Lipidomics Reveals Reduced Inflammatory Lipid Species and Storage Lipids after Switching from EFV/FTC/TDF to RPV/FTC/TDF: A Randomized Open-Label Trial


 , , and
, , and
Abstract
1. Introduction
2. Patients and Methods
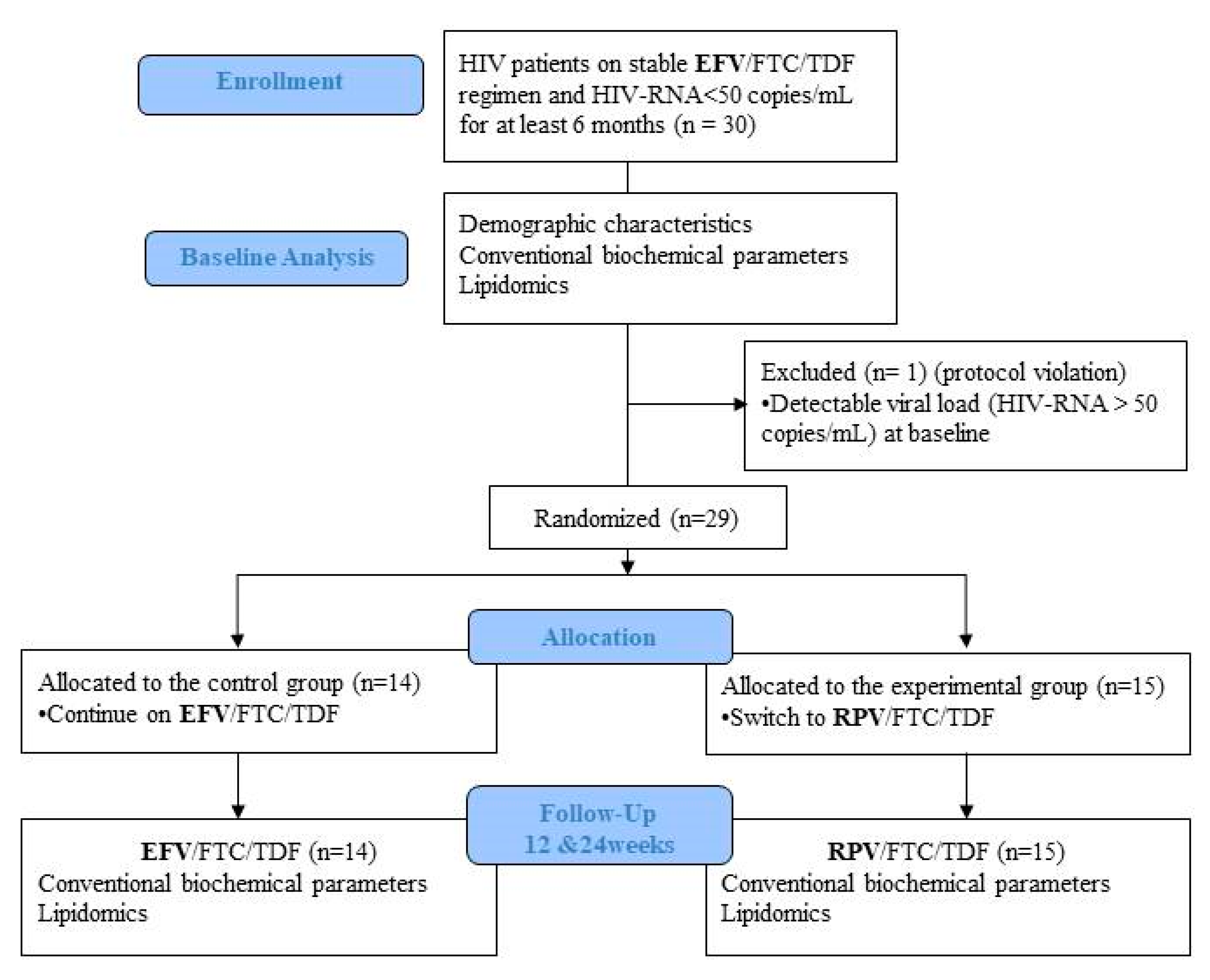
2.1. Study Design and Participants
2.2. Demographic Characteristics and Conventional Biochemical Parameters
2.3. Lipidomics
2.4. OWLiver® Care and OWLiver® Test
2.5. Statistical Analyses
3. Results
3.1. Patient Characteristics
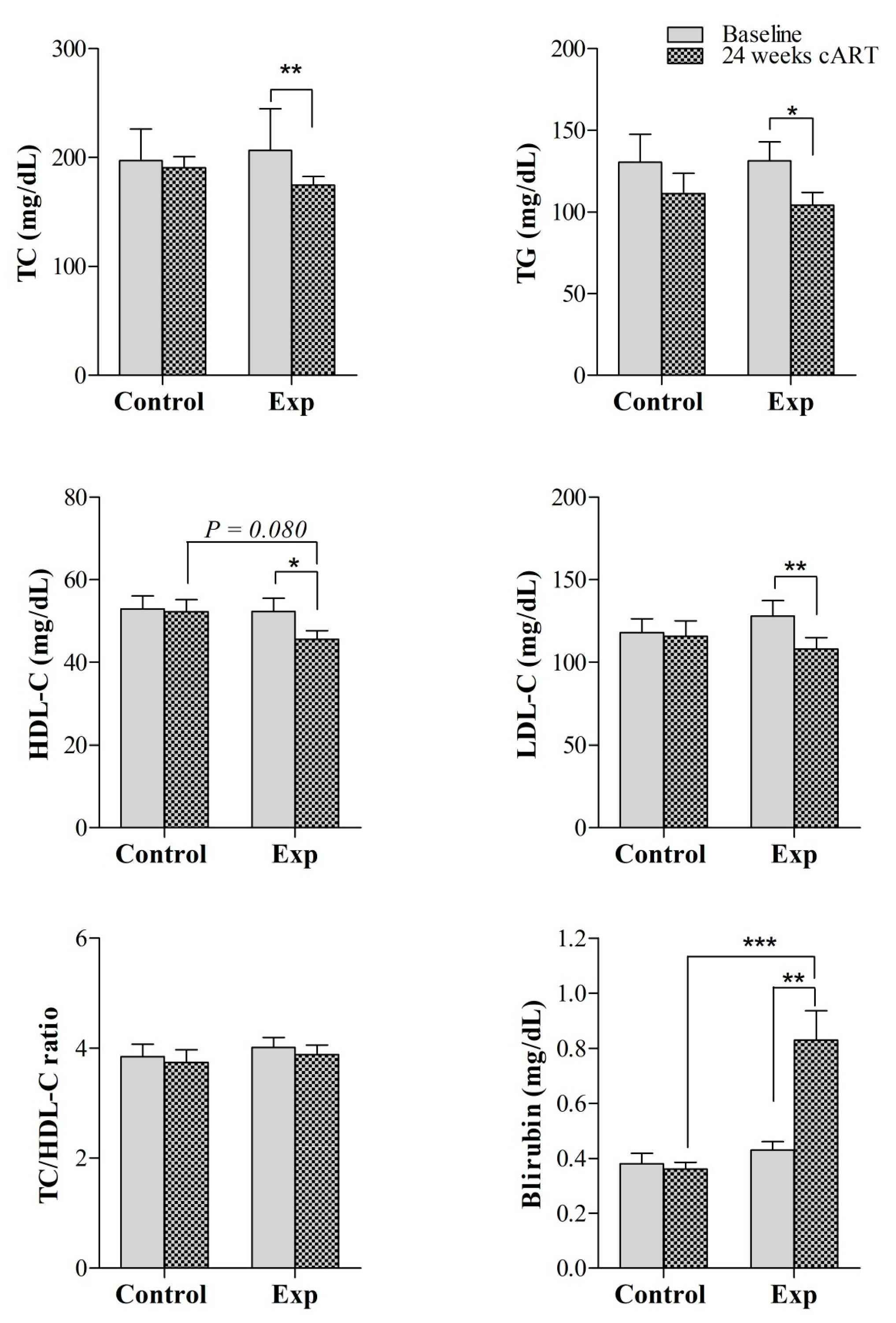
3.2. Conventional Biochemical Parameters
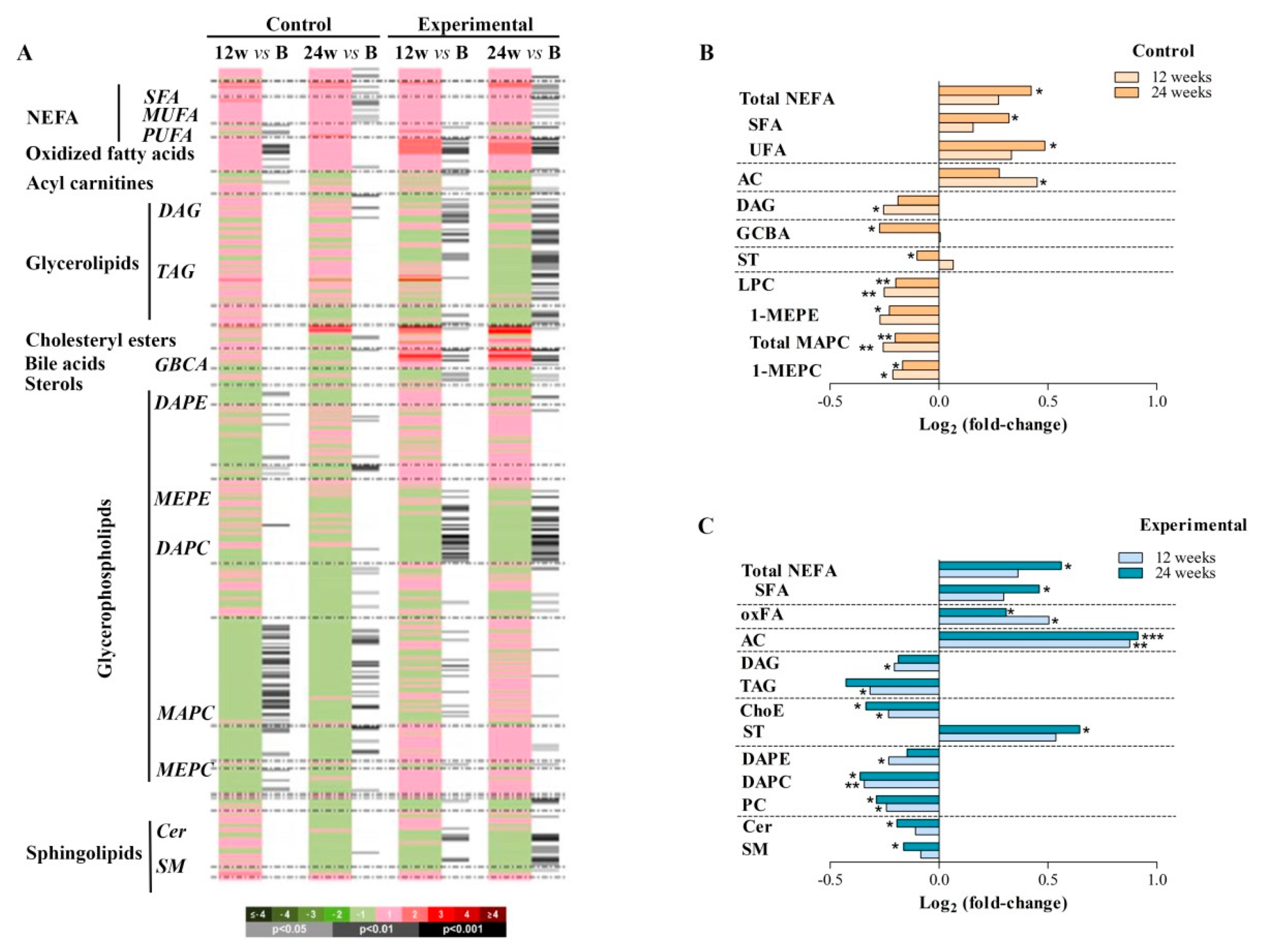
3.3. Using Efavirenz or Rilpivirine in ART has a Different Effect on Lipid Metabolism
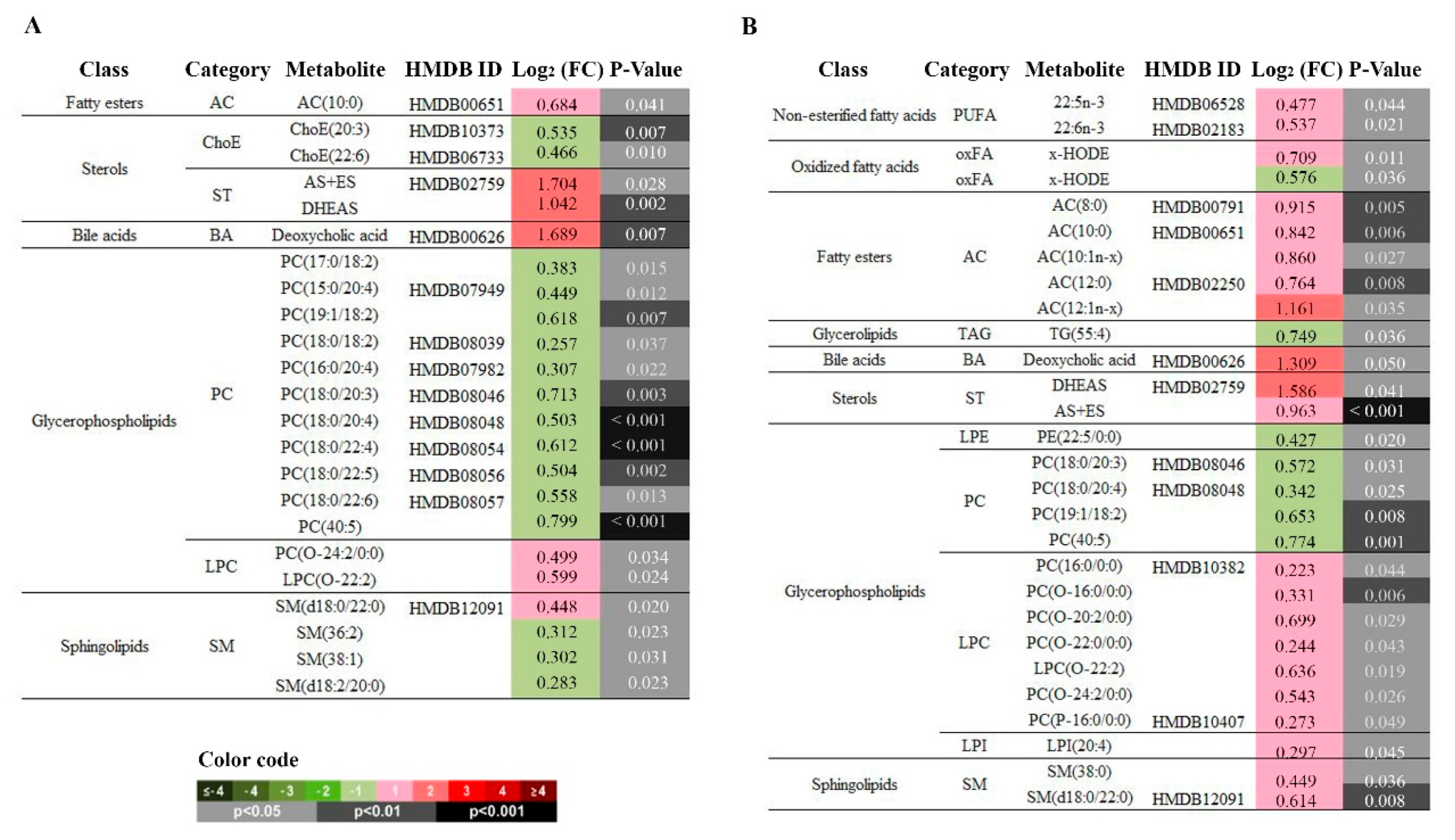
3.4. Storage Lipids Decrease when Using RPV in Co-Formulated TDF/FTC ART Therapy
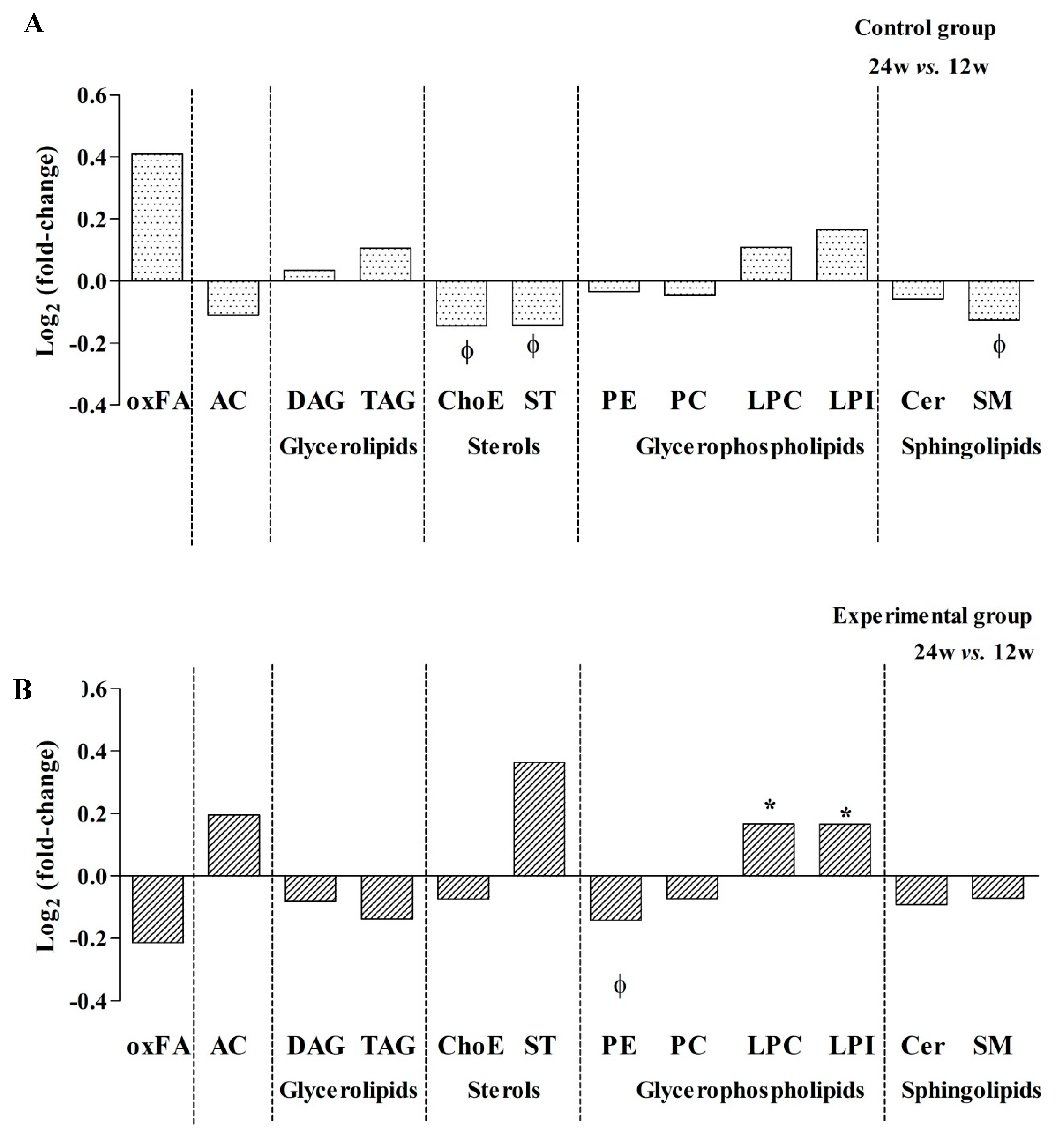
3.5. Effect of switching from EFV to RPV: decreased PCs but increased LPCs and ACs
3.6. Good Correlation between Lipidomics and Conventional Laboratory Measurements
3.7. Evaluation of non-Alcoholic Fatty Liver Disease using Plasma Samples
3.8. Effectiveness and Adverse Events
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lewden, C.; Bouteloup, V.; De Wit, S.; Sabin, C.; Mocroft, A.; Wasmuth, J.C.; van Sighem, A.; Kirk, O.; Obel, N.; Panos, G.; et al. All-cause mortality in treated HIV-infected adults with CD4 >=500/mm3 compared with the general population: Evidence from a large European observational cohort collaboration. Int. J. Epidemiol. 2011, 41, 433–445. [Google Scholar] [PubMed]
- Rodger, A.J.; Lodwick, R.; Schechter, M.; Deeks, S.; Amin, J.; Gilson, R.; Paredes, R.; Bakowska, E.; Engsig, F.N.; Phillips, A. Mortality in well controlled HIV in the continuous antiretroviral therapy arms of the SMART and ESPRIT trials compared with the general population. AIDS 2013, 27, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Ballocca, F.; D’Ascenzo, F.; Gili, S.; Grosso Marra, W.; Gaita, F. Cardiovascular disease in patients with HIV. Trends Cardiovasc. Med. 2017, 27, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.; Feinstein, M.J. Coronary Artery Disease Manifestations in HIV: What, How, and Why. Can. J. Cardiol. 2019, 35, 270–279. [Google Scholar] [CrossRef]
- Hemkens, L.G.; Bucher, H.C. HIV infection and cardiovascular disease. Eur. Heart J. 2014, 35, 1373–1381. [Google Scholar] [CrossRef]
- Lonardo, A.; Ballestri, S.; Guaraldi, G.; Nascimbeni, F.; Romagnoli, D.; Zona, S.; Targher, G. Fatty liver is associated with an increased risk of diabetes and cardiovascular disease-Evidence from three different disease models: NAFLD, HCV and HIV. World J. Gastroenterol. 2016, 22, 9674–9693. [Google Scholar] [CrossRef]
- Sax, P.E.; Erlandson, K.M.; Lake, J.E.; McComsey, G.A.; Orkin, C.; Esser, S.; Brown, T.T.; Rockstroh, J.K.; Wei, X.; Carter, C.C.; et al. Weight Gain Following Initiation of Antiretroviral Therapy: Risk Factors in Randomized Comparative Clinical Trials. Clin. Infectious Diseases 2019, 1–11. [Google Scholar] [CrossRef]
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Department of Health and Human Services. Available online: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf (accessed on 10 March 2020).
- European AIDS Clinical Society (EACS) guidelines for the Treatment of Adult HIV-Positive Persons. Version 10.0 November 2019. Available online: https://www.eacsociety.org/files/2019_guidelines-10.0_final.pdf (accessed on 10 March 2020).
- Gwag, T.; Meng, Z.; Sui, Y.; Helsley, R.N.; Park, S.H.; Wang, S.; Greenberg, R.N.; Zhou, C. Non-Nucleoside Reverse Transcriptase Inhibitor Efavirenz Activates PXR to Induce Hypercholesterolemia and Hepatic Steatosis. J Hepatol. 2019, 70, 930–940. [Google Scholar] [CrossRef]
- Dalwadi, D.A.; Kim, S.; Amdani, S.M.; Chen, Z.; Huang, R.-Q.; Schetz, J.A. HHS Public AccessMolecular mechanisms of serotonergic action of the HIV-1 antiretroviral efavirenz. Pharm. Res. 2016, 110, 10–24. [Google Scholar] [CrossRef]
- Blas-García, A.; Polo, M.; Alegre, F.; Funes, H.A.; Martínez, E.; Apostolova, N.; Esplugues, J.V. Lack of mitochondrial toxicity of darunavir, raltegravir and rilpivirine in neurons and hepatocytes: A comparison with efavirenz. J. Antimicrob. Chemother. 2014, 69, 2995–3000. [Google Scholar] [CrossRef]
- Behrens, G.; Rijnders, B.; Nelson, M.; Orkin, C.; Cohen, C.; Mills, A.; Elion, R.A.; Vanveggel, S.; Stevens, M.; Rimsky, L.; et al. Rilpivirine Versus Efavirenz with Emtricitabine/Tenofovir Disoproxil Fumarate in Treatment-Naïve HIV-1–Infected Patients with HIV-1 RNA ≤100,000 Copies/mL: Week 96 Pooled ECHO/THRIVE Subanalysis. AIDS Patient Care STDS 2014, 28, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Tebas, P.; Sension, M.; Arribas, J.; Duiculescu, D.; Florence, E.; Hung, C.C.; Wilkin, T.; Vanveggel, S.; Stevens, M.; Deckx, H. Lipid levels and changes in body fat distribution in treatment-naive, HIV-1-infected adults treated with rilpivirine or efavirenz for 96 weeks in the ECHO and THRIVE trials. Clin. Infect. Dis. 2014, 59, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Thamrongwonglert, P.; Chetchotisakd, P.; Anunnatsiri, S.; Mootsikapun, P. Improvement of lipid profiles when switching from efavirenz to rilpivirine in HIV-infected patients with dyslipidemia. HIV Clin. Trials 2016, 17, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Taramasso, L.; Tatarelli, P.; Ricci, E.; Madeddu, G.; Menzaghi, B.; Squillace, N.; De Socio, G.V.; Martinelli, C.; Gulminetti, R.; Maggi, P.; et al. Improvement of lipid profile after switching from efavirenz or ritonavir-boosted protease inhibitors to rilpivirine or once-daily integrase inhibitors: Results from a large observational cohort study (SCOLTA). BMC Infect. Dis. 2018, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hagins, D.; Orkin, C.; Daar, E.S.; Mills, A.; Brinson, C.; DeJesus, E.; Post, F.A.; Morales-Ramirez, J.; Thompson, M.; Osiyemi, O.; et al. Switching to coformulated rilpivirine (RPV), emtricitabine (FTC) and tenofovir alafenamide from either RPV, FTC and tenofovir disoproxil fumarate (TDF) or efavirenz, FTC and TDF: 96-week results from two randomized clinical trials. HIV Med. 2018, 19, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.; Trevillyan, J.M.; Fatou, B.; Cinel, M.; Weir, J.M.; Hoy, J.F.; Meikle, P.J. Plasma lipidomic profiling of treated HIV-positive individuals and the implications for cardiovascular risk prediction. PLoS ONE 2014, 9, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bowman, E.R.; Kulkarni, M.; Gabriel, J.; Cichon, M.J.; Riedl, K.; Belury, M.A.; Lake, J.E.; Richardson, B.; Cameron, C.; Cameron, M.; et al. Altered Lipidome Composition Is Related to Markers of Monocyte and Immune Activation in Antiretroviral Therapy Treated Human Immunodeficiency Virus (HIV) Infection and in Uninfected Persons. Front. Immunol. 2019, 10, 785. [Google Scholar] [CrossRef]
- Belury, M.A.; Bowman, E.; Gabriel, J.; Snyder, B.; Kulkarni, M.; Palettas, M.; Mo, X.; Lake, J.E.; Zidar, D.; Sieg, S.F.; et al. Prospective Analysis of Lipid Composition Changes with Antiretroviral Therapy and Immune Activation in Persons Living with HIV. Pathog. Immun. 2017, 2, 376. [Google Scholar] [CrossRef]
- Trevillyan, J.M.; Wong, G.; Puls, R.; Petoumenos, K.; Emery, S.; Mellett, N.A.; Mundra, P.A.; Meikle, P.J.; Hoy, J.F. Changes in plasma lipidome following initiation of antiretroviral therapy. PLoS ONE 2018, 13, e0202944. [Google Scholar] [CrossRef]
- Martínez-Arranz, I.; Mayo, R.; Pérez-Cormenzana, M.; Mincholé, I.; Salazar, L.; Alonso, C.; Mato, J.M. Enhancing metabolomics research through data mining. J. Proteom. 2015, 127, 275–288. [Google Scholar] [CrossRef]
- Barr, J.; Caballería, J.; Martínez-Arranz, I.; Domínguez-Díez, A.; Alonso, C.; Muntané, J.; Pérez-Cormenzana, M.; García-Monzón, C.; Mayo, R.; Martín-Duce, A.; et al. Obesity dependent metabolic signatures associated with nonalcoholic fatty liver disease progression. J. Proteome Res. 2012, 11, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Fahy, E.; Subramaniam, S.; Brown, H.; Glass, C.; Merrill, A.; Murphy, R.; Raetz, C.; Russell, D.; Seyama, Y.; Shaw, W.; et al. A Comprehensive Classification System for Lipids. J. Lipid Res. 2005, 46, 839–861. [Google Scholar] [CrossRef] [PubMed]
- Mayo, R.; Crespo, J.; Martínez-Arranz, I.; Banales, J.M.; Arias, M.; Mincholé, I.; Aller de la Fuente, R.; Jimenez-Agüero, R.; Alonso, C.; de Luis, D.A.; et al. Metabolomic-based noninvasive serum test to diagnose nonalcoholic steatohepatitis: Results from discovery and validation cohorts. Hepatol. Commun. 2018, 2, 807–820. [Google Scholar] [CrossRef] [PubMed]
- Bril, F.; Millán, L.; Kalavalpalli, S.; McPhaul, M.J.; Caulfield, M.P.; Martinez-Arranz, I.; Alonso, C.; Betes, P.O.; Mato, J.M.; Cusi, K. Use of a Metabolomic Approach to Non-invasively Diagnose Nonalcoholic Fatty Liver Disease in Patients with Type 2 Diabetes Mellitus. Diabetes Obes Metab. 2018, 20, 1702–1709. [Google Scholar] [CrossRef] [PubMed]
- Villoslada, P.; Alonso, C.; Agirrezabal, I.; Kotelnikova, E.; Zubizarreta, I.; Pulido-Valdeolivas, I.; Saiz, A.; Comabella, M.; Montalban, X.; Villar, L.; et al. Metabolomic signatures associated with disease severity in multiple sclerosis. Neurol. Neuroimmunol. Neuroinflammation 2017, 4, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Banales, J.M.; Iñarrairaegui, M.; Arbelaiz, A.; Milkiewicz, P.; Muntané, J.; Muñoz-Bellvis, L.; La Casta, A.; Gonzalez, L.M.; Arretxe, E.; Alonso, C.; et al. Serum Metabolites as Diagnostic Biomarkers for Cholangiocarcinoma, Hepatocellular Carcinoma, and Primary Sclerosing Cholangitis. Hepatology 2019, 0, 1–16. [Google Scholar] [CrossRef]
- Cassol, E.; Misra, V.; Holman, A.; Kamat, A.; Morgello, S.; Gabuzda, D. Plasma metabolomics identifies lipid abnormalities linked to markers of inflammation, microbial translocation, and hepatic function in HIV patients receiving protease inhibitors. BMC Infect. Dis. 2013, 13, 203. [Google Scholar] [CrossRef]
- Fernandez, C.; Sandin, M.; Sampaio, J.L.; Almgren, P.; Narkiewicz, K.; Hoffmann, M.; Hedner, T.; Wahlstrand, B.; Simons, K.; Shevchenko, A.; et al. Plasma Lipid Composition and Risk of Developing Cardiovascular Disease. PLoS ONE 2013, 8, e71846. [Google Scholar] [CrossRef]
- Rai, S.; Bhatnagar, S. Novel Lipidomic Biomarkers in Hyperlipidemia and Cardiovascular Diseases: An Integrative Biology Analysis. Omics A J. Integr. Biol. 2017, 21, 132–142. [Google Scholar] [CrossRef]
- Preuss, C.; Jelenik, T.; Bódis, K.; Müssig, K.; Burkart, V.; Szendroedi, J.; Roden, M.; Markgraf, D.F. A New Targeted Lipidomics Approach Reveals Lipid Droplets in Liver, Muscle and Heart as a Repository for Diacylglycerol and Ceramide Species in Non-Alcoholic Fatty Liver. Cells 2019, 8, 277. [Google Scholar] [CrossRef]
- Orešič, M.; Hyötyläinen, T.; Kotronen, A.; Gopalacharyulu, P.; Nygren, H.; Arola, J.; Castillo, S.; Mattila, I.; Hakkarainen, A.; Borra, R.J.H.; et al. Prediction of non-alcoholic fatty-liver disease and liver fat content by serum molecular lipids. Diabetologia 2013, 56, 2266–2274. [Google Scholar] [CrossRef] [PubMed]
- Kasumov, T.; Li, L.; Li, M.; Gulshan, K.; Kirwan, J.P.; Liu, X.; Previs, S.; Willard, B.; Smith, J.D.; McCullough, A. Ceramide as a mediator of non-alcoholic fatty liver disease and associated atherosclerosis. PLoS ONE 2015, 10, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Millan, J.; Pinto, X.; Munoz, A.; Zuniga, M.; Rubies-Prat, J.; Pallardo, L.F.; Masana, L.; Mangas, A.; Hernandez-Mijares, A.; Gonzalez-Santos, P.; et al. Lipoprotein ratios: Physiological significance and clinical usefulness in cardiovascular prevention. Vasc. Health Risk Manag. 2009, 5, 757–765. [Google Scholar] [PubMed]
- Sniderman, A.D.; Junger, I.; Holme, I.; Aastveit, A.; Walldius, G. Errors that result from using the TC/HDL C ratio rather than the apoB/apoA-I ratio to identify the lipoprotein-related risk of vascular disease. J. Intern. Med. 2006, 259, 455–461. [Google Scholar] [CrossRef]
- Maggi, P.; Di Biagio, A.; Rusconi, S.; Cicalini, S.; D’Abbraccio, M.; d’Ettorre, G.; Martinelli, C.; Nunnari, G.; Sighinolfi, L.; Spagnuolo, V.; et al. Cardiovascular risk and dyslipidemia among persons living with HIV: A review. BMC Infect. Dis. 2017, 17, 1–17. [Google Scholar] [CrossRef]
- Suh, S.; Cho, Y.R.; Park, M.K.; Kim, D.K.; Cho, N.H.; Lee, M.K. Relationship between serum bilirubin levels and cardiovascular disease. PLoS ONE 2018, 13, 1–9. [Google Scholar] [CrossRef]
- Akerele, O.A.; Cheema, S.K. Fatty acyl composition of lysophosphatidylcholine is important in atherosclerosis. Med. Hypotheses 2015, 85, 754–760. [Google Scholar] [CrossRef]
- Law, S.H.; Chan, M.L.; Marathe, G.K.; Parveen, F.; Chen, C.H.; Ke, L.Y. An updated review of lysophosphatidylcholine metabolism in human diseases. Int. J. Mol. Sci. 2019, 20, 1149. [Google Scholar] [CrossRef]
- Jiang, X.C.; Paultre, F.; Pearson, T.A.; Reed, R.G.; Francis, C.K.; Lin, M.; Berglund, L.; Tall, A.R. Plasma sphingomyelin level as a risk factor for coronary artery disease. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 2614–2618. [Google Scholar] [CrossRef]
- Hilvo, M.; Meikle, P.J.; Pedersen, E.R.; Tell, G.S.; Dhar, I.; Brenner, H.; Schöttker, B.; Lääperi, M.; Kauhanen, D.; Koistinen, K.M.; et al. Development and validation of a ceramide- and phospholipid-based cardiovascular risk estimation score for coronary artery disease patients. Eur. Heart J. 2020, 441, 371–380. [Google Scholar] [CrossRef]
- Nicolaides, N.C.; Kyratzi, E.; Lamprokostopoulou, A.; Chrousos, G.P.; Charmandari, E. Stress, the stress system and the role of glucocorticoids. NeuroImmunoModulation 2014, 22, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Walker, B.R. Glucocorticoids and cardiovascular disease. Eur. J. Endocrinol. 2007, 157, 545–559. [Google Scholar] [CrossRef] [PubMed]
- Koorneef, L.L.; Van Den Heuvel, J.K.; Kroon, J.; Boon, M.R.; Hoen, P.A.C.; Hettne, K.M.; Van De Velde, N.M.; Kolenbrander, K.B.; Streefland, T.C.M.; Mol, I.M.; et al. Selective Glucocorticoid Receptor Modulation Prevents and Reverses Nonalcoholic Fatty Liver Disease in Male Mice. Endocrinology 2018, 159, 3925–3936. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Title | Experimental (n = 15) | Control (n = 14) | Total (n = 29) | p- value |
|---|---|---|---|---|
| Age, years | 45 (36–52) | 44 (35–45) | 44 (36–48) | 0.373 |
| Male | 12 (80) | 13 (87) | 25 (83) | 1 |
| BMI, kg/m2 | 23.9 (21.5–24.8) | 22.7 (20.9–24.4] | 23.8 (21.5–24.6] | 0.361 |
| Race/ethnicity | 0.597 | |||
| Hispanic | 1 (7) | 3 (20) | 4 (13) | |
| Caucasian | 13 (87) | 12 (80) | 25 (83) | |
| African | 1 (7) | 0 (0) | 1 (3) | |
| Current smoker | 6 (40) | 5 (33) | 11 (37) | 0.705 |
| HIV infection, years | 10 (7–13) | 9 (7–16) | 10 (7–15) | 0.604 |
| HIV risk factor | 1 | |||
| Heterosexual | 4 (27) | 4 (27) | 8 (27) | |
| MSM | 10 (67) | 9 (60) | 19 (63) | |
| Injection drug abuse | 0 (0) | 1 (7) | 1 (3) | |
| Other | 1 (7) | 1 (7) | 1 (3) | |
| Prior AIDS | 3 (20) | 1 (7) | 4 (13) | 0.598 |
| Time on ART, years | 7 (4–13) | 8 (5–16) | 7 (5–14) | 0.330 |
| Time on EFV/FTC/TDF, years | 6 (4–8) | 6 (4–9) | 6 (4–8) | 0.756 |
| Nadir CD4+ count, cells/µL | 224 (109–400) | 240 (168–365) | 236 (139–390) | 0.576 |
| Current CD4+ count, cells/µL | 730 (560–950) | 740 (540–1000) | 740 (540–950) | 0.678 |
| Current CD8+ count, cells/µL | 675 (510–760) | 630 (490–830) | 660 (510–820) | 0.861 |
| Lipid parameters | ||||
| TC, mg/dL | 214 (189–240) | 200 (184–226) | 207 (185–234) | 0.175 |
| LDL-c, mg/dL | 137 (122–157) | 126 (93–147) | 133 (96–151) | 0.141 |
| HDL-c, mg/dL | 58 (40–64) | 54 (41–64) | 57 (41–64) | 0.927 |
| Triglycerides, mg/dL | 122 (103–141] | 115 (87–166) | 117 (100–152) | 0.646 |
| apoA, g/dL | 149 (140–178] | 150 (128–172) | 149 (133–172) | 0.468 |
| apoB, g/dL | 94 (83–108] | 88 (70–100) | 91 (74–103) | 0.340 |
| Other laboratory parameters | ||||
| ALT, UI/L | 29 (22–38] | 23 (20–31) | 23 (21–32) | 0.197 |
| ALP, UI/L | 116 (80–135] | 94.50 (84–134) | 98 (80–134) | 0.854 |
| AST, UI/L | 22 (20–32] | 24 (20–27) | 23 (20–28) | 0.729 |
| Bilirubin, mg/dL | 0.42 (0.35–0.52] | 0.35 (0.27–0.39) | 0.38 (0.33–0.47) | 0.135 |
| GGT, UI/L | 53 (37–61] | 36 (28–66) | 45 (31–63) | 0.141 |
| Glucose, mg/dL | 92 (83–100] | 89 (83–90) | 90 (83–99) | 0.596 |
| Insulin, mU/L | 15.0 (10.4–17.8) | 11.6 (7.6–28.1) | 14.2 (9.3–22.7) | 0.604 |
| Total protein, g/dL | 7.20 (7.00–7.60) | 7.20 (7.00–7.50) | 7.20 (7.00–7.55) | 0.854 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Curran, A.; Rull, A.; Navarro, J.; Vidal-González, J.; Martin-Castillo, M.; Burgos, J.; Falcó, V.; Ribera, E.; Torrella, A.; Planas, B.; et al. Lipidomics Reveals Reduced Inflammatory Lipid Species and Storage Lipids after Switching from EFV/FTC/TDF to RPV/FTC/TDF: A Randomized Open-Label Trial. J. Clin. Med. 2020, 9, 1246. https://doi.org/10.3390/jcm9051246
Curran A, Rull A, Navarro J, Vidal-González J, Martin-Castillo M, Burgos J, Falcó V, Ribera E, Torrella A, Planas B, et al. Lipidomics Reveals Reduced Inflammatory Lipid Species and Storage Lipids after Switching from EFV/FTC/TDF to RPV/FTC/TDF: A Randomized Open-Label Trial. Journal of Clinical Medicine. 2020; 9(5):1246. https://doi.org/10.3390/jcm9051246
Chicago/Turabian StyleCurran, Adrian, Anna Rull, Jordi Navarro, Judit Vidal-González, Mario Martin-Castillo, Joaquin Burgos, Vicenç Falcó, Esteban Ribera, Ariadna Torrella, Bibiana Planas, and et al. 2020. "Lipidomics Reveals Reduced Inflammatory Lipid Species and Storage Lipids after Switching from EFV/FTC/TDF to RPV/FTC/TDF: A Randomized Open-Label Trial" Journal of Clinical Medicine 9, no. 5: 1246. https://doi.org/10.3390/jcm9051246
APA StyleCurran, A., Rull, A., Navarro, J., Vidal-González, J., Martin-Castillo, M., Burgos, J., Falcó, V., Ribera, E., Torrella, A., Planas, B., Peraire, J., & Crespo, M. (2020). Lipidomics Reveals Reduced Inflammatory Lipid Species and Storage Lipids after Switching from EFV/FTC/TDF to RPV/FTC/TDF: A Randomized Open-Label Trial. Journal of Clinical Medicine, 9(5), 1246. https://doi.org/10.3390/jcm9051246