Self-Assessment of Competence and Referral Behavior for Musculoskeletal Injections among Dutch General Practitioners


Abstract
1. Introduction
- To what extent do Dutch GPs feel competent in administering musculoskeletal injections?
- How does self-assessed (in)competence affect their clinical treatment and referral behavior?
- Which factors are associated with self-assessed incompetence?
- Which barriers and facilitators to administer musculoskeletal injections do Dutch GPs experience?
2. Methods
2.1. Development of the Questionnaire
2.2. Study Population and Recruitment
2.3. Statistical Analysis
3. Results
3.1. Responses
3.2. Representativeness
3.3. Competence
3.4. Number of Injections
3.4.1. Injections Aministered
3.4.2. Injections Referred to GP Colleague
3.4.3. Injections Referred to Scondary Care
3.5. Injection Indications
3.6. Factors Associated with Incompetence and Referral Behavior
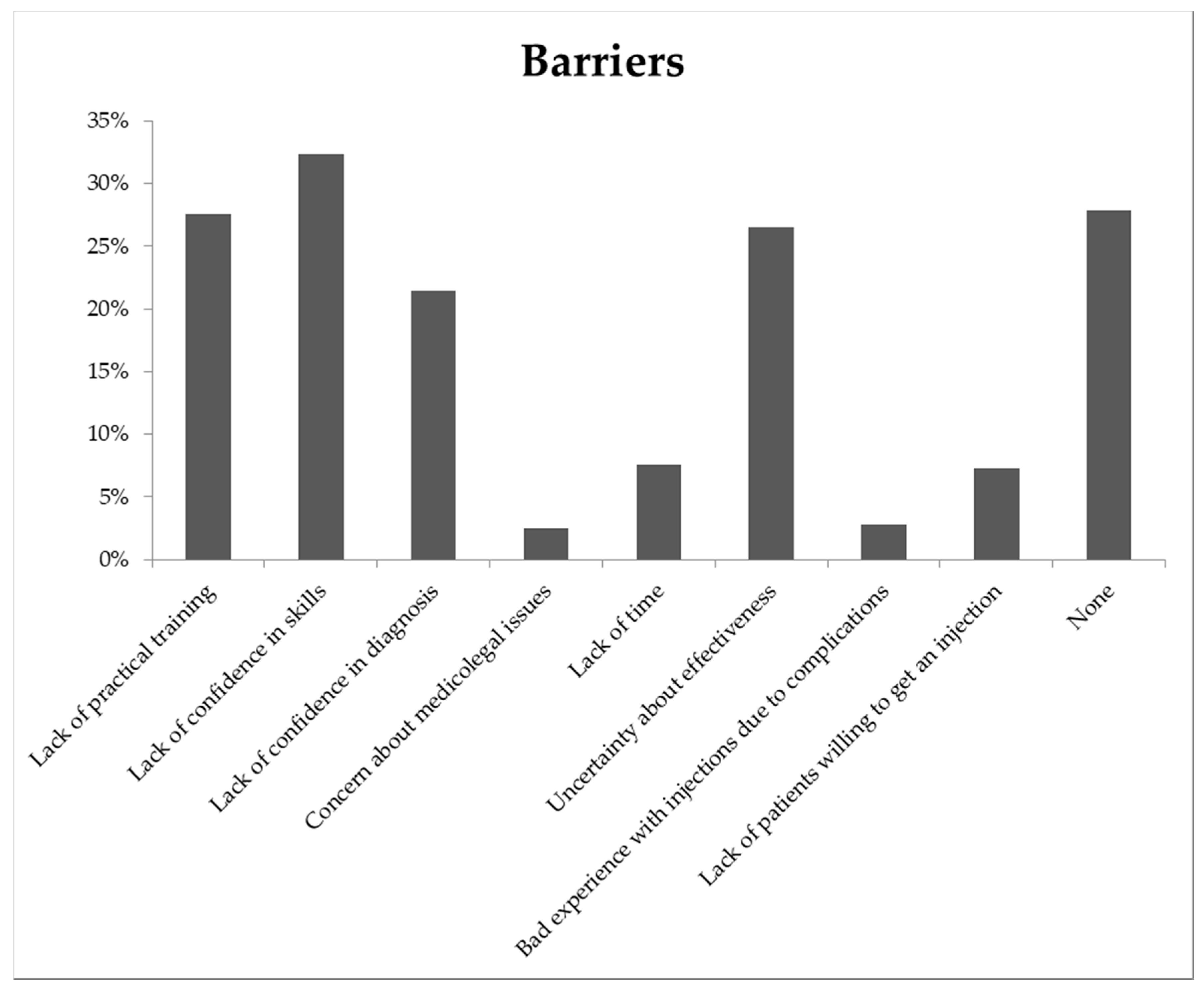
3.7. Barriers
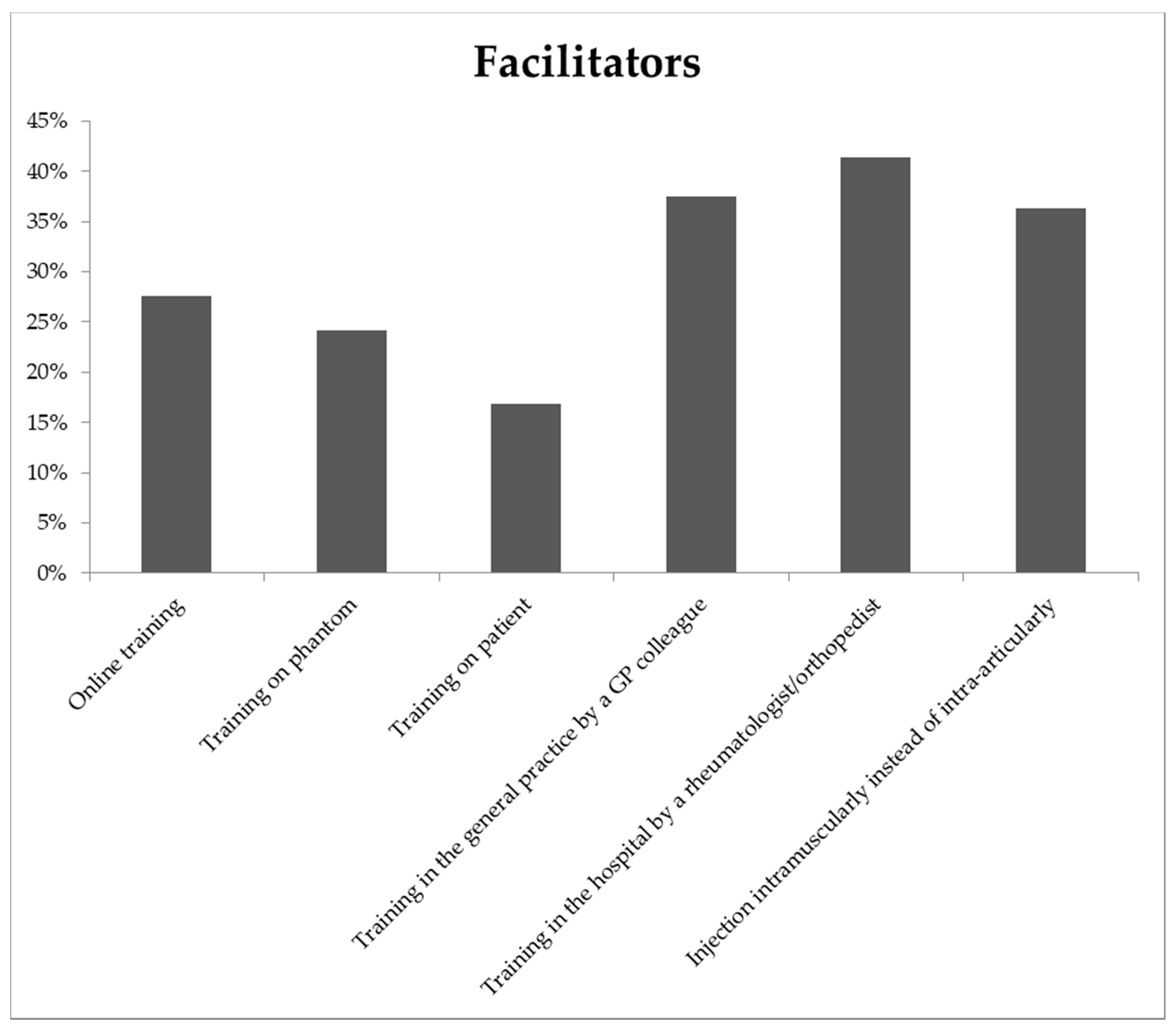
3.8. Facilitators
4. Discussion
4.1. Comparison with Other Studies
4.1.1. Number of Injections
4.1.2. Barriers
4.1.3. Training
4.2. Limitations
4.3. Implications for Practice and Further Research
Author Contributions
Funding
Conflicts of Interest
Appendix A
Questionnaire
- To what extent do you agree with the following statement? (1 answer possible) I consider myself competent in administering musculoskeletal injections.
- □
- completely disagree
- □
- disagree
- □
- neutral
- □
- agree
- □
- completely agree
- Which barriers do you experience in administering musculoskeletal injections? (multiple answers possible)
- □
- Lack of training
- □
- Lack of confidence in skills
- □
- Lack of confidence in diagnosis
- □
- Medical-legal issues
- □
- Lack of time
- □
- Uncertainty about effectiveness of an injection
- □
- Bad experience with injections due to complications
- □
- Lack of patients willing to get an injection
- □
- None
- What would facilitate administering musculoskeletal injections for you? (multiple answers possible)
- □
- Online training
- □
- Training on a phantom
- □
- Training on a patient
- □
- Training in primary care by a GP colleague
- □
- Training in secondary care by a rheumatologists/orthopaedist
- □
- Possibility to perform an intramuscular injection instead of an intra articular injection
- How many musculoskeletal injections did you administer in the past month? (1 answer possible)
- □
- None
- □
- Indicate how many (enter only numbers)
- How many musculoskeletal injections did you refer to a GP colleague in the past month? (1 answer possible)
- □
- None
- □
- Indicate how many (enter only numbers)
- How many musculoskeletal injections did you refer to secondary care (rheumatologist/orthopaedist) in the past month?
- □
- None
- □
- Indicate how many (enter only numbers)
- What is your sex? (1 answer possible)
- □
- Man
- □
- Woman
- □
- Neutral
- What is the organisation of your practice? (1 answer possible)
- □
- Healthcare centre
- □
- Duo practice
- □
- Solo practice
- □
- Group practice
- □
- Other, namely:
- What is the setting of your practice? (1 answer possible)
- □
- Rural
- □
- Urban
- How many FTE (fulltime-equivalent) do you work as a GP? (1 answer possible) (fulltime-equivalent)
- □
- 0–0.20
- □
- 0.21–0.40
- □
- 0.41–0.60
- □
- 0.61–0.80
- □
- 0.81–1
- What is the size of your patient population (standard practice = 2095)? (1 answer possible)
- □
- Smaller than the standard practice
- □
- Equal to the standard practice
- □
- Bigger than the standard practice
- How many years ago did you graduate from the GP training? (1 answer possible)
- □
- < 5 years
- □
- 5–15 years
- □
- 16–25 years
- □
- >25 years
- Are you a GP trainer? (1 answer possible)
- □
- Yes
- □
- No
- Are you a GP specialised in the musculoskeletal system? (1 answer possible)
- □
- Yes
- □
- No
- Finally, for the following indications, please indicate whether you would administer the injection yourself, would refer for the injection to a colleague GP or to secondary care (rheumatologist/orthopaedist), or would not advise an injection/indication did not occur in your practice (multiple answers possible per indication).
| Indication | Self | Colleague GP | Secondary Care | No Injection/Did Not occur |
| Bursitis shoulder | □ | □ | □ | □ |
| Osteoarthritis shoulder | □ | □ | □ | □ |
| Supraspinatus tendinitis | □ | □ | □ | □ |
| Lateral epicondylitis | □ | □ | □ | □ |
| Medial epicondylitis | □ | □ | □ | □ |
| Olecranon bursitis | □ | □ | □ | □ |
| Carpal tunnel syndrome | □ | □ | □ | □ |
| Trigger finger/thumb | □ | □ | □ | □ |
| De Quervain’s tenosynovitis | □ | □ | □ | □ |
| Osteoarthritis MCP/PIP/DIP | □ | □ | □ | □ |
| Osteoarthritis CMC | □ | □ | □ | □ |
| Trochanteric bursitis | □ | □ | □ | □ |
| Sacro-iliitis | □ | □ | □ | □ |
| Knee osteoarthritis | □ | □ | □ | □ |
| Prepatellar bursitis | □ | □ | □ | □ |
| Achilles tendinitis | □ | □ | □ | □ |
| Ankle osteoarthritis | □ | □ | □ | □ |
| Plantar fasciitis | □ | □ | □ | □ |
References
- Meeste Consulten bij Huisarts voor Klachten aan het Bewegingsapparaat. NIVEL Zorgregistraties, infographic. Available online: https://www.nivel.nl/nl/nieuws/nederlanders-vooral-met-beweegklachten-naar-de-huisarts (accessed on 1 September 2019).
- Hermans, J.; Koopmanschap, M.A.; Bierma-Zeinstra, S.M.; van Linge, J.H.; Verhaar, J.A.; Reijman, M.; Burdorf, A. Productivity costs and medical costs among working patients with knee osteoarthritis. Arthritis Care Res. (Hoboken) 2012, 64, 853–861. [Google Scholar] [CrossRef] [PubMed]
- March, L.; Smith, E.U.; Hoy, D.G.; Cross, M.J.; Sanchez-Riera, L.; Blyth, F.; Buchbinder, R.; Vos, T.; Woolf, A.D. Burden of disability due to musculoskeletal (MSK) disorders. Best Pract. Res. Clin. Rheumatol. 2014, 28, 353–366. [Google Scholar] [CrossRef] [PubMed]
- Lubeck, D.P. The costs of musculoskeletal disease: Health needs assessment and health economics. Best Pract. Res. Clin. Rheumatol. 2003, 17, 529–539. [Google Scholar] [CrossRef][Green Version]
- GBD 2016. Analysis of the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar]
- Nederlandse Huisartsen Genootschap (NHG) Richtlijnen. Available online: https://www.nhg.org (accessed on 1 September 2019).
- Curatolo, M.; Bogduk, N. Pharmacologic pain treatment of musculoskeletal disorders: Current perspectives and future prospects. Clin. J. Pain 2001, 17, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Foster, Z.J.; Voss, T.T.; Hatch, J.; Frimodig, A. Corticosteroid Injections for Common Musculoskeletal Conditions. Am. Fam. Physician 2015, 92, 694–699. [Google Scholar]
- Babatunde, O.O.; Jordan, J.L.; Van der Windt, D.A.; Hill, J.C.; Foster, N.E.; Protheroe, J. Effective treatment options for musculoskeletal pain in primary care: A systematic overview of current evidence. PLoS ONE 2017, 12, e0178621. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef]
- National Clinical Guideline Centre (UK). Osteoarthritis: Care and Management in Adults; National Institute for Health and Care Excellence (UK): London, UK, 2014. [Google Scholar]
- Gormley, G.J.; Corrigan, M.; Steele, W.K.; Stevenson, M.; Taggart, A.J. Joint and soft tissue injections in the community: Questionnaire survey of general practitioners’ experiences and attitudes. Ann. Rheum. Dis. 2003, 62, 61–64. [Google Scholar] [CrossRef]
- Liddell, W.G.; Carmichael, C.R.; McHugh, N.J. Joint and soft tissue injections: A survey of general practitioners. Rheumatology (Oxford) 2005, 44, 1043–1046. [Google Scholar] [CrossRef]
- Brown, J.S.; Smith, R.R.; Cantor, T.; Chesover, D.; Yearsley, R. General practitioners as providers of minor surgery--a success story? Br. J. Gen. Pract. 1997, 47, 205–210. [Google Scholar] [PubMed]
- Bruens, M.L.; van der Zaag-Loonen, H.J.; Steenstra, F.; Stemerding, A.M.; Wijngaarden, S. Septic arthritis after intra-articular injection is rare: Does the Taskforce Infection Prevention use a sledgehammer to crack a nut? Ned. Tijdschr. Geneeskd. 2016, 160, D789. [Google Scholar] [PubMed]
- Van der Velden, L.; Kasteleijn, A.; Kenens, R. Cijfers uit de registratie van huisartsen, peiling 2016. Proc. Natl. Acad. Sci. USA 2017. [Google Scholar]
- Bridges, J.S. Sex Differences in Occupational Performance Expectations. Psychol. Women Q. 1988, 12, 75–90. [Google Scholar] [CrossRef]
- Beyer, S. Gender differences in the accuracy of self-evaluations of performance. J. Personal. Soc. Psychol. 1990, 59, 960–970. [Google Scholar] [CrossRef]
- Lind, D.S.; Rekkas, S.; Bui, V.; Lam, T.; Beierle, E.; Copeland, E.M. Competency-based student self-assessment on a surgery rotation. J. Surg. Res. 2002, 105, 31–34. [Google Scholar] [CrossRef]
- Blanch, D.C.; Hall, J.A.; Roter, D.L.; Frankel, R.M. Medical student gender and issues of confidence. Patient Educ. Couns. 2008, 72, 374–381. [Google Scholar] [CrossRef]
- Minter, R.M.; Gruppen, L.D.; Napolitano, K.S.; Gauger, P.G. Gender differences in the self-assessment of surgical residents. Am. J. Surg. 2005, 189, 647–650. [Google Scholar] [CrossRef]
- Kilminster, S.; Downes, J.; Gough, B.; Murdoch-Eaton, D.; Roberts, T. Women in medicine—Is there a problem? A literature review of the changing gender composition, structures and occupational cultures in medicine. Med. Educ. 2007, 41, 39–49. [Google Scholar] [CrossRef]
- Whittle, S.R.; Eaton, D.G. Attitudes towards transferable skills in medical undergraduates. Med. Educ. 2001, 35, 148–153. [Google Scholar] [CrossRef]
- Sharp, L.K.; Wang, R.; Lipsky, M.S. Perception of competency to perform procedures and future practice intent: A national survey of family practice residents. Acad. Med. 2003, 78, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Van der Velden, L.; Batenburg, R.S. Aantal huisartsen en aantal FTE van huisartsen vanaf 2007 tot en met 2016: Werken er nu meer of minder huisartsen dan 10 jaar geleden en werken zij nu meer of minder FTE? Proc. Natl. Acad. Sci. USA 2017. [Google Scholar]
- Arthur, W., Jr.; Bennett, W., Jr.; Stanush, P.L.; McNelly, T.L. Factors That Influence Skill Decay and Retention: A Quantitative Review and Analysis. Hum. Perform. 1998, 11, 57–101. [Google Scholar] [CrossRef]
- Lugtenberg, M.; Burgers, J.S.; Besters, C.F.; Han, D.; Westert, G.P. Perceived barriers to guideline adherence: A survey among general practitioners. BMC Fam. Pract. 2011, 12, 98–2296. [Google Scholar] [CrossRef]
- Jansen, J.J.; Tan, L.H.; van der Vleuten, C.P.; van Luijk, S.J.; Rethans, J.J.; Grol, R.P. Assessment of competence in technical clinical skills of general practitioners. Med. Educ. 1995, 29, 247–253. [Google Scholar] [CrossRef][Green Version]
- Dorleijn, D.M.J.; Luijsterburg, P.A.J.; Reijman, M.; Kloppenburg, M.; Verhaar, J.A.N.; Bindels, P.J.E.; Bos, P.K.; Bierma-Zeinstra, S.M.A. Intramuscular glucocorticoid injection versus placebo injection in hip osteoarthritis: A 12-week blinded randomised controlled trial. Ann. Rheum. Dis. 2018, 77, 875–882. [Google Scholar] [CrossRef]
- Ekeberg, O.M.; Bautz-Holter, E.; Tveita, E.K.; Juel, N.G.; Kvalheim, S.; Brox, J.I. Subacromial ultrasound guided or systemic steroid injection for rotator cuff disease: Randomised double blind study. BMJ 2009, 338, a3112. [Google Scholar] [CrossRef]
- Mol, M.F.; Runhaar, J.; Bos, P.K.; Dorleijn, D.M.J.; Vis, M.; Gussekloo, J.; Bindels, P.J.E.; Bierma-Zeinstra, S.M.A. Effectiveness of intramuscular gluteal glucocorticoid injection versus intra-articular glucocorticoid injection in knee osteoarthritis: Design of a multicenter randomized, 24 weeks comparative parallel-group trial. BMC Musculoskelet. Disord. 2020, 21, 225. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic | Current Study % a | NIVEL % | |
|---|---|---|---|
| Sex | Man | 42.0 | 49 b |
| Woman | 52.1 | 51 b | |
| Neutral | 0.3 | - | |
| Organization | Solo practice | 19.2 | 17.8 b |
| Duo practice | 23.7 | 40.3 b | |
| Group practice | 20.8 | 41.9 b | |
| Health center | 15.5 | - | |
| Other c | 11.5 | - | |
| Work setting | Rural | 26.8 | 30.2 d |
| Urban | 67.6 | 69.8 d | |
| FTE | 0–0.20 | 1.7 | 0.2 |
| 0.21–0.40 | 5.9 | 2.8 | |
| 0.41–0.60 | 20.6 | 15.9 | |
| 0.61–0.80 | 30.7 | 28.5 | |
| 0.81–1 | 35.2 | 52.6 | |
| Patient population e | < standard practice | 13.2 | - |
| = standard practice | 25.9 | - | |
| > standard practice | 55.2 | - | |
| Completion GP training | <5 years | 23.1 | 13.6 f |
| 5–15 years | 33.2 | 29.4 f | |
| 16–25 years | 18.9 | 18.5 fg | |
| >25 years | 19.4 | 38.6 fg | |
| Trainer | Yes | 24.5 | - |
| No | 70.1 | - | |
| GP musculoskeletal system | Yes | 1.7 | - |
| No | 93.0 | - | |
| Indication | All GPs % (N) | Competent % (N) | Incompetent % (N) | P-Value |
|---|---|---|---|---|
| Indications for which an injection is recommended by the Dutch College of General Practitioners | ||||
| Carpal tunnel syndrome | 36.1 (330) | 32.2 (267) | 52.4 (63) | 0.003 |
| Knee osteoarthritis | 26.7 (333) | 23.0 (270) | 42.9 (63) | 0.001 |
| Plantar fasciitis | 22.7 (326) | 20.9 (263) | 30.2 (63) | 0.116 |
| De Quervain’s tenosynovitis | 22.5 (329) | 16.1 (267) | 50.0 (62) | 0.000 |
| Supraspinatus tendinitis | 20.0 (320) | 16.9 (260) | 33.3 (60) | 0.004 |
| Trigger finger/thumb | 17.1 (333) | 12.6 (270) | 36.5 (63) | 0.000 |
| Osteoarthritis shoulder | 16.9 (325) | 14.5 (262) | 27.0 (63) | 0.018 |
| Trochanteric bursitis | 5.8 (330) | 4.1 (268) | 12.9 (62) | 0.007 |
| Bursitis shoulder | 2.1 (333) | 0.7 (270) | 7.9 (63) | 0.000 |
| Indications for which an injection is not recommended by the Dutch College of General Practitioners | ||||
| Ankle osteoarthritis | 50.0 (324) | 50.2 (261) | 49.2 (63) | 0.888 |
| Osteoarthritis MCP/PIP/DIP | 48.9 (321) | 44.2 (258) | 68.3 (63) | 0.001 |
| Osteoarthritis CMC | 48.9 (319) | 45.1 (257) | 64.5 (62) | 0.006 |
| Sacroiliitis | 44.4 (420) | 43.4 (258) | 48.4 (62) | 0.479 |
| Achilles tendinitis | 33.1 (323) | 31.2 (260) | 41.3 (63) | 0.126 |
| Prepatellar bursitis | 11.9 (327) | 9.1 (264) | 23.8 (63) | 0.001 |
| Medial epicondylitis | 8.5 (329) | 7.5 (266) | 12.7 (63) | 0.185 |
| Lateral epicondylitis | 7.0 (328) | 6.4 (265) | 9.5 (63) | 0.385 |
| Olecranon bursitis | 5.8 (327) | 4.9 (265) | 9.7 (62) | 0.148 |
| Demographic | N | Competent % | Incompetent % | P-Value | |
|---|---|---|---|---|---|
| Sex | Man | 149 | 93.3 | 6.7 | - |
| Woman | 185 | 70.8 | 29.2 | 0.000 | |
| Organization | Solo practice | 70 | 81.4 | 18.6 | - |
| Duo practice | 85 | 78.8 | 21.2 | - | |
| Group practice | 74 | 79.7 | 20.3 | - | |
| Health center | 55 | 83.6 | 16.4 | - | |
| Other | 41 | 80.5 | 19.5 | 0.967 | |
| Work setting | Rural | 95 | 78.9 | 21.1 | - |
| Urban | 240 | 81.2 | 18.8 | 0.631 | |
| Full-time equivalent (FTE) | 0–0.20 | 6 | 66.7 | 33.3 | - |
| 0.21–0.40 | 21 | 61.9 | 38.1 | - | |
| 0.41–0.60 | 73 | 68.5 | 31.5 | - | |
| 0.61–0.80 | 109 | 84.4 | 15.6 | - | |
| 0.81–1 | 125 | 80.2 | 19.2 | 0.001 | |
| Patient population | < standard practice | 47 | 76.6 | 23.4 | - |
| = standard practice | 92 | 83.7 | 16.3 | - | |
| > Standard practice | 196 | 80.1 | 19.9 | 0.584 | |
| Completion GP training | < 5 years | 82 | 81.7 | 18.3 | - |
| 5–15 years | 118 | 78.8 | 21.2 | - | |
| 16–25 years | 67 | 73.1 | 26.9 | - | |
| > 25 years | 69 | 89.9 | 10.1 | 0.090 | |
| Trainer | Yes | 87 | 81.6 | 18.4 | - |
| No | 249 | 80.3 | 19.7 | 0.793 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spruit, E.; Mol, M.F.; Bos, P.K.; Bierma-Zeinstra, S.M.A.; Krastman, P.; Runhaar, J. Self-Assessment of Competence and Referral Behavior for Musculoskeletal Injections among Dutch General Practitioners. J. Clin. Med. 2020, 9, 1880. https://doi.org/10.3390/jcm9061880
Spruit E, Mol MF, Bos PK, Bierma-Zeinstra SMA, Krastman P, Runhaar J. Self-Assessment of Competence and Referral Behavior for Musculoskeletal Injections among Dutch General Practitioners. Journal of Clinical Medicine. 2020; 9(6):1880. https://doi.org/10.3390/jcm9061880
Chicago/Turabian StyleSpruit, Emely, Marianne F. Mol, P. Koen Bos, Sita M.A. Bierma-Zeinstra, Patrick Krastman, and Jos Runhaar. 2020. "Self-Assessment of Competence and Referral Behavior for Musculoskeletal Injections among Dutch General Practitioners" Journal of Clinical Medicine 9, no. 6: 1880. https://doi.org/10.3390/jcm9061880
APA StyleSpruit, E., Mol, M. F., Bos, P. K., Bierma-Zeinstra, S. M. A., Krastman, P., & Runhaar, J. (2020). Self-Assessment of Competence and Referral Behavior for Musculoskeletal Injections among Dutch General Practitioners. Journal of Clinical Medicine, 9(6), 1880. https://doi.org/10.3390/jcm9061880