Impulsivity, Emotional Dysregulation and Executive Function Deficits Could Be Associated with Alcohol and Drug Abuse in Eating Disorders

 , ,
, ,  , , ,
, , ,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure and Assessment
2.2.1. Psychopathological/Personality Measures
2.2.2. Neuropsychological Measures
2.3. Statistical Analyses
3. Results
3.1. Characteristics of the Sample
3.2. Prevalence of A/DA in ED Patients
3.3. Comparison of the Clinical and Neuropsychological Profile of Patients with and without A/DA
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Bahji, A.; Mazhar, M.N.; Hudson, C.C.; Nadkarni, P.; MacNeil, B.A.; Hawken, E. Prevalence of substance use disorder comorbidity among individuals with eating disorders: A systematic review and meta-analysis. Psychiatry Res. 2019, 273, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.I.; Hiripi, E.; Pope, H.G.; Kessler, R.C. The Prevalence and Correlates of Eating Disorders in the National Comorbidity Survey Replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Fouladi, F.; Mitchell, J.E.; Crosby, R.D.; Engel, S.G.; Crow, S.; Hill, L.; Le Grange, D.; Powers, P.; Steffen, K.J. Prevalence of Alcohol and Other Substance Use in Patients with Eating Disorders. Eur. Eat. Disord. Rev. 2015, 23, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Dennis, A.B.; Pryor, T. The Complex Relationship between Eating Disorders and Substance Use Disorders. In Clinical Handbook of Complex and Atypical Eating Disorders; Anderson, L.K., Murray, S.B., Kaye, W.H., Eds.; Oxford University Press: New York, NY, USA, 2017; pp. 60–78. [Google Scholar]
- Harrop, E.N.; Marlatt, G.A. The comorbidity of substance use disorders and eating disorders in women: Prevalence, etiology, and treatment. Addict. Behav. 2010, 35, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Munn-Chernoff, M.A.; Baker, J.H. A Primer on the Genetics of Comorbid Eating Disorders and Substance Use Disorders. Eur. Eat. Disord. Rev. 2016, 24, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Munn-Chernoff, M.A.; Johnson, E.C.; Chou, Y.L.; Coleman, J.R.I.; Thornton, L.M.; Walters, R.K.; Yilmaz, Z.; Baker, J.H.; Hübel, C.; Gordon, S.; et al. Shared genetic risk between eating disorder- and substance-use-related phenotypes: Evidence from genome-wide association studies. Addict. Biol. 2020. [Google Scholar] [CrossRef]
- Krug, I.; Pinheiro, A.P.; Bulik, C.; Jiménez-Murcia, S.; Granero, R.; Penelo, E.; Masuet, C.; Agüera, Z.; Fernández-Aranda, F. Lifetime substance abuse, family history of alcohol abuse/dependence and novelty seeking in eating disorders: Comparison study of eating disorder subgroups. Psychiatry Clin. Neurosci. 2009, 63, 82–87. [Google Scholar] [CrossRef]
- Fernández-Mondragón, S.; Adan, A. Personality in male patients with substance use disorder and/or severe mental illness. Psychiatry Res. 2015, 228, 488–494. [Google Scholar] [CrossRef]
- Wingo, T.; Nesil, T.; Choi, J.S.; Li, M.D. Novelty Seeking and Drug Addiction in Humans and Animals: From Behavior to Molecules. J. Neuroimmune Pharmcol. 2016, 11, 456–470. [Google Scholar] [CrossRef]
- Lilenfeld, L.R.; Kaye, W.H.; Greeno, C.G.; Merikangas, K.R.; Plotnicov, K.; Pollice, C.; Rao, R.; Strober, M.; Bulik, C.M.; Nagy, L. Psychiatric disorders in women with bulimia nervosa and their first-degree relatives: Effects of comorbid substance dependence. Int. J. Eat. Disord. 1997, 22, 253–264. [Google Scholar] [CrossRef]
- Sloan, E.; Hall, K.; Moulding, R.; Bryce, S.; Mildred, H.; Staiger, P.K. Emotion regulation as a transdiagnostic treatment construct across anxiety, depression, substance, eating and borderline personality disorders: A systematic review. Clin. Psychol. Rev. 2017, 57, 141–163. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S. Specificity of cognitive emotion regulation strategies: A transdiagnostic examination. Behav. Res. Ther. 2010, 48, 974–983. [Google Scholar] [CrossRef]
- Wu, M.; Hartmann, M.; Skunde, M.; Herzog, W.; Friederich, H.-C. Inhibitory Control in Bulimic-Type Eating Disorders: A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e83412. [Google Scholar] [CrossRef]
- Lavagnino, L.; Arnone, D.; Cao, B.; Soares, J.C.; Selvaraj, S. Inhibitory control in obesity and binge eating disorder: A systematic review and meta-analysis of neurocognitive and neuroimaging studies. Neurosci. Biobehav. Rev. 2016, 68, 714–726. [Google Scholar] [CrossRef]
- Roberts, M.E.; Tchanturia, K.; Treasure, J.L. Overlapping neurocognitive inefficiencies in anorexia nervosa: A preliminary investigation of women with both poor set-shifting and weak central coherence. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2016, 21, 725–729. [Google Scholar] [CrossRef][Green Version]
- Aloi, M.; Rania, M.; Caroleo, M.; Bruni, A.; Palmieri, A.; Cauteruccio, M.A.; De Fazio, P.; Segura-García, C. Decision making, central coherence and set-shifting: A comparison between Binge Eating Disorder, Anorexia Nervosa and Healthy Controls. BMC Psychiatry 2015, 15, 1–10. [Google Scholar] [CrossRef]
- Fagundo, A.B.; de la Torre, R.; Jiménez-Murcia, S.; Agüera, Z.; Granero, R.; Tárrega, S.; Botella, C.; Baños, R.; Fernández-Real, J.M.; Rodríguez, R.; et al. Executive Functions Profile in Extreme Eating/Weight Conditions: From Anorexia Nervosa to Obesity. PLoS ONE 2012, 7, e43382. [Google Scholar] [CrossRef]
- Guillaume, S.; Gorwood, P.; Jollant, F.; Van den Eynde, F.; Courtet, P.; Richard-Devantoy, S. Impaired decision-making in symptomatic anorexia and bulimia nervosa patients: A meta-analysis. Psychol. Med. 2015, 45, 3377–3391. [Google Scholar] [CrossRef]
- Luijten, M.; Machielsen, M.W.J.; Veltman, D.J.; Hester, R.; de Haan, L.; Franken, I.H.A. Systematic review of ERP and fMRI studies investigating inhibitory control and error processing in people with substance dependence and behavioural addictions. J. Psychiatry Neurosci. 2014, 39, 149–169. [Google Scholar] [CrossRef]
- Allen, D.N.; Woods, S.P. Neuropsychological Aspects of Substance Use Disorders: Evidence-Based Perspectives; Oxford University Press: New York, NY, USA, 2014; ISBN 9780199930838. [Google Scholar]
- Ersche, K.D.; Turton, A.J.; Chamberlain, S.R.; Müller, U.; Bullmore, E.T.; Robbins, T.W. Cognitive dysfunction and anxious-impulsive personality traits are endophenotypes for drug dependence. Am. J. Psychiatry 2012, 169, 926–936. [Google Scholar] [CrossRef]
- Fernández-Serrano, M.J.; Pérez-García, M.; Verdejo-García, A. What are the specific vs. generalized effects of drugs of abuse on neuropsychological performance? Neurosci. Biobehav. Rev. 2011, 35, 377–406. [Google Scholar] [CrossRef]
- Henry, B.L.; Minassian, A.; Perry, W. Effect of methamphetamine dependence on everyday functional ability. Addict. Behav. 2010, 35, 593–598. [Google Scholar] [CrossRef]
- Ersche, K.D.; Sahakian, B.J. The neuropsychology of amphetamine and opiate dependence: Implications for treatment. Neuropsychol. Rev. 2007, 17, 317–336. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Serrano, M.J.; Perales, J.C.; Moreno-López, L.; Pérez-García, M.; Verdejo-García, A. Neuropsychological profiling of impulsivity and compulsivity in cocaine dependent individuals. Psychopharmacology 2012, 219, 673–683. [Google Scholar] [CrossRef]
- Lezak, M.D.; Howieson, D.B.; Bigler, E.D.; Tranel, D. Neuropsychological Assessment, 5th ed.; Oxford University Press: New York, NY, USA, 2012; ISBN 9780195395525. [Google Scholar]
- First, M.; Williams, J.; Karg, R.; Spitzer, R. Structured Clinical Interview for DSM-5 Disorders, Clinician Version (SCID-5-CV); American Psychiatric Association: Arlington, VA, USA, 2016. [Google Scholar]
- Cloninger, C.R.; Przybeck, T.R.; Svrakic, D.M.; Wetzel, R.D. The Temperament and Character Inventory (TCI): A Guide to Its Development and Use; Center for Psychobiology of Personality, Washington University: St. Louis, MO, USA, 1994; ISBN 0-9642917-03. [Google Scholar]
- Gutiérrez-Zotes, J.A.; Bayón, C.; Montserrat, C.; Valero, J.; Labad, A.; Cloninger, C.; Fernández-Aranda, F. Temperament and Character Inventory-Revised (TCI-R). Standardization and normative data in a general population sample. Actas Esp Psiquiatr 2004, 32, 8–15. [Google Scholar]
- Derogatis, L.R. Symptom Checklist-90-R (SCL-90-R): Administration, scoring, and procedures manual, 3rd ed.; NCS Pearson: Minneapolis, MN, USA, 1994; ISBN 2090-6684 (Print) 2090-6692. [Google Scholar]
- González de Rivera, J.L.; de las Cuevas, C.; Rodríguez-Abuín, M.; y Rodríguez-Pulido, F. SCL-90-R. Cuestionario de 90 Síntomas. Manual; TEA Ediciones: Madrid, Spain, 2002. [Google Scholar]
- Garner, D.M. Eating Disorder Inventory-2; Psychological Assessment Resources: Odessa, Ukraine, 1991. [Google Scholar]
- Garner, D.M. Inventario de Trastornos de la Conducta Alimentaria (EDI-2)-Manual; TEA: Madrid, Spain, 1998.
- Golden, C.J. Stroop colour and word test. Age 1978, 15, 90. [Google Scholar]
- Golden, C.J. Stroop: Test de Colores y Palabras: Manual; TEA Ediciones: Madrid, Spain, 2001. [Google Scholar]
- Heaton, R.K. PAR Staff Wisconsin Card Sorting TestTM: Computer Version 4, Research Edition; Psychological Assessment Resources: Lutz, FL, USA, 2003. [Google Scholar]
- Bechara, A.; Damasio, A.R.; Damasio, H.; Anderson, S.W. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 1994, 50, 7–15. [Google Scholar] [CrossRef]
- Eisinger, A.; Magi, A.; Gyurkovics, M.; Szabo, E.; Demetrovics, Z.; Kokonyei, G. Iowa Gambling Task: Illustration of a behavioral measurement. Neuropsychopharmacol. Hung. 2016, 18, 45–55. [Google Scholar]
- StataCorp Stata Statistical Software: Release 16; StataCorp LLC.: College Station, TX, USA, 2019.
- Kelley, K.; Preacher, K.J. On effect size. Psychol. Methods 2012, 17, 137–152. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for Behavioural Sciences; Lawrence Earlbaum Associates: Hillsdale, NJ, USA, 1998; ISBN 0805802835. [Google Scholar]
- Finner, H. On a Monotonicity Problem in Step-Down Multiple Test Procedures. J. Am. Stat. Assoc. 1993, 88, 920. [Google Scholar] [CrossRef]
- Root, T.L.; Pinheiro, A.P.; Thornton, L.; Strober, M.; Fernandez-Aranda, F.; Brandt, H.; Crawford, S.; Fichter, M.M.; Halmi, K.A.; Johnson, C.; et al. Substance use disorders in women with anorexia nervosa. Int. J. Eat. Disord. 2010, 43, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Bongers, P.; Jansen, A.; Houben, K.; Roefs, A. Happy eating: The single target implicit association test predicts overeating after positive emotions. Eat. Behav. 2013, 14, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Leehr, E.J.; Krohmer, K.; Schag, K.; Dresler, T.; Zipfel, S.; Giel, K.E. Emotion regulation model in binge eating disorder and obesity-a systematic review. Neurosci. Biobehav. Rev. 2015, 49, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Fassino, S.; Pierò, A.; Gramaglia, C.; Abbate-Daga, G. Clinical, psychopathological and personality correlates of interoceptive awareness in anorexia nervosa, bulimia nervosa and obesity. Psychopathology 2004, 37, 168–174. [Google Scholar] [CrossRef]
- Hasin, D.; Katz, H. Somatoform and substance use disorders. Psychosom. Med. 2007, 69, 870–875. [Google Scholar] [CrossRef]
- Kanner, R. Substance Abuse, Somatization, and Personality Disorders. In Emergency Neurology; Roos, K.L., Ed.; Elseiver: Boston, MA, USA, 2012; pp. 375–384. ISBN 9780387885858. [Google Scholar]
- Fernández-Aranda, F.; Jiménez-Murcia, S.; Álvarez-Moya, E.M.; Granero, R.; Vallejo, J.; Bulik, C.M. Impulse control disorders in eating disorders: Clinical and therapeutic implications. Compr. Psychiatry 2006, 47, 482–488. [Google Scholar] [CrossRef]
- Jiménez-Murcia, S.; Granero, R.; Moragas, L.; Steiger, H.; Israel, M.; Aymamí, N.; Gómez-Peña, M.; Sauchelli, S.; Agüera, Z.; Sánchez, I.; et al. Differences and similarities between bulimia nervosa, compulsive buying and gambling disorder. Eur. Eat. Disord. Rev. 2015, 23, 126–132. [Google Scholar] [CrossRef]
- Grant, J.E. Impulse control disorders, a clinician’s guide to understanding and treating behavi oral addictions. Psicoter. Cogn. E Comport. 2011, 17, 130–131. [Google Scholar] [CrossRef]
- Schreiber, L.; Odlaug, B.L.; Grant, J.E. Impulse control disorders: Updated review of clinical characteristics and pharmacological management. Front. Psychiatry 2011, 2. [Google Scholar] [CrossRef]
- Schag, K.; Schönleber, J.; Teufel, M.; Zipfel, S.; Giel, K.E. Food-related impulsivity in obesity and Binge Eating Disorder-a systematic review. Obes. Rev. 2013, 14, 477–495. [Google Scholar] [CrossRef]
- Wrege, J.; Schmidt, A.; Walter, A.; Smieskova, R.; Bendfeldt, K.; Radue, E.-W.; Lang, U.; Borgwardt, S. Effects of Cannabis on Impulsivity: A Systematic Review of Neuroimaging Findings. Curr. Pharm. Des. 2014, 20, 2126–2137. [Google Scholar] [CrossRef] [PubMed]
- Verdejo-Garcia, A.; Benbrook, A.; Funderburk, F.; David, P.; Cadet, J.L.; Bolla, K.I. The differential relationship between cocaine use and marijuana use on decision-making performance over repeat testing with the Iowa Gambling Task. Drug Alcohol Depend. 2007, 90, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Bechara, A.; Tranel, D.; Damasio, H. Characterization of the decision-making deficit of patients with ventromedial prefrontal cortex lesions. Brain 2000, 123, 2189–2202. [Google Scholar] [CrossRef] [PubMed]
- Bechara, A.; Damasio, H.; Damasio, A.R.; Lee, G.P. Different contributions of the human amygdala and ventromedial prefrontal cortex to decision-making. J. Neurosci. 1999, 19, 5473–5481. [Google Scholar] [CrossRef] [PubMed]
- Turton, R.; Nazar, B.P.; Burgess, E.E.; Lawrence, N.S.; Cardi, V.; Treasure, J.; Hirsch, C.R. To Go or Not to Go: A Proof of Concept Study Testing Food-Specific Inhibition Training for Women with Eating and Weight Disorders. Eur. Eat. Disord. Rev. 2018, 26, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Claudat, K.; Brown, T.A.; Anderson, L.; Bongiorno, G.; Berner, L.A.; Reilly, E.; Luo, T.; Orloff, N.; Kaye, W.H. Correlates of co-occurring eating disorders and substance use disorders: A case for dialectical behavior therapy. Eat. Disord. 2020, 28, 142–156. [Google Scholar] [CrossRef]
- Hagan, K.E.; Christensen, K.A.; Forbush, K.T. A preliminary systematic review and meta-analysis of randomized-controlled trials of cognitive remediation therapy for anorexia nervosa. Eat. Behav. 2020, 37. [Google Scholar] [CrossRef]


{kind=link}
| Without A/DA | With A/DA | p | ||||
|---|---|---|---|---|---|---|
| n = 118 | n = 27 | |||||
| n | % | n | % | |||
| Sex | Women | 88 | 74.6% | 20 | 74.1% | 0.957 |
| Men | 30 | 25.4% | 7 | 25.9% | ||
| ED subtype | Anorexia restrictive | 49 | 41.5% | 8 | 29.6% | 0.751 |
| Anorexia binge/purge | 20 | 16.9% | 6 | 22.2% | ||
| Bulimia | 21 | 17.8% | 7 | 25.9% | ||
| Binge eating disorder | 18 | 15.3% | 4 | 14.8% | ||
| Other specified feeding eating dis. | 10 | 8.5% | 2 | 7.4% | ||
| Education | Primary | 30 | 25.4% | 10 | 37.0% | 0.438 |
| Secondary | 52 | 44.1% | 11 | 40.7% | ||
| University | 36 | 30.5% | 6 | 22.2% | ||
| Mean | SD | Mean | SD | p | ||
| Age (years-old) | 30.30 | 10.13 | 30.56 | 11.22 | 0.907 | |
| Onset of the ED (years-old) | 22.94 | 8.99 | 21.59 | 9.83 | 0.491 | |
| Duration of the ED (years) | 7.36 | 7.58 | 8.96 | 6.72 | 0.312 | |
| BMI (kg/m2) | 21.70 | 8.47 | 22.50 | 8.87 | 0.663 | |
| Other impulsive behaviours | n | % | n | % | p | |
| Binges episodes | 46 | 39.3% | 16 | 59.3% | 0.049 * | |
| Theft | 18 | 15.3% | 9 | 33.3% | 0.029 * | |
| Kleptomania | 2 | 1.7% | 3 | 11.1% | 0.045 * | |
| Compulsive buying | 10 | 8.5% | 6 | 22.2% | 0.040 * | |
| Total | AN-R | AN-BP | BN | BED | OSFED | Women | Men | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 145 | n = 57 | n = 26 | n = 28 | n = 22 | n = 12 | n = 108 | n = 37 | ||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % |
| 27 | 18.6% | 8 | 14.0% | 6 | 23.1% | 7 | 25.0% | 4 | 18.2% | 2 | 16.7% | 20 | 18.5% | 7 | 18.9% |
| χ2 | 1.92 | (df = 4) | 0.01 | (df = 1) | |||||||||||
| p | 0.751 | 0.957 | |||||||||||||
| α | Without A/DA | With A/DA | p | |d| | η2 | Power | |||
|---|---|---|---|---|---|---|---|---|---|
| n = 118 | n = 27 | ||||||||
| Mean | SD | Mean | SD | ||||||
| EDI Drive for thinness | 0.846 | 11.24 | 6.65 | 12.10 | 6.50 | 0.544 | 0.13 | 0.003 | 0.093 |
| EDI Body dissatisfaction | 0.922 | 13.35 | 8.86 | 15.66 | 7.70 | 0.213 | 0.28 | 0.011 | 0.237 |
| EDI Interoceptive awareness | 0.868 | 8.98 | 7.13 | 12.10 | 5.95 | 0.036 * | 0.52 † | 0.030 | 0.556 |
| EDI Bulimia | 0.791 | 4.92 | 5.20 | 6.51 | 4.83 | 0.148 | 0.32 | 0.015 | 0.303 |
| EDI Interpersonal distrust | 0.824 | 5.59 | 4.84 | 5.92 | 4.47 | 0.752 | 0.07 | 0.001 | 0.061 |
| EDI Ineffectiveness | 0.905 | 8.61 | 6.89 | 10.78 | 6.91 | 0.142 | 0.32 | 0.015 | 0.312 |
| EDI Maturity fears | 0.841 | 7.54 | 5.08 | 7.58 | 5.89 | 0.975 | 0.01 | 0.001 | 0.050 |
| EDI Perfectionism | 0.842 | 5.31 | 4.40 | 5.16 | 4.54 | 0.878 | 0.03 | 0.001 | 0.053 |
| EDI Impulse regulation | 0.850 | 5.43 | 5.85 | 5.60 | 4.43 | 0.886 | 0.03 | 0.001 | 0.052 |
| EDI Ascetic | 0.703 | 5.99 | 4.37 | 6.92 | 3.76 | 0.307 | 0.23 | 0.007 | 0.175 |
| EDI Social insecurity | 0.825 | 6.37 | 5.17 | 7.28 | 5.72 | 0.417 | 0.17 | 0.005 | 0.127 |
| EDI Total score | 0.974 | 83.33 | 48.73 | 95.62 | 42.19 | 0.228 | 0.27 | 0.010 | 0.225 |
| SCL-90R Somatization | 0.857 | 1.45 | 0.90 | 1.82 | 0.77 | 0.049 * | 0.44 | 0.026 | 0.497 |
| SCL-90-R Obsessive-compulsive | 0.909 | 1.57 | 0.98 | 1.78 | 0.89 | 0.308 | 0.22 | 0.007 | 0.174 |
| SCL-90-R Interpersonal sensitive | 0.912 | 1.76 | 1.04 | 1.94 | 0.91 | 0.416 | 0.18 | 0.005 | 0.128 |
| SCL-90-R Depression | 0.946 | 2.00 | 1.05 | 2.21 | 0.82 | 0.329 | 0.22 | 0.007 | 0.164 |
| SCL-90-R Anxiety | 0.911 | 1.38 | 0.95 | 1.66 | 0.74 | 0.145 | 0.34 | 0.015 | 0.307 |
| SCL-90-R Hostility | 0.774 | 1.17 | 0.88 | 1.25 | 0.97 | 0.672 | 0.09 | 0.001 | 0.071 |
| SCL-90-R Phobic anxiety | 0.854 | 0.78 | 0.87 | 0.86 | 0.73 | 0.667 | 0.10 | 0.001 | 0.072 |
| SCL-90-R Paranoia | 0.875 | 1.27 | 0.89 | 1.32 | 0.81 | 0.821 | 0.05 | 0.001 | 0.056 |
| SCL-90-R Psychotic | 0.893 | 1.17 | 0.77 | 1.28 | 0.67 | 0.529 | 0.14 | 0.003 | 0.096 |
| SCL-90-R GSI | 0.980 | 1.50 | 0.82 | 1.69 | 0.68 | 0.257 | 0.26 | 0.009 | 0.204 |
| SCL-90-R PST | 0.980 | 56.61 | 19.91 | 63.15 | 17.64 | 0.119 | 0.35 | 0.017 | 0.345 |
| SCL-90-R PSDI | 0.980 | 2.20 | 0.66 | 2.32 | 0.42 | 0.383 | 0.21 | 0.005 | 0.140 |
| TCI-R Novelty seeking | 0.797 | 94.68 | 13.80 | 103.37 | 13.83 | 0.004 * | 0.63 † | 0.057 | 0.834 |
| TCI-R Harm avoidance | 0.925 | 112.31 | 20.84 | 116.07 | 21.50 | 0.402 | 0.18 | 0.005 | 0.133 |
| TCI-R Reward dependence | 0.700 | 101.21 | 15.47 | 102.56 | 17.33 | 0.691 | 0.08 | 0.001 | 0.068 |
| TCI-R Persistence | 0.860 | 114.12 | 20.30 | 107.33 | 24.13 | 0.133 | 0.30 | 0.016 | 0.323 |
| TCI-R Self-directedness | 0.908 | 125.72 | 21.84 | 119.33 | 24.19 | 0.181 | 0.28 | 0.012 | 0.266 |
| TCI-R Cooperativeness | 0.831 | 136.66 | 17.28 | 135.89 | 15.97 | 0.832 | 0.05 | 0.001 | 0.055 |
| TCI-R Self-transcendence | 0.893 | 63.16 | 15.28 | 63.37 | 18.91 | 0.951 | 0.01 | 0.001 | 0.050 |
| Without A/DA | With A/DA | p | |d| | η2 | Power | |||
|---|---|---|---|---|---|---|---|---|
| n = 118 | n = 27 | |||||||
| Mean | SD | Mean | SD | |||||
| Stroop Words | 104.43 | 19.39 | 95.61 | 24.53 | 0.045 * | 0.40 | 0.028 | 0.521 |
| Stroop Colour | 75.84 | 16.06 | 80.24 | 19.74 | 0.221 | 0.24 | 0.010 | 0.231 |
| Stroop Words-colour | 48.27 | 11.75 | 46.50 | 9.33 | 0.467 | 0.17 | 0.004 | 0.112 |
| Stroop Interference | 5.09 | 8.99 | 4.42 | 7.92 | 0.725 | 0.08 | 0.001 | 0.064 |
| WCST Total trials | 94.42 | 20.72 | 100.55 | 20.70 | 0.168 | 0.30 | 0.013 | 0.280 |
| WCST Correct | 67.83 | 10.87 | 68.06 | 14.02 | 0.924 | 0.02 | 0.001 | 0.051 |
| WCST Perseverative errors | 12.40 | 10.33 | 18.54 | 19.41 | 0.023 * | 0.39 | 0.036 | 0.629 |
| WCST Non-perseverative errors | 14.20 | 15.25 | 14.22 | 11.91 | 0.993 | 0.01 | 0.001 | 0.050 |
| WCST Conceptual | 60.64 | 16.54 | 59.18 | 19.97 | 0.692 | 0.08 | 0.001 | 0.068 |
| WCST Categories completed | 5.10 | 1.80 | 4.88 | 1.98 | 0.577 | 0.12 | 0.002 | 0.086 |
| WCST Trials completed 1st categ. | 20.36 | 24.17 | 26.73 | 31.78 | 0.248 | 0.23 | 0.009 | 0.210 |
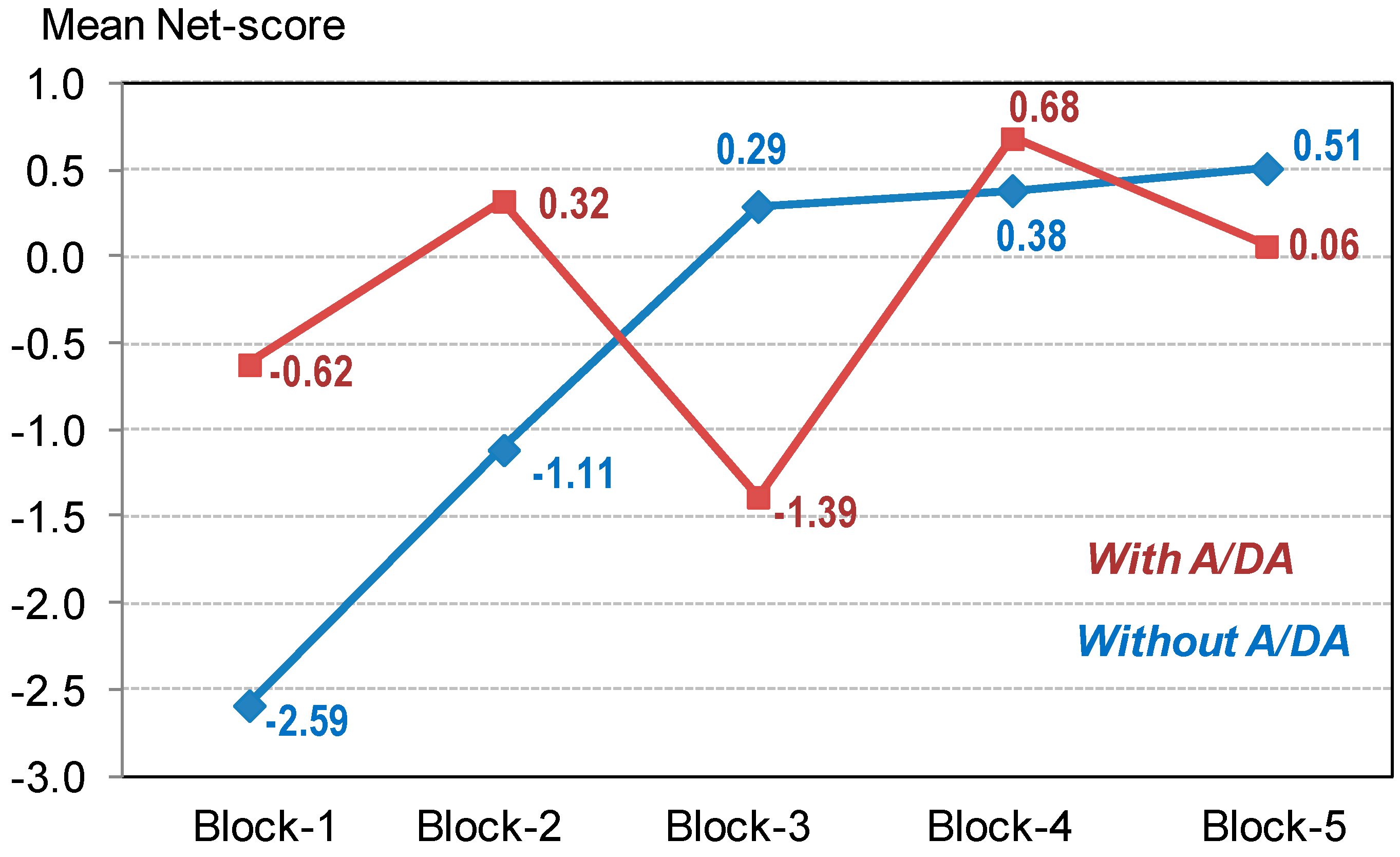
| IGT Block 1 | −2.59 | 4.21 | −0.62 | 2.84 | 0.023 * | 0.55 † | 0.036 | 0.629 |
| IGT Block 2 | −1.11 | 4.91 | 0.32 | 4.41 | 0.165 | 0.31 | 0.013 | 0.284 |
| IGT Block 3 | 0.29 | 5.80 | −1.39 | 3.55 | 0.152 | 0.35 | 0.014 | 0.298 |
| IGT Block 4 | 0.38 | 6.69 | 0.68 | 6.67 | 0.834 | 0.04 | 0.001 | 0.055 |
| IGT Block 5 | 0.51 | 7.78 | 0.06 | 5.42 | 0.777 | 0.07 | 0.001 | 0.059 |
| IGT Total | −2.52 | 20.79 | −0.95 | 11.51 | 0.704 | 0.09 | 0.001 | 0.067 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lozano-Madrid, M.; Clark Bryan, D.; Granero, R.; Sánchez, I.; Riesco, N.; Mallorquí-Bagué, N.; Jiménez-Murcia, S.; Treasure, J.; Fernández-Aranda, F. Impulsivity, Emotional Dysregulation and Executive Function Deficits Could Be Associated with Alcohol and Drug Abuse in Eating Disorders. J. Clin. Med. 2020, 9, 1936. https://doi.org/10.3390/jcm9061936
Lozano-Madrid M, Clark Bryan D, Granero R, Sánchez I, Riesco N, Mallorquí-Bagué N, Jiménez-Murcia S, Treasure J, Fernández-Aranda F. Impulsivity, Emotional Dysregulation and Executive Function Deficits Could Be Associated with Alcohol and Drug Abuse in Eating Disorders. Journal of Clinical Medicine. 2020; 9(6):1936. https://doi.org/10.3390/jcm9061936
Chicago/Turabian StyleLozano-Madrid, María, Danielle Clark Bryan, Roser Granero, Isabel Sánchez, Nadine Riesco, Núria Mallorquí-Bagué, Susana Jiménez-Murcia, Janet Treasure, and Fernando Fernández-Aranda. 2020. "Impulsivity, Emotional Dysregulation and Executive Function Deficits Could Be Associated with Alcohol and Drug Abuse in Eating Disorders" Journal of Clinical Medicine 9, no. 6: 1936. https://doi.org/10.3390/jcm9061936
APA StyleLozano-Madrid, M., Clark Bryan, D., Granero, R., Sánchez, I., Riesco, N., Mallorquí-Bagué, N., Jiménez-Murcia, S., Treasure, J., & Fernández-Aranda, F. (2020). Impulsivity, Emotional Dysregulation and Executive Function Deficits Could Be Associated with Alcohol and Drug Abuse in Eating Disorders. Journal of Clinical Medicine, 9(6), 1936. https://doi.org/10.3390/jcm9061936