Quantitative Assessment of Gait Characteristics in Degenerative Cervical Myelopathy: A Prospective Clinical Study

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Scores
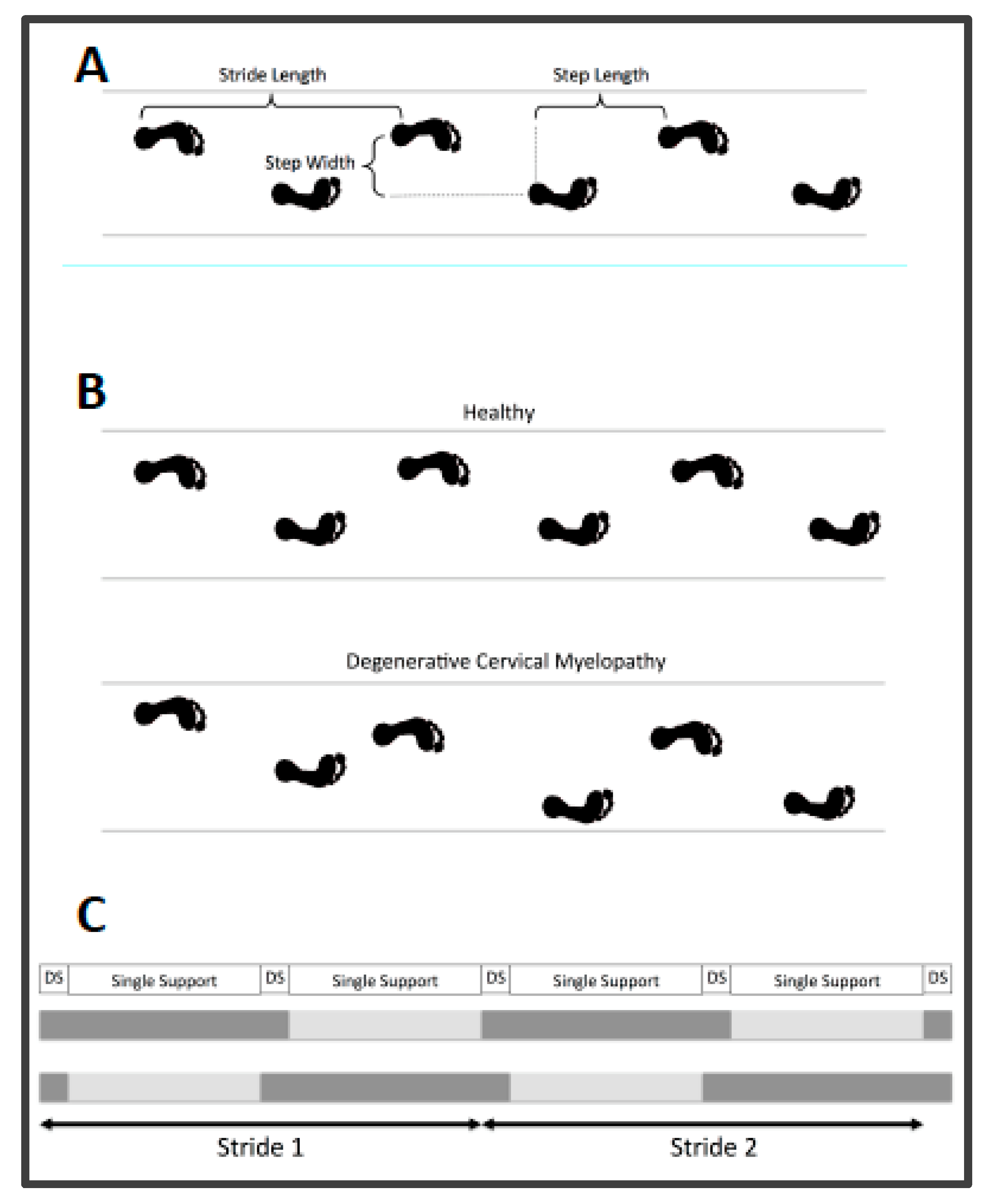
2.3. Gait Assessment
2.4. Enhanced Gait Variability Index
2.5. Statistics
3. Results
3.1. Patient Demographics
3.2. Quantitative Assessment of Gait Parameters
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kalsi-Ryan, S.; Karadimas, S.K.; Fehlings, M.G. Cervical spondylotic myelopathy: The clinical phenomenon and the current pathobiology of an increasingly prevalent and devastating disorder. Neuroscientist 2013, 19, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Fehlings, M.G.; Tetreault, L.; Hsieh, P.C.; Traynelis, V.; Wang, M.Y. Introduction: Degenerative cervical myelopathy: Diagnostic, assessment, and management strategies, surgical complications, and outcome prediction. Neurosurg. Focus 2016, 40, E1. [Google Scholar] [CrossRef] [PubMed]
- Nouri, A.; Tetreault, L.; Singh, A.; Karadimas, S.K.; Fehlings, M.G. Degenerative Cervical Myelopathy: Epidemiology, Genetics, and Pathogenesis. Spine 2015, 40, E675–E693. [Google Scholar] [CrossRef] [PubMed]
- Ray, S.K.; Matzelle, D.D.; Wilford, G.G.; Hogan, E.L.; Banik, N.L. Increased calpain expression is associated with apoptosis in rat spinal cord injury: Calpain inhibitor provides neuroprotection. Neurochem. Res. 2000, 25, 1191–1198. [Google Scholar] [CrossRef]
- Tetreault, L.; Goldstein, C.L.; Arnold, P.; Harrop, J.; Hilibrand, A.; Nouri, A.; Fehlings, M.G. Degenerative Cervical Myelopathy: A Spectrum of Related Disorders Affecting the Aging Spine. Neurosurgery 2015, 77 (Suppl. 4), S51–S67. [Google Scholar] [CrossRef]
- Young, W.F. Cervical spondylotic myelopathy: A common cause of spinal cord dysfunction in older persons. Am. Fam. Physician 2000, 62, 1064–1070, 1073. [Google Scholar]
- King, J.T., Jr.; McGinnis, K.A.; Roberts, M.S. Quality of life assessment with the medical outcomes study short form-36 among patients with cervical spondylotic myelopathy. Neurosurgery 2003, 52, 113–120; discussion 121. [Google Scholar]
- Tracy, J.A.; Bartleson, J.D. Cervical spondylotic myelopathy. Neurologist 2010, 16, 176–187. [Google Scholar] [CrossRef]
- Malone, A.; Meldrum, D.; Bolger, C. Gait impairment in cervical spondylotic myelopathy: Comparison with age- and gender-matched healthy controls. Eur. Spine J. 2012, 21, 2456–2466. [Google Scholar] [CrossRef]
- Kuhtz-Buschbeck, J.P.; Johnk, K.; Mader, S.; Stolze, H.; Mehdorn, M. Analysis of gait in cervical myelopathy. Gait Posture 1999, 9, 184–189. [Google Scholar] [CrossRef]
- Siasios, I.D.; Spanos, S.L.; Kanellopoulos, A.K.; Fotiadou, A.; Pollina, J.; Schneider, D.; Becker, A.; Dimopoulos, V.G.; Fountas, K.N. The Role of Gait Analysis in the Evaluation of Patients with Cervical Myelopathy: A Literature Review Study. World Neurosurg. 2017, 101, 275–282. [Google Scholar] [CrossRef]
- Kidd, G.; Lawes, N.; Musa, I. Understanding Neuromuscular Plasticity: A Basic for Clinical Rehabilitation; Edward Arnolds: London, UK, 1992. [Google Scholar]
- Drew, T.; Prentice, S.; Schepens, B. Cortical and brainstem control of locomotion. Prog. Brain Res. 2004, 143, 251–261. [Google Scholar]
- Dietz, V. Human neuronal control of automatic functional movements: Interaction between central programs and afferent input. Physiol. Rev. 1992, 72, 33–69. [Google Scholar] [CrossRef] [PubMed]
- Kopjar, B.; Fehlings, M.; Hanson, B. Validity of the Modified Japanese Orthopedic Association Score in Patients with Cervical Spondylotic Myelopathy: The AOSpine North America Multicenter Prospective Study. Spine J. 2011, 11, S73–S74. [Google Scholar] [CrossRef]
- Kim, C.R.; Yoo, J.Y.; Lee, S.H.; Lee, D.H.; Rhim, S.C. Gait analysis for evaluating the relationship between increased signal intensity on t2-weighted magnetic resonance imaging and gait function in cervical spondylotic myelopathy. Arch. Phys. Med. Rehabil. 2010, 91, 1587–1592. [Google Scholar] [CrossRef] [PubMed]
- Haddas, R.; Patel, S.; Arakal, R.; Boah, A.; Belanger, T.; Ju, K.L. Spine and lower extremity kinematics during gait in patients with cervical spondylotic myelopathy. Spine J. 2018, 18, 1645–1652. [Google Scholar] [CrossRef]
- Singh, A.; Choi, D.; Crockard, A. Use of walking data in assessing operative results for cervical spondylotic myelopathy: Long-term follow-up and comparison with controls. Spine 2009, 34, 1296–1300. [Google Scholar] [CrossRef]
- Pope, D.H.; Mowforth, O.D.; Davies, B.M.; Kotter, M.R.N. Diagnostic Delays Lead To Greater Disability In Degenerative Cervical Myelopathy and Represent A Health-Inequality. Spine 2020, 45, 368–377. [Google Scholar] [CrossRef]
- Tetreault, L.; Kopjar, B.; Nouri, A.; Arnold, P.; Barbagallo, G.; Bartels, R.; Qiang, Z.; Singh, A.; Zileli, M.; Vaccaro, A.; et al. The modified Japanese Orthopaedic Association scale: Establishing criteria for mild, moderate and severe impairment in patients with degenerative cervical myelopathy. Eur. Spine J. 2017, 26, 78–84. [Google Scholar] [CrossRef]
- Berg, K.O.; Wood-Dauphinee, S.L.; Williams, J.I.; Maki, B. Measuring balance in the elderly: Validation of an instrument. Can. J. Public Health = Rev. Can. Sante Publique 1992, 83 (Suppl. 2), S7–S11. [Google Scholar]
- Menz, H.B.; Latt, M.D.; Tiedemann, A.; Mun San Kwan, M.; Lord, S.R. Reliability of the GAITRite walkway system for the quantification of temporo-spatial parameters of gait in young and older people. Gait Posture 2004, 20, 20–25. [Google Scholar] [CrossRef]
- Vallabhajosula, S.; Humphrey, S.K.; Cook, A.J.; Freund, J.E. Concurrent Validity of the Zeno Walkway for Measuring Spatiotemporal Gait Parameters in Older Adults. J. Geriatr. Phys. Ther. (2001). 2019, 42, E42–E50. [Google Scholar] [CrossRef] [PubMed]
- Gouelle, A.; Rennie, L.; Clark, D.J.; Megrot, F.; Balasubramanian, C.K. Addressing limitations of the Gait Variability Index to enhance its applicability: The enhanced GVI (EGVI). PLoS ONE 2018, 13, e0198267. [Google Scholar] [CrossRef] [PubMed]
- Gouelle, A.; Megrot, F.; Presedo, A.; Husson, I.; Yelnik, A.; Pennecot, G.F. The gait variability index: A new way to quantify fluctuation magnitude of spatiotemporal parameters during gait. Gait Posture 2013, 38, 461–465. [Google Scholar] [CrossRef]
- Moon, Y.; Sung, J.; An, R.; Hernandez, M.E.; Sosnoff, J.J. Gait variability in people with neurological disorders: A systematic review and meta-analysis. Hum. Mov. Sci. 2016, 47, 197–208. [Google Scholar] [CrossRef]
- Fehlings, M.G.; Wilson, J.R.; Kopjar, B.; Yoon, S.T.; Arnold, P.M.; Massicotte, E.M.; Vaccaro, A.R.; Brodke, D.S.; Shaffrey, C.I.; Smith, J.S.; et al. Efficacy and safety of surgical decompression in patients with cervical spondylotic myelopathy: Results of the AOSpine North America prospective multi-center study. J. Bone Jt. Surg. Am. Vol. 2013, 95, 1651–1658. [Google Scholar] [CrossRef]
- Chen, G.; Patten, C.; Kothari, D.H.; Zajac, F.E. Gait differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds. Gait Posture 2005, 22, 51–56. [Google Scholar] [CrossRef]
- Guzik, A.; Druzbicki, M.; Przysada, G.; Wolan-Nieroda, A.; Szczepanik, M.; Bazarnik-Mucha, K.; Kwolek, A. Validity of the gait variability index for individuals after a stroke in a chronic stage of recovery. Gait Posture 2019, 68, 63–67. [Google Scholar] [CrossRef]
- Zheng, C.F.; Liu, Y.C.; Hu, Y.C.; Xia, Q.; Miao, J.; Zhang, J.D.; Zhang, K. Correlations of Japanese Orthopaedic Association Scoring Systems with Gait Parameters in Patients with Degenerative Spinal Diseases. Orthop. Surg. 2016, 8, 447–453. [Google Scholar] [CrossRef]
- Virmani, T.; Gupta, H.; Shah, J.; Larson-Prior, L. Objective measures of gait and balance in healthy non-falling adults as a function of age. Gait Posture 2018, 65, 100–105. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Lower Extremity Subscore (/7) | 0 | Complete loss of movement and sensation |
| 1 | Complete loss of movement, some sensation present | |
| 2 | Inability to walk, but some movement | |
| 3 | Able to walk on flat ground with walking aid | |
| 4 | Able to walk without walking aid but must hold a handrail on stairs | |
| 5 | Moderate to severe walking imbalance, but able to perform stairs without handrail | |
| 6 | Mild imbalance when standing OR walking | |
| 7 | Normal walking |
| Parameter | Description | Unit |
|---|---|---|
| Velocity | Walking speed = distance per time | cm/s |
| Cadence | Steps per minute | steps/min |
| Base of support | Step width = perpendicular distance between two points on both feet measured during two consecutive steps | m |
| Step length | Distance between ground contact of one foot and the next subsequent ground contact of the opposite foot in the direction of progression | m |
| Stride length | Distance between ground contact of one foot and the next subsequent ground contact of the same foot in the direction of progression | m |
| Step time | Time between ground contact of one foot and the next subsequent ground contact of the opposite foot | s |
| Single-stance time | Time during gait cycle while one foot is on the ground | s |
| Double-stance time | Time during gait cycle while two feet are on the ground | s |
| Total stance time | Time that passes during single and double support of the stance phase of one extremity during a gait cycle | s |
| eGVI | enhanced gait variability index (includes 5 spatiotemporal gait parameters: step time, step length, step velocity, total stance time, single-stance time) |
| Variable | Control Group n = 13 | Mild DCM n = 82 | Moderate DCM n = 40 | Severe DCM n = 31 | All DCM n = 153 |
|---|---|---|---|---|---|
| Age | 56.75 (6.77) | 55.3 (11.01) | 55.73 (9.75) | 62.19 (10.91) | 56.81 (10.92) |
| mJOA Score | 15.92 (0.73) | 13.13 (0.82) | 9.94(2.5) | 13.98 (2.50) | |
| mJOA LE Subscore | 6.51 (0.55) | 5.10 (1.12) | 3.71 (1.35) | 5.58 (1.35) | |
| Berg Balance Score | 53.52 (5.24) | 49.63 (7.09) | 42.59 (4.65) | 47(6.1) | |
| Velocity (cm/sec) | 119.22 (11.61) | 114.84 (23.71) | 106.44 (23.72) | 74.18 (29.51) | 104.41 (29.51) |
| Cadence (steps/min) | 114.74(9.49) | 111.49 (12.67) | 108.58 (12.46) | 92.55(15.98) | 106.89 (15.99) |
| Base of Support (cm) | 8.16 (3.74) | 9.13 (3.28) | 8.21 (3.85) | 9.24 (3.65) | 8.91 (3.65) |
| Step Length (cm) | 63.57 (4.87) | 60.81 (9.66) | 57.94 (8.83) | 45.96 (11.44) | 57.05 (11.44) |
| Total Stance Time (sec) | 0.649 (0.12) | 0.702 (0.10) | 0.717 (0.09) | 0.905 (0.25) | 0.747 (0.163) |
| Single-Support Time (sec) | 0.410 (0.03) | 0.389 (0.04) | 0.395 (0.04) | 0.409 (0.07) | 0.394 (0.046) |
| Double-Support Time (sec) | 0.249 (0.029) | 0.303 (0.08) | 0.316 (0.06) | 0.485 (0.22) | 0.343 (0.138) |
| Single-Stance Ratio | 1.56 (0.20) | 1.35 (0.29) | 1.29 (0.23) | 0.99 (0.38) | 1.26 (0.32) |
| Enhanced Gait Variability Index | 103.36(4.54) | 110.9 (9.73) | 119.14 (10.14) | 132.94 (12.78) | 117.54 (13.5) |
| Gait Parameters | mJOA LE | p−Value | mJOA | p−Value |
|---|---|---|---|---|
| Velocity (cm/sec) | 0.456 | <0.001 | 0.426 | <0.001 |
| Cadence (steps/min) | 0.346 | <0.001 | 0.286 | <0.001 |
| Base of Support (cm) | 0.044 | 0.6 | 0.038 | 0.6 |
| Step Length (cm) | 0.434 | <0.001 | 0.417 | <0.001 |
| Total Stance Time (sec) | −0.352 | <0.001 | −0.303 | <0.001 |
| Single-Support Time (sec) | −0.058 | 0.47 | 0.004 | 0.959 |
| Double-Support Time (sec) | −0.404 | <0.001 | −0.382 | <0.001 |
| Single-Stance Ratio | 0.413 | <0.001 | 0.417 | <0.001 |
| Enhanced Gait Variability Index | −0.567 | <0.001 | −0.551 | <0.001 |
| Gait Parameter | H(df) | p | Padj Mild/Moderate | Padj Mild/Severe | Padj Moderate/Severe | Epsilon2 |
|---|---|---|---|---|---|---|
| Velocity | 35.59(2) | <0.0001 | 0.081 | <0.0001 | 0.001 | 0.23 + |
| Cadence | 22.92(2) | <0.0001 | 0.59 | <0.0001 | 0.004 | 0.15 |
| Base of support | 2.73(2) | 0.26 | - | - | - | 0.02 |
| Step Length | 30.23(2) | <0.0001 | 0.25 | <0.0001 | 0.002 | 0.19 + |
| Stride Velocity | 32.79(2) | <0.0001 | 0.08 | <0.0001 | 0.003 | 0.22 + |
| Total Stance Time | 21.80(2) | 0.0002 | 0.72 | <0.0001 | 0.005 | 0.14 |
| Single-Support Time | 1.83(2) | 0.4 | - | - | - | 0.01 |
| Double-Support Time | 25.54(2) | <0.0001 | 0.34 | <0.0001 | 0.0043 | 0.16 |
| Single-Stance Ratio | 25.96(2) | <0.0001 | 0.59 | <0.0001 | 0.002 | 0.17 |
| eGVI | 55.04(2) | <0.0001 | 0.001* | <0.0001 * | 0.001 * | 0.36 ++ |
| Age | 9.22(2) | 0.01 | 1 | 0.012 | 0.023 | 0.06 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalsi-Ryan, S.; Rienmueller, A.C.; Riehm, L.; Chan, C.; Jin, D.; Martin, A.R.; Badhiwala, J.H.; Akbar, M.A.; Massicotte, E.M.; Fehlings, M.G. Quantitative Assessment of Gait Characteristics in Degenerative Cervical Myelopathy: A Prospective Clinical Study. J. Clin. Med. 2020, 9, 752. https://doi.org/10.3390/jcm9030752
Kalsi-Ryan S, Rienmueller AC, Riehm L, Chan C, Jin D, Martin AR, Badhiwala JH, Akbar MA, Massicotte EM, Fehlings MG. Quantitative Assessment of Gait Characteristics in Degenerative Cervical Myelopathy: A Prospective Clinical Study. Journal of Clinical Medicine. 2020; 9(3):752. https://doi.org/10.3390/jcm9030752
Chicago/Turabian StyleKalsi-Ryan, Sukhvinder, Anna C. Rienmueller, Lauren Riehm, Colin Chan, Daniel Jin, Allan R. Martin, Jetan H. Badhiwala, Muhammad A. Akbar, Eric M. Massicotte, and Michael G. Fehlings. 2020. "Quantitative Assessment of Gait Characteristics in Degenerative Cervical Myelopathy: A Prospective Clinical Study" Journal of Clinical Medicine 9, no. 3: 752. https://doi.org/10.3390/jcm9030752
APA StyleKalsi-Ryan, S., Rienmueller, A. C., Riehm, L., Chan, C., Jin, D., Martin, A. R., Badhiwala, J. H., Akbar, M. A., Massicotte, E. M., & Fehlings, M. G. (2020). Quantitative Assessment of Gait Characteristics in Degenerative Cervical Myelopathy: A Prospective Clinical Study. Journal of Clinical Medicine, 9(3), 752. https://doi.org/10.3390/jcm9030752