The Evaluation of Optic Nerves Using 7 Tesla “Silent” Zero Echo Time Imaging in Patients with Leber’s Hereditary Optic Neuropathy with or without Idebenone Treatment

 , ,
, ,  , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Silent-MT Sequence
2.2. Participant Population
2.3. Radiological Assessment
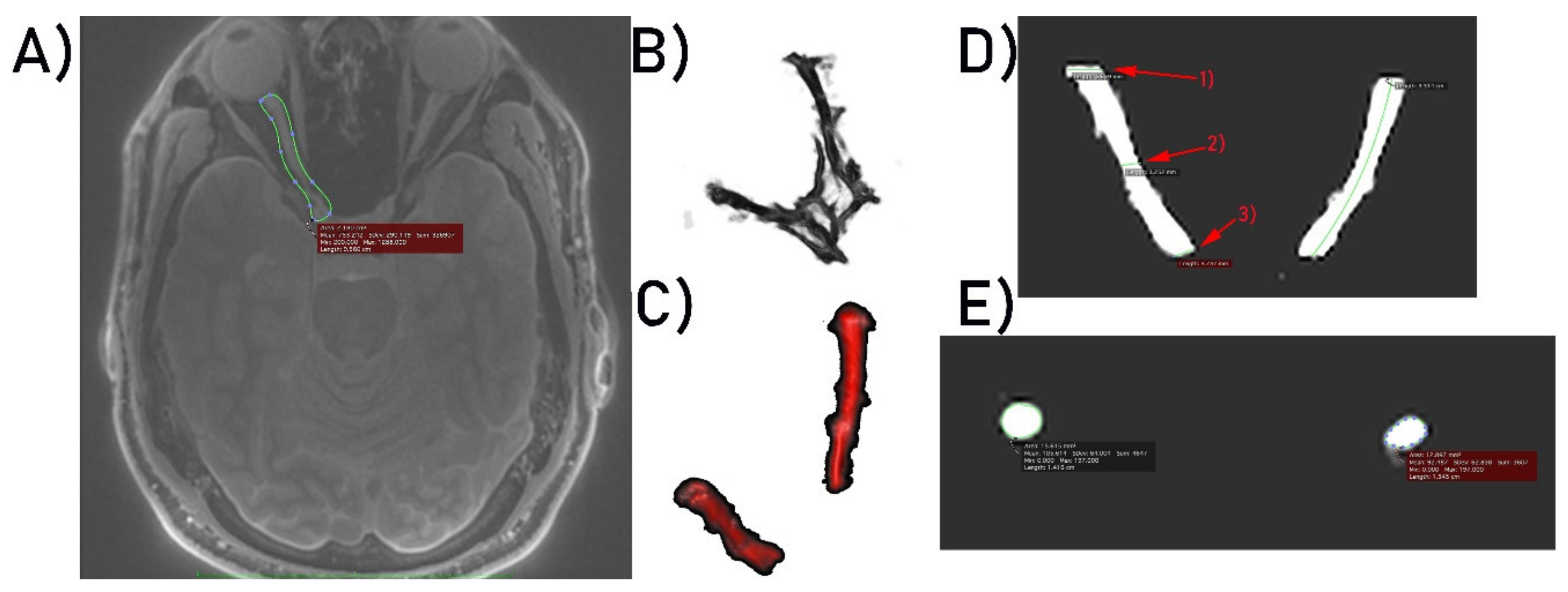
2.4. Image Analysis
3. Results
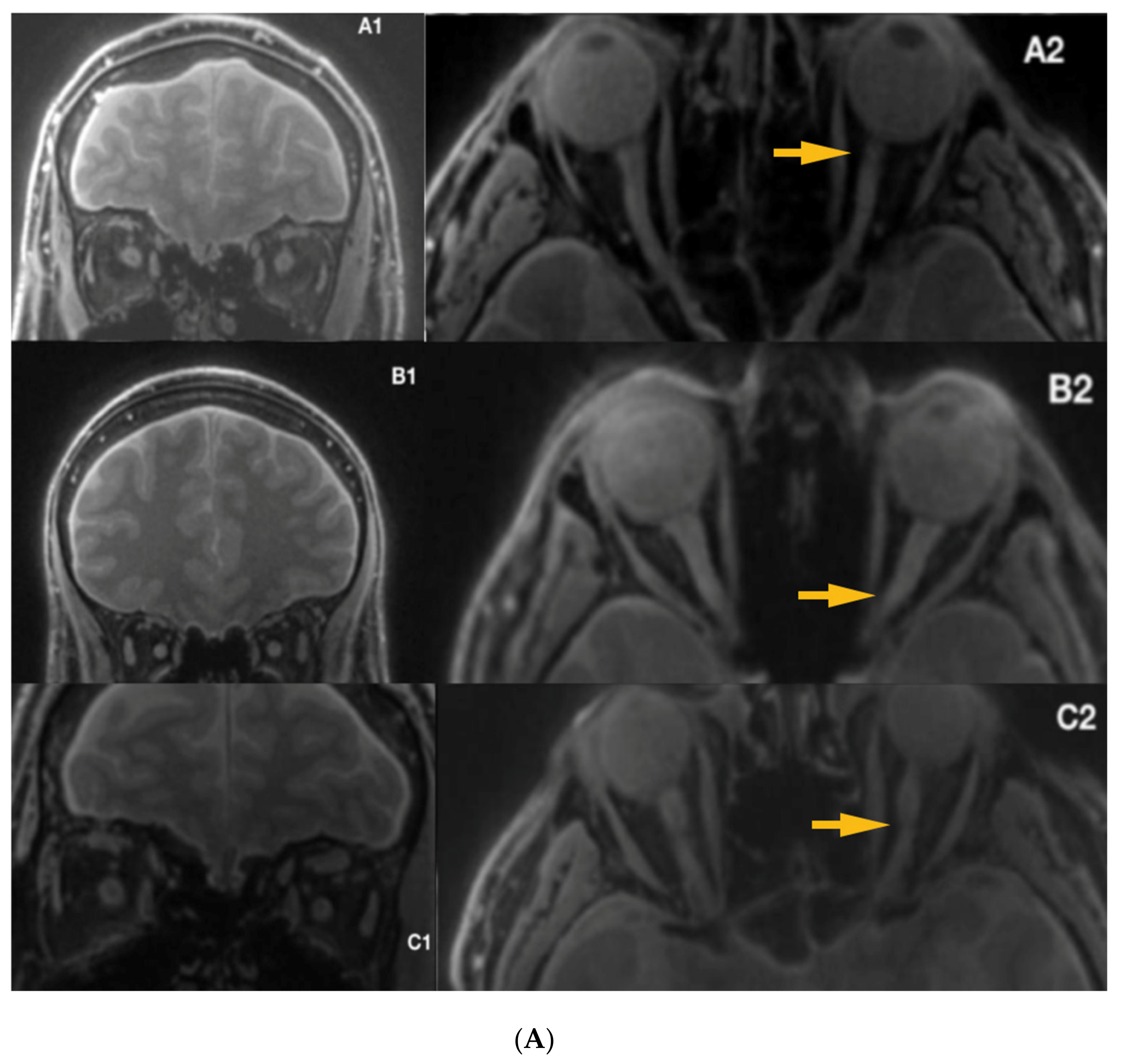
3.1. Radiological Inspection
3.2. Quantitative Analysis
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Barker, G.J. Technical issues for the study of the optic nerve with MRI. J. Neurol. Sci. 2000, 172, 13–16. [Google Scholar] [CrossRef]
- Al-Haddad, C.E.; Sebaaly, M.G.; Tutunji, R.N.; Mehanna, C.J.; Saaybi, S.R.; Khamis, A.M.; Hourani, R.G. Optic Nerve Measurement on MRI in the Pediatric Population: Normative Values and Correlations. Am. J. Neuroradiol. 2018, 39, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Maresky, H.S.; Ben Ely, A.; Bartischovsky, T.; Coret-Simon, J.; Morad, Y.; Rozowsky, S.; Klar, M.; Negieva, S.; Bekerman, I.; Tal, S. MRI measurements of the normal pediatric optic nerve pathway. J. Clin. Neurosci. 2018, 48, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Yiannakas, M.C.; Toosy, A.T.; Raftopoulos, R.E.; Kapoor, R.; Miller, D.H.; Wheeler-Kingshott, C.A. MRI acquisition and analysis protocol for in vivo intraorbital optic nerve segmentation at 3T. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4235–4240. [Google Scholar] [CrossRef] [PubMed]
- Dodds, N.I.; Atcha, A.W.; Birchall, D.; Jackson, A. Use of high-resolution MRI of the optic nerve in Graves’ ophthalmopathy. Br. J. Radiol. 2009, 82, 541–544. [Google Scholar] [CrossRef]
- Harrigan, R.L.; Smith, A.K.; Mawn, L.A.; Smith, S.A.; Landman, B.A. Short Term Reproducibility of a High Contrast 3-D Isotropic Optic Nerve Imaging Sequence in Healthy Controls. Proc. SPIE Int. Soc. Opt. Eng. 2016, 9783. [Google Scholar] [CrossRef]
- Barker, G.J. Diffusion-weighted imaging of the spinal cord and optic nerve. J. Neurol. Sci. 2001, 186, 45–49. [Google Scholar] [CrossRef]
- Wheeler-Kingshott, C.A.; Trip, S.A.; Symms, M.R.; Parker, G.J.; Barker, G.J.; Miller, D.H. In vivo diffusion tensor imaging of the human optic nerve: Pilot study in normal controls. Magn. Reson. Med. 2006, 56, 446–451. [Google Scholar] [CrossRef]
- Samson, R.S.; Kolappan, M.; Thomas, D.L.; Symms, M.R.; Connick, P.; Miller, D.H.; Wheeler-Kingshott, C.A.M. Development of a high-resolution fat and CSF-suppressed optic nerve DTI protocol at 3T: Application in multiple sclerosis. Funct. Neurol. 2013, 28, 93–100. [Google Scholar] [CrossRef]
- Thorpe, J.W.; Barker, G.J.; Jones, S.J.; Moseley, I.; Losseff, N.; MacManus, D.G.; Webb, S.; Mortimer, C.; Plummer, D.L.; Tofts, P.S. Magnetisation transfer ratios and transverse magnetisation decay curves in optic neuritis: Correlation with clinical findings and electrophysiology. J. Neurol. Neurosurg. Psychiatry 1995, 59, 487–492. [Google Scholar] [CrossRef][Green Version]
- Kolappan, M.; Henderson, A.P.; Jenkins, T.M.; Wheeler-Kingshott, C.A.; Plant, G.T.; Thompson, A.J.; Miller, D.H. Assessing structure and function of the afferent visual pathway in multiple sclerosis and associated optic neuritis. J. Neurol. 2009, 256, 305–319. [Google Scholar] [CrossRef] [PubMed]
- Klistorner, A.; Chaganti, J.; Garrick, R.; Moffat, K.; Yiannikas, C. Magnetisation transfer ratio in optic neuritis is associated with axonal loss, but not with demyelination. Neuroimage 2011, 56, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Van der Walt, A.; Paine, M.; Klistorner, A.; Butzkueven, H.; Egan, G.F.; Kilpatrick, T.J.; Kolbe, S.C. Optic Nerve Magnetisation Transfer Ratio after Acute Optic Neuritis Predicts Axonal and Visual Outcomes. PLoS ONE 2012, 7, e52291. [Google Scholar] [CrossRef]
- Leber, T. Ueber hereditaere und congenital angelegte sehnervenleiden. Graefes Arch. Clin. Exp. Ophthalmol. 1871, 17, 249–291. [Google Scholar] [CrossRef]
- Bell, J. Hereditary optic atrophy (Leber’s disease). In The Treasury of Human Inheritance; Pearson, K., Ed.; Cambridge University Press: Cambridge, UK, 1931; pp. 345–423. [Google Scholar]
- Imai, Y.; Moriwaki, D. A probable case of cytoplasmic inheritance in man: A critique of Leber’s disease. J. Genet. 1936, 33, 163. [Google Scholar] [CrossRef]
- Lundsgaard, R. A genealogic, genetic and clinical study of 101 cases of retrobulbar optic neuritis in 20 Danish families. Acta. Ophthalmol. 1944, 21, 1–306. [Google Scholar]
- Van Senus, A.H.C. Leber’s disease in the Netherlands. Doc. Ophthalmol. 1963, 17, 1–162. [Google Scholar] [CrossRef]
- Wallace, D. A new manifestation of Leber’s disease and a new explanation for the agency responsible for its unusual pattern of inheritance. Brain 1970, 93, 121–132. [Google Scholar] [CrossRef]
- Wallace, D.; Singh, G.; Lott, M.; Hodge, J.A.; Schurr, T.G.; Lezza, A.M.; Elsas, L.J.; Nikoskelainen, E.K. Mitochondrial DNA mutation associated with Leber’s hereditary optic neuropathy. Science 1988, 242, 1427–1430. [Google Scholar] [CrossRef]
- Miller, D.H.; Newton, M.R.; Van der Poel, J.C.; Du Boulay, E.P.G.H.; Halliday, A.M.; Kendall, B.E.; Johnson, G.; MacManus, D.G.; Moseley, I.F.; McDonald, W.I. Magnetic resonance imaging of the optic nerve in optic neuritis. Neurology 1988, 38, 175–179. [Google Scholar] [CrossRef]
- Kermode, A.G.; Moseley, I.F.; Kendall, B.E.; Miller, D.H.; MacManus, D.G.; McDonald, W.I. Magnetic resonance imaging in Leber’s optic neuropathy. J. Neurol. Neurosurg. Psychiatry 1989, 52, 671–674. [Google Scholar] [CrossRef] [PubMed]
- Dotti, M.T.; Caputo, N.; Signorini, E.; Federico, A. Magnetic resonance imaging findings in Leber’s hereditary optic neuropathy. Eur. Neurol. 1992, 32, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Tourbah, A. Contribution of imaging to the diagnosis of optic neuropathies. Rev. Neurol. 2012, 168, 702–705. [Google Scholar] [CrossRef]
- Honda, H.; Tsujihata, M.; Ochi, M.; Satoh, A.; Tomita, I.; Fujikawa, A. Hyperintense optic nerve lesion on T2-weighted MRI imaging in the acute stage of Leber’s hereditary optic neuropathy: A case report. Rinsho Shinkeigaku 2006, 46, 294–296. [Google Scholar] [PubMed]
- Mashima, Y.; Oshitari, K.; Imamura, Y.; Momoshima, S.; Shiga, H.; Oguchi, Y. Orbital high resolution magnetic resonance imaging with fast spin echo in the acute stage of Leber’s hereditary optic neuropathy. J. Neurol. Neurosurg. Psychiatry 1998, 64, 124–127. [Google Scholar] [CrossRef]
- Batioglu, F.; Atilla, H.; Eryilmaz, T. Chiasmal high signal on magnetic resonance imaging in the atrophic phase of Leber hereditary optic neuropathy. J. Neuroophthalmol. 2003, 23, 28–30. [Google Scholar]
- McClelland, C.M.; Van Stavern, G.P.; Tselis, A.C. Leber hereditary optic neuropathy mimicking neuromyelitis optica. J. Neuroophthalmol. 2011, 31, 265–268. [Google Scholar] [CrossRef]
- Van Westen, D.; Hammar, B.; Bynke, G. Magnetic resonance findings in the pregeniculate visual pathways in Leber heredi-tary optic neuropathy. J. Neuroophtalmol. 2011, 31, 48–51. [Google Scholar] [CrossRef]
- Vaphiades, M.S. Magnetic resonance findings in the pregeniculate visual pathways in Leber hereditary optic neu-ropathy. J. Neuroophthalmol. 2011, 31, 194. [Google Scholar] [CrossRef]
- Phillips, P.H.; Vaphiades, M.S.; Glasier, C.M.; Gray, L.G.; Lee, A.G. Chiasmal enlargement and optic nerve enhancement on magnetic resonance imaging in Leber hereditary optic neuropathy. Arch. Ophthalmol. 2003, 121, 577–579. [Google Scholar] [CrossRef]
- Blanc, C.; Heran, F.; Habas, C.; Bejot, Y.; Sahel, J.; Vignal-Clermont, C. MRI of the Optic Nerves and Chiasm in Patients with Leber He-reditary Optic Neuropathy. J. Neuro-Ophthalmol. 2018, 38. [Google Scholar] [CrossRef] [PubMed]
- Ong, E.; Biotti, D.; Abouaf, L.; Louis-Tisserand, G.; Tilikete, C.; Vighetto, A. Teaching neuroimages: Chiasmal enlargement and enhancement in Leber hereditary optic neuropathy. Neurology 2013, 81, 126–127. [Google Scholar] [CrossRef] [PubMed]
- Inglese, M.; Rovaris, M.; Bianchi, S.; La Mantiac, L.; Mancardid, G.L.; Ghezzie, A.; Montagnaf, P.; Salvig, F.; Filippia, M. Magnetic resonance imaging, magnetisation transfer imaging, and diffusion weighted imaging correlates of optic nerve, brain, and cervical cord damage in Leber’s hereditary optic neuropathy. J. Neurol. Neurosurg. Psychiatry 2001, 70, 444–449. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Iorga, R.E.; Mihailovici, R.; Ozturk, M.R.; Costin, D. Leber’s hereditary optic neuropathy—Case report. Rom. J. Ophthalmol. 2018, 62, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Mafee, M.F.; Rapoport, M.; Karimi, A.; Ansari, S.A.; Shah, J. Orbital and ocular imaging using 3- and 1.5-T MR imaging systems. Neuroimaging Clin. 2005, 15, 1–21. [Google Scholar] [CrossRef]
- Beenakker, J.M.; Wezel, J.; Groen, J.; Webb, A.G.; Börnert, P. Silent volumetric multi-contrast 7 Tesla MRI of ocular tumors using Zero Echo Time imaging. PLoS ONE 2019, 14, e0222573. [Google Scholar] [CrossRef]
- Symms, M.; Costagli, M.; Buonincontri, G.; Wiesinger, F.; Kelley, D.; Janich, M.A.; Aringhieri, G.; Marletta, M.; Barker, G.; Zampa, V.; et al. Zero Time of Echo imaging with an Adiabatic Fat Suppression Pulse at 7T. In Proceedings of the International Society for Magnetic Resonance in Medicine, Berlin, Germany, 19–25 May 2007. [Google Scholar]
- Guven, N. Idebenone for Leber’s hereditary optic neuropathy. Drugs Today 2016, 52, 173–181. [Google Scholar] [CrossRef]
- Lyseng-Williamson, K.A. Idebenone: A review in Leber’s Hereditary Optic Neuropathy. Drugs 2016, 76, 805–813. [Google Scholar] [CrossRef]
- Chinnery, P.F.; Klopstock, T. A Double-Blind, Randomised, Placebo-Controlled Study of the Efficacy, Safety and Tolerability of Idebenone in the Treatment of Patients with Leber’s Hereditary Optic Neuropathy. Available online: https://www.orpha.net/consor4.01/www/cgi-bin/ResearchTrials_Networks.php?lng=PT&data_id=81479&title=A-double-blind--randomised--placebo-controlled-study-of-the-efficacy--safety-and-tolerability-of-idebenone-in-the-treatment-of-patients-with-Leber-s-Hereditary-Optic-Neuropathy--LHON---Phase-II---coordination-&search=Disease_Search_Simple (accessed on 19 February 2010).
- Madio, D.P.; Lowe, I.J. Ultra-Fast Imaging Using Low Flip Angles and FIDs. Magn. Reson. Med. 1995, 34, 525–529. [Google Scholar] [CrossRef]
- Costagli, M.; Symms, M.R.; Angeli, L.; Kelley, D.A.C.; Biagi, L.; Farnetani, A.; Rua, C.; Donatelli, G.; Tiberi, G.; Tosetti, M.; et al. Assessment of Silent T1-weighted head imaging at 7 T. Eur. Radiol. 2016, 26, 1879–1888. [Google Scholar] [CrossRef]
- Kaldoudi, E.; Williams, S.C.R.E.; Barker, G.J.; Tofts, P.S. A Chemical Shift Inversion Recovery Sequence for Fat-Suppressed MRI: Theory and Experimental Validation. Magn. Reson. Imaging 1993, 11, 341–355. [Google Scholar] [CrossRef]
- Helms, G.; Dathe, H.; Kallenberg, K.; Dechent, P. High-Resolution Maps of Magnetization Transfer with Inherent Correction for RF Inhomogeneity and T1 Relaxation Obtained from 3D FLASH MRI. Magn. Reson. Med. 2008, 60, 1396–1407. [Google Scholar] [CrossRef] [PubMed]
- Heilmaier, C.; Theysohn, J.M.; Maderwald, S.; Kraff, O.; Ladd, M.E.; Ladd, C.S. A large-scale study on subjective perception of discomfort during 7 and 1.5 T MRI examinations. Bioelectromagnetics 2011, 32, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Cosottini, M.; Frosini, D.; Biagi, L.; Pesaresi, I.; Costagli, M.; Tiberi, G.; Symms, M.; Tosetti, M. Short-term side-effects of brain MR examination at 7 T: A single-centre experience. Eur. Radiol. 2014, 24, 1923–1928. [Google Scholar] [CrossRef]
- Klopstock, T.; Yu-Wai-Man, P.; Dimitriadis, K.; Rouleau, J.; Heck, S.; Bailie, M.; Atawan, A.; Chattopadhyay, S.; Schubert, M.; Garip, A.; et al. A randomized placebo-controlled trial of idebe- none in Leber’s hereditary optic neuropathy. Brain 2011, 134, 2677–2686. [Google Scholar] [CrossRef]
- Carelli, V.; Carbonelli, M.; De Coo, I.F.; Kawasaki, A.; Klopstock, T.; Lagreze, W.A.; La Morgia, C.; Newman, N.J.; Orssaud, C.; Pott, J.W.R.; et al. International consensus statement on the clini-cal and therapeutic management of leber hereditary optic neuropathy. J. Neuroophthalmol. 2017, 37, 371–381. [Google Scholar] [CrossRef]
- Carelli, V.; La Morgia, C.; Valentino, M.L.; Rizzo, G.; Carbonelli, M.; De Negri, A.M.; Sadun, F.; Carta, A.; Guerriero, S.; Simonelli, F.; et al. Idebenone treatment in Leber’s hereditary optic neuropathy. Brain 2011, 134, e188. [Google Scholar] [CrossRef]
- Jurkute, N.; Yu-Wai-Man, P. Leber hereditary optic neuropathy: Bridging the translational gap. Curr. Opin. Ophthalmol. 2017, 28, 403–409. [Google Scholar] [CrossRef]
- Klopstock, T.; Metz, G.; Yu-Wai-Man, P.; Büchner, B.; Gallenmüller, C.; Bailie, M.; Nwali, N.; Griffiths, P.G.; Von Livonius, B.; Reznicek, L.; et al. Persistence of the treatment effect of idebenone in Leber’s hereditary optic neuropathy. Brain 2013, 136, e230. [Google Scholar] [CrossRef]
- Man, P.; Griffiths, P.; Brown, D. The epidemiology of Leber hereditary optic neuropathy in the North East of England. Am. J. Hum. Genet. 2003, 72, 333–339. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Left | Right | |||||
|---|---|---|---|---|---|---|
| M (SD) | Min–Max | M (SD) | Min–Max | Z | p | |
| Length (cm) | 4.31 (0.49) | 3.50–5.50 | 4.28 (0.39) | 3.70–5.20 | 0.59 | 0.550 |
| Diameter (mm) 1 | 3.89 (0.63) | 2.30–4.90 | 4.06 (0.81) | 2.70–5.10 | 0.62 | 0.532 |
| Diameter 2 | 1.95 (0.55) | 0.70–3.00 | 2.32 (0.55) | 0.90–3.10 | 2.03 | 0.043 |
| Diameter 3 | 3.19 (0.39) | 2.50–3.80 | 3.24 (0.31) | 2.80–3.80 | 0.85 | 0.394 |
| Surface area (mm2) 1 | 12.23 (3.84) | 3.80–17.66 | 13.50 (5.23) | 5.55–21.58 | 0.91 | 0.364 |
| Surface area 2 | 3.27 (1.74) | 0.39–7.48 | 4.56 (1.91) | 0.64–7.95 | 2.04 | 0.040 |
| Surface area 3 | 8.05 (1.92) | 4.44–11.79 | 8.35 (1.64) | 6.41–11.52 | 0.62 | 0.532 |
| Idebenone Treatment (n = 6) | Without Treatment (n = 9) | |||||
|---|---|---|---|---|---|---|
| M (SD) | Min–Max | M (SD) | Min–Max | Z | p | |
| L. Length (cm) | 4.28 (0.43) | 3.50–4.70 | 4.33 (0.55) | 3.60–5.50 | 0.02 | 0.968 |
| L. Diameter (mm) 1 | 3.75 (0.82) | 2.30–4.40 | 3.98 (0.51) | 3.20–4.90 | 0.05 | 0.952 |
| L. Diameter 2 | 2.06 (0.77) | 0.70–3.00 | 1.87 (0.39) | 1.30–2.50 | −1.00 | 0.315 |
| L. Diameter 3 | 3.47 (0.38) | 2.90–3.80 | 3.01 (0.28) | 2.50–3.40 | −2.06 | 0.038 |
| L. Surface area (mm2) 1 | 11.66 (4.79) | 3.80–16.59 | 12.61 (3.33) | 7.52–17.66 | 0.05 | 0.953 |
| L. Surface area 2 | 3.96 (2.36) | 0.39–7.48 | 2.81 (1.11) | 1.33–4.75 | −1.12 | 0.262 |
| L. Surface area 3 | 9.47 (1.28) | 7.18–11.79 | 7.11 (1.38) | 4.44–8.66 | −2.06 | 0.038 |
| R. Length (cm) | 4.16 (0.30) | 3.70–4.60 | 4.36 (0.44) | 3.80–5.20 | 0.94 | 0.345 |
| R. Diameter (mm) 1 | 3.96 (0.75) | 2.70–4.80 | 4.12 (0.88) | 2.80–5.10 | 0.53 | 0.595 |
| R. Diameter 2 | 2.38 (0.54) | 1.50–3.10 | 2.27 (0.58) | 0.90–3.00 | −0.17 | 0.859 |
| R. Diameter 3 | 3.35 (0.32) | 2.80–3.80 | 3.17 (0.31) | 2.90–3.80 | −1.00 | 0.316 |
| R. Surface area (mm2) 1 | 12.54 (4.35) | 5.55–17.16 | 14.14 (5.90) | 6.75–20.58 | 0.76 | 0.443 |
| R. Surface area 2 | 4.76 (2.07) | 1.73–7.95 | 4.42 (1.90) | 0.64–7.75 | −0.41 | 0.679 |
| R. Surface area 3 | 8.85 (1.65) | 6.63–11.35 | 8.02 (1.64) | 6.41–11.52 | −1.00 | 0.316 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grochowski, C.; Symms, M.; Jonak, K.; Krukow, P.; Wood, T.C.; Ljungberg, E.; Enseñat, J.; Nowomiejska, K.; Rejdak, R.; Maciejewski, R.; et al. The Evaluation of Optic Nerves Using 7 Tesla “Silent” Zero Echo Time Imaging in Patients with Leber’s Hereditary Optic Neuropathy with or without Idebenone Treatment. J. Clin. Med. 2020, 9, 1112. https://doi.org/10.3390/jcm9041112
Grochowski C, Symms M, Jonak K, Krukow P, Wood TC, Ljungberg E, Enseñat J, Nowomiejska K, Rejdak R, Maciejewski R, et al. The Evaluation of Optic Nerves Using 7 Tesla “Silent” Zero Echo Time Imaging in Patients with Leber’s Hereditary Optic Neuropathy with or without Idebenone Treatment. Journal of Clinical Medicine. 2020; 9(4):1112. https://doi.org/10.3390/jcm9041112
Chicago/Turabian StyleGrochowski, Cezary, Mark Symms, Kamil Jonak, Paweł Krukow, Tobias C Wood, Emil Ljungberg, Joaquim Enseñat, Katarzyna Nowomiejska, Robert Rejdak, Ryszard Maciejewski, and et al. 2020. "The Evaluation of Optic Nerves Using 7 Tesla “Silent” Zero Echo Time Imaging in Patients with Leber’s Hereditary Optic Neuropathy with or without Idebenone Treatment" Journal of Clinical Medicine 9, no. 4: 1112. https://doi.org/10.3390/jcm9041112
APA StyleGrochowski, C., Symms, M., Jonak, K., Krukow, P., Wood, T. C., Ljungberg, E., Enseñat, J., Nowomiejska, K., Rejdak, R., Maciejewski, R., & Barker, G. J. (2020). The Evaluation of Optic Nerves Using 7 Tesla “Silent” Zero Echo Time Imaging in Patients with Leber’s Hereditary Optic Neuropathy with or without Idebenone Treatment. Journal of Clinical Medicine, 9(4), 1112. https://doi.org/10.3390/jcm9041112