ECG Changes in Melanoma Patients Undergoing Cancer Therapy—Data from the ECoR Registry

 ,
, 
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Baseline Characteristics
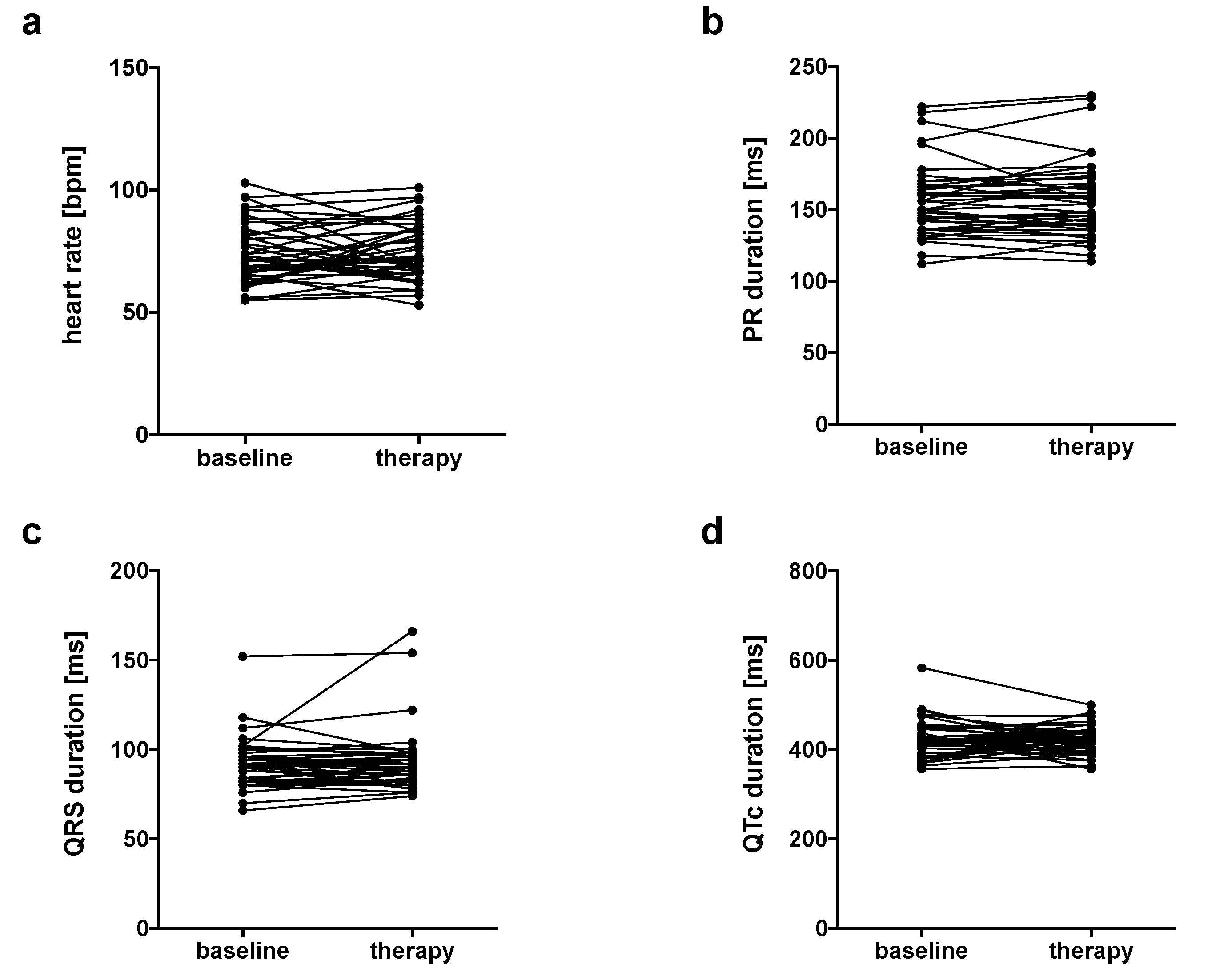
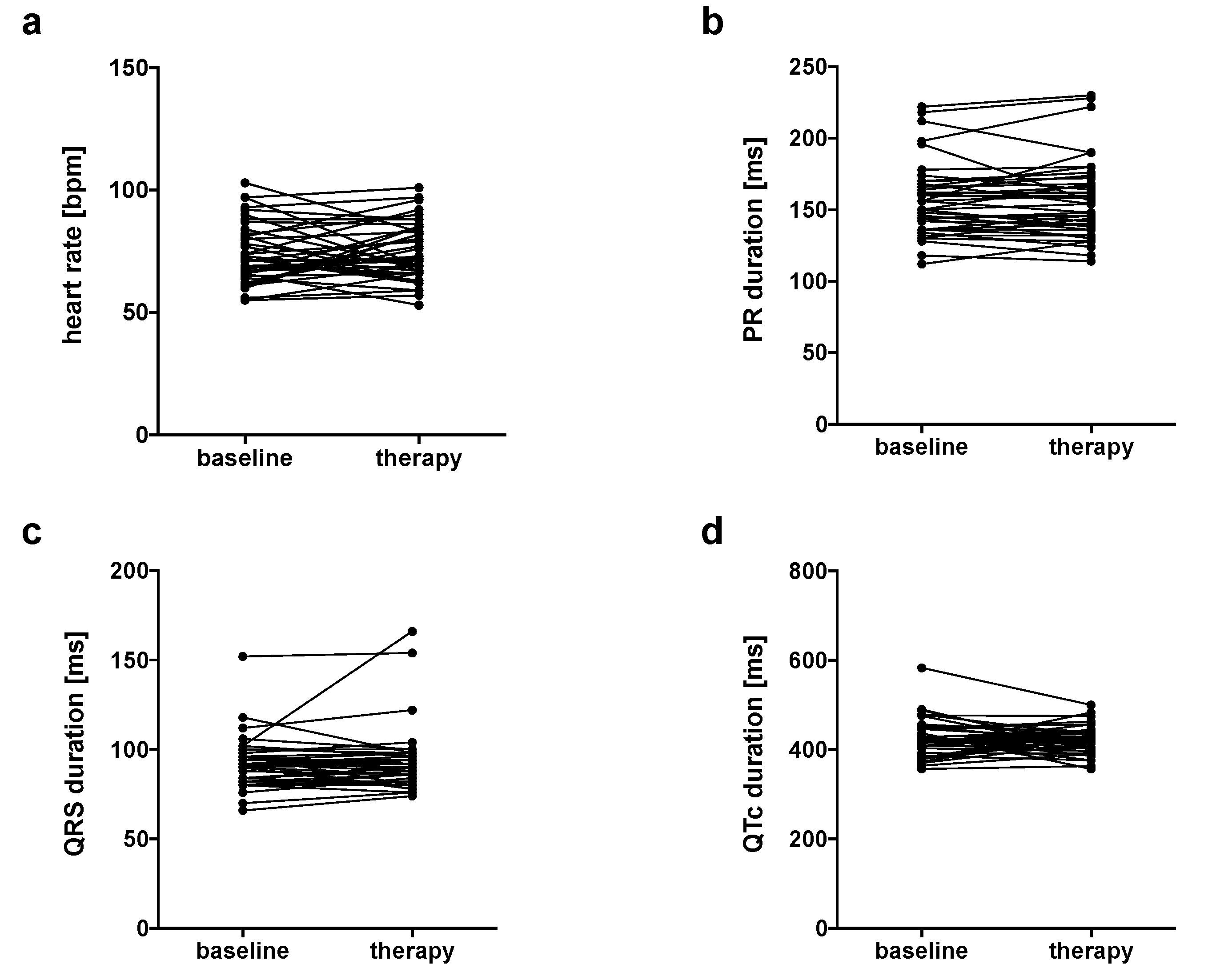
3.2. No Changes in Heart Rate, PR, QRS and QTc Intervals
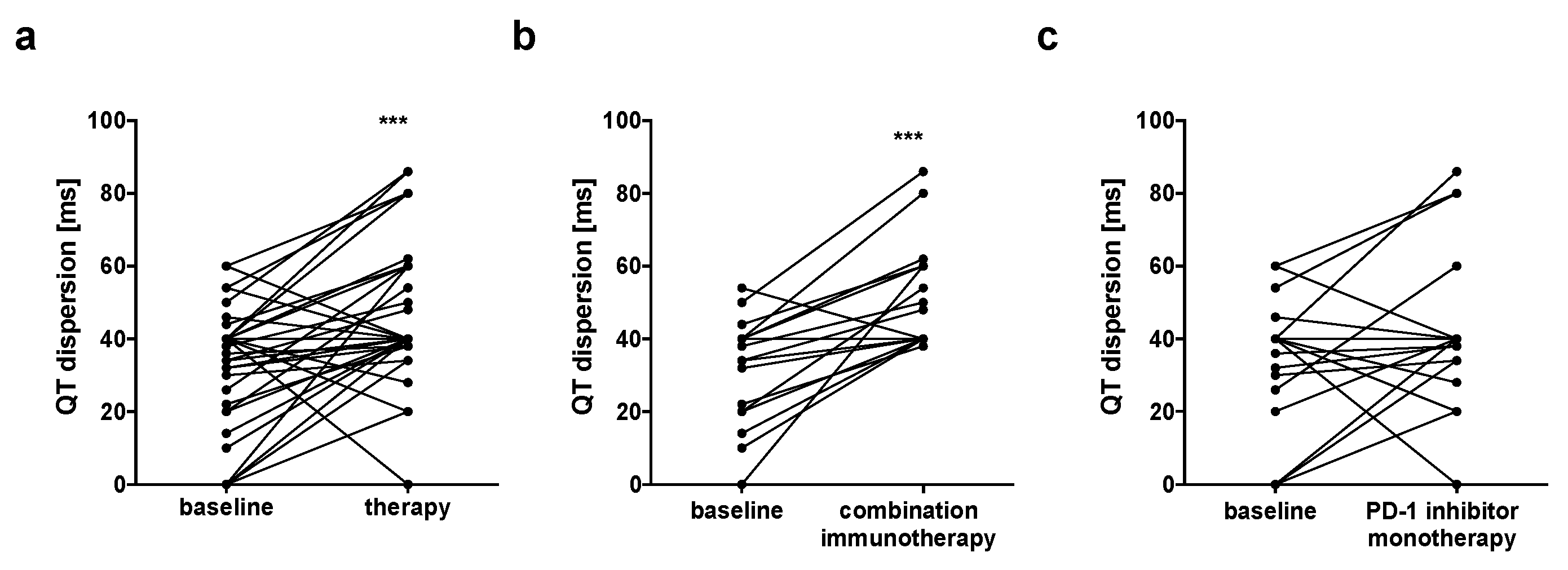
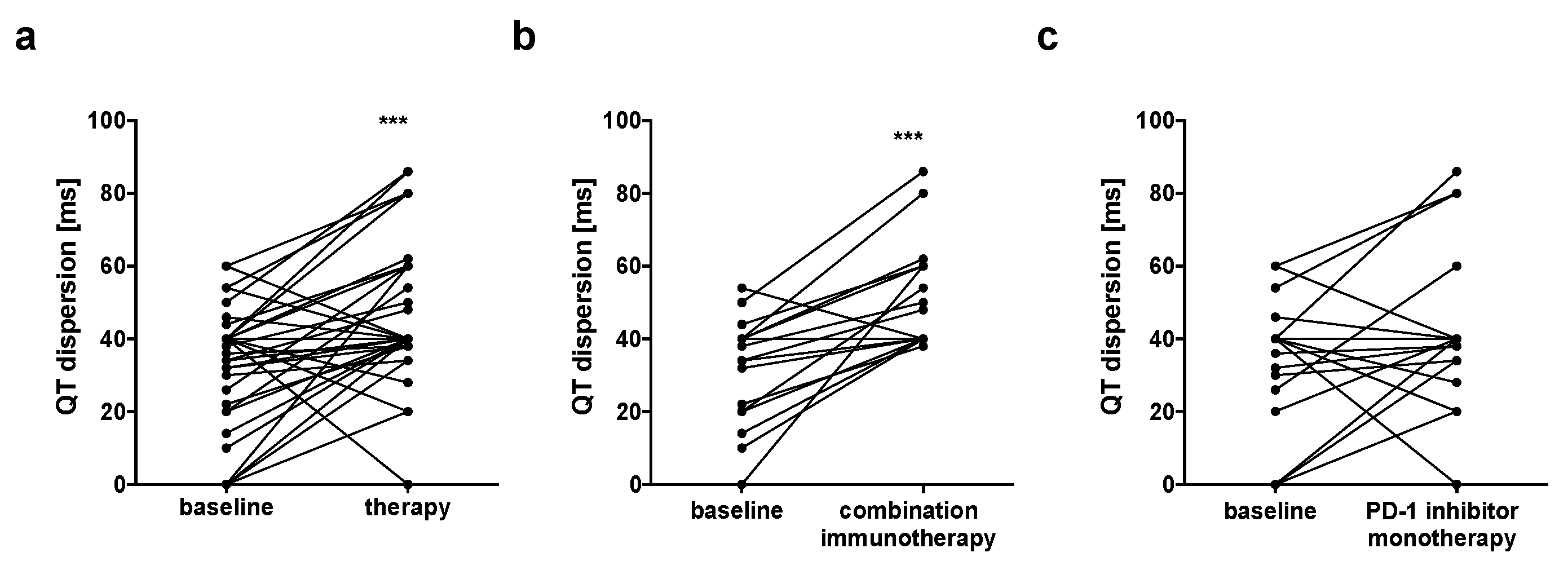
3.3. Prolongation of QT Dispersion in Patients Undergoing Combination Immunotherapy
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Schadendorf, D.; van Akkooi, A.C.J.; Berking, C.; Griewank, K.G.; Gutzmer, R.; Hauschild, A.; Stang, A.; Roesch, A.; Ugurel, S. Melanoma. Lancet 2018, 392, 971–984. [Google Scholar] [CrossRef]
- Robert, C.; Ribas, A.; Wolchok, J.D.; Hodi, F.S.; Hamid, O.; Kefford, R.; Weber, J.S.; Joshua, A.M.; Hwu, W.J.; Gangadhar, T.C.; et al. Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: A randomised dose-comparison cohort of a phase 1 trial. Lancet 2014, 384, 1109–1117. [Google Scholar] [CrossRef]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.Y.; Salem, J.E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L.; et al. Fatal Toxic Effects Associated With Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef] [Green Version]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in Patients Treated with Immune Checkpoint Inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. [Google Scholar] [CrossRef]
- Lyon, A.R.; Yousaf, N.; Battisti, N.M.L.; Moslehi, J.; Larkin, J. Immune checkpoint inhibitors and cardiovascular toxicity. Lancet Oncol. 2018, 19, e447–e458. [Google Scholar] [CrossRef]
- Johnson, D.B.; Chandra, S.; Sosman, J.A. Immune Checkpoint Inhibitor Toxicity in 2018. JAMA 2018, 320, 1702–1703. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2017, 19, 9–42. [Google Scholar] [CrossRef]
- Michel, L.; Mincu, R.I.; Mahabadi, A.A.; Settelmeier, S.; Al-Rashid, F.; Rassaf, T.; Totzeck, M. Troponins and brain natriuretic peptides for the prediction of cardiotoxicity in cancer patients: A meta-analysis. Eur. J. Heart Fail. 2020, 22, 350–361. [Google Scholar] [CrossRef] [Green Version]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648, 48a–48d. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Tao, J.; Zhai, M.; Li, C.; Zhou, N.; Lv, J.; Wang, L.; Lin, L.; Bai, R. Anticancer drugs-related QTc prolongation, torsade de pointes and sudden death: Current evidence and future research perspectives. Oncotarget 2018, 9, 25738–25749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porta-Sanchez, A.; Gilbert, C.; Spears, D.; Amir, E.; Chan, J.; Nanthakumar, K.; Thavendiranathan, P. Incidence, Diagnosis, and Management of QT Prolongation Induced by Cancer Therapies: A Systematic Review. J. Am. Heart Assoc. 2017, 6, e007724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, C.P.; McComb, J.M.; Campbell, R.W. QT dispersion: An indication of arrhythmia risk in patients with long QT intervals. Br. Heart J. 1990, 63, 342–344. [Google Scholar] [CrossRef] [Green Version]
- Zabel, M.; Portnoy, S.; Franz, M.R. Electrocardiographic indexes of dispersion of ventricular repolarization: An isolated heart validation study. J. Am. Coll. Cardiol. 1995, 25, 746–752. [Google Scholar] [CrossRef] [Green Version]
- Moreno, F.L.; Villanueva, T.; Karagounis, L.A.; Anderson, J.L. Reduction in QT interval dispersion by successful thrombolytic therapy in acute myocardial infarction. TEAM-2 Study Investigators. Circulation 1994, 90, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Day, C.P.; McComb, J.M.; Matthews, J.; Campbell, R.W. Reduction in QT dispersion by sotalol following myocardial infarction. Eur. Heart J. 1991, 12, 423–427. [Google Scholar] [CrossRef]
- Bazoukis, G.; Yeung, C.; Wui Hang Ho, R.; Varrias, D.; Papadatos, S.; Lee, S.; Ho Christien Li, K.; Sakellaropoulou, A.; Saplaouras, A.; Kitsoulis, P.; et al. Association of QT dispersion with mortality and arrhythmic events-A meta-analysis of observational studies. J. Arrhythm. 2020, 36, 105–115. [Google Scholar] [CrossRef]
- Orditura, M.I.; Sarubbi, B.E.; DeVita, F.E.; Ducceschi, V.A.; Santangelo, L.U.; Cariello, A.; Iacono, A.; Catalano, G. Prolonged corrected QT dispersion. Oncol. Rep. 1997, 4, 1047–1050. [Google Scholar] [CrossRef]
- Nakamae, H.; Tsumura, K.; Hino, M.; Hayashi, T.; Tatsumi, N. QT dispersion as a predictor of acute heart failure after high-dose cyclophosphamide. Lancet 2000, 355, 805–806. [Google Scholar] [CrossRef]
- Tanriverdi, O.; Meydan, N.; Barutca, S. Long-term effect of trastuzumab on QT dispersion in adjuvant treatment for patients with Her2 receptor positive breast cancer: A pilot study. Med. Oncol. 2012, 29, 3265–3271. [Google Scholar] [CrossRef] [PubMed]
- Sahu, P.; Lim, P.O.; Rana, B.S.; Struthers, A.D. QT dispersion in medicine: Electrophysiological holy grail or fool’s gold? QJM 2000, 93, 425–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, M.; Batchvarov, V.N. Measurement, interpretation and clinical potential of QT dispersion. J. Am. Coll. Cardiol. 2000, 36, 1749–1766. [Google Scholar] [CrossRef] [Green Version]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anker, M.S.; Frey, M.K.; Goliasch, G.; Bartko, P.E.; Prausmüller, S.; Gisslinger, H.; Kornek, G.; Strunk, G.; Raderer, M.; Zielinski, C.; et al. Increased resting heart rate and prognosis in treatment-naive unselected cancer patients: Results from a prospective observational study. Eur. J. Heart Fail. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anker, M.S.; Ebner, N.; Hildebrandt, B.; Springer, J.; Sinn, M.; Riess, H.; Anker, S.D.; Landmesser, U.; Haverkamp, W.; von Haehling, S. Resting heart rate is an independent predictor of death in patients with colorectal, pancreatic, and non-small cell lung cancer: Results of a prospective cardiovascular long-term study. Eur. J. Heart Fail. 2016, 18, 1524–1534. [Google Scholar] [CrossRef]
- Piotrowski, G.; Gawor, R.; Stasiak, A.; Gawor, Z.; Potemski, P.; Banach, M. Cardiac complications associated with trastuzumab in the setting of adjuvant chemotherapy for breast cancer overexpressing human epidermal growth factor receptor type 2—A prospective study. Arch. Med. Sci. 2012, 8, 227–235. [Google Scholar] [CrossRef]
- Benjanuwattra, J.; Siri-Angkul, N.; Chattipakorn, S.C.; Chattipakorn, N. Doxorubicin and its proarrhythmic effects: A comprehensive review of the evidence from experimental and clinical studies. Pharm. Res. 2020, 151, 104542. [Google Scholar] [CrossRef]
- Zhang, L.; Awadalla, M.; Mahmood, S.S.; Nohria, A.; Hassan, M.Z.; Thuny, F.; Zlotoff, D.A.; Murphy, S.P.; Stone, J.R.; Golden, D.L.; et al. Cardiovascular magnetic resonance in immune checkpoint inhibitor-associated myocarditis. Eur. Heart J. 2020. [Google Scholar] [CrossRef]
- Michel, L.; Rassaf, T.; Totzeck, M. Cardiotoxicity from immune checkpoint inhibitors. Int. J. Cardiol. Heart Vasc. 2019, 25, 100420. [Google Scholar] [CrossRef]
- Agrawal, S.; Waxman, I.; Lambert, A.; Roy, A.; Darbenzio, R. Evaluation of the potential for QTc prolongation in patients with solid tumors receiving nivolumab. Cancer Chemother. Pharm. 2016, 77, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Black, N.; D’Souza, A.; Wang, Y.; Piggins, H.; Dobrzynski, H.; Morris, G.; Boyett, M.R. Circadian rhythm of cardiac electrophysiology, arrhythmogenesis, and the underlying mechanisms. Heart Rhythm 2019, 16, 298–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilan, A.; Witczak, A.; Palusinski, R.; Ignatowicz, A.; Hanzlik, J. Circadian rhythm of the QT interval dispersion in healthy subjects. Correlation with heart rate variability circadian pattern. J. Electrocardiol. 2005, 38, 36–42. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Parameters | All (n = 41) | Combination Immunotherapy (n = 21) | PD-1 Inhibitor Monotherapy (n = 20) |
|---|---|---|---|
| Age (years), mean ± SD | 61 ± 12 | 61 ± 14 | 60 ± 11 |
| Female sex (%) | 46 | 48 | 45 |
| BMI (kg/m2), mean ± SD | 27.3 ± 4.2 | 26 ± 3 | 28.7 ± 4.9 |
| Hemoglobin (g/dL), median (range) | 13.1 (8–16) | 13.7 (10–16) | 13.7 (10–16) |
| Platelets (×1000/µL), median (range) | 274 (154–577) | 263 (234–577) | 273 (161–549) |
| Creatinine (mg/dL), median (range) | 0.9 (0.7–1.4) | 1 (0.7–1.4) | 0.9 (0.5–1.1) |
| CRP (mg/dL), median (range) | 0 (0–18) | 0 (1–18) | 0 (0–4) |
| Troponin (ng/L), median (range) | 5 (0–114) | 0 (0–114) | 0 (0–17) |
| NTproBNP (pg/mL), median (range) | 70 (9–848) | 87 (9–512) | 51 (20–848) |
| Comorbidities | |||
| Arterial hypertension (%) | 41 | 38 | 45 |
| Diabetes (%) | 5 | 5 | 5 |
| Smoking (%) | 24 | 14 | 10 |
| Previous stroke (%) | 7 | 10 | 5 |
| Known CAD (%) | 7 | 0 | 15 |
| Known CHF (%) | 10 | 10 | 10 |
| Premedication | |||
| ACE-I/ARB (%) | 32 | 29 | 35 |
| Betablocker (%) | 29 | 29 | 30 |
| Statins (%) | 7 | 5 | 10 |
| Aspirin/DAPT (%) | 22 | 5 | 20 |
| Tumor stadium III (%) | 29 | 38 | 20 |
| Tumor stadium IV (%) | 71 | 62 | 80 |
| Therapy regimen | |||
| Nivolumab monotherapy (%) | 46 | 0 | 100 |
| Nivolumab/Ipilimumab (%) | 53 | 100 | 0 |
| ECG Parameters | All (n = 41) | Combination Immunotherapy (n = 21) | PD-1 Inhibitor Monotherapy (n = 20) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Therapy | p | Baseline | Therapy | p | Baseline | Therapy | p | |
| Heart rate (bpm) | 74 ± 12 | 75 ± 12 | 0.6201 | 74 ± 10 | 79 ± 12 | 0.0367 | 73 ± 15 | 70 ± 10 | 0.3283 |
| PR interval (ms) | 157 ± 26 | 157 ± 28 | 0.7681 | 157 ± 25 | 155 ± 25 | 0.4475 | 156 ± 27 | 160 ± 31 | 0.0495 |
| 1st degree AV block (%) | 7.3 | 7.3 | 1.0000 | 4.8 | 4.8 | 1.0000 | 5 | 10 | 1.0000 |
| 2nd degree AV block (%) | 0 | 0 | - | 0 | 0 | - | 0 | 0 | - |
| 3rd degree AV block (%) | 0 | 0 | - | 0 | 0 | - | 0 | 0 | - |
| QRS interval (ms) | 92 ± 14 | 93 ± 18 | 0.6431 | 91 ± 13 | 93 ± 20 | 0.6736 | 94 ± 15 | 94 ± 16 | 0.8557 |
| LBBB (%) | 0 | 0 | - | 0 | 0 | - | 0 | 0 | - |
| RBBB (%) | 0 | 0 | - | 0 | 0 | - | 0 | 0 | - |
| QTc interval (ms) | 428 ± 42 | 421 ± 31 | 0.3383 | 432 ± 50 | 424 ± 32 | 0.4055 | 423 ± 32 | 419 ± 30 | 0.6240 |
| QTc > 450 ms (%) | 24.3 | 14.6 | 0.7284 | 33.3 | 14.3 | 0.7174 | 20 | 15 | 1.00 |
| QTd (ms) | 32 ± 16 | 47 ± 19 | <0.0001 | 31 ± 14 | 51 ± 14 | <0.0001 | 32 ± 18 | 41 ± 21 | 0.1099 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pohl, J.; Mincu, R.-I.; Mrotzek, S.M.; Hinrichs, L.; Michel, L.; Livingstone, E.; Zimmer, L.; Wakili, R.; Schadendorf, D.; Rassaf, T.; et al. ECG Changes in Melanoma Patients Undergoing Cancer Therapy—Data from the ECoR Registry. J. Clin. Med. 2020, 9, 2060. https://doi.org/10.3390/jcm9072060
Pohl J, Mincu R-I, Mrotzek SM, Hinrichs L, Michel L, Livingstone E, Zimmer L, Wakili R, Schadendorf D, Rassaf T, et al. ECG Changes in Melanoma Patients Undergoing Cancer Therapy—Data from the ECoR Registry. Journal of Clinical Medicine. 2020; 9(7):2060. https://doi.org/10.3390/jcm9072060
Chicago/Turabian StylePohl, Julia, Raluca-Ileana Mincu, Simone Maria Mrotzek, Lena Hinrichs, Lars Michel, Elisabeth Livingstone, Lisa Zimmer, Reza Wakili, Dirk Schadendorf, Tienush Rassaf, and et al. 2020. "ECG Changes in Melanoma Patients Undergoing Cancer Therapy—Data from the ECoR Registry" Journal of Clinical Medicine 9, no. 7: 2060. https://doi.org/10.3390/jcm9072060
APA StylePohl, J., Mincu, R.-I., Mrotzek, S. M., Hinrichs, L., Michel, L., Livingstone, E., Zimmer, L., Wakili, R., Schadendorf, D., Rassaf, T., & Totzeck, M. (2020). ECG Changes in Melanoma Patients Undergoing Cancer Therapy—Data from the ECoR Registry. Journal of Clinical Medicine, 9(7), 2060. https://doi.org/10.3390/jcm9072060