Long-Term Efficacy of the Workshop Vs. Online SUCCEAT (Supporting Carers of Children and Adolescents with Eating Disorders) Intervention for Parents: A Quasi-Randomised Feasibility Trial

 , , , , ,
, , , , , 

Abstract
1. Introduction
2. Methods
2.1. Study Design
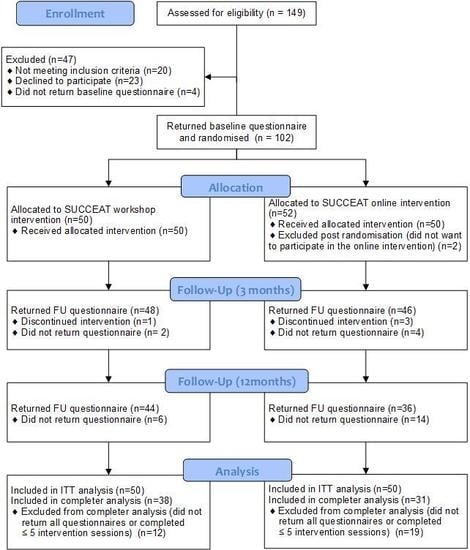
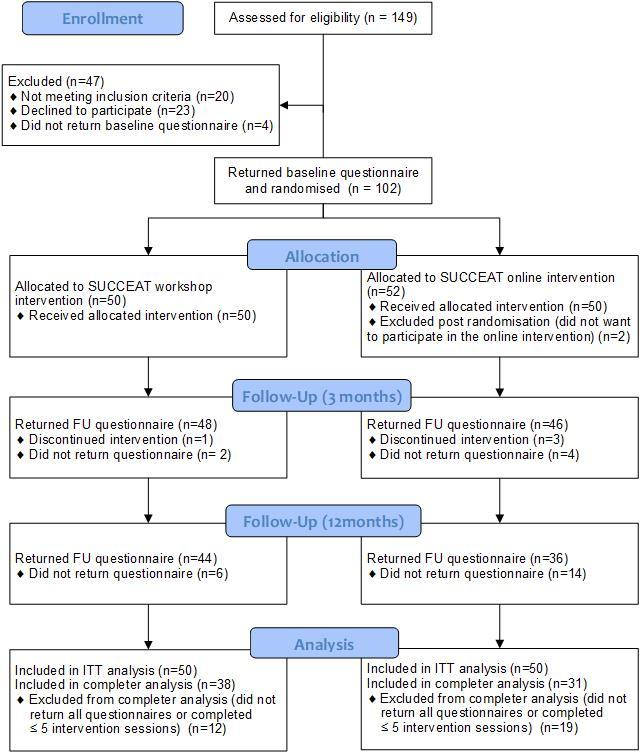
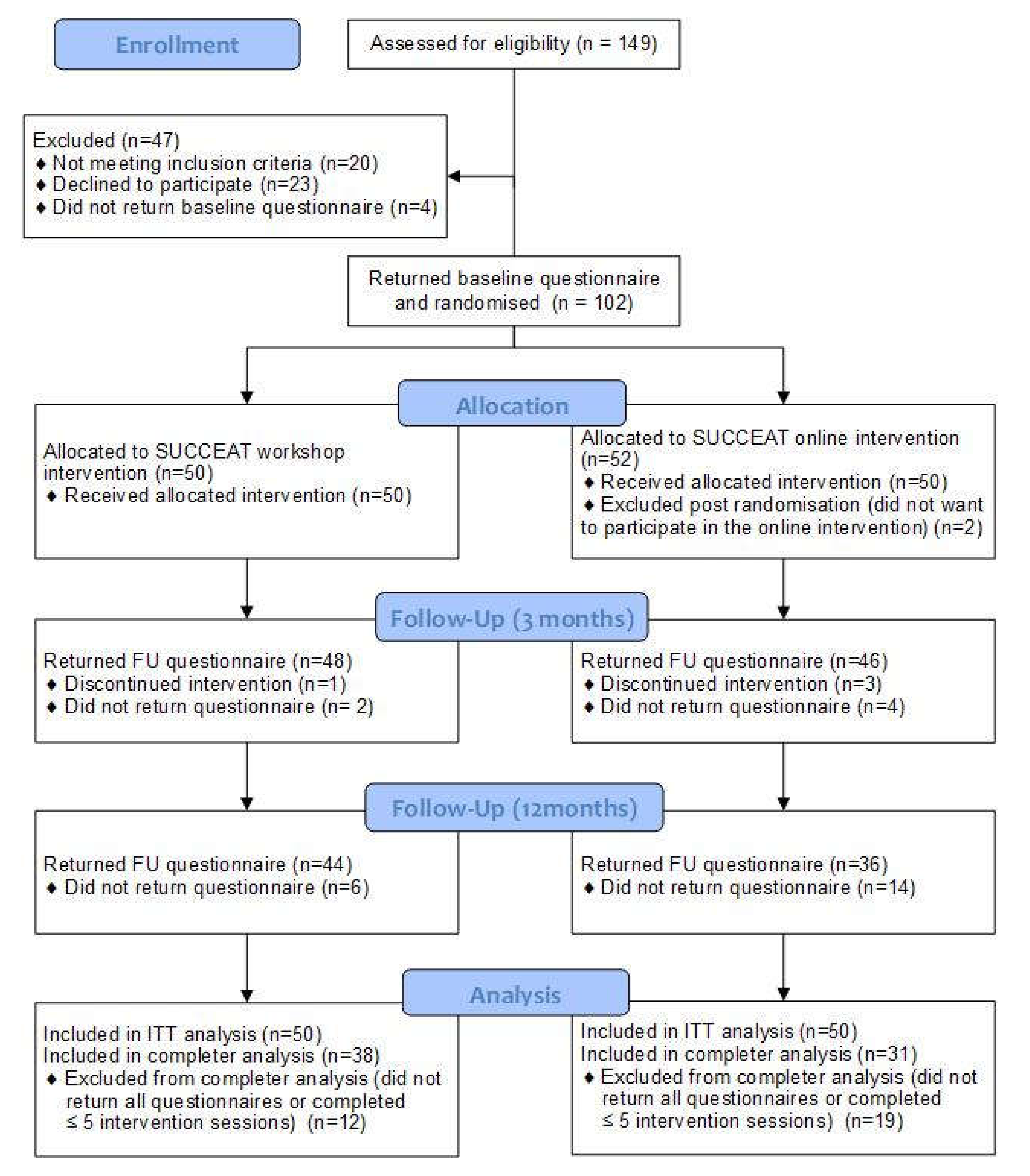
2.2. Recruitment and Randomisation
2.3. Interventions
2.3.1. Workshop Group
2.3.2. Online Group
2.3.3. Comparison Group
2.4. Assessments
2.5. Statistical Analysis
3. Results
3.1. Participants
3.2. Adherence
3.3. Primary Outcome
3.4. Secondary Outcomes
3.5. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Guideline Alliance (UK). Eating Disorders: Recognition and Treatment; National Institute for Health and Care Excellence: Clinical Guidelines; National Institute for Health and Care Excellence (UK): London, UK, 2017. [Google Scholar]
- Herpertz-Dahlmann, B.; van Elburg, A.; Castro-Fornieles, J.; Schmidt, U. ESCAP Expert Paper: New developments in the diagnosis and treatment of adolescent anorexia nervosa—A European perspective. Eur. Child Adolesc. Psychiatry 2015, 24, 1153–1167. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, U.; Treasure, J. Anorexia nervosa: Valued and visible. A cognitive-interpersonal maintenance model and its implications for research and practice. Br. J. Clin. Psychol. 2006, 45, 343–366. [Google Scholar] [CrossRef] [PubMed]
- Zabala, M.J.; Macdonald, P.; Treasure, J. Appraisal of caregiving burden, expressed emotion and psychological distress in families of people with eating disorders: A systematic review. Eur. Eat. Disord. Rev. 2009, 17, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Treasure, J.; Whitaker, W.; Todd, G.; Whitney, J. A description of multiple family workshops for carers of people with anorexia nervosa. Eur. Eat. Disord. Rev. 2012, 20, e17–e22. [Google Scholar] [CrossRef]
- Rhind, C.; Salerno, L.; Hibbs, R.; Micali, N.; Schmidt, U.; Gowers, S.; Macdonald, P.; Goddard, E.; Todd, G.; Tchanturia, K.; et al. The Objective and Subjective Caregiving Burden and Caregiving Behaviours of Parents of Adolescents with Anorexia Nervosa. Eur. Eat. Disord. Rev. 2016, 24. [Google Scholar] [CrossRef]
- Kyriacou, O.; Treasure, J.; Schmidt, U. Understanding how parents cope with living with someone with anorexia nervosa: Modelling the factors that are associated with carer distress. Int. J. Eat. Disord. 2008, 41, 233–242. [Google Scholar] [CrossRef]
- Anastasiadou, D.; Medina-Pradas, C.; Sepulveda, A.R.; Treasure, J. A systematic review of family caregiving in eating disorders. Eat. Behav. 2014, 15, 464–477. [Google Scholar] [CrossRef]
- Hibbs, R.; Rhind, C.; Leppanen, J.; Treasure, J. Interventions for caregivers of someone with an eating disorder: A meta-analysis. Int. J. Eat. Disord. 2015, 48, 349–361. [Google Scholar] [CrossRef]
- Treasure, J.; Schmidt, U. The cognitive-interpersonal maintenance model of anorexia nervosa revisited: A summary of the evidence for cognitive, socio-emotional and interpersonal predisposing and perpetuating factors. J. Eat. Disord. 2013, 1, 13. [Google Scholar] [CrossRef]
- Treasure, J.; Willmott, D.; Ambwani, S.; Cardi, V.; Clark Bryan, D.; Rowlands, K.; Schmidt, U. Cognitive Interpersonal Model for Anorexia Nervosa Revisited: The Perpetuating Factors that Contribute to the Development of the Severe and Enduring Illness. J. Clin. Med. 2020, 9. [Google Scholar] [CrossRef]
- Whitney, J.; Murphy, T.; Landau, S.; Gavan, K.; Todd, G.; Whitaker, W.; Treasure, J. A practical comparison of two types of family intervention: An exploratory RCT of family day workshops and individual family work as a supplement to inpatient care for adults with anorexia nervosa. Eur. Eat. Disord. Rev. J. Eat. Disord. Assoc. 2012, 20, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, A.R.; Lopez, C.; Todd, G.; Whitaker, W.; Treasure, J. An examination of the impact of “the Maudsley eating disorder collaborative care skills workshops” on the well being of carers: A pilot study. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Goddard, E.; Macdonald, P.; Sepulveda, A.R.; Naumann, U.; Landau, S.; Schmidt, U.; Treasure, J. Cognitive interpersonal maintenance model of eating disorders: Intervention for carers. Br. J. Psychiatry 2011, 199, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Hodsoll, J.; Rhind, C.; Micali, N.; Hibbs, R.; Goddard, E.; Nazar, B.P.; Schmidt, U.; Gowers, S.; Macdonald, P.; Todd, G.; et al. A Pilot, Multicentre Pragmatic Randomised Trial to Explore the Impact of Carer Skills Training on Carer and Patient Behaviours: Testing the Cognitive Interpersonal Model in Adolescent Anorexia Nervosa. Eur. Eat. Disord. Rev. J. Eat. Disord. Assoc. 2017, 25, 551–561. [Google Scholar] [CrossRef] [PubMed]
- Hibbs, R.; Magill, N.; Goddard, E.; Rhind, C.; Raenker, S.; Macdonald, P.; Todd, G.; Arcelus, J.; Morgan, J.; Beecham, J.; et al. Clinical effectiveness of a skills training intervention for caregivers in improving patient and caregiver health following in-patient treatment for severe anorexia nervosa: Pragmatic randomised controlled trial. BJPsych Open 2015, 1, 56–66. [Google Scholar] [CrossRef]
- Grover, M.; Naumann, U.; Mohammad-Dar, L.; Glennon, D.; Ringwood, S.; Eisler, I.; Williams, C.; Treasure, J.; Schmidt, U. A randomized controlled trial of an Internet-based cognitive-behavioural skills package for carers of people with anorexia nervosa. Psychol. Med. 2011, 41, 2581–2591. [Google Scholar] [CrossRef]
- Hoyle, D.; Slater, J.; Williams, C.; Schmidt, U.; Wade, T.D. Evaluation of a web-based skills intervention for carers of people with anorexia nervosa: A randomized controlled trial. Int. J. Eat. Disord. 2013, 46, 634–638. [Google Scholar] [CrossRef]
- Dimitropoulos, G.; Landers, A.; Freeman, V.; Novick, J.; Schmidt, U.; Olmsted, M. A feasibility study comparing a web-based intervention to a workshop intervention for caregivers of adults with eating disorders. Eur. Eat. Disord. Rev. 2019, 27, 641–654. [Google Scholar] [CrossRef]
- Amichai-Hamburger, Y.; Vinitzky, G. Social network use and personality. Comput. Hum. Behav. 2010, 26, 1289–1295. [Google Scholar] [CrossRef]
- Titov, N.; Hadjistavropoulos, H.D.; Nielssen, O.; Mohr, D.C.; Andersson, G.; Dear, B.F. From Research to Practice: Ten Lessons in Delivering Digital Mental Health Services. J. Clin. Med. 2019, 8, 1239. [Google Scholar] [CrossRef]
- Spencer, L.; Potterton, R.; Allen, K.; Musiat, P.; Schmidt, U. Internet-Based Interventions for Carers of Individuals With Psychiatric Disorders, Neurological Disorders, or Brain Injuries: Systematic Review. J. Med. Internet Res. 2019, 21, e10876. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.B.; Fitzsimmons-Craft, E.E.; Graham, A.K. Digital technology can revolutionize mental health services delivery: The COVID-19 crisis as a catalyst for change. Int. J. Eat. Disord. 2020. [Google Scholar] [CrossRef] [PubMed]
- Grover, M.; Williams, C.; Eisler, I.; Fairbairn, P.; McCloskey, C.; Smith, G.; Treasure, J.; Schmidt, U. An off-line pilot evaluation of a web-based systemic cognitive-behavioral intervention for carers of people with anorexia nervosa. Int. J. Eat. Disord. 2011, 44, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Zipfel, S.; Giel, K.E.; Bulik, C.M.; Hay, P.; Schmidt, U. Anorexia nervosa: Aetiology, assessment, and treatment. Lancet Psychiatry 2015, 2, 1099–1111. [Google Scholar] [CrossRef]
- Franta, C.; Philipp, J.; Waldherr, K.; Truttmann, S.; Merl, E.; Schöfbeck, G.; Koubek, D.; Laczkovics, C.; Imgart, H.; Zanko, A.; et al. Supporting Carers of Children and Adolescents with Eating Disorders in Austria (SUCCEAT): Study protocol for a randomised controlled trial. Eur. Eat. Disord. Rev. 2018, 26, 447–461. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://handbook-5-1.cochrane.org/ (accessed on 29 April 2020).
- Treasure, J.; Smith, G.; Crane, A. Skills-Based Learning for Caring for a Loved One with an Eating Disorder: The New Maudsley Method; Routledge: London, UK, 2007; pp. 1–245. [Google Scholar] [CrossRef]
- The Succeed Foundation. How to Care for Someone with an Eating Disorder; Learn the techniques designed by one of the world’s top eating disorder researchers; The Succeed Foundation: London, UK, 2011; (DVD). [Google Scholar]
- Imgart, H.; Plassmann, R. [Effective factors in multifamily therapy in patients with eating disorders: Critical appraisal and implications for practice]. Neuropsychiatr. Klin. Diagn. Ther. Rehabil. 2020. [Google Scholar] [CrossRef]
- Linden, M.; Maier, W.; Achberger, M.; Herr, R.; Helmchen, H.; Benkert, O. Psychische erkrankungen und ihre behandlung in allgemeinarztpraxen in Deutschland: Ergebnisse aus einer studie der Weltgesundheitsorganisation (WHO). [Psychological disorders and their treatment in general practice in Germany: Results of a WHO study.]. Nervenarzt 1996, 67, 205–215. [Google Scholar]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef]
- Sepulveda, A.R.; Whitney, J.; Hankins, M.; Treasure, J. Development and validation of an Eating Disorders Symptom Impact Scale (EDSIS) for carers of people with eating disorders. Health Qual. Life Outcomes 2008, 6, 28. [Google Scholar] [CrossRef]
- Franke, G.H. Die Symptom-Checkliste von Derogatis (SCL-90-R)—Deutsche; Version 2; Beltz: Göttingen, Germany, 2002. [Google Scholar]
- Hautzinger, M.; Keller, F.; Kühner, C. Beck Depressions Inventar, 2. Auflage (BDI-II); Pearson: Hallbergmoos, Germany, 2006. [Google Scholar]
- Kühner, C.; Bürger, C.; Keller, F.; Hautzinger, M. Reliabilität und Validität des revidierten Beck-Depressionsinventars (BDI-II). Nervenarzt 2007, 78, 651–656. [Google Scholar] [CrossRef]
- Laux, L.; Glanzmann, P.; Schaffner, P.; Spielsberger, C.D. STAI—Das State-Trait-Angstinventar, 1st ed.; Beltz: Weinheim, Germany, 1981. [Google Scholar]
- Hibbs, R.; Rhind, C.; Salerno, L.; Lo Coco, G.; Goddard, E.; Schmidt, U.; Micali, N.; Gowers, S.; Beecham, J.; Macdonald, P.; et al. Development and validation of a scale to measure caregiver skills in eating disorders. Int. J. Eat. Disord. 2015, 48, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Schlegl, S.; Bürger, C.; Schmidt, L.; Herbst, N.; Voderholzer, U. The potential of technology-based psychological interventions for anorexia and bulimia nervosa: A systematic review and recommendations for future research. J. Med. Internet Res. 2015, 17, e85. [Google Scholar] [CrossRef] [PubMed]
- Haigh, R.; Treasure, J. Investigating the needs of carers in the area of eating disorders: Development of the Carers’ Needs Assessment Measure (CANAM). Eur. Eat. Disord. Rev. 2003, 11, 125–141. [Google Scholar] [CrossRef]
- Yim, S.H.; Spencer, L.; Gordon, G.; Allen, K.; Musiat, P.; Schmidt, U. Eating disorder sufferers’ and carers’ views on online self-help programmes. Eur. J. Public Health 2019. (submitted). [Google Scholar]
- Wagner, G.; Penelo, E.; Wanner, C.; Gwinner, P.; Trofaier, M.-L.; Imgart, H.; Waldherr, K.; Wöber-Bingöl, C.; Karwautz, A.F.K. Internet-delivered cognitive-behavioural therapy v. conventional guided self-help for bulimia nervosa: Long-term evaluation of a randomised controlled trial. Br. J. Psychiatry J. Ment. Sci. 2013, 202, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Yim, S.H.; Schmidt, U. Self-Help Treatment of Eating Disorders. Psychiatr. Clin. 2019, 42, 231–241. [Google Scholar] [CrossRef]
- Fernández-Aranda, F.; Casas, M.; Claes, L.; Bryan, D.C.; Favaro, A.; Granero, R.; Gudiol, C.; Jiménez-Murcia, S.; Karwautz, A.; Grange, D.L.; et al. COVID-19 and implications for eating disorders. Eur. Eat. Disord. Rev. 2020, 28, 239–245. [Google Scholar] [CrossRef]
- Reich, G. Familienbeziehungen und Familientherapie bei Essstörungen. Prax. Kinderpsychol. Kinderpsychiatr. 2005, 54, 318–336. [Google Scholar]


{kind=link}
{kind=link}
| SUCCEAT Workshop Intervention (N = 50) | SUCCEAT Online Intervention (N = 50) | Group Difference | ||
|---|---|---|---|---|
| Test Statistic (df) | p | |||
| Carers (SUCCEAT Participants) | ||||
| Females (N, %) | 42 (84.0%) | 44 (88.0%) | χ2 (1) = 0.332 | 0.564 |
| Age (mean, SD) | 46.64 (5.43) | 47.72 (4.25) | t(98) = 1.108 | 0.271 |
| Highest educational degree | ||||
| university degree (N, %) | 30 (60.0%) | 23 (46.0%) | χ2 (2) = 2.885 | 0.236 |
| A level degree (N, %) | 11 (22.0%) | 11 (22.0%) | ||
| <A-level degree (N, %) | 9 (18.0%) | 16 (32.0%) | ||
| Marital status | ||||
| single (N, %) | 0 (0.0%) | 3 (6.3%) | χ2 (2) = 3.481 | 0.175 |
| married or living in partnership (N, %) | 42 (84.0%) | 36 (75.0%) | ||
| divorced or widowed (N, %) | 8 (16.0%) | 9 (18.8%) | ||
| Ethnicity | χ2 (1) = 0.000 | 1.000 | ||
| Caucasian (N, %) | 49 (98%) | 49 (98%) | ||
| Asian (N, %) | 1 (2%) | 1 (2%) | ||
| Patients | ||||
| Females (N, %) | 45 (90.0%) | 48 (96.0%) | χ2 (1) = 1.382 | 0.240 |
| Age (mean, SD) | 14.66 (1.91) | 15.12 (1.80) | t(98) = 1.238 | 0.219 |
| Eating disorder diagnosis | ||||
| Anorexia nervosa—restrictive type (N, %) | 45 (90.0%) | 45 (90.0%) | χ2 (2) = 0.000 | 1.000 |
| Anorexia nervosa—binge/purging type (N, %) | 4 (8.0%) | 4 (8.0%) | ||
| Atypical anorexia nervosa (N, %) | 1 (2.0%) | 1 (2.0%) | ||
| Eating disorder duration in months (mean, SD) | 10.41 (7.10) | 16.03 (16.03) | t(87) = 2.076 | 0.041 |
| Type of treatment | ||||
| Inpatient (N, %) | 24 (48.0%) | 24 (48.0%) | χ2 (1) = 0.000 | 1.000 |
| Outpatients (N, %) | 26 (52.0%) | 26 (52.0%) | ||
| BMI at baseline (Mean, SD) | 15.53 (2.13) | 16.36 (2.54) | t(96) = 1.743 | 0.084 |
| Mean (SD) | ANOVA (F, p) | Cohen’s d (95% CI Lower; Upper) | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline (T0) | 3M FU (T1) | 12M FU (T2) | Group | Time | Time × Group | T0-T1 | T0-T2 | |
| GHQ Total Score a | ||||||||
| SUCCEAT Workshop | 4.41 (3.15) | 1.84 (2.74) | 1.94 (1.39) | 0.065 (0.800) | 36.252 (<0.001) | 0.752 (0.473) | 0.87 (0.48; 1.26) | 0.81 (0.42; 1.21) |
| SUCCEAT Online | 4.33 (3.76) | 2.14 (2.92) | 1.39 (2.18) | 0.65 (0.31; 0.98) | 0.98 (0.50; 1.39) | |||
| EDSIS Total Score | ||||||||
| SUCCEAT Workshop | 33.32 (15.02) | 22.59 (13.24) | 20.28 (16.29) | 2.421 (0.123) | 57.005 (<0.001) | 0.166 (0.847) | 0.75 (0.50; 1.00) | 0.83 (0.54; 1.12) |
| SUCCEAT Online | 29.11 (12.70) | 19.83 (11.82) | 16.60 (11.41) | 0.76 (0.42; 1.09) | 1.04 (0.60; 1.47) | |||
| EDSIS Nutrition b | ||||||||
| SUCCEAT Workshop | 16.61 (7.34) | 10.09 (5.78) | 8.09 (6.28) | 1.983 (0.162) | 99.430 (<0.001) | 0.747 (0.475) | 0.96 (0.69; 1.22) | 1.24 (0.91; 1.56) |
| SUCCEAT Online | 14.38 (6.31) | 8.83 (5.83) | 7.24 (5.03) | 0.91 (0.58; 1.24) | 1.24 (0.80; 1.69) | |||
| EDSIS Guilt b | ||||||||
| SUCCEAT Workshop | 7.80 (4.75) | 5.52 (3.96) | 5.17 (4.75) | 1.547 (0.217) | 19.856 (<0.001) | 0.534 (0.587) | 0.52 (0.22; 0.81) | 0.55 (0.26; 0.85) |
| SUCCEAT Online | 6.51 (4.23) | 5.06 (3.52) | 4.33 (3.63) | 0.37 (0.08; 0.66) | 0.55 (0.19; 0.91) | |||
| EDSIS Dysregulated Behavior b | ||||||||
| SUCCEAT Workshop | 6.02 (4.96) | 4.51 (4.21) | 4.53 (4.29) | 0.167 (0.683) | 9.651 (<0.001) | 0.197 (0.821) | 0.32 (0.12; 0.52) | 0.32 (0.05; 0.59) |
| SUCCEAT Online | 5.64 (3.93) | 4.50 (3.36) | 4.07 (3.74) | 0.31 (0.03; 0.59) | 0.41 (0.08; 0.74) | |||
| EDSIS Social Isolation b | ||||||||
| SUCCEAT Workshop | 2.87 (2.60) | 2.48 (2.72) | 2.49 (3.17) | 5.971 (0.016) | 7.190 (0.001) | 2.698 (0.070) | 0.14 (−0.16; 0.45) | 0.12 (−0,19; 0.45) |
| SUCCEAT Online | 2.64 (2.82) | 1.43 (1.95) | 0.96 (1.50) | 0.50 (0.12; 0.87) | 0.73 (0.31; 1.15) | |||
| SCL 90-R Total Mean Score | ||||||||
| SUCCEAT Workshop | 0.42 (0.36) | 0.24 (0.26) | 0.33 (0.37) | 0.003 (0.953) | 12.864 (<0.001) | 2.261 (0.107) | 0.53 (0.32; 0.75) | 0.25 (−0.02; 0.54) |
| SUCCEAT Online | 0.43 (0.42) | 0.31 (0.36) | 0.26 (0.26) | 0.29 (0.03; 0.54) | 0.45 (0.12; 0.78) | |||
| BDI Total Score | ||||||||
| SUCCEAT Workshop | 11.60 (7.01) | 6.45 (5.43) | 6.80 (6.24) | 0.155 (0.694) | 25.946 (<0.001) | 2.394 (0.094) | 0.80 (0.52; 1.08) | 0.72 (0.33; 1.12) |
| SUCCEAT Online | 10.11 (7.03) | 7.72 (8.18) | 5.74 (5.97) | 0.31 (0.04; 0.58) | 0.67 (0.30; 1.03) | |||
| STAI State Score c | ||||||||
| SUCCEAT Workshop | 49.44 (10.14) | 39.80 (10.16) | 37.85 (10.31) | 0.060 (0.807) | 42.972 (<0.001) | 3.312 (0.039) | 0.95 (0.57; 1.33) | 1.13 (0.73; 1.54) |
| SUCCEAT Online | 45.98 (11.16) | 41.84 (12.17) | 37.99 (10.31) | 0.35 (0.06; 0.65) | 0.74 (0.40; 1.08) | |||
| STAI Trait Score c | ||||||||
| SUCCEAT Workshop | 41.73 (8.61) | 37.86 (8.62) | 36.16 (9.65) | <0.001 (0.987) | 22.651 (<0.001) | 0.169 (0.845) | 0.45 (0.22; 0.68) | 0.61 (0.29; 0.92) |
| SUCCEAT Online | 41.25 (10.15) | 38.01 (10.57) | 36.56 (9.50) | 0.31 (0.10; 0.52) | 0.48 (0.20; 0.75) | |||
| Mean (SD) | ANOVA (F, p) | Cohen’s d (95% CI Lower; Upper) | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline (T0) | 3M FU (T1) | 12M FU (T2) | Group | Time | Time × Group | T0–T1 | T0–T2 | |
| CASK Total Score | ||||||||
| SUCCEAT Workshop | 64.64 (15.34) | 75.33 (13.68) | 79.53 (15.25) | 0.202 (0.654) | 51.351 (<0.001) | 0.636 (0.530) | 0.73 (0.40; 1.05) | 0.97 (0.56; 1.38) |
| SUCCEAT Online | 65.20 (13.74) | 74.08 (12.63) | 77.01 (12.87) | 0.67 (0.35; 0.99) | 0.89 (0.55; 1.22) | |||
| CASK Bigger Picture a | ||||||||
| SUCCEAT Workshop | 71.01 (17.63) | 79.14 (13.68) | 83.98 (15.38) | 0.530 (0.468) | 23.631 (<0.001) | 1.420 (0.244) | 0.51 (0.19; 0.83) | 0.78 (0.36; 1.21) |
| SUCCEAT Online | 71.27 (14.22) | 78.60 (12.54) | 79.28 (13.80) | 0.54 (0.21; 0.88) | 0.57 (0.24; 0.90) | |||
| CASK Selfcare a | ||||||||
| SUCCEAT Workshop | 57.23 (18.00) | 71.23 (17.00) | 76.37 (20.19) | 0.222 (0.638) | 59.621 (<0.001) | 0.012 (0.988) | 0.80 (0.44; 1.16) | 1.00 (0.60; 1.39) |
| SUCCEAT Online | 58.33 (19.05) | 72.86 (14.69) | 77.57 (15.28) | 0.84 (0.53; 1.14) | 1.11 (0.70; 1.52) | |||
| CASK Biting Tongue a | ||||||||
| SUCCEAT Workshop | 53.73 (20.44) | 72.20 (17.13) | 78.40 (19.11) | 0.178 (0.674) | 90.700 (<0.001) | 0.465 (0.629) | 0.97 (0.64; 1.30) | 1.25 (0.84; 1.64) |
| SUCCEAT Online | 57.03 (22.07) | 72.56 (16.78) | 78.69 (15.78) | 0.78 (0.46; 1.10) | 1.10 (0.74; 1.45) | |||
| CASK Insight and Acceptance a | ||||||||
| SUCCEAT Workshop | 68.67 (20.27) | 77.94 (17.99) | 82.11 (18.29) | 0.005 (0.944) | 32.987 (<0.001) | <0.001 (1.000) | 0.48 (0.23; 0.74) | 0.69 (0.39; 1.00) |
| SUCCEAT Online | 68.50 (19.23) | 77.76 (14.57) | 81.85 (13.21) | 0.54 (0.21; 0.86) | 0.79 (0.43; 1.16) | |||
| CASK Emotional Intelligence a | ||||||||
| SUCCEAT Workshop | 66.10 (19.03) | 74.54 (16.66) | 75.40 (17.07) | 2.652 (0.107) | 6.804 (0.001) | 1.606 (0.203) | 0.47 (0.15; 0.80) | 0.51 (0.13; 0.90) |
| SUCCEAT Online | 65.36 (17.64) | 67.59 (18.50) | 69.20 (18.59) | 0.12 (−0.18; 0.42) | 0.21 (−0.10; 0.52) | |||
| CASK Frustration Tolerance a | ||||||||
| SUCCEAT Workshop | 64.45 (16.40) | 73.85 (15.02) | 78.13 (15.36) | 0.045 (0.833) | 37.927 (<0.001) | 0.347 (0.707) | 0.60 (0.26; 0.93) | 0.93 (0.51; 1.35) |
| SUCCEAT Online | 64.88 (16.36) | 73.90 (14.31) | 75.84 (13.87) | 0.58 (0.26; 0.91) | 0.81 (0.44; 1.19) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Truttmann, S.; Philipp, J.; Zeiler, M.; Franta, C.; Wittek, T.; Merl, E.; Schöfbeck, G.; Koubek, D.; Laczkovics, C.; Imgart, H.; et al. Long-Term Efficacy of the Workshop Vs. Online SUCCEAT (Supporting Carers of Children and Adolescents with Eating Disorders) Intervention for Parents: A Quasi-Randomised Feasibility Trial. J. Clin. Med. 2020, 9, 1912. https://doi.org/10.3390/jcm9061912
Truttmann S, Philipp J, Zeiler M, Franta C, Wittek T, Merl E, Schöfbeck G, Koubek D, Laczkovics C, Imgart H, et al. Long-Term Efficacy of the Workshop Vs. Online SUCCEAT (Supporting Carers of Children and Adolescents with Eating Disorders) Intervention for Parents: A Quasi-Randomised Feasibility Trial. Journal of Clinical Medicine. 2020; 9(6):1912. https://doi.org/10.3390/jcm9061912
Chicago/Turabian StyleTruttmann, Stefanie, Julia Philipp, Michael Zeiler, Claudia Franta, Tanja Wittek, Elisabeth Merl, Gabriele Schöfbeck, Doris Koubek, Clarissa Laczkovics, Hartmut Imgart, and et al. 2020. "Long-Term Efficacy of the Workshop Vs. Online SUCCEAT (Supporting Carers of Children and Adolescents with Eating Disorders) Intervention for Parents: A Quasi-Randomised Feasibility Trial" Journal of Clinical Medicine 9, no. 6: 1912. https://doi.org/10.3390/jcm9061912
APA StyleTruttmann, S., Philipp, J., Zeiler, M., Franta, C., Wittek, T., Merl, E., Schöfbeck, G., Koubek, D., Laczkovics, C., Imgart, H., Zanko, A., Auer-Welsbach, E., Treasure, J., Karwautz, A. F. K., & Wagner, G. (2020). Long-Term Efficacy of the Workshop Vs. Online SUCCEAT (Supporting Carers of Children and Adolescents with Eating Disorders) Intervention for Parents: A Quasi-Randomised Feasibility Trial. Journal of Clinical Medicine, 9(6), 1912. https://doi.org/10.3390/jcm9061912