Early Postoperative Death in Patients Undergoing Emergency High-Risk Surgery: Towards a Better Understanding of Patients for Whom Surgery May not Be Beneficial

Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
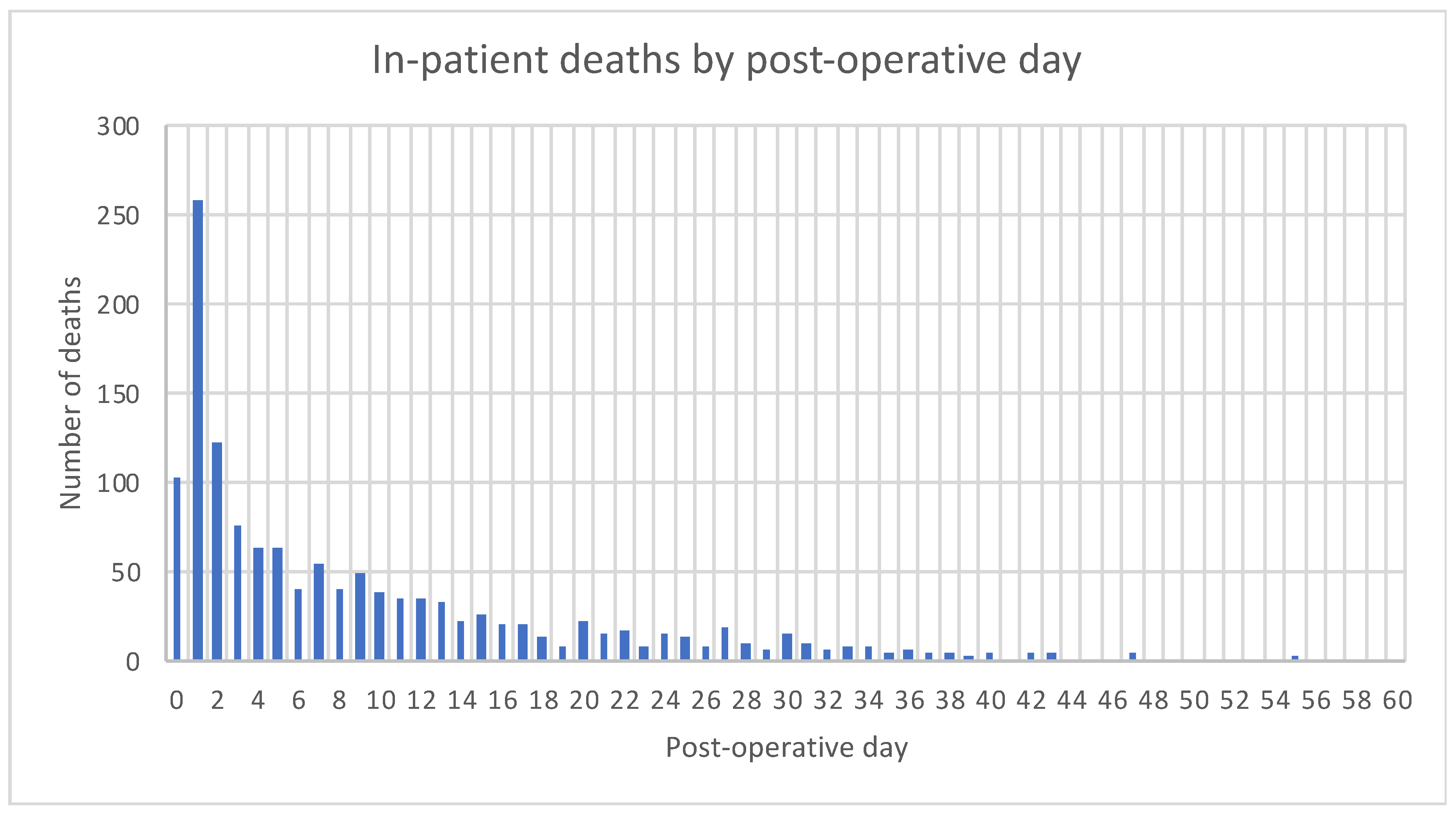
3.1. In-Patient Mortality
3.2. Demographics and Physiological Variables
3.3. Surgical Indications and Findings
3.4. Standards of Care
3.5. Univariate and Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| 95% CI for OR | |||||
|---|---|---|---|---|---|
| n = 13,688 (98% of Cases) | df | p-Value | OR | Lower | Upper |
| Age on Arrival | 1 | 0.000 | 1.022 | 1.014 | 1.031 |
| ln_postoperative P-POSSUM | 1 | 0.000 | 2.173 | 1.885 | 2.505 |
| ASA Score (ref = 1) | 4 | 0.000 | |||
| ASA Score 2 | 1 | 0.726 | 1.243 | 0.368 | 4.195 |
| ASA Score 3 | 1 | 0.068 | 2.967 | 0.922 | 9.547 |
| ASA Score 4 | 1 | 0.002 | 6.246 | 1.936 | 20.145 |
| ASA Score 5 | 1 | 0.000 | 16.254 | 4.827 | 54.734 |
| ln_creatinine | 1 | 0.011 | 1.274 | 1.058 | 1.535 |
| Systolic blood pressure | 1 | 0.000 | 0.992 | 0.988 | 0.997 |
| Glasgow coma score | 1 | 0.001 | 0.942 | 0.910 | 0.975 |
| ln time to theater | 1 | 0.002 | 0.890 | 0.827 | 0.957 |
| Histology (reference = Other) | 7 | 0.000 | |||
| Histology (Crohn’s Disease) | 1 | 0.706 | 0.786 | 0.224 | 2.758 |
| Histology (Diverticulitis) | 1 | 0.074 | 0.629 | 0.378 | 1.047 |
| Histology (Ischemia) | 1 | 0.125 | 0.729 | 0.487 | 1.092 |
| Histology (Malignancy) | 1 | 0.698 | 1.075 | 0.747 | 1.546 |
| Histology (PUD) | 1 | 0.086 | 0.500 | 0.227 | 1.102 |
| Histology (UC) | 1 | 0.260 | 0.309 | 0.040 | 2.388 |
| Histology (NA) | 1 | 0.000 | 0.547 | 0.397 | 0.752 |
| Operative findings; Intestinal ischemia | 1 | 0.029 | 1.451 | 1.039 | 2.026 |
| Operative findings; Perforated Small Bowel | 1 | 0.007 | 1.389 | 1.093 | 1.765 |
| Indication for surgery; Ischemia | 1 | 0.000 | 2.003 | 1.418 | 2.829 |
References
- National Emergency Laparotomy Audit. Available online: https://www.nela.org.uk (accessed on 9 April 2020).
- Aggarwal, G.; Peden, C.J.; Mohammed, M.A.; Pullyblank, A.; Williams, B.; Stephens, T.; Kellett, S.; Kirkby-Bott, J.; Quiney, N. Evaluation of an evidence-based care bundle in emergency laparotomy. JAMA Surg. 2019, 154, e190145. [Google Scholar] [CrossRef] [PubMed]
- Chiu, A.S.; Jean, R.A.; Resio, B.; Pei, K.Y. Early postoperative death in extreme-risk patients: A perspective on surgical futility. Surgery 2019, 166, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Vester-Andersen, M.; Lundstrom, L.H.; Moller, M.H.; Waldau, T.; Rosenberg, J.; Moller, A.M.; The Danish Anaesthesia Database. Mortality and postoperative care pathways after emergency gastrointestinal surgery in 2904 patients: A population-based cohort study. Br. J. Anaesth. 2014, 112, 860–870. [Google Scholar] [CrossRef]
- Columbus, A.B.; Morris, M.A.; Lilley, E.J.; Harlow, A.F.; Haider, A.H.; Salim, A.; Havens, J.M. Critical differences between elective and emergency surgery: Identifying domains for quality improvement in emergency general surgery. Surgery 2018, 163, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Havens, J.M.; Peetz, A.B.; Do, W.S.; Cooper, Z.; Kelly, E.; Askari, R.; Reznor, G.; Salim, A. The excess morbidity and mortality of emergency general surgery. J. Trauma Acute Care Surg. 2015, 78, 306–311. [Google Scholar] [CrossRef]
- Saunders, D.I.; Murray, D.; Pichel, A.C.; Varley, S.; Peden, C.J. Variations in mortality after emergency laparotomy: The first report of the UK Emergency Laparotomy Network. Br. J. Anaesth. 2012, 109, 368–375. [Google Scholar] [CrossRef]
- Huddart, S.; Peden, C.J.; Swart, M.; McCormick, B.; Dickinson, M.; Mohammed, M.A.; Quiney, N.; ELPQuiC Collaborator Group; Hemmings, V.; Riga, A.; et al. Use of a pathway quality improvement care bundle to reduce mortality after emergency laparotomy. Br. J. Surg. 2015, 102, 57–66. [Google Scholar] [CrossRef]
- Tengberg, L.T.; Bay-Nielsen, M.; Bisgaard, T.; Cihoric, M.; Lauritsen, M.L.; Foss, N.B. Multidisciplinary perioperative protocol in patients undergoing acute high-risk abdominal surgery. Br. J. Surg. 2017, 104, 463–471. [Google Scholar] [CrossRef]
- Goeteyn, J.; Evans, L.A.; De Cleyn, S.; Fauconnier, S.; Damen, C.; Hewitt, J.; Ceelen, W.; Older Persons Surgical Outomes Collaborative. Frailty as a predictor of mortality in the elderly emergency general surgery patient. Acta Chir. Belg. 2015, 117, 370–375. [Google Scholar] [CrossRef]
- Torrance, A.D.; Powell, S.L.; Griffiths, E.A. Emergency Surgery in the elderly: Challenges and solutions. Open Access Emerg. Med. 2015, 7, 55–68. [Google Scholar]
- Cauley, C.E.; Panizales, M.T.; Reznor, G.; Haynes, A.B.; Havens, J.M.; Kelley, E.; Mosenthal, A.C.; Cooper, Z. Outcomes after emergency abdominal surgery in patients with advanced cancer: Opportunities to reduce complications and improve palliative care. J. Trauma Acute Care Surg. 2015, 79, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Kärkkäinen, J.M.; Lehtimäki, T.T.; Manninen, H.; Paajanen, H. Acute Mesenteric Ischemia Is a More Common Cause than Expected of Acute Abdomen in the Elderly. J. Gastrointest. Surg. 2015, 19, 1407–1414. [Google Scholar] [CrossRef] [PubMed]
- Kwok, A.C.; Lipsitz, S.R.; Bader, A.M.; Gawande, A.A. Are targeted preoperative risk prediction tools more powerful? A test of models for emergency colon surgery in the very elderly. J. Am. Coll. Surg. 2011, 213, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Cooper, Z.; Courtwright, A.; Karlage, A.; Gawande, A.; Block, S. Pitfalls in Communication That Lead to Nonbeneficial Emergency Surgery in Elderly Patients with Serious Illness. Description of the Problem and Elements of a Solution. Ann. Surg. 2014, 260, 949–957. [Google Scholar] [CrossRef] [PubMed]
- Cooper, Z. Indicated but Not Always Appropriate. Surgery in Terminally Ill Patients with Abdominal Catastrophe. Ann. Surg. 2018, 268, e4. [Google Scholar] [CrossRef]
- Howes, T.E.; Cook, T.M.; Corrigan, L.J.; Dalton, S.J.; Richards, S.K.; Peden, C.J. Postoperative morbidity survey, mortality and length of stay following emergency laparotomy. Anaesthesia 2015, 70, 1020–1027. [Google Scholar] [CrossRef]
- Prytherch, D.R.; Whiteley, M.S.; Higgins, B.; Weaver, P.C.; Prout, W.G.; Powell, S.J. POSSUM and Portsmouth POSSUM for predicting mortality. Br. J. Surg. 1998, 85, 1217–1220. [Google Scholar]
- National Confidential Enquiry into Perioperative Deaths. Classification of Intervention. Available online: https://www.ncepod.org.uk/classification.html (accessed on 4 June 2019).
- Schneiderman, L.J.; Gilmer, T.; Teetzel, H.D.; Dugan, D.O.; Blustein, J.; Cranford, R.; Briggs, K.B.; Komatsu, G.I.; Goodman-Crews, P.; Cohn, F.; et al. Effect of ethics Consultations on Nonbeneficial Life-Sustaining Treatments in the Intensive Care Setting. J. Am. Med. Assoc. 2003, 290, 1166. [Google Scholar] [CrossRef]
- Parmar, K.L.; Pearce, L.; Farrell, I.; Hewitt, J.; Moug, S. Influence of frailty in older patients undergoing emergency laparotomy: A UK-based observational study. BMJ Open 2017, 7, e017928. [Google Scholar] [CrossRef]
- Lin, H.S.; Watts, J.N.; Peel, N.M.; Hubbard, R.E. Frailty and post-operative outcomes in older surgical patients: A systematic review. BMC Geriatr. 2016, 16, 157. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. Can. Med. Assoc. J. 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Basta, Y.; Bolle, S.; Fockens, P.; Tytgat, K.M.A.J. The Value of Multidisciplinary Team Meetings for Patients with Gastrointestinal Malignancies: A Systematic Review. Ann. Surg. Oncol. 2017, 24, 2669–2678. [Google Scholar] [CrossRef] [PubMed]
- Pillay, B.; Wootten, A.C.; Crowe, H.; Corcoran, N.; Tran, B.; Bowden, P.; Crowe, J.; Costello, A.J. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat. Rev. 2016, 42, 56–72. [Google Scholar] [CrossRef] [PubMed]
- Richards, S.K.; Cook, T.M.; Dalton, S.J.; Peden, C.J.; Howes, T.E. The ‘Bath Boarding Card’: A novel tool for improving pre-operative care for emergency laparotomy patients. Anaesthesia 2016, 71, 974–976. [Google Scholar] [CrossRef][Green Version]
- Cooper, Z.; Lilley, E.J.; Bollens-Lund, E.; Mitchell, S.L.; Ritchie, C.S.; Lipstiz, S.R.; Kelley, A.S. High Burden of Palliative Care Needs of Older Adults During Emergency Major Abdominal Surgery. J. Am. Geriatr. Soc. 2018, 66, 2072–2078. [Google Scholar] [CrossRef]
- Cooper, Z.; Scott, J.W.; Rosenthal, R.A.; Mitchell, S.L. Emergency Major Abdominal Surgical Procedures in Older Adults: A Systematic Review of Mortality and Functional Outcomes. J. Am. Geriatr. Soc. 2015, 63, 2563–2571. [Google Scholar] [CrossRef]
- Schwarze, M.L.; Bradley, C.T.; Brasel, K.J. Surgical ‘buy’ in: The contractual relationship between surgeons and patients that influences decisions regarding life-supporting therapy. Crit. Care Med. 2010, 38, 843–848. [Google Scholar] [CrossRef]
- Schneiderman, L.J. Defining medical futility and improving medical care. J. Bioeth. Inq. 2011, 8, 123–131. [Google Scholar] [CrossRef]
- Shay, A.; Elston Lafata, J. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med. Decis. Mak. 2015, 35, 114–131. [Google Scholar] [CrossRef]
- Rubin, E.B.; Buehler, A.E.; Halpen, S.D. States Worse Than Death Among Hospitalized Patients With Serious Illnesses. JAMA Int. Med. 2016, 176, 1557–1558. [Google Scholar] [CrossRef]
- Spatz, E.S.; Krumholz, H.M.; Moulton, B.W. Prime Time for Shared Decision Making. J. Am. Med. Assoc. 2017, 317, 1309–1310. [Google Scholar] [CrossRef] [PubMed]
- McIlveen, E.C.; Wright, E.; Shaw, M.; Edwards, J.; Vella, M.; Quasim, T.; Moug, S.J. A prospective cohort study characterising patients declined emergency laparotomy: Survival in the ‘NoLap’ population. Anaesthesia 2020, 75, 54–72. [Google Scholar] [CrossRef] [PubMed]


| “All Others” (n = 13,434) | “Early Deaths” (n =519) | p-Value | |
|---|---|---|---|
| Mean Age (IQR) | 68 (54–78) | 75 (67–83) | <0.0001 |
| Gender | |||
| Male (%) | 6284 (47%) | 250 (48%) | 0.53 |
| Female (%) | 7150 (53%) | 269 (52%) | |
| Lactate (IQR) | 1.3 (1.0–2.1) | 3.6 (1.7–7.1) | <0.0001 |
| Pre-op P-POSSUM mortality (range) | 6.2 (3.5–18.9) | 54.2 (23.4–80.6) | <0.0001 |
| Post-op P-POSSUM mortality (range) | 6.5 (2.5–18.9) | 53.5 (27.1–80.8) | <0.0001 |
| ASA-PS (range) | 3 (2–3) | 4 (3–4) | <0.0001 |
| Creatinine (range) | 75 (60–97) | 115 (81–165) | <0.0001 |
| Sodium (range) | 137 (134–139) | 136 (132–140) | 0.01 |
| WCC (range) | 11.0 (7.8–15.2) | 11.7 (6.8–18.0) | 0.15 |
| Systolic BP (range) | 127 (112–140) | 110 (90–130) | <0.0001 |
| Heart rate | 88 (77–100) | 100 (88–120) | <0.0001 |
| GCS (range) | 15 (15–15) | 15 (14–15) | <0.0001 |
| Potassium (range) | 4.1 (3.8–4.5) | 4.2 (3.8–4.8) | <0.0001 |
| “Early Deaths” | “All Others” | p-Value | |
|---|---|---|---|
| Number | 519 | 13,434 | |
| Preoperative lactate measured | 89.2% | 69.9% | <0.0001 |
| Time from admission to surgery (median) Time from admission to surgery (mean) | 25 h – – – – 4.5 days | 34 h – – – – 3.4 days | 0.07 – – – – <0.0001 |
| Antibiotic therapy administered at least 6 h prior to surgery [2] | 32.1% | 28.4% | 0.06 |
| Preoperative CT scan performed | 83.4% | 86.1% | 0.09 |
| Met NCEPOD-based target of surgery <2 h [19] | 44.1% | 55.0% | <0.0001 |
| Intraoperative goal-directed fluid therapy | 70.3% | 64.0% | 0.003 |
| Postoperative critical care admission | 90.8% | 88.6% | <0.0001 |
| Consultant/attending surgeon present for operation | 93.3% | 88.6% | 0.001 |
| Consultant/attending anesthesiologist present for operation | 90.8% | 81.9% | <0.0001 |
| Positive Predictors of “Early” Deaths | Negative Predictors of “Early” Deaths |
|---|---|
| Age | Systolic blood pressure |
| Log of postoperative P-POSSUM | Glasgow Coma Score |
| ASA-PS score | Log of time to theater |
| Log of creatinine | |
| A surgical finding of intestinal ischemia | |
| A surgical finding of perforation of the small bowel |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aggarwal, G.; Broughton, K.J.; Williams, L.J.; Peden, C.J.; Quiney, N. Early Postoperative Death in Patients Undergoing Emergency High-Risk Surgery: Towards a Better Understanding of Patients for Whom Surgery May not Be Beneficial. J. Clin. Med. 2020, 9, 1288. https://doi.org/10.3390/jcm9051288
Aggarwal G, Broughton KJ, Williams LJ, Peden CJ, Quiney N. Early Postoperative Death in Patients Undergoing Emergency High-Risk Surgery: Towards a Better Understanding of Patients for Whom Surgery May not Be Beneficial. Journal of Clinical Medicine. 2020; 9(5):1288. https://doi.org/10.3390/jcm9051288
Chicago/Turabian StyleAggarwal, Geeta, Katherine J. Broughton, Linda J. Williams, Carol J. Peden, and Nial Quiney. 2020. "Early Postoperative Death in Patients Undergoing Emergency High-Risk Surgery: Towards a Better Understanding of Patients for Whom Surgery May not Be Beneficial" Journal of Clinical Medicine 9, no. 5: 1288. https://doi.org/10.3390/jcm9051288
APA StyleAggarwal, G., Broughton, K. J., Williams, L. J., Peden, C. J., & Quiney, N. (2020). Early Postoperative Death in Patients Undergoing Emergency High-Risk Surgery: Towards a Better Understanding of Patients for Whom Surgery May not Be Beneficial. Journal of Clinical Medicine, 9(5), 1288. https://doi.org/10.3390/jcm9051288