Hyperspectral Ophthalmoscope Images for the Diagnosis of Diabetic Retinopathy Stage



Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Preparation
2.2. Ethical Statement
2.3. Clinical Features and Stages of Diabetic Retinopathy
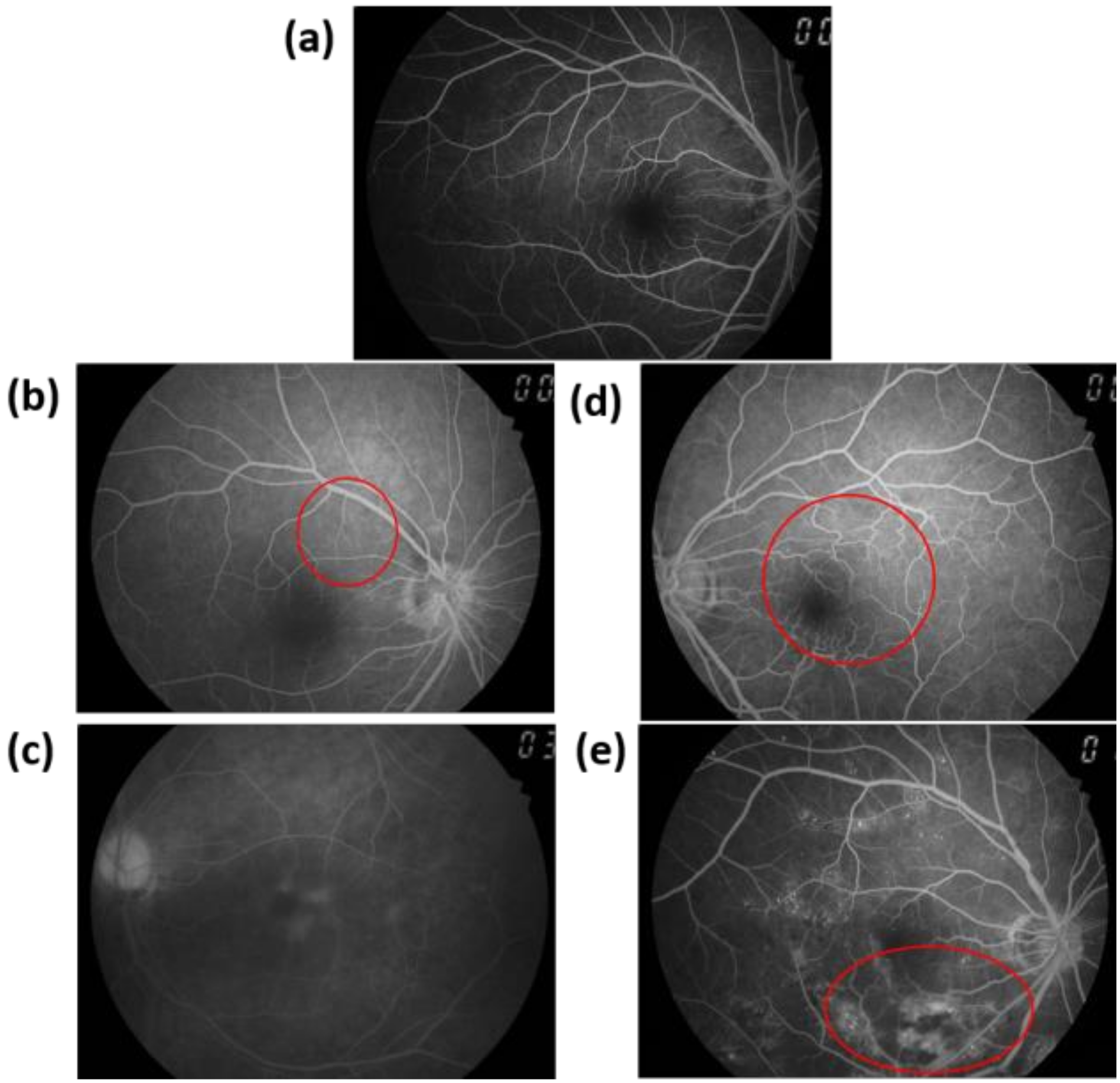
2.4. Fluorescein Angiography
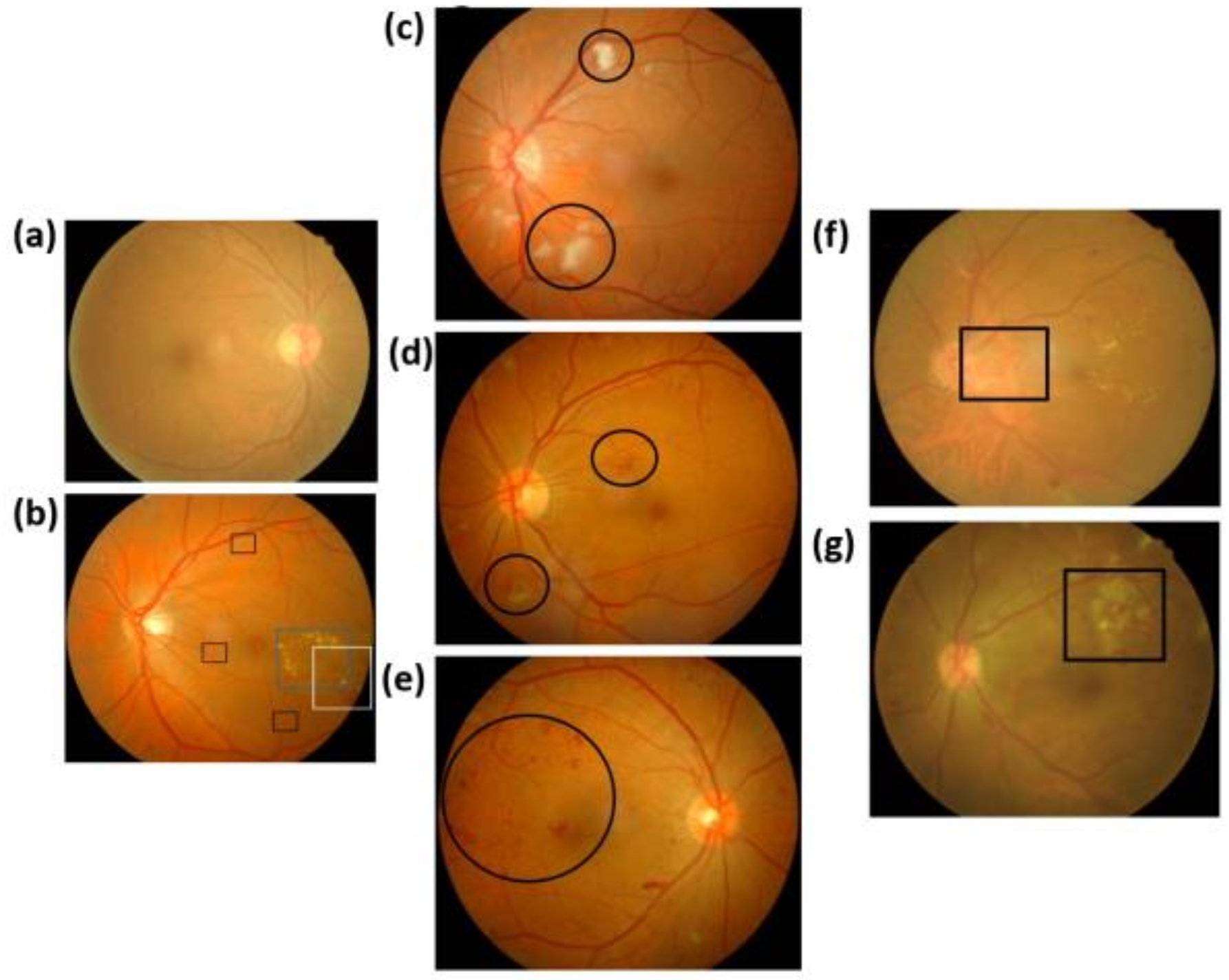
2.5. Ophthalmoscope Images
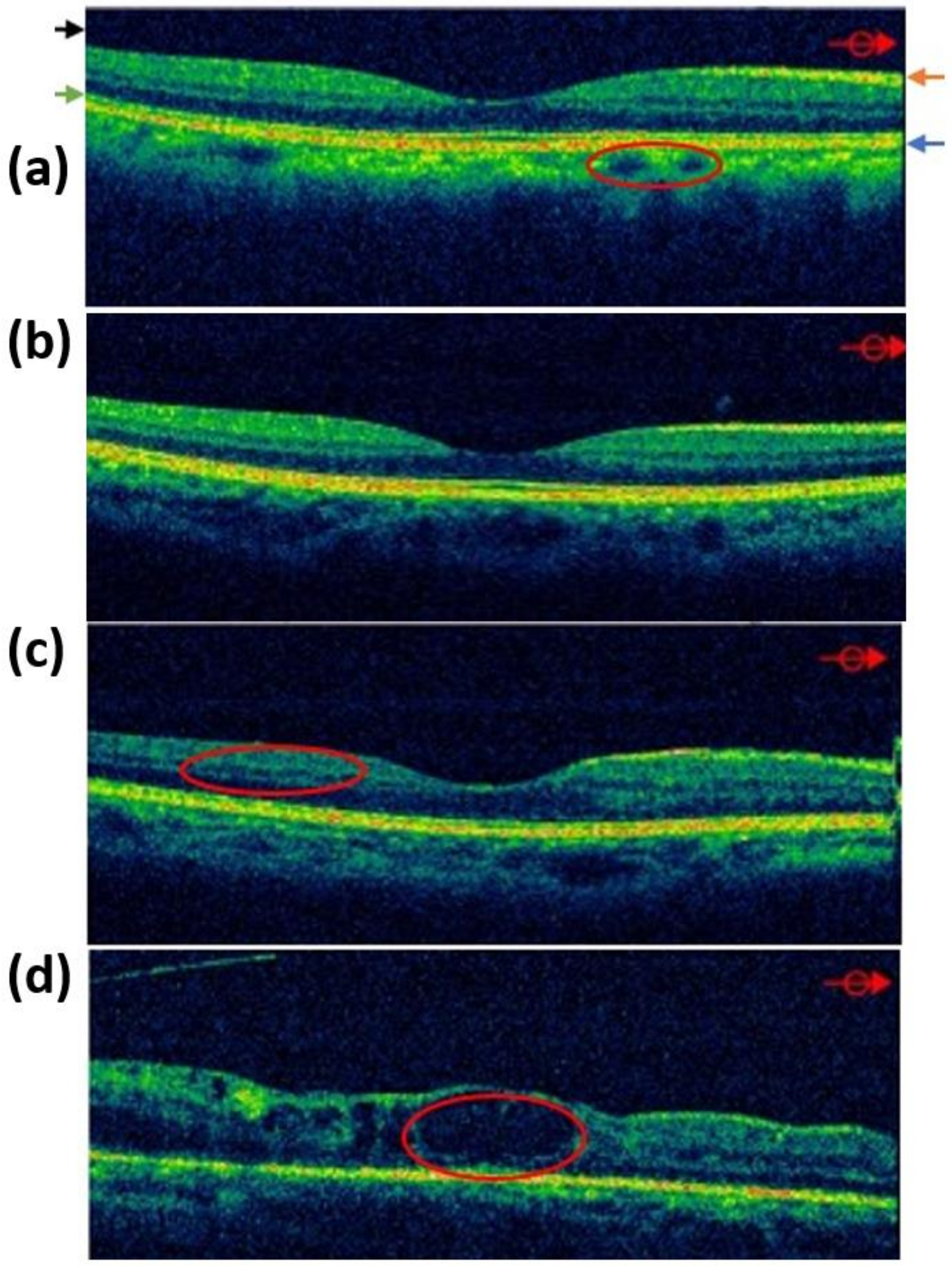
2.6. Optical Coherence Tomography Images
2.7. Hyperspectral Ophthalmoscope Images
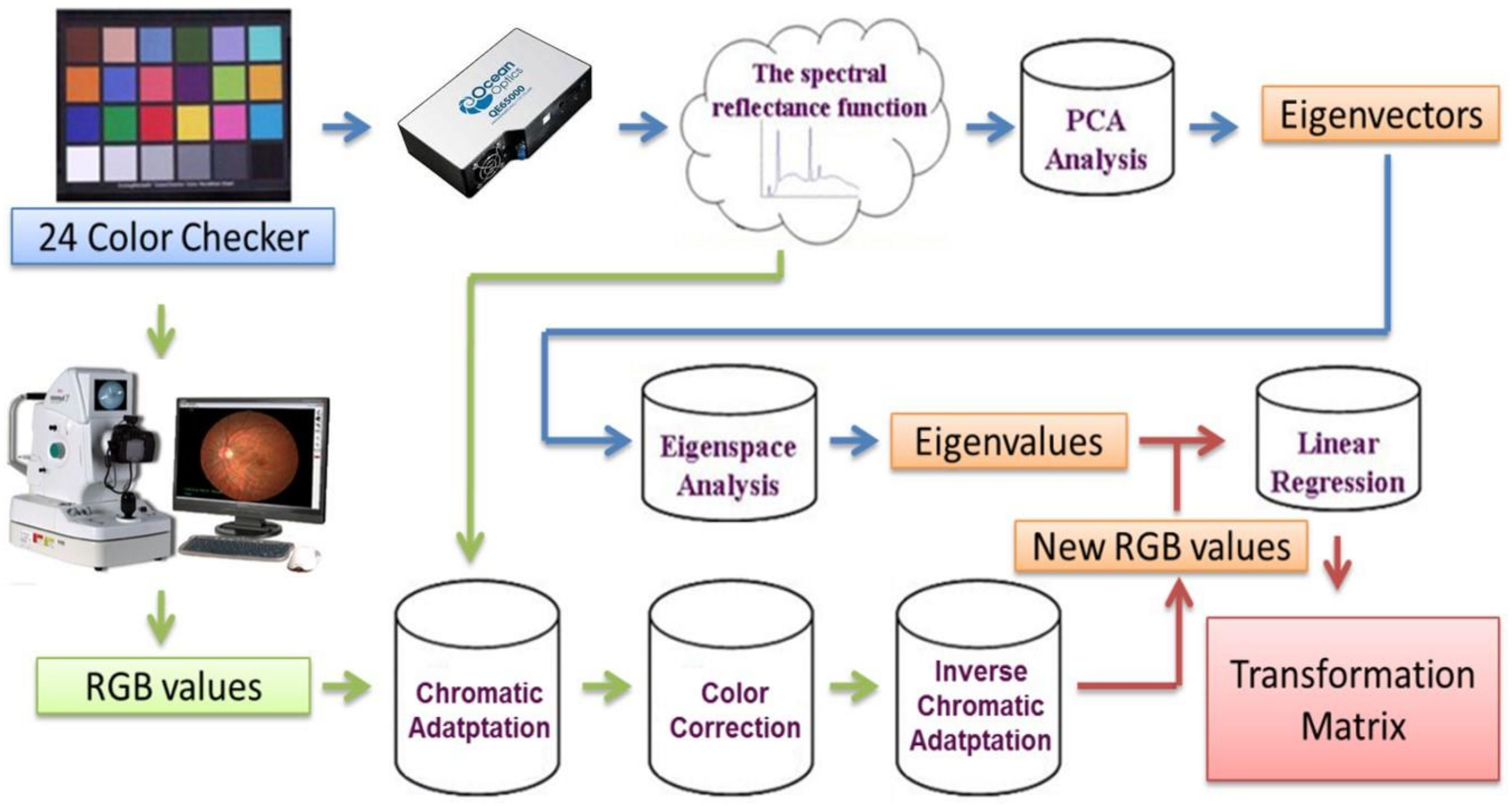
2.8. Hyperspectral Ophthalmoscope Imaging Calculated Processes
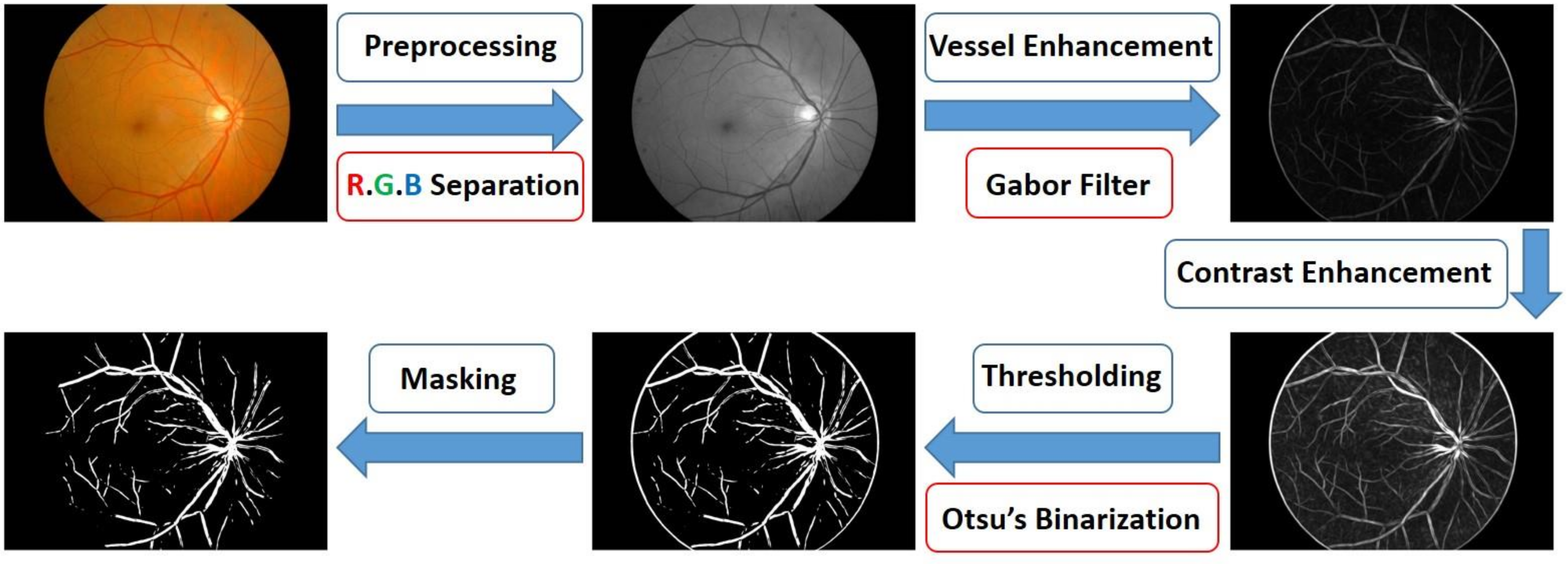
2.9. Retinal Image Processing Algorithm
2.10. Blood Oxygen Saturation Calculation
3. Results
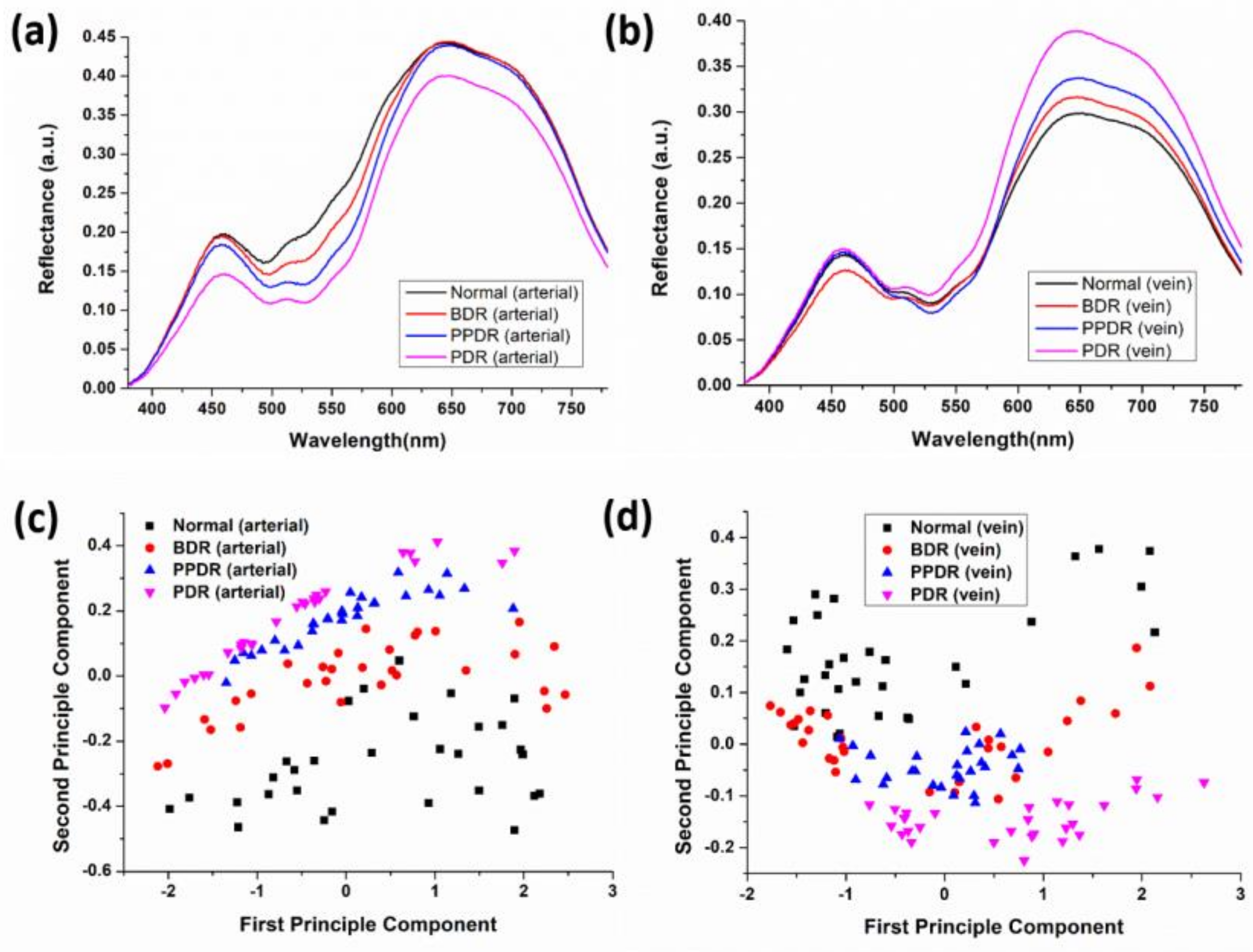
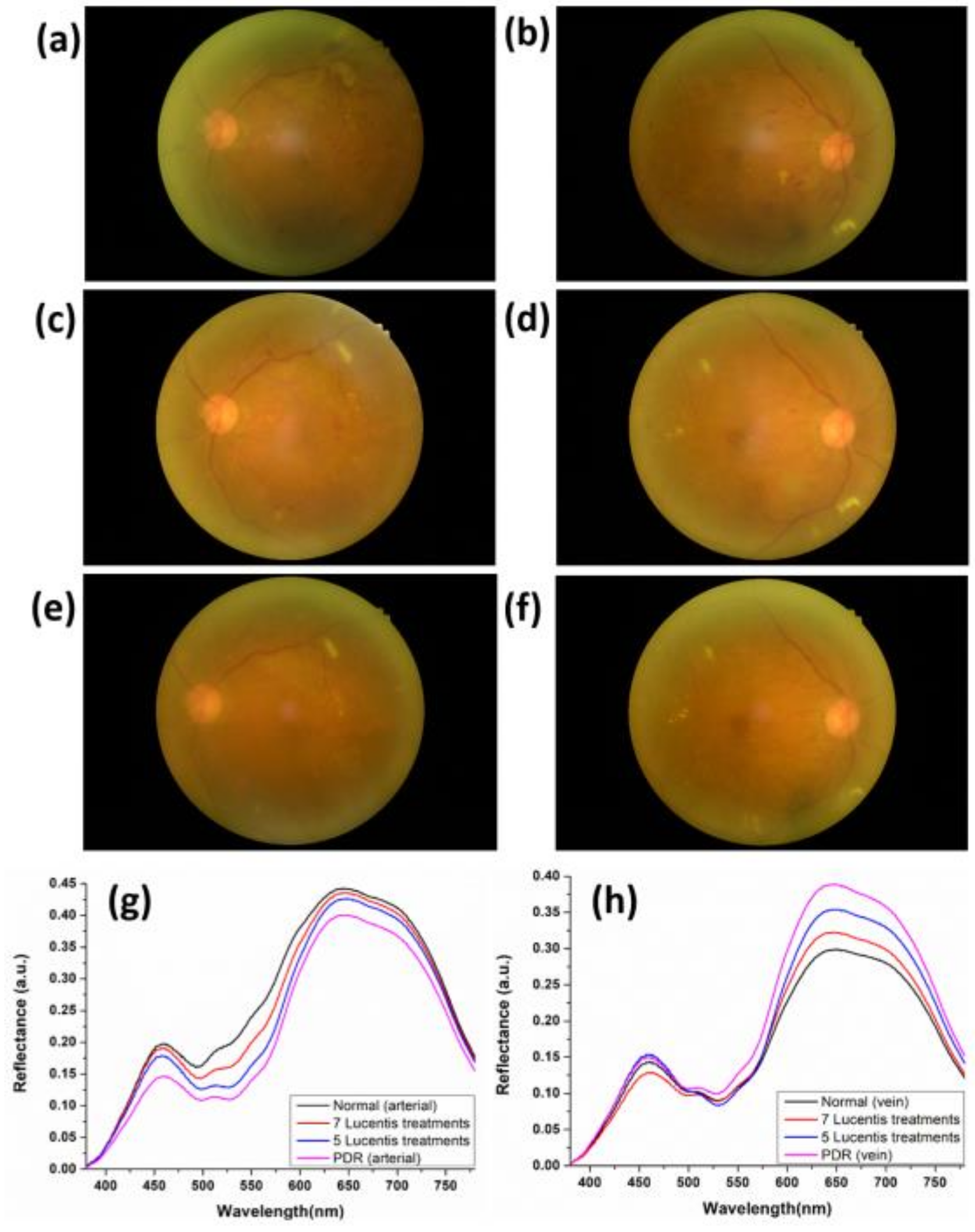
3.1. Average Reflection Spectrum
3.2. Spectral Characteristics
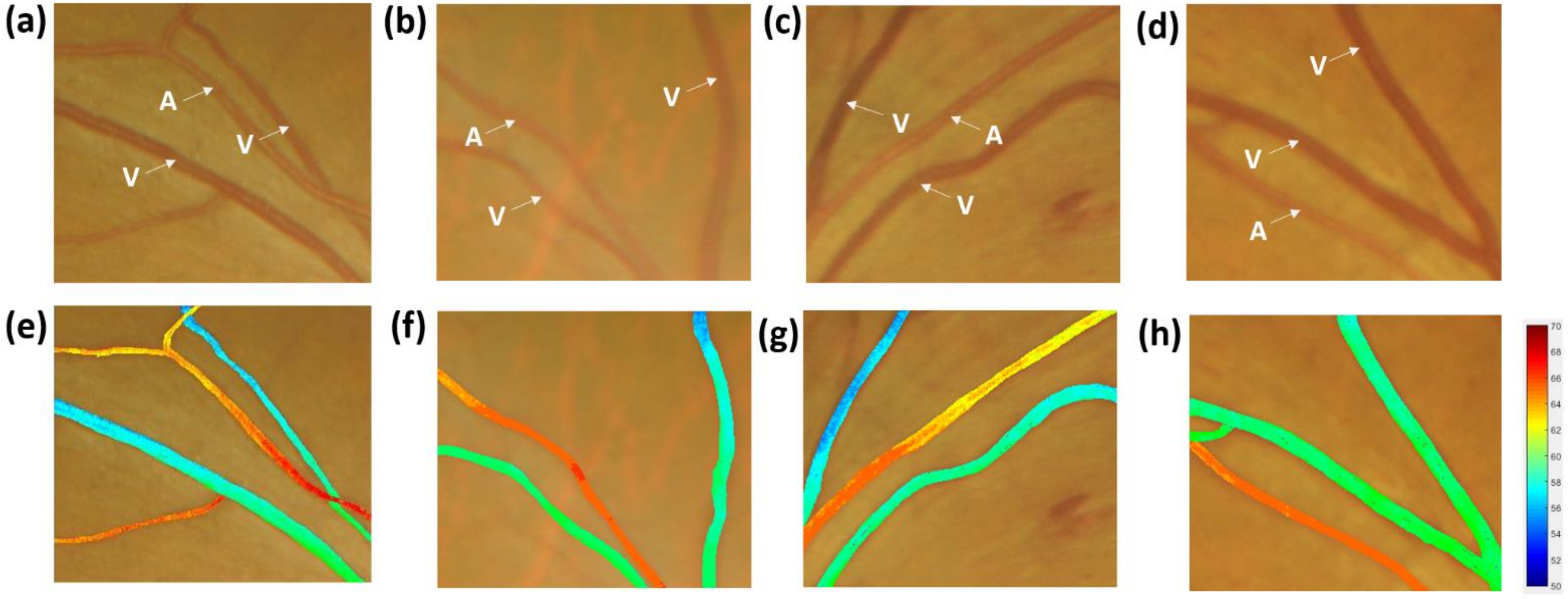
3.3. Oxygen Saturation Profile
3.4. Patient Referral Decision
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Unger, R.H. Reinventing type 2 diabetes: Pathogenesis, treatment, and prevention. JAMA 2008, 299, 1185–1187. [Google Scholar] [CrossRef] [PubMed]
- Whiting, D.R.; Guariguata, L.; Weil, C.; Shaw, J. IDF diabetes atlas: Global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res. Clin. Pract. 2011, 94, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Robert, N.; Frank, M.D. Diabetic Retinopathy. N. Engl. J. Med. 2004, 350, 48–58. [Google Scholar] [CrossRef]
- Aiello, L.P.; Gardner, T.W.; King, G.L.; Blankenship, G.; Cavallerano, J.D.; Ferris, F.L.; Klein, R. Diabetic Retinopathy. Diabetes Care 1998, 21, 143–156. [Google Scholar] [CrossRef]
- Kern, T.S.; Tang, J.; Mizutani, M.; Kowluru, R.A.; Nagaraj, R.H.; Romeo, G.; Podesta, F.; Lorenzi, M. Response of capillary cell death to aminoguanidine predicts the development of retinopathy: Comparison of diabetes and galactosemia. Investig. Ophthalmol. Vis. Sci. 2000, 41, 3972–3978. [Google Scholar]
- Kowluru, R.A.; Odenbach, S. Effect of long-term administration of α-lipoic acid on retinal capillary cell death and the development of retinopathy in diabetic rats. Diabetes 2004, 53, 3233–3238. [Google Scholar] [CrossRef]
- Robinson, R.; Barathi, V.A.; Chaurasia, S.S.; Wong, T.Y.; Kern, T.S. Update on animal models of diabetic retinopathy: From molecular approaches to mice and higher mammals. Dis. Models Mech. 2012, 5, 444–456. [Google Scholar] [CrossRef]
- Akram, M.U.; Khalid, S.; Khan, S.A. Identification and classification of microaneurysms for early detection of diabetic retinopathy. Pattern Recognit. 2013, 46, 107–116. [Google Scholar] [CrossRef]
- Akram, M.U.; Khalid, S.; Tariq, A.; Khan, S.A.; Azam, F. Detection and classification of retinal lesions for grading of diabetic retinopathy. Comput. Biol. Med. 2014, 45, 161–171. [Google Scholar] [CrossRef]
- Wan, S.; Liang, Y.; Zhang, Y. Deep convolutional neural networks for diabetic retinopathy detection by image classification. Comput. Electr. Eng. 2018, 72, 274–282. [Google Scholar] [CrossRef]
- Arsalan, M.; Owais, M.; Mahmood, T.; Cho, S.W.; Park, K.R. Aiding the Diagnosis of Diabetic and Hypertensive Retinopathy Using Artificial Intelligence-Based Semantic Segmentation. J. Clin. Med. 2019, 8, 1446. [Google Scholar] [CrossRef] [PubMed]
- Sacconi, R.; Casaluci, M.; Borrelli, E.; Mulinacci, G.; Lamanna, F.; Gelormini, F.; Carnevali, A.; Querques, L.; Zerbini, G.; Bandello, F. Multimodal Imaging Assessment of Vascular and Neurodegenerative Retinal Alterations in Type 1 Diabetic Patients without Fundoscopic Signs of Diabetic Retinopathy. J. Clin. Med. 2019, 8, 1409. [Google Scholar] [CrossRef] [PubMed]
- Welikala, R.A.; Fraz, M.M.; Dehmeshki, J.; Hoppe, A.; Tah, V.; Mann, S.; Williamson, T.H.; Barman, S.A. Genetic algorithm based feature selection combined with dual classification for the automated detection of proliferative diabetic retinopathy. Comput. Med Imaging Graph. 2015, 43, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Nourrit, V.; Denniss, J.; Muqit, M.; Schiessl, I.; Fenerty, C.; Stanga, P.; Henson, D. High-resolution hyperspectral imaging of the retina with a modified fundus camera. J. Fr. Ophtalmol. 2010, 33, 686–692. [Google Scholar] [CrossRef]
- Kashani, A.H.; Jaime, G.R.L.; Saati, S.; Martin, G.; Varma, R.; Humayun, M.S. Non-invasive assessment of retinal vascular oxygen content among normal and diabetic human subjects: A study using hyperspectral computed tomographic imaging spectroscopy. Retina 2014, 34, 1854. [Google Scholar] [CrossRef]
- Weinberger, D.; Kramer, M.; Priel, E.; Gaton, D.D.; Axer-Siegel, R.; Yassur, Y. Indocyanine green angiographic findings in nonproliferative diabetic retinopathy. Am. J. Ophthalmol. 1998, 126, 238–247. [Google Scholar] [CrossRef]
- Browning, D.J.; McOwen, M.D.; Bowen Jr, R.M.; Tisha, L.O. Comparison of the clinical diagnosis of diabetic macular edema with diagnosis by optical coherence tomography. Ophthalmology 2004, 111, 712–715. [Google Scholar] [CrossRef]
- Mrejen, S.; Jung, J.J.; Chen, C.; Patel, S.N.; Gallego-Pinazo, R.; Yannuzzi, N.; Xu, L.; Marsiglia, M.; Boddu, S.; Freund, K.B. Long-term visual outcomes for a treat and extend anti-vascular endothelial growth factor regimen in eyes with neovascular age-related macular degeneration. J. Clin. Med. 2015, 4, 1380–1402. [Google Scholar] [CrossRef]
- Palochak, C.M.A.; Lee, H.E.; Song, J.; Geng, A.; Linsenmeier, R.A.; Burns, S.A.; Fawzi, A.A. Retinal Blood Velocity and Flow in Early Diabetes and Diabetic Retinopathy Using Adaptive Optics Scanning Laser Ophthalmoscopy. J. Clin. Med. 2019, 8, 1165. [Google Scholar] [CrossRef]
- Ginner, L.; Blatter, C.; Fechtig, D.; Schmoll, T.; Gröschl, M.; Leitgeb, R.A. Wide-Field OCT Angiography at 400 KHz Utilizing Spectral Splitting. In Proceedings of the Photonics, Kharagpur, India, 13–16 December 2014; pp. 369–379. [Google Scholar]
- Miura, M.; Hong, Y.-J.; Yasuno, Y.; Muramatsu, D.; Iwasaki, T.; Goto, H. Three-dimensional vascular imaging of proliferative diabetic retinopathy by Doppler optical coherence tomography. Am. J. Ophthalmol. 2015, 159, 528–538. [Google Scholar] [CrossRef]
- Wold, S.; Esbensen, K.; Geladi, P. Principal component analysis. Chemom. Intell. Lab. Syst. 1987, 2, 37–52. [Google Scholar] [CrossRef]
- Gadekallu, T.R.; Khare, N.; Bhattacharya, S.; Singh, S.; Reddy Maddikunta, P.K.; Ra, I.-H.; Alazab, M. Early detection of diabetic retinopathy using PCA-firefly based deep learning model. Electronics 2020, 9, 274. [Google Scholar] [CrossRef]
- Davis, M.D. Diabetic retinopathy: A clinical overview. Diabetes Care 1992, 15, 1844–1874. [Google Scholar] [CrossRef] [PubMed]
- Bowling, B. Kanski’s Clinical Ophthalmology: A Systematic Approach; Saunders Ltd.: Nottingham, UK, 2015. [Google Scholar]
- Wang, H.-C.; Chen, Y.-T.; Lin, J.-T.; Chiang, C.-P.; Cheng, F.-H. Enhanced visualization of oral cavity for early inflamed tissue detection. Opt. Express 2010, 18, 11800–11809. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-C.; Chen, Y.-T. Optimal lighting of RGB LEDs for oral cavity detection. Opt. Express 2012, 20, 10186–10199. [Google Scholar] [CrossRef]
- Wang, H.-C.; Tsai, M.-T.; Chiang, C.-P. Visual perception enhancement for detection of cancerous oral tissue by multi-spectral imaging. J. Opt. 2013, 15, 055301. [Google Scholar] [CrossRef]
- Hsiao, Y.-P.; Wang, H.-C.; Chen, S.-H.; Tsai, C.-H.; Yang, J.-H. Optical perception for detection of cutaneous T-cell lymphoma by multi-spectral imaging. J. Opt. 2014, 16, 125301. [Google Scholar] [CrossRef]
- Hsiao, Y.-P.; Wang, H.-C.; Chen, S.-H.; Tsai, C.-H.; Yang, J.-H. Identified early stage mycosis fungoides from psoriasis and atopic dermatitis using non-invasive color contrast enhancement by LEDs lighting. Opt. Quantum Electron. 2015, 47, 1599–1611. [Google Scholar] [CrossRef]
- Chang, S.-C.; Syu, H.-Y.; Wang, Y.-L.; Lai, C.-J.; Huang, S.-Y.; Wang, H.-C. Identifying the incidence level of periodontal disease through hyperspectral imaging. Opt. Quantum Electron. 2018, 50, 409. [Google Scholar] [CrossRef]
- Wu, I.-C.; Syu, H.-Y.; Jen, C.-P.; Lu, M.-Y.; Chen, Y.-T.; Wu, M.-T.; Kuo, C.-T.; Tsai, Y.-Y.; Wang, H.-C. Early identification of esophageal squamous neoplasm by hyperspectral endoscopic imaging. Sci. Rep. 2018, 8, 1–10. [Google Scholar] [CrossRef]
- Siddalingaswamy, P.; Prabhu, K.G. Automatic detection of multiple oriented blood vessels in retinal images. J. Biomed. Sci. Eng. 2010, 3, 101–107. [Google Scholar] [CrossRef]
- Rossant, F.; Badellino, M.; Chavillon, A.; Bloch, I.; Paques, M. A morphological approach for vessel segmentation in eye fundus images, with quantitative evaluation. J. Med. Imaging Health Inform. 2011, 1, 42–49. [Google Scholar] [CrossRef]
- Karunanayake, N.; Gnanasekera, M.; Kodikara, N. A Robust Algorithm for Retinal Blood Vessel Extraction. IJIRCCE 2015, 3297, 39. [Google Scholar] [CrossRef]
- Rangayyan, R.M.; Ayres, F.J.; Oloumi, F.; Oloumi, F.; Eshghzadeh-Zanjani, P. Detection of blood vessels in the retina with multiscale Gabor filters. J. Electron. Imaging 2008, 17, 023018. [Google Scholar] [CrossRef]
- Otsu, N. A threshold selection method from gray-level histograms. IEEE Trans. Syst. Man Cybern. 1979, 9, 62–66. [Google Scholar] [CrossRef]
- Prahl, S. Optical Absorption of Hemoglobin. 1999. Available online: http://omlc.ogi.edu/spectra/hemoglobin (accessed on 26 May 2020).
- Beach, J.; Schwenzer, K.; Srinivas, S.; Kim, D.; Tiedeman, J. Oximetry of retinal vessels by dual-wavelength imaging: Calibration and influence of pigmentation. J. Appl. Physiol. 1999, 86, 748–758. [Google Scholar] [CrossRef]
- Wang, H.-C.; Jen, C.-P.; Huang, C.-T.; Chen, Y.-S.; Kuo, C.-T. Diagnosis of Human Bladder Cancer Cells at Different Stages Using Multispectral Imaging Microscopy. IEEE J. Sel. Top. Quantum Electron. 2014, 20, 68800808. [Google Scholar] [CrossRef]
- Michelson, G.; Scibor, M. Intravascular oxygen saturation in retinal vessels in normal subjects and open-angle glaucoma subjects. Acta Ophthalmol. Scand. 2006, 84, 289–295. [Google Scholar] [CrossRef]
- Hammer, M.; Vilser, W.; Riemer, T.; Mandecka, A.; Schweitzer, D.; Kühn, U.; Dawczynski, J.; Liemt, F.; Strobel, J. Diabetic patients with retinopathy show increased retinal venous oxygen saturation. Graefe’ Arch. Clin. Exp. Ophthalmol. 2009, 247, 1025–1030. [Google Scholar] [CrossRef]
- Olafsdottir, O.B.; Hardarson, S.H.; Gottfredsdottir, M.S.; Harris, A.; Stefánsson, E. Retinal oximetry in primary open-angle glaucoma. Investig. Ophthalmol. Vis. Sci. 2011, 52, 6409–6413. [Google Scholar] [CrossRef]
- Hardarson, S.H.; Stefánsson, E. Retinal oxygen saturation is altered in diabetic retinopathy. Br. J. Ophthalmol. 2012, 96, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.W.; Shima, D.T.; Calias, P.; Cunningham, E.T.; Guyer, D.R.; Adamis, A.P. Pegaptanib, a targeted anti-VEGF aptamer for ocular vascular disease. Nat. Rev. Drug Discov. 2006, 5, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Simo, R.; Hernandez, C. Intravitreous anti-VEGF for diabetic retinopathy: Hopes and fears for a new therapeutic strategy. Diabetologia 2008, 51, 1574. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Predicted Referral | ||||
|---|---|---|---|---|
| Gold Standard Referral | Normal | BRD | PPDR | PDR |
| Normal | 45 | 5 | 0 | 0 |
| BDR | 5 | 43 | 4 | 1 |
| PPDR | 0 | 2 | 43 | 4 |
| PDR | 0 | 0 | 3 | 45 |
| Sensitivity (%) | Precision (%) | F1-Score (%) | Accuracy (%) | |
|---|---|---|---|---|
| Normal | 90.00 | 90.00 | 90.00 | 95.00 |
| BDR | 81.13 | 86.00 | 83.49 | 91.50 |
| PPDR | 87.75 | 86.00 | 86.86 | 93.50 |
| PDR | 93.75 | 90.00 | 91.83 | 96.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yao, H.-Y.; Tseng, K.-W.; Nguyen, H.-T.; Kuo, C.-T.; Wang, H.-C. Hyperspectral Ophthalmoscope Images for the Diagnosis of Diabetic Retinopathy Stage. J. Clin. Med. 2020, 9, 1613. https://doi.org/10.3390/jcm9061613
Yao H-Y, Tseng K-W, Nguyen H-T, Kuo C-T, Wang H-C. Hyperspectral Ophthalmoscope Images for the Diagnosis of Diabetic Retinopathy Stage. Journal of Clinical Medicine. 2020; 9(6):1613. https://doi.org/10.3390/jcm9061613
Chicago/Turabian StyleYao, Hsin-Yu, Kuang-Wen Tseng, Hong-Thai Nguyen, Chie-Tong Kuo, and Hsiang-Chen Wang. 2020. "Hyperspectral Ophthalmoscope Images for the Diagnosis of Diabetic Retinopathy Stage" Journal of Clinical Medicine 9, no. 6: 1613. https://doi.org/10.3390/jcm9061613
APA StyleYao, H.-Y., Tseng, K.-W., Nguyen, H.-T., Kuo, C.-T., & Wang, H.-C. (2020). Hyperspectral Ophthalmoscope Images for the Diagnosis of Diabetic Retinopathy Stage. Journal of Clinical Medicine, 9(6), 1613. https://doi.org/10.3390/jcm9061613