Arthroscopy-Assisted Corrective Osteotomy, Reduction, Internal Fixation and Strut Allograft Augmentation for Tibial Plateau Malunion or Nonunion


Abstract
1. Introduction
2. Materials and Methods
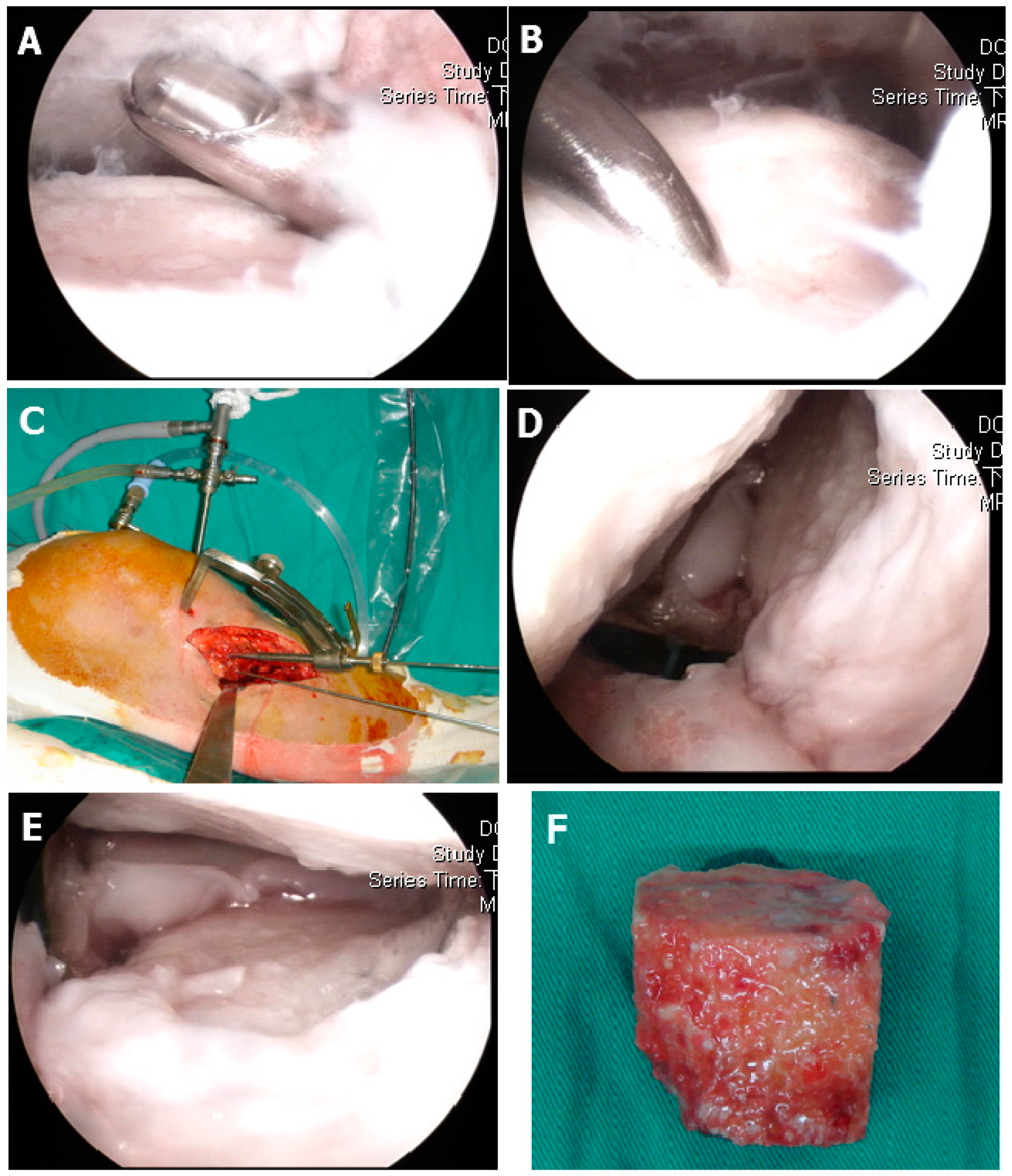
2.1. Surgical Technique
2.2. Clinical and Radiologic Assessment
2.3. Statistical Methods
3. Results
3.1. Clinical Assessment
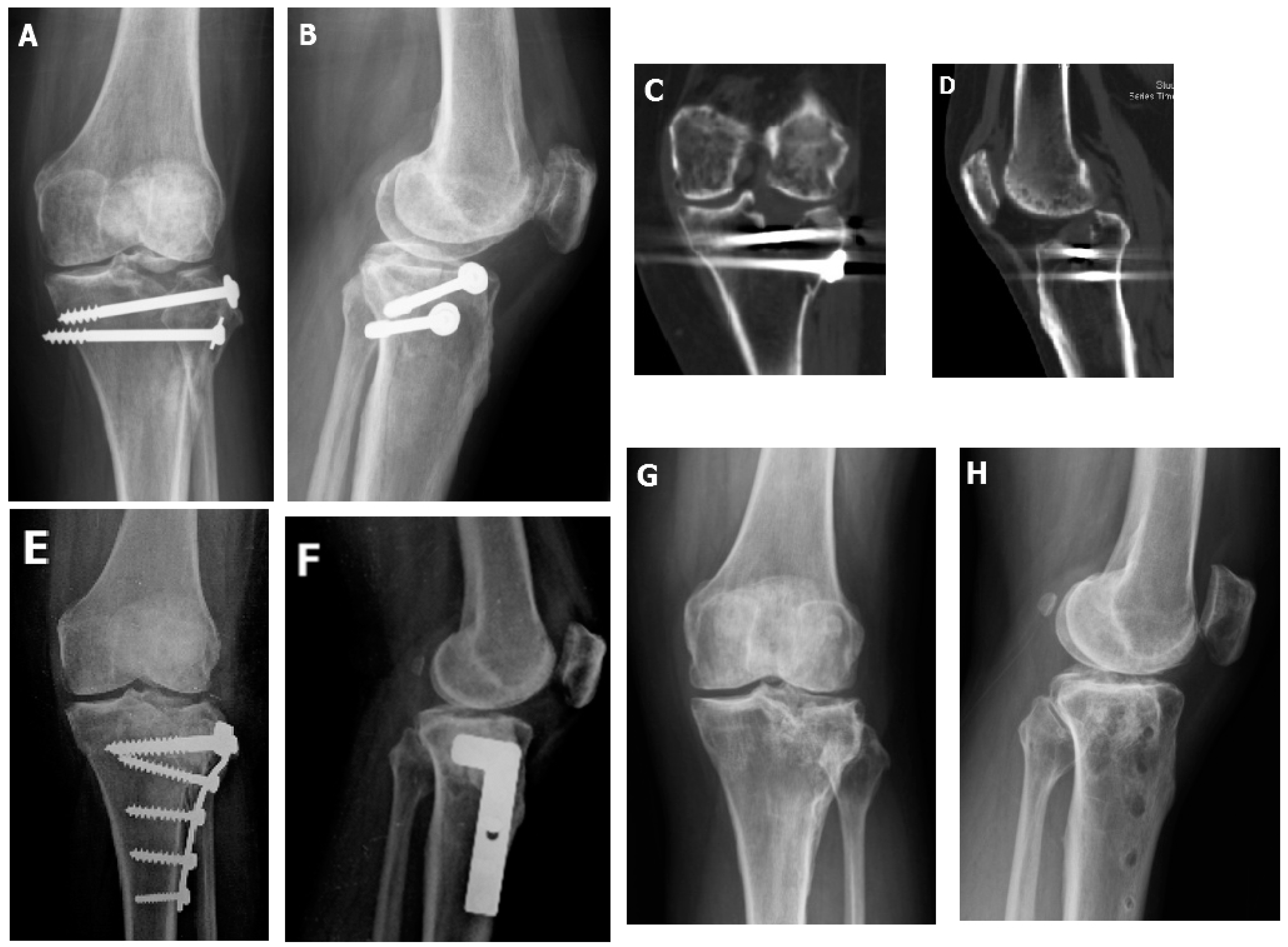
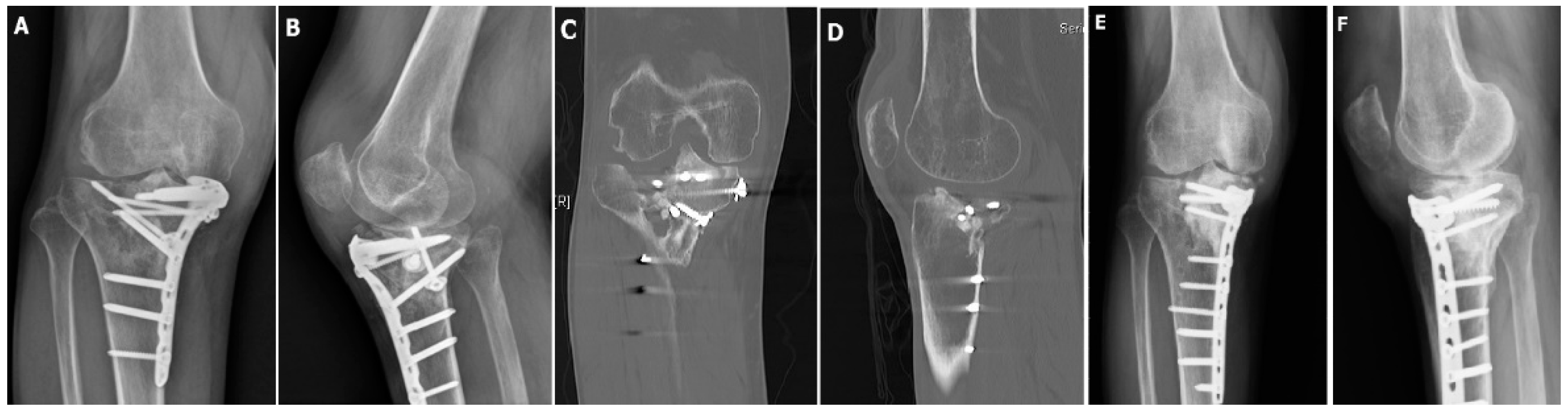
3.2. Radiologic Assessment
3.3. Associated Injuries and Procedures
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Papagelopoulos, P.J.; Partsinevelos, A.A.; Themistocleous, G.S.; Mavrogenis, A.F.; Korres, D.S.; Soucacos, P.N. Complications after tibia plateau fracture surgery. Injury 2006, 37, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.C. Salvage of proximal tibial malunion or nonunion with the use of angled blade plate. Arch. Orthop. Trauma Surg. 2006, 126, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.-H.; Cheng, C.-Y.; Chen, Y.-J.; Chao-Yu Chen, A.; Hsu, K.-Y.; Chan, Y.-S.; Chen, W.-J. Reasons for failure of surgical treatment in 25 tibial plateau fractures. Formos. J. Musculoskelet. Disord. 2012, 3, 14–18. [Google Scholar] [CrossRef]
- Kerkhoffs, G.M.; Rademakers, M.V.; Altena, M.; Marti, R.K. Combined intra-articular and varus opening wedge osteotomy for lateral depression and valgus malunion of the proximal part of the tibia. JBJS 2008, 90, 1252–1257. [Google Scholar] [CrossRef] [PubMed]
- Kerkhoffs, G.M.; Rademakers, M.V.; Altena, M.; Marti, R.K. Combined intra-articular and varus opening wedge osteotomy for lateral depression and valgus malunion of the proximal part of the tibia. Surgical technique. JBJS 2009, 91 Pt 1 (Suppl. 2), 101–115. [Google Scholar] [CrossRef]
- Saengnipanthkul, S. Uni-condyle high tibial osteotomy for malunion of medial plateau fracture: Surgical technique and case report. J. Med Assoc. Thail. Chotmaihet Thangphaet 2012, 95, 1619–1624. [Google Scholar]
- Prasad, G.; Zahn, H. Medial tibial hemi-condylar elevation osteotomy as an operative technique to treat varus mal-united tibial plateau fracture. Musculoskelet. Surg. 2012, 96, 63–66. [Google Scholar] [CrossRef]
- Singh, H.; Singh, V.R.; Yuvarajan, P.; Maini, L.; Gautam, V.K. Open wedge osteotomy of the proximal medial tibia for malunited tibial plateau fractures. J. Orthop. Surg. 2011, 19, 57–59. [Google Scholar] [CrossRef]
- Marti, R.K.; Kerkhoffs, G.M.; Rademakers, M.V. Correction of lateral tibial plateau depression and valgus malunion of the proximal tibia. Oper. Orthop. Und Traumatol. 2007, 19, 101–113. [Google Scholar] [CrossRef]
- Hung, S.S.; Chao, E.K.; Chan, Y.S.; Yuan, L.J.; Chung, P.C.; Chen, C.Y.; Lee, M.S.; Wang, C.J. Arthroscopically assisted osteosynthesis for tibial plateau fractures. J. Trauma 2003, 54, 356–363. [Google Scholar] [CrossRef]
- Chan, Y.S.; Yuan, L.J.; Hung, S.S.; Wang, C.J.; Yu, S.W.; Chen, C.Y.; Chao, E.K.; Lee, M.S. Arthroscopic-assisted reduction with bilateral buttress plate fixation of complex tibial plateau fractures. Arthrosc. J. Arthrosc. Relat. Surg. 2003, 19, 974–984. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.S.; Chiu, C.H.; Lo, Y.P.; Chen, A.C.; Hsu, K.Y.; Wang, C.J.; Chen, W.J. Arthroscopy-assisted surgery for tibial plateau fractures: 2- to 10-year follow-up results. Arthrosc. J. Arthrosc. Relat. Surg. 2008, 24, 760–768. [Google Scholar] [CrossRef]
- Suganuma, J.; Akutsu, S. Arthroscopically assisted treatment of tibial plateau fractures. Arthrosc. J. Arthrosc. Relat. Surg. 2004, 20, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Lubowitz, J.H.; Vance, K.J.; Ayala, M.; Guttmann, D.; Reid, J.B., 3rd. Interference screw technique for arthroscopic reduction and internal fixation of compression fractures of the tibial plateau. Arthrosc. J. Arthrosc. Relat. Surg. 2006, 22, 1359-e1. [Google Scholar] [CrossRef] [PubMed]
- Cetik, O.; Cift, H.; Asik, M. Second-look arthroscopy after arthroscopy-assisted treatment of tibial plateau fractures. Knee Surg. Sports Traumatol. Arthrosc. Off. J. Esska 2007, 15, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.S. Arthroscopy- assisted surgery for tibial plateau fractures. Chang. Gung. Med. J. 2011, 34, 239–247. [Google Scholar] [CrossRef]
- Van Glabbeek, F.; van Riet, R.; Jansen, N.; D’Anvers, J.; Nuyts, R. Arthroscopically assisted reduction and internal fixation of tibial plateau fractures: Report of twenty cases. Acta Orthop. Belg. 2002, 68, 258–264. [Google Scholar]
- Fowble, C.D.; Zimmer, J.W.; Schepsis, A.A. The role of arthroscopy in the assessment and treatment of tibial plateau fractures. Arthrosc. J. Arthrosc. Relat. Surg. 1993, 9, 584–590. [Google Scholar] [CrossRef]
- Guanche, C.A.; Markman, A.W. Arthroscopic management of tibial plateau fractures. Arthrosc. J. Arthrosc. Relat. Surg. 1993, 9, 467–471. [Google Scholar] [CrossRef][Green Version]
- Vangsness, C.T., Jr.; Ghaderi, B.; Hohl, M.; Moore, T.M. Arthroscopy of meniscal injuries with tibial plateau fractures. J. Bone Jt. Surg. Br. Vol. 1994, 76, 488–490. [Google Scholar] [CrossRef]
- Schatzker, J.; McBroom, R.; Bruce, D. The tibial plateau fracture. The Toronto experience 1968–1975. Clin. Orthop. Relat. Res. 1979, 138, 94–104. [Google Scholar]
- Outerbridge, R.E.; Dunlop, J.A. The problem of chondromalacia patellae. Clin. Orthop. Relat. Res. 1975, 177–196. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, P.S. Tibial condylar fractures. Impairment of knee joint stability as an indication for surgical treatment. JBJS 1973, 55, 1331–1350. [Google Scholar] [CrossRef]
- Hohl, M. Tibial condylar fractures. JBJS 1967, 49, 1455–1467. [Google Scholar] [CrossRef]
- Jensen, D.B.; Rude, C.; Duus, B.; Bjerg-Nielsen, A. Tibial plateau fractures. A comparison of conservative and surgical treatment. J. Bone Jt. Surg. Br. Vol. 1990, 72, 49–52. [Google Scholar] [CrossRef]
- Lobenhoffer, P.; Schulze, M.; Gerich, T.; Lattermann, C.; Tscherne, H. Closed reduction/percutaneous fixation of tibial plateau fractures: Arthroscopic versus fluoroscopic control of reduction. J. Orthop. Trauma 1999, 13, 426–431. [Google Scholar] [CrossRef]
- Hsu, C.J.; Chang, W.N.; Wong, C.Y. Surgical treatment of tibial plateau fracture in elderly patients. Arch. Orthop. Trauma Surg. 2001, 121, 67–70. [Google Scholar] [CrossRef]
- Gill, T.J.; Moezzi, D.M.; Oates, K.M.; Sterett, W.I. Arthroscopic reduction and internal fixation of tibial plateau fractures in skiing. Clin. Orthop. Relat. Res. 2001, 243–249. [Google Scholar] [CrossRef]
- Whittle, A.P.; Russell, T.A.; Taylor, J.C.; Lavelle, D.G. Treatment of open fractures of the tibial shaft with the use of interlocking nailing without reaming. JBJS 1992, 74, 1162–1171. [Google Scholar] [CrossRef]
- Ahlback, S. Osteoarthrosis of the knee. A radiographic investigation. Acta Radiol. Diagn. 1968, 227 (Suppl. 277), 7–72. [Google Scholar]
- Honkonen, S.E. Degenerative arthritis after tibial plateau fractures. J. Orthop. Trauma 1995, 9, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Rademakers, M.V.; Kerkhoffs, G.M.; Sierevelt, I.N.; Raaymakers, E.L.; Marti, R.K. Operative treatment of 109 tibial plateau fractures: Five- to 27-year follow-up results. J. Orthop. Trauma 2007, 21, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Scott, C.E.; Davidson, E.; MacDonald, D.J.; White, T.O.; Keating, J.F. Total knee arthroplasty following tibial plateau fracture: A matched cohort study. Bone Jt. J. 2015, 97, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Lizaur-Utrilla, A.; Collados-Maestre, I.; Miralles-Munoz, F.A.; Lopez-Prats, F.A. Total Knee Arthroplasty for Osteoarthritis Secondary to Fracture of the Tibial Plateau. A Prospective Matched Cohort Study. J. Arthroplast. 2015, 30, 1328–1332. [Google Scholar] [CrossRef]
- Houdek, M.T.; Watts, C.D.; Shannon, S.F.; Wagner, E.R.; Sems, S.A.; Sierra, R.J. Posttraumatic Total Knee Arthroplasty Continues to Have Worse Outcome Than Total Knee Arthroplasty for Osteoarthritis. J. Arthroplast. 2015. [Google Scholar] [CrossRef]
- Abdel, M.P.; von Roth, P.; Cross, W.W.; Berry, D.J.; Trousdale, R.T.; Lewallen, D.G. Total Knee Arthroplasty in Patients With a Prior Tibial Plateau Fracture: A Long-Term Report at 15 Years. J. Arthroplast. 2015, 30, 2170–2172. [Google Scholar] [CrossRef]
- Wasserstein, D.; Henry, P.; Paterson, J.M.; Kreder, H.J.; Jenkinson, R. Risk of total knee arthroplasty after operatively treated tibial plateau fracture: A matched-population-based cohort study. JBJS 2014, 96, 144–150. [Google Scholar] [CrossRef]
- Parratte, S.; Bonnevialle, P.; Pietu, G.; Saragaglia, D.; Cherrier, B.; Lafosse, J.M. Primary total knee arthroplasty in the management of epiphyseal fracture around the knee. Orthop. Traumatol. Surg. Res. Otsr 2011, 97, S87–S94. [Google Scholar] [CrossRef]
- Civinini, R.; Carulli, C.; Matassi, F.; Villano, M.; Innocenti, M. Total knee arthroplasty after complex tibial plateau fractures. La Chir. Degli Organi Di Mov. 2009, 93, 143–147. [Google Scholar] [CrossRef]
- Saleh, K.J.; Sherman, P.; Katkin, P.; Windsor, R.; Haas, S.; Laskin, R.; Sculco, T. Total knee arthroplasty after open reduction and internal fixation of fractures of the tibial plateau: A minimum five-year follow-up study. JBJS 2001, 83-a, 1144–1148. [Google Scholar] [CrossRef]
- Pagkalos, J.; Molloy, R.; Snow, M. Bi-planar intra-articular deformity following malunion of a Schatzker V tibial plateau fracture: Correction with intra-articular osteotomy using patient-specific guides and arthroscopic resection of the tibial spine bone block. Knee 2018, 25, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Newman, S.; Wang, J.; Wang, Q.; Wang, Q. Corrective Osteotomies for Complex Intra-Articular Tibial Plateau Malunions using Three-Dimensional Virtual Planning and Novel Patient-Specific Guides. J. Knee Surg. 2018, 31, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Furnstahl, P.; Vlachopoulos, L.; Schweizer, A.; Fucentese, S.F.; Koch, P.P. Complex Osteotomies of Tibial Plateau Malunions Using Computer-Assisted Planning and Patient-Specific Surgical Guides. J. Orthop. Trauma 2015, 29, e270–e276. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Type II | Type III | Type IV | Type V | Type VI | Total | |
|---|---|---|---|---|---|---|
| No. of patients (%) | 19 (32.7%) | 2 (3.4%) | 7 (12%) | 20 (34.5%) | 10 (17.2%) | 58 (100%) |
| Mean age (yr) | 49.8 ± 12.9 | 34 ± 16.9 | 49.3 ± 7.2 | 49.5 ± 13.4 | 49.2 ± 8.3 | 49 ± 11.9 |
| Gender (M/F) | 5/14 | 0/2 | 1/6 | 6/14 | 4/6 | 16/42 |
| Side (R/L) | 7/12 | 0/2 | 0/7 | 9/11 | 7/3 | 23/35 |
| Preoperative condition | ||||||
| Range of motion | 1.3 ± 3.3~102.3 ± 30.6 | 0.0 ± 0.0~110.0 ± 28.3 | 3.6 ± 6.3~115.0 ± 15.0 | 4.0 ± 7.7~93.7 ± 27.9 | 12.5 ± 16.2~84.0 ± 28.6 | 4.4 ± 9.18~98.0 ± 28.5 |
| Mean depression plateau (mm) | 15.9 ± 6.2 | 7.5 ± 3.53 | 16.4 ± 3.77 | 19.5 ± 7.7 | 20.7 ± 5.6 | 17.7 ± 6.8 |
| Mean tibiofemoral angle | 7.3 ± 3.3 | 8.0 ± 2.8 | −2.4 ± 5.44 | −1.5 ± 9.6 | 0.4 ± 7.6 | - |
| Postoperative condition | ||||||
| Range of motion (latest follow up) | 1.1 ± 3.1~111.6 ± 22.4 | 0.0 ± 0.0~130.0 ± 0.0 | 0.0 ± 0.0~122.8 ± 7.6 | 1.3 ± 3.9~112.3 ± 17.0 | 4.5 ± 6.0~105.0 ± 19.0 | 1.5 ± 4.0~112.7 ± 18.8 |
| Mean depression plateau (mm) | 2.8 ± 3.6 | 0.0 ± 0.0 | 2.7 ± 4.0 | 5.1 ± 4.9 | 5.5 ± 3.4 | 3.9 ± 4.2 |
| Mean tibiofemoral angle | 6.7 ± 5.7 | 6.0 ± 0.0 | 4.6 ± 4.3 | 3.4 ± 9.3 | 1.0 ± 7.5 | - |
| Associated injuries | ||||||
| High grade chondral injury (Outerbridge Gr 3, Gr 4) (%) | 11(57.9%) | 0 | 2 (28.6%) | 9 (45%) | 6 (60%) | 28 (48.3%) |
| Meniscus (%) | 10 | 1 | 3 | 8 | 4 | 26 (44.8%) |
| ACL (%) | 1 | 0 | 1 | 4 | 2 | 8 (13.8%) |
| PCL (%) | 1 | 0 | 1 | 3 | 0 | 5 (8.6%) |
| MCL (%) | 0 | 0 | 0 | 1 | 0 | 1 (1.7%) |
| Frequency of patients involved (%) | 52.6% (10/19) | 50% | 57.1% (4/7) | 55.5% (11/20) | 50% (5/10) | 53.4% (31/58) |
| Clinical Parameter | Points | Excellent | Good | Fair | Poor |
|---|---|---|---|---|---|
| Subjective | |||||
| Pain | 5 | 4 | 2 | 0 | |
| None | 6 | ||||
| Occasional pain, needs no medication | 5 | ||||
| Stabbing pain | 4 | ||||
| Intense, activity-related | 2 | ||||
| Night pain, at rest | 0 | ||||
| Walking capacity | 6 | 4 | 2 | 1 | |
| Normal | 6 | ||||
| Outdoors >1 h | 4 | ||||
| Outdoors >15 min | 2 | ||||
| Indoors only | 1 | ||||
| Wheelchair/bedridden | 0 | ||||
| Objective | |||||
| Extension | 6 | 4 | 2 | 2 | |
| Normal | 6 | ||||
| <10° loss | 4 | ||||
| >10° loss | 2 | ||||
| Total range of motion | 5 | 4 | 2 | 1 | |
| >140° | 6 | ||||
| >120° | 5 | ||||
| >90° | 4 | ||||
| >60° | 2 | ||||
| >30° | 1 | ||||
| 0° | 0 | ||||
| Stability | 5 | 4 | 2 | 2 | |
| Normal | 6 | ||||
| Abnormal in 20° flexion | 5 | ||||
| Instability in extension <10° | 4 | ||||
| Instability in extension >10° | 2 | ||||
| Total (minimum) | 30–27 | 26–20 | 19–10 | 9–6 | |
| Radiological Parameter | Points | Excellent | Good | Fair | Poor |
|---|---|---|---|---|---|
| Depression | 6 | 4 | 2 | 0 | |
| None | 6 | ||||
| <6 mm | 4 | ||||
| 6–10 mm | 2 | ||||
| >10 mm | 0 | ||||
| Condylar widening | 6 | 4 | 2 | 0 | |
| None | 6 | ||||
| <6 mm | 4 | ||||
| 6–10 mm | 2 | ||||
| >10 mm | 0 | ||||
| Angulation (valgus/varus) | 6 | 4 | 2 | 0 | |
| Normal | 6 | ||||
| <10° | 4 | ||||
| 10°–20° | 2 | ||||
| >20° | 0 | ||||
| Total (minimum) | 18 | 17–12 | 11–6 | 5–0 |
| Fracture Type | No. of Patients | Average Clinical Score | Excellent | Good | Fair | Poor | Satisfactory Results |
|---|---|---|---|---|---|---|---|
| Type II | 19 | 22.6 ± 5.3 | 4 (21%) | 10 (52.6%) | 5 (26.3%) | None | 73.7% |
| Type III | 2 | 26.0 ± 0.0 | None | 2 (100%) | None | None | 100% |
| Type IV | 7 | 25.3 ± 1.4 | 1 (14.3%) | 6 (85.7%) | None | None | 100% |
| Type V | 20 | 23.6 ± 4.0 | 1 (5%) | 17 (85%) | 1 (5%) | 1(5%) | 90% |
| Type VI | 10 | 21.6 ± 5.2 | 1 (10%) | 5 (50%) | 4 (40%) | None | 60% |
| Total Injuries | 58 | 23.2 ± 4.5 | 7(12%) | 40(68.9%) | 10(17.2%) | 1(1.7%) | 47(81%) |
| Fracture Type | No. of Patients | Average Radiological Score | Excellent | Good | Fair | Poor | Satisfactory Results |
|---|---|---|---|---|---|---|---|
| Type IV | 5 | 16 (range: 14–18) | 3 (60%) | 2 (40%) | None | None | 100% |
| Type V | 2 | 16.5 (range: 14–18) | 1 (50%) | 1 (50%) | None | None | 100% |
| Type VI | 18 | 15 (range: 10–18) | 9 (34%) | 8 (44%) | 1 (22%) | None | 94% |
| Total Injuries | 25 | 15.8 | 13 (52%) | 11 (44%) | 1 (4%) | None | 96% (24/25) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.-Y.; Cheng, C.-Y.; Chen, A.C.-Y.; Chan, Y.-S. Arthroscopy-Assisted Corrective Osteotomy, Reduction, Internal Fixation and Strut Allograft Augmentation for Tibial Plateau Malunion or Nonunion. J. Clin. Med. 2020, 9, 973. https://doi.org/10.3390/jcm9040973
Wang J-Y, Cheng C-Y, Chen AC-Y, Chan Y-S. Arthroscopy-Assisted Corrective Osteotomy, Reduction, Internal Fixation and Strut Allograft Augmentation for Tibial Plateau Malunion or Nonunion. Journal of Clinical Medicine. 2020; 9(4):973. https://doi.org/10.3390/jcm9040973
Chicago/Turabian StyleWang, Jr-Yi, Chun-Ying Cheng, Alvin Chao-Yu Chen, and Yi-Sheng Chan. 2020. "Arthroscopy-Assisted Corrective Osteotomy, Reduction, Internal Fixation and Strut Allograft Augmentation for Tibial Plateau Malunion or Nonunion" Journal of Clinical Medicine 9, no. 4: 973. https://doi.org/10.3390/jcm9040973
APA StyleWang, J.-Y., Cheng, C.-Y., Chen, A. C.-Y., & Chan, Y.-S. (2020). Arthroscopy-Assisted Corrective Osteotomy, Reduction, Internal Fixation and Strut Allograft Augmentation for Tibial Plateau Malunion or Nonunion. Journal of Clinical Medicine, 9(4), 973. https://doi.org/10.3390/jcm9040973