleMushiga, Y., Minami, S., Uchida, A., Nagai, N., Suzuki, M., Kurihara, T., Sonobe, H., Ban, N., Watanabe, K., Shinoda, H., Tsubota, K., & Ozawa, Y. (2020). Hyperreflective Material in Optical Coherence Tomography Images of Eyes with Myopic Choroidal Neovascularization May Affect the Visual Outcome. Journal of Clinical Medicine, 9(8), 2394. https://doi.org/10.3390/jcm9082394