Home Respiratory Polygraphy is Useful in the Diagnosis of Childhood Obstructive Sleep Apnea Syndrome

 ,
,
Abstract
1. Introduction
2. Experimental Section
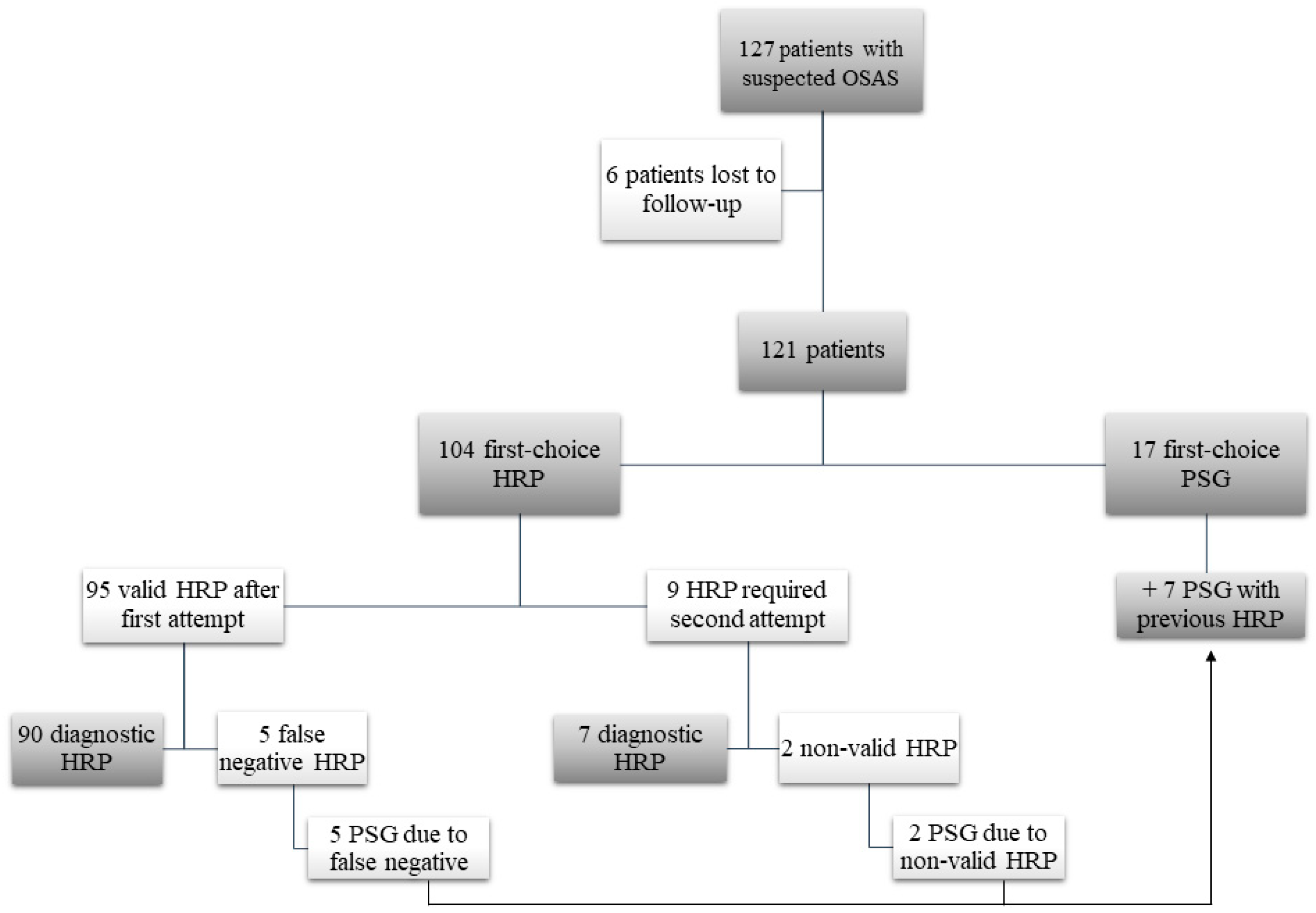
2.1. Study Design and Population
2.2. Clinical Protocol
2.3. Diagnostic Protocol
2.4. Patient Groups
2.5. Therapeutic Protocol
2.6. Sample Size Calculation
2.7. Statistical Analysis
2.8. Ethical Aspects
3. Results
3.1. Overal
3.2. Study Population
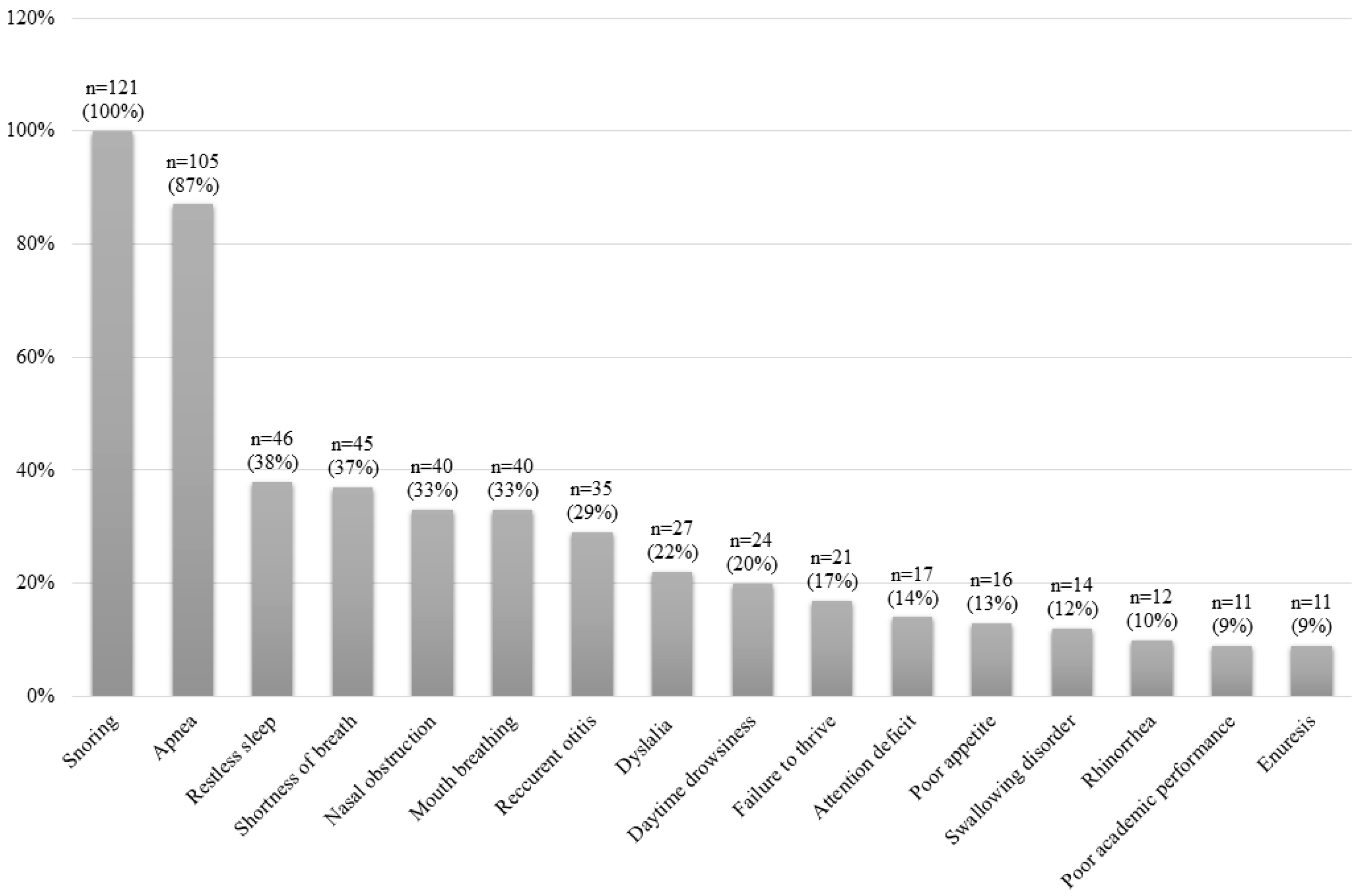
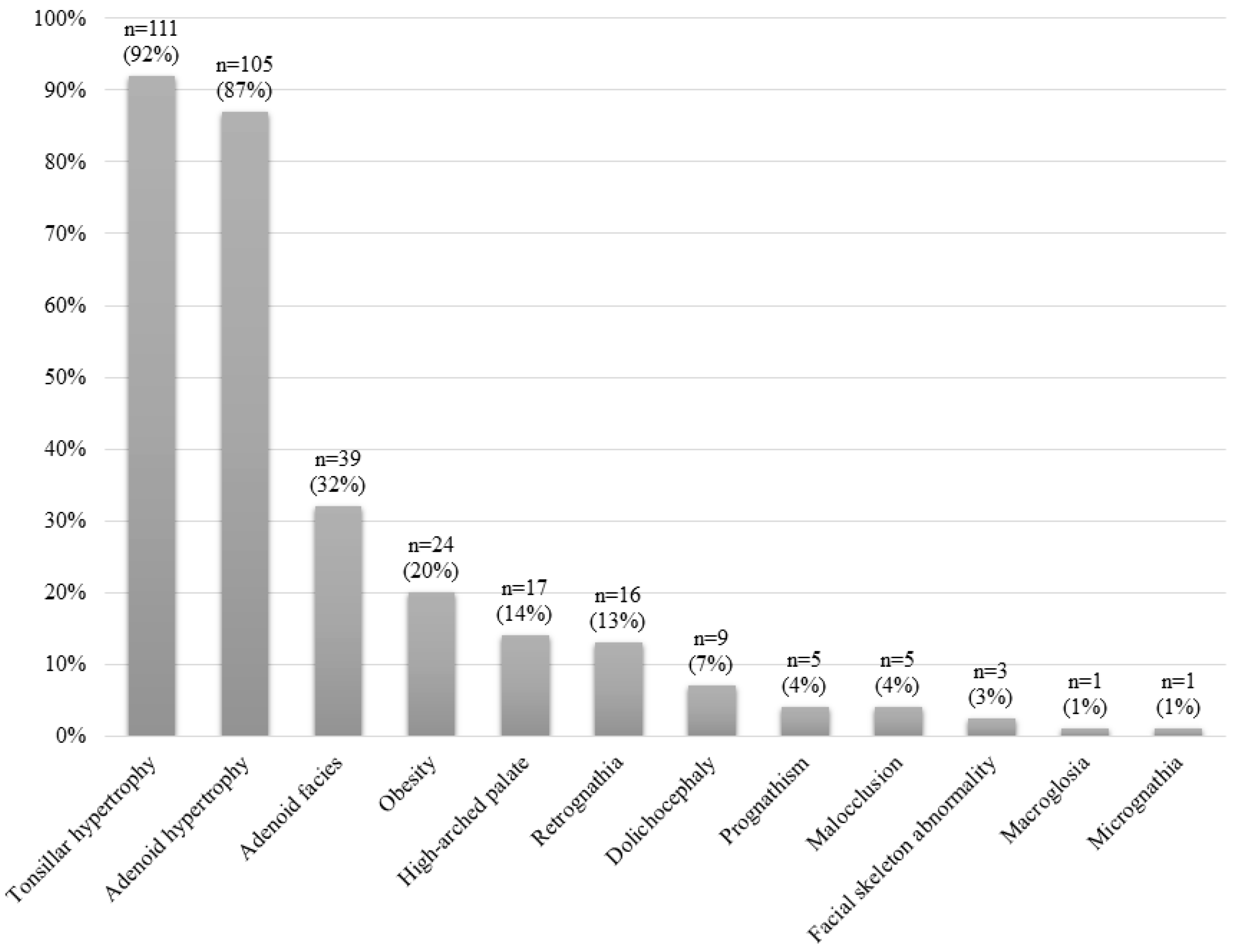
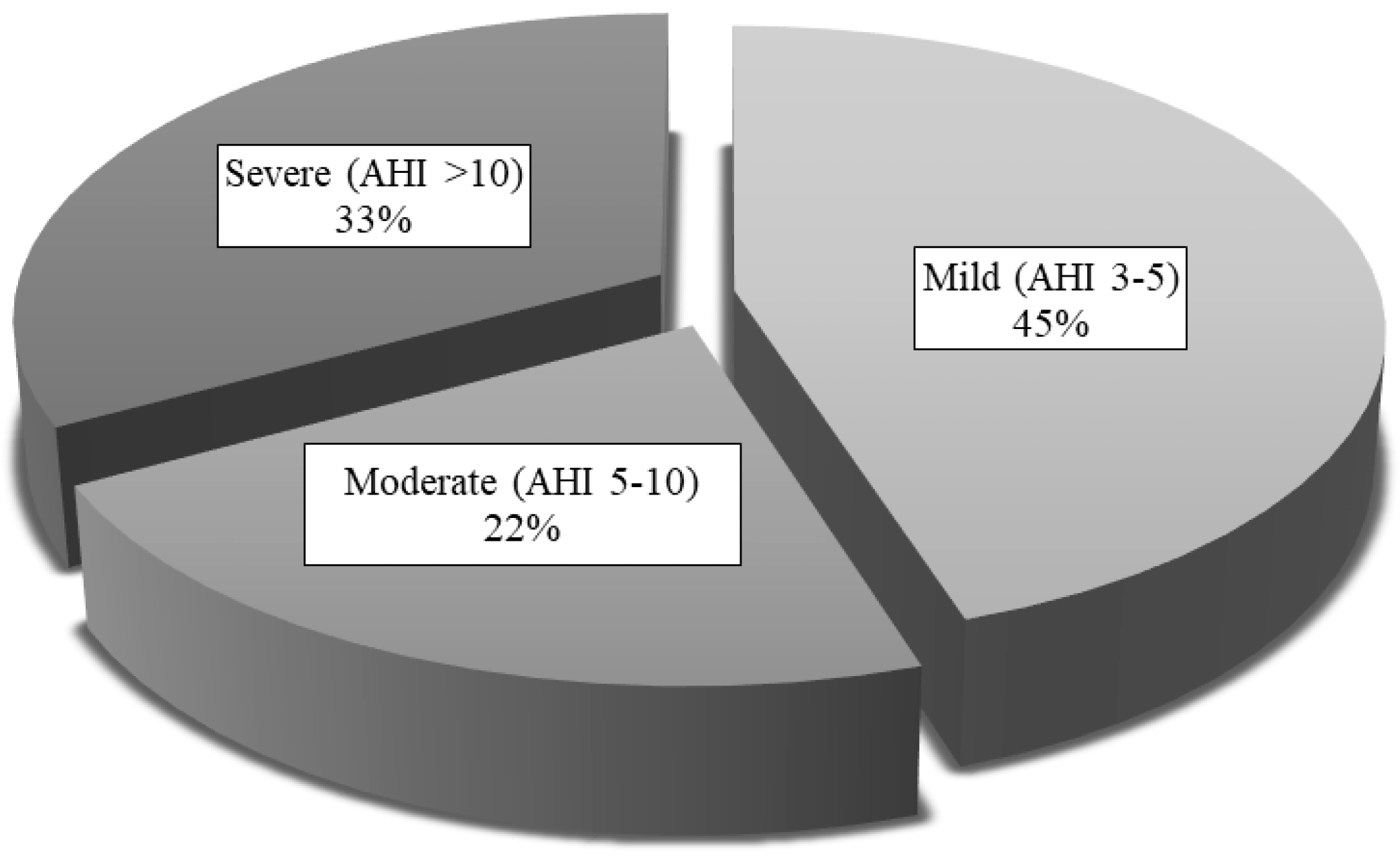
3.2.1. All Patients
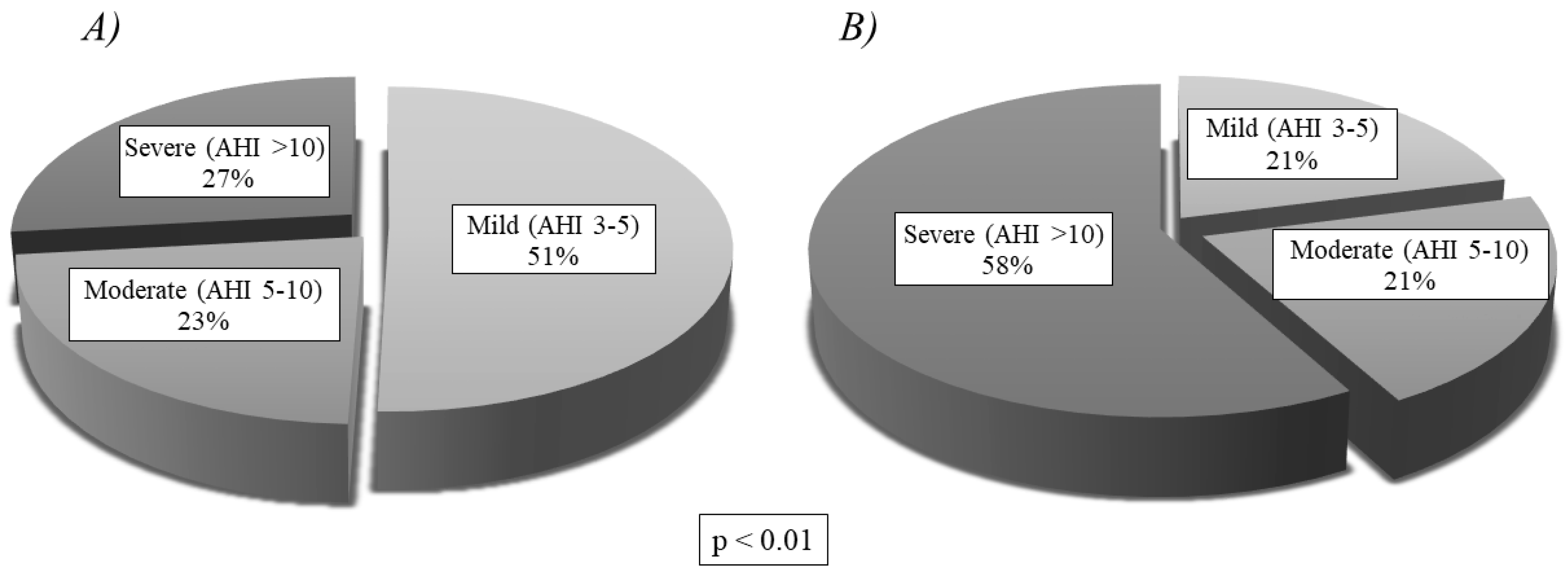
3.2.2. Comparison between Groups
3.3. Treatment
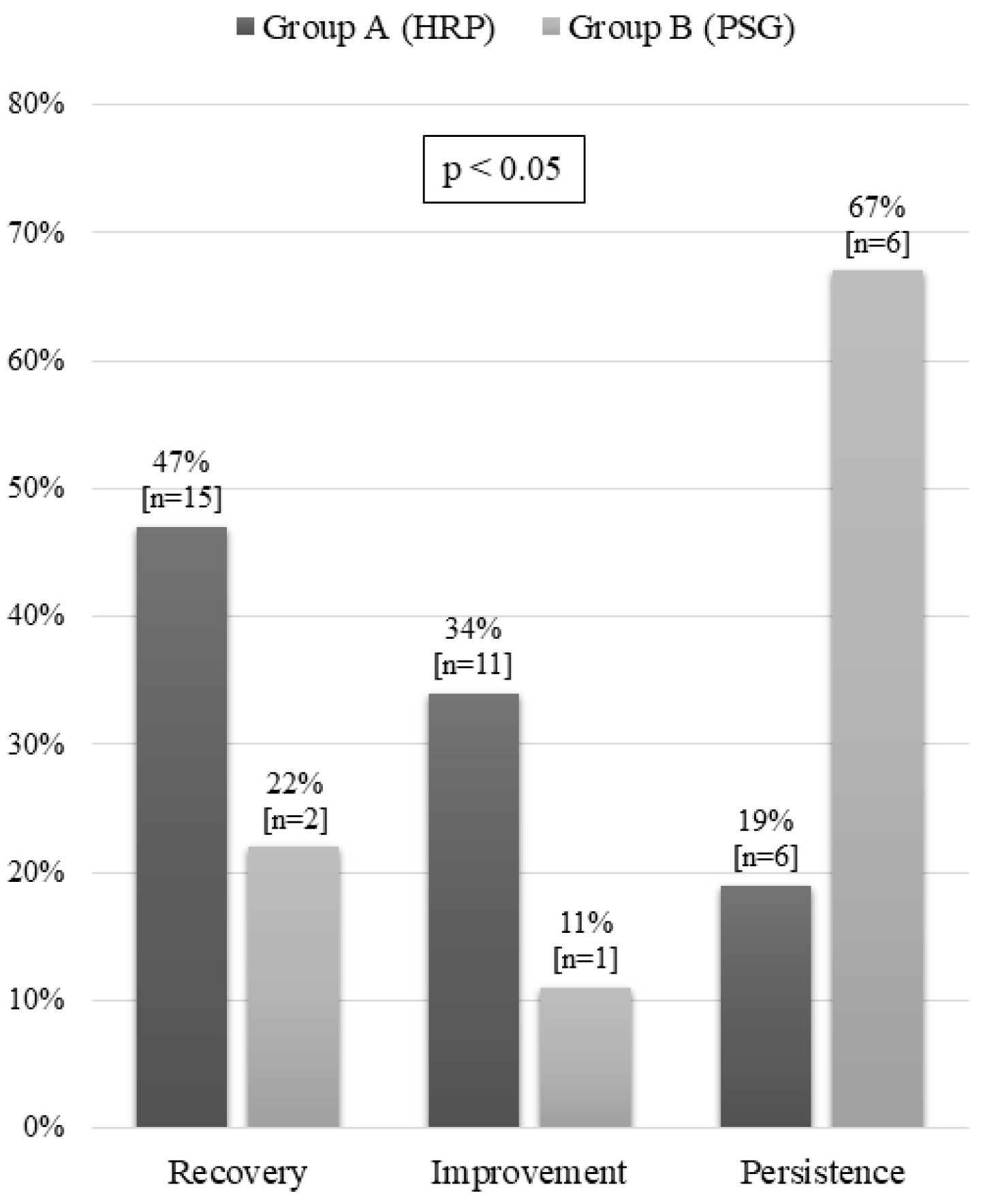
3.4. Progress
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Thoracic Society. Standards and indications for cardiopulmonary sleep studies in children. Am. J. Respir. Crit. Care Med. 1996, 153, 866–878. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Ward, S.D.; Sheldon, S.H.; Shiffman, R.N. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012, 130, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Pastrana, D.; Álvarez Gil, D. Síndrome de apneas-hipopneas durante el sueño. Protoc. Diagn. Ter. Pediatr. 2017, 1, 237–251. [Google Scholar]
- Gusmao, T.S.; Pompéia, S.; Miranda, M.C. Cognitive and behavioral effects of obstructive sleep apnea syndrome in children: A systematic literature review. Sleep Med. 2018, 46, 46–55. [Google Scholar]
- Trosman, I.; Trosman, S.J. Cognitive and behavioral consequences of sleep disordered breathing in children. Med. Sci. 2017, 5, E30. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Álvarez, M.L.; Canet, T.; Cubell-Alarco, M.; Estivill, E.; Fernández-Julian, E.; Gozal, D.; Jurado-Luque, M.J.; Lluch-Roselló, M.A.; Martínez-Pérez, F.; Merino-Andreu, M.; et al. Consensus document on sleep apnea-hypopnea syndrome in children (full version). Sociedad Española de Sueño. El Área de Sueño de la Sociedad Española de Neumología y Cirugía Torácica (SEPAR). Arch. Bronconeumol. 2011, 47, 2–18. [Google Scholar]
- Bixler, E.O.; Vgontzas, A.N.; Lin, H.M.; Liao, D.; Calhoun, S.; Vela-Bueno, A.; Fedok, F.; Vlasic, V.; Graff, G. Sleep disordered breathing in children in a general population sample: Prevalence and risk factors. Sleep 2009, 32, 731–736. [Google Scholar] [CrossRef]
- Huang, Y.S.; Guillerminault, C. Pediatric obstructive sleep apnea: Where do we stand? Adv. Otorhinolaryngol. 2017, 80, 136–144. [Google Scholar]
- Verhulst, S.L.; Franckx, H.; Van Gaal, L.; De Backer, W.; Desager, K. The effect of weight loss on sleep-disordered breathing in obese teenagers. Obesity 2009, 17, 1178–1183. [Google Scholar]
- O’Brien, L.M.; Sitha, S.; Baur, L.A.; Waters, K.A. Obesity increases the risk for persisting obstructive sleep apnea after treatment in children. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 1555–1560. [Google Scholar] [CrossRef]
- Andersen, I.G.; Holm, J.C.; Homoe, P. Obstructive sleep apnea in obese children and adolescents, treatment methods and outcome of treatment—A systematic review. Int. J. Pediatr. Otorhinolaryngol. 2016, 87, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Al Ali, A.; Richmond, S.; Popat, H.; Playle, R.; Pickles, T.; Zhurov, A.I.; Marshall, D.; Rosin, P.L.; Henderson, J.; Bonuck, K. The influence of snoring, mouth breathing and apnoea on facial morphology in late childhood: A three-dimensinal study. BMJ Open 2015, 5, e009027. [Google Scholar] [CrossRef] [PubMed]
- Kaditis, A.G.; Alonso-Álvarez, M.L.; Boudewyns, A.; Alexopoulos, E.I.; Ersu, R.; Joostes, K.; Larramona, H.; Miano, S.; Narang, I.; Trang, H.; et al. Obstructive sleep disordered breathing in 2- to 18-year-old children: Diagnosis and management. Eur. Respir. J. 2016, 47, 69–94. [Google Scholar] [CrossRef] [PubMed]
- Reckley, L.K.; Fernandez-Salvador, C.; Camacho, M. The effect of tonsillectomy on obstructive sleep apnea: An overview of systematic reviews. Nat. Sci. Sleep 2018, 10, 105–110. [Google Scholar] [CrossRef]
- Marcus, C.L.; Moore, R.H.; Rosen, C.L.; Giordani, B.; Garetz, S.L.; Taylor, H.G.; Mitchell, R.B.; Amin, R.; Katz, E.S.; Arens, R.; et al. A randomized trial of adenotonsillectomy for childhood sleep apnea. N. Engl. J. Med. 2013, 368, 2366–2376. [Google Scholar] [CrossRef]
- De Miguel-Díez, J.; Villa-Asensi, J.R.; Álvarez-Sala, J.L. Prevalence of sleep-disordered breathing in children with down syndrome: Polygraphic findings in 108 children. Sleep 2003, 26, 1006–1009. [Google Scholar] [CrossRef]
- Chiner, E. Approach to the cost of polysomnography In a Spanish hospital. Internet J. Pulm. Med. 2001, 2, 1–5. [Google Scholar]
- Lumeng, J.C.; Chervin, R.D. Epidemiology of pediatric obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 242–252. [Google Scholar] [CrossRef]
- Collop, N.A.; Anderson, W.M.; Boehlecke, B.; Claman, D.; Goldberg, R.; Gottlieb, D.J.; Hudgel, D.; Sateia, M.; Schwab, R. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. Portable monitoring task force of the American academy of sleep medicine. J. Clin. Sleep Med. 2007, 3, 737–747. [Google Scholar]
- Alonso-Álvarez, M.L.; Terán-Santos, J.; Ordax-Carbajo, E.; Cordero-Guevara, J.A.; Navazo-Egüia, A.I.; Kheirandish-Gozal, L.; Gozal, D. Reliability of home respiratory polygraphy for the diagnosis of sleep apnea in children. Chest 2015, 147, 1020–1028. [Google Scholar] [CrossRef] [PubMed]
- Sardón Prado, O.; González Pérez-Yarza, E.; Aldasoro Ruiz, A.; Estévez Domingo, M.; Mintegui Aranburua, J.; Korta Murua, J.; Emparanza Knörrb, J.L. Rentabilidad de la poligrafía respiratoria del sueño realizada en el domicilio. Anales de Pediatría 2006, 65, 310–315. [Google Scholar]
- WHO. Growth Reference 5–19 years. Available online: http://www.who.int/growthref/en/ (accessed on 10 March 2020).
- Masa, J.F.; Corral, J.; Pereira, R.; Duran-Cantolla, J.; Cabello, M.; Hernández-Blasco, L.; Monasterio, C.; Alonso, A.; Chiner, E.; Rubio, M.; et al. Effectiveness of home respiratory polygraphy for the diagnosis of sleep apnoea and hypopnoea syndrome. Thorax 2011, 66, 567–573. [Google Scholar] [CrossRef]
- Rechtschaffen, A.; Kales, A. A Manual of Standardized Terminology, Techniques and Scoring System of Sleep Stages in Human Subjects, 1st ed.; Brain Information Service/Brain Research Institute, University of California: Los Angeles, CA, USA, 1968. [Google Scholar]
- Moser, D.; Anderer, P.; Gruber, G.; Parapatics, S.; Loretz, E.; Boeck, M.; Kloesch, G.; Heller, E.; Schmidt, A.; Danker-Hopfe, H.; et al. Sleep classification according to AASM and rechtschaffen & kales: Effects on sleep scoring parameters. Sleep 2009, 32, 139–149. [Google Scholar] [PubMed]
- Nieminen, P.; Tolonen, U.; Lopponen, H. Snoring and obstructive sleep apnea in children. Arch. Otolaryngol. Head Neck Surg. 2000, 126, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.L.; McColley, S.A.; Marcus, C.L.; Curtis, S.; Loughlin, G.M. Inability of clinical history to distinguish primary snoring from obstructive sleep apnea syndrome in children. Chest 1995, 108, 610–618. [Google Scholar] [CrossRef]
- Masa, J.F.; Corral, J.; Pereira, R.; Duran-Cantolla, J.; Cabello, M.; Hernández-Blasco, L.; Monasterio, C.; Alonso-Fernandez, A.; Chiner, E.; Vázquez-Polo, F.J.; et al. Effectiveness of sequential automatic-manual home respiratory polygraphy scoring. Eur. Respir. J. 2013, 41, 879–887. [Google Scholar] [CrossRef]
- Lloberes, P.; Durán-Cantolla, J.; Martínez-García, M.A.; Marín, J.M.; Ferrer, A.; Corral, J.; Masa, J.F.; Parra, O.; Alonso-Álvarez, M.L.; Terán-Santos, J. Diagnóstico y tratamiento del síndrome de apneas-hipopneas del sueño. Normativa SEPAR. Arch. Bronconeumol. 2011, 47, 143–156. [Google Scholar]
- Tan, H.L.; Gozal, D.; Ramírez, H.M.; Bandla, H.P.; Kheirandish-Gozal, L. Overnight polysomnography versus respiratory polygraphy in the diagnosis of pediatric obstructive sleep apnea. Sleep 2014, 37, 255–260. [Google Scholar] [CrossRef]
- Brockmann, P.E.; Perez, J.L.; Moya, A. Feasibility of unattended home polysomnography in children with sleep-disordered- breathing. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 1960–1964. [Google Scholar] [CrossRef]
- Rosen, C.L.; Larkin, E.K.; Kirchner, H.L.; Emancipator, J.L.; Bivins, S.F.; Surovec, S.A.; Martin, R.J.; Redline, S. Prevalence and risk factors for sleep-disordered breathing in 8 to 11 year-old children: Association with race and prematurity. J. Pediatr. 2003, 142, 383–389. [Google Scholar] [CrossRef]
- Franco, P.; Bourdin, H.; Braun, F.; Briffod, J.; Pin, I.; Challamel, M.J. Overnight polysomnography versus respiratory polygraphy in the diagnosis of pediatric obstructive sleep apnea. Arch. Pediatr. 2017, 24 (Suppl. 1), S16–S27. [Google Scholar]
- Scalzitti, N.; Hansen, S.; Maturo, S.; Lospinoso, J.; O’Connor, P. Comparison of home sleep apnea testing versus laboratory polysomnography for the diagnosis of obstructive sleep apnea in children. Int. J. Pediatr. Otorhinolaryngol. 2017, 100, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Gudnadottir, G.; Hafsten, L.; Redfors, S.; Ellegård, E.; Hellgren, J. Respiratory polygraphy in children with sleep-disordered breathing. J. Sleep Res. 2019, 28, e12856. [Google Scholar] [CrossRef] [PubMed]
- Imanguli, M.; Ulualp, S.O. Risk factors for residual obstructive sleep apnea after adenotonsillectomy in children. Laryngoscope 2016, 126, 2624–2629. [Google Scholar] [CrossRef]
- Gozal, D.; Tan, H.L.; Kheirandish-Gozal, L. Treatment of obstructive sleep apnea in children: Handling the unknown with precision. J. Clin. Med. 2020, 9, 888. [Google Scholar] [CrossRef]
- Tan, H.L.; Kheirandish-Gozal, L.; Gozal, D. Pediatric home sleep apnea testing; slowly getting there! Chest 2015, 148, 1382–1395. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.C.; Chaput, K.H.; Kirk, V.; Yunker, W. Overnight oximetry in children undergoing adenotonsillectomy: A single center experience. J. Otolaryngol. Head Neck Surg. 2019, 48, 69. [Google Scholar] [CrossRef]
- Weinstock, T.G.; Rosen, C.L.; Marcus, C.L.; Garetz, S.; Mitchell, R.B.; Amin, R.; Paruthi, S.; Katz, E.; Arens, M.; Weng, J.; et al. Predictors of obstructive sleep apnea severity in adenotonsillectomy candidates. Sleep 2014, 37, 261–262. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Age (years) | 7 ± 4 |
| Weight (kg) | 28 ± 15 |
| Height (cm) | 122 ± 22 |
| BMI (kg/m2) | 19 ± 5 |
| BMI percentile | 62 ± 38 |
| Parameter | Value |
|---|---|
| Duration of recording (minutes) | 461 ± 95 |
| AHI (h−1) | 10 ± 9 |
| ODI (h−1) | 4 ± 7 |
| Baseline SpO2 (%) | 97 ± 2 |
| Minimum SpO2 (%) | 81 ± 8 |
| CT90% (minutes) | 3 ± 5 |
| Group A (HRP) | Group B (PSG) | p Value | |
|---|---|---|---|
| Sex | |||
| - Boy - Girl | 46% (55) 35% (42) | 12% (15) 7% (9) | NS |
| Concomitant disease | 20% (19) | 46% (11) | p < 0.001 |
| Snoring | 100% (97) | 100% (24) | NS |
| Apnea | 87% (84) | 88% (21) | NS |
| Shortness of breath | 35% (34) | 46% (11) | NS |
| Restless sleep | 36% (35) | 46% (11) | NS |
| Rhinorrhea | 12% (12) | 0% (0) | NS |
| Nasal obstruction | 32% (31) | 38% (9) | NS |
| Mouth breathing | 32% (31) | 38% (9) | NS |
| Tonsillitis | 53% (51) | 54% (13) | NS |
| Vomiting/nausea | 3% (3) | 0% (0) | NS |
| Swallowing disorder | 8% (8) | 25% (6) | p < 0.05 |
| Night sweats | 3% (3) | 4% (1) | NS |
| Hearing problems | 5% (5) | 8% (2) | NS |
| Daytime drowsiness | 20% (19) | 21% (5) | NS |
| Poor appetite | 13% (13) | 13% (3) | NS |
| Frequent otitis media | 28% (27) | 33% (8) | NS |
| Shyness | 4% (4) | 0% (0) | NS |
| Attention deficit | 14% (14) | 13% (3) | NS |
| Poor academic performance | 8% (8) | 13% (3) | NS |
| Enuresis | 9% (9) | 8% (2) | NS |
| Headaches | 3% (3) | 4% (1) | NS |
| Heartburn | 1% (1) | 0% (0) | NS |
| Wheezing | 8% (8) | 13% (3) | NS |
| Failure to thrive | 18% (17) | 17% (4) | NS |
| Group A (HRP) | Group B (PSG) | p Value | |
|---|---|---|---|
| Tonsillar hypertrophy | 93% (90) | 88% (21) | NS |
| Adenoid hypertrophy | 87% (84) | 88% (21) | NS |
| High-arched palate | 14% (14) | 13% (3) | NS |
| Macroglossia | 1% (1) | 0% (0) | NS |
| Facial skeleton abnormality | 3% (3) | 0% (0) | NS |
| Micrognathia | 1% (1) | 0% (0) | NS |
| Prognathism | 3% (3) | 8% (2) | NS |
| Retrognathia | 16% (15) | 4% (1) | NS |
| Malocclusion | 3% (3) | 8% (2) | NS |
| Dolichocephaly | 7% (7) | 8% (2) | NS |
| Adenoid facies | 34% (33) | 25% (6) | NS |
| Obesity | 20% (19) | 21% (5) | NS |
| Group A (HRP) (Mean ± SD) | Group B (PSG) (Mean ± SD) | p Value | |
|---|---|---|---|
| Age (years) | 7 ± 4 | 7 ± 4 | NS |
| Weight (kg) | 28 ± 16 | 25 ± 11 | NS |
| Height (cm) | 123 ± 22 | 118 ± 20 | NS |
| BMI (kg/m2) | 18 ± 4 | 20 ± 5 | NS |
| BMI percentile | 60 ± 40 | 72 ± 32 | NS |
| Recording duration (mins) | 473 ± 92 | 411 ± 90 | NS |
| AHI (h−1) | 8 ± 8 | 14 ± 11 | p < 0.01 |
| ODI (h−1) | 3 ± 5 | 8 ± 10 | p < 0.001 |
| Baseline SpO2 (%) | 97 ± 1 | 97 ± 1 | NS |
| Minimum SpO2 (%) | 80 ± 8 | 83 ± 9 | NS |
| CT90% | 3 ± 4 | 6 ± 8 | p < 0.01 |
| Group A (HRP) % (n) | Group B (PSG) % (n) | p Value | |
|---|---|---|---|
| Adenotonsillectomy | 76% (74) | 79% (19) | NS |
| Conservative | 17% (16) | 4% (1) | NS |
| CPAP | 7% (7) | 13% (3) | NS |
| BiPAP | 0% (0) | 4% (1) | NS |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiner, E.; Cánovas, C.; Molina, V.; Sancho-Chust, J.N.; Vañes, S.; Pastor, E.; Martinez-Garcia, M.A. Home Respiratory Polygraphy is Useful in the Diagnosis of Childhood Obstructive Sleep Apnea Syndrome. J. Clin. Med. 2020, 9, 2067. https://doi.org/10.3390/jcm9072067
Chiner E, Cánovas C, Molina V, Sancho-Chust JN, Vañes S, Pastor E, Martinez-Garcia MA. Home Respiratory Polygraphy is Useful in the Diagnosis of Childhood Obstructive Sleep Apnea Syndrome. Journal of Clinical Medicine. 2020; 9(7):2067. https://doi.org/10.3390/jcm9072067
Chicago/Turabian StyleChiner, Eusebi, Cristina Cánovas, Virginia Molina, Jose N. Sancho-Chust, Sandra Vañes, Esther Pastor, and Miguel Angel Martinez-Garcia. 2020. "Home Respiratory Polygraphy is Useful in the Diagnosis of Childhood Obstructive Sleep Apnea Syndrome" Journal of Clinical Medicine 9, no. 7: 2067. https://doi.org/10.3390/jcm9072067
APA StyleChiner, E., Cánovas, C., Molina, V., Sancho-Chust, J. N., Vañes, S., Pastor, E., & Martinez-Garcia, M. A. (2020). Home Respiratory Polygraphy is Useful in the Diagnosis of Childhood Obstructive Sleep Apnea Syndrome. Journal of Clinical Medicine, 9(7), 2067. https://doi.org/10.3390/jcm9072067