The Benefits of emotion Regulation Interventions in Virtual Reality for the Improvement of Wellbeing in Adults and Older Adults: A Systematic Review

 ,
, 
Abstract
1. Introduction
2. Method
2.1. Search Methodology
2.2. Study Selection and Inclusion Criteria
2.3. Risk of Bias Assessment
3. Results
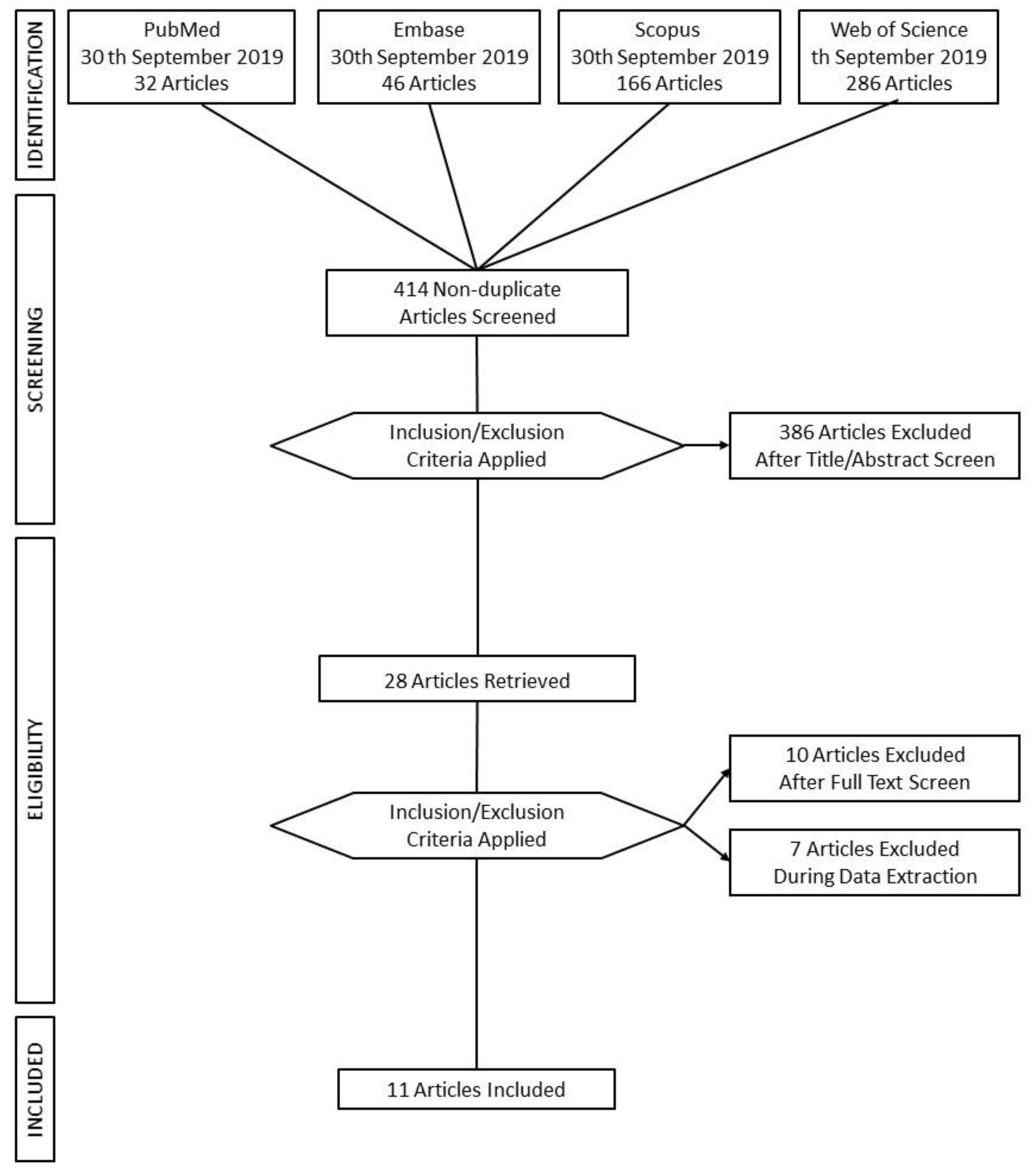
3.1. Flow Chart of the Results
3.2. Risk of Bias
3.3. Study Characteristics
3.4. Interventions for Adults and Older Adults
3.4.1. Age Differences in Emotional Experience
3.4.2. Interventions for Adults
3.4.3. Virtual Environments (VE) for Healthy Participants
3.4.4. Virtual Environments for Patients
3.4.5. Virtual Reality Set-Up
3.4.6. VR Interventions for Older Adults
3.5. Outcome Measures for Wellbeing
3.5.1. Physiological Markers
3.5.2. Wellbeing Scales Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Scherer, K.R. Emotions are emergent processes: They require a dynamic computational architecture. Philos. Trans. R. Soc. B Biol. Sci. 2009, 364, 3459–3474. [Google Scholar] [CrossRef] [PubMed]
- Leahy, R.; Tirch, D.; Napolitano, L. Why is emotion regulation important? Psychother. Aust. 2012, 19, 68–81. [Google Scholar]
- Beck, A.T. Cognitive Therapy and the Emotional Disorders, 1st ed.; International Universities Press: Madison, CT, USA, 1976. [Google Scholar]
- Gross, J.J. The Emerging Field of Emotion Regulation: An Integrative Review. Rev. Gen. Psychol. 1998, 2, 271–299. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion regulation: Affective, cognitive, and social consequences. Psychophysiology 2002, 39, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J. Emotion regulation: Current status and future prospects. Psychol. Inq. 2015, 26, 1–26. [Google Scholar] [CrossRef]
- Gross, J.J.; Thompson, R.A. Emotion Regulation: Conceptual Foundations. In Handbook of Emotion Regulation; The Guilford Press: New York, NY, USA, 2007; pp. 3–24. [Google Scholar]
- Cole, P.M.; Michel, M.K.; Teti, L.O.D. The Development of Emotion Regulation and Dysregulation: A Clinical Perspective. Monogr. Soc. Res. Child Dev. Dev. Emot. Regul. Biol. Behav. Consid. 1994, 59, 73–100. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: Berlin/Heidelberg, Germany, 1984. [Google Scholar]
- Thompson, R.A.; Calkins, S.D. The double-edged sword: Emotional regulation for children at risk. Dev. Psychopathol. 1996, 8, 163–182. [Google Scholar] [CrossRef]
- Parker, J.D.A.; Endler, N.S. Coping and defense: A historical overview. In Handbook of Coping: Theory, Research, Applications; John Wiley & Sons: Oxford, UK, 1996; pp. 3–23. [Google Scholar]
- Folkman, S.; Lazarus, R.S. Coping as a Mediator of Emotion. J. Personal. Soc. Psychol. 1988, 54, 466–475. [Google Scholar] [CrossRef]
- Suri, G.; Sheppes, G.; Young, G.; Abraham, D.; McRae, K.; Gross, J.J. Emotion regulation choice: The role of environmental affordances. Cogn. Emot. 2018, 32, 963–971. [Google Scholar] [CrossRef]
- John, O.P.; Gross, J.J. Healthy and unhealthy emotion regulation: Personality processes, individual differences, and life span development. J. Personal. 2004, 72, 1301–1334. [Google Scholar] [CrossRef]
- Greenberg, L.S. Emotion-Focused Therapy; Theories of Psychotherapy; American Psychological Association: Worcester, MA, USA, 2011. [Google Scholar]
- Lucas, R.E.; Diener, E. Subjective Well-Being. In Handbook of Emotion; T.G. Press: New York, NY, USA, 2008; pp. 471–484. [Google Scholar]
- Diener, E.; Suh, E.M.; Lucas, R.E.; Smith, H.L. Subjective Well-Being: Three Decades of Progress. Psychol. Bull. 1999, 125, 276–302. [Google Scholar] [CrossRef]
- Montana, J.I.; Tuena, C.; Serino, S.; Cipresso, P.; Riva, G. Neurorehabilitation of Spatial Memory Using Virtual Environments: A Systematic Review. J. Clin. Med. 2019, 8, 1516. [Google Scholar] [CrossRef] [PubMed]
- Mishkind, M.C.; Norr, A.M.; Katz, A.C.; Reger, G.M. Review of Virtual Reality Treatment in Psychiatry: Evidence Versus Current Diffusion and Use. Curr. Psychiatry Rep. 2017, 19. [Google Scholar] [CrossRef] [PubMed]
- Clus, D.; Larsen, M.E.; Lemey, C.; Berrouiguet, S. The use of virtual reality in patients with eating disorders: Systematic review. J. Med. Internet Res. 2018, 20, 1–9. [Google Scholar] [CrossRef]
- Wiederhold, B.K.; Riva, G.; Gutiérrez-Maldonado, J. Virtual Reality in the Assessment and Treatment of Weight-Related Disorders. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 67–73. [Google Scholar] [CrossRef]
- Rus-Calafell, M.; Garety, P.; Sason, E.; Craig, T.J.K.; Valmaggia, L.R. Virtual reality in the assessment and treatment of psychosis: A systematic review of its utility, acceptability and effectiveness. Psychol. Med. 2018, 48, 362–391. [Google Scholar] [CrossRef]
- Riva, G.; Gaggioli, A.; Villani, D.; Preziosa, A.; Morganti, F.; Corsi, R.; Faletti, G.; Vezzadini, L. NeuroVR: An open source virtual reality platform for clinical psychology and behavioral neurosciences. Stud. Health Technol. Inf. 2007, 125, 394–399. [Google Scholar]
- Riches, S.; Garety, P.; Rus-Calafell, M.; Stahl, D.; Evans, C.; Sarras, N.; Yeboah, K.; Valmaggia, L. Using Virtual Reality to Assess Associations Between Paranoid Ideation and Components of Social Performance: A Pilot Validation Study. Cyberpsychol. Behav. Soc. Netw. 2019, 22, 51–59. [Google Scholar] [CrossRef]
- Valmaggia, L. The use of virtual reality in psychosis research and treatment. World Psychiatry 2017, 16, 245–246. [Google Scholar] [CrossRef]
- Parsons, T.D.; Carlew, A.R.; Magtoto, J.; Stonecipher, K. The potential of function-led virtual environments for ecologically valid measures of executive function in experimental and clinical neuropsychology. Neuropsychol. Rehabil. 2017, 27, 777–807. [Google Scholar] [CrossRef]
- Serino, S.; Baglio, F.; Rossetto, F.; Realdon, O.; Cipresso, P.; Parsons, T.D.; Cappellini, G.; Mantovani, F.; De Leo, G.; Nemni, R.; et al. Picture Interpretation Test (PIT) 360°: An Innovative Measure of Executive Functions. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bohil, C.J.; Alicea, B.; Biocca, F.A. Virtual reality in neuroscience research and therapy. Nat. Rev. Neurosci. 2011, 12. [Google Scholar] [CrossRef]
- Colombo, D.; Fernández-álvarez, J.; Palacios, A.G.; Cipresso, P.; Botella, C.; Riva, G. New technologies for the understanding, assessment, and intervention of emotion regulation. Front. Psychol. 2019, 10. [Google Scholar] [CrossRef]
- Villani, D.; Carissoli, C.; Triberti, S.; Marchetti, A.; Gilli, G.; Riva, G. Videogames for Emotion Regulation: A Systematic Review. Games Health J. 2018, 7, 85–99. [Google Scholar] [CrossRef] [PubMed]
- Kompus, K. Virtual-reality-assisted therapy in patients with psychosis Title. Lancet Psychiatry 2018, 5, 189–191. [Google Scholar] [CrossRef]
- Riva, G.; Baños, R.M.; Botella, C.; Mantovani, F.; Gaggioli, A. Transforming experience: The potential of augmented reality and virtual reality for enhancing personal and clinical change. Front. Psychiatry 2016, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Baños, R.M.; Etchemendy, E.; Mira, A.; Riva, G.; Gaggioli, A.; Botella, C. Online positive interventions to promote well-being and resilience in the adolescent population: A narrative review. Front. Psychiatry 2017, 8. [Google Scholar] [CrossRef]
- Schek, E.J.; Mantovani, F.; Realdon, O.; Dias, J.; Paiva, A.; Schramm-Yavin, R.; Pat-Horenczyk, S. Positive Technologies for Promoting Emotion Regulation Abilities in Adolescents. In Lecture Notes of the Institute for Computer Sciences, Social Informatics and Telecommunications Engineering; Springer: Berlin/Heidelberg, Germany, 2016; pp. 169–174. [Google Scholar]
- Sanchez-Vives, M.V.; Slater, M. Opinion: From presence to consciousness through virtual reality. Nat. Rev. Neurosci. 2005, 6, 332–339. [Google Scholar] [CrossRef]
- Feller, S.C.; Castillo, E.G.; Greenberg, J.M.; Abascal, P.; Van Horn, R.; Wells, K.B.; University of California, Los Angeles Community Translational Science Team. Emotional well-being and public health: Proposal for a model national initiative. Public Health Rep. 2018, 133, 136–141. [Google Scholar] [CrossRef]
- Vik, M.H. Measuring subjective well-being for policy purposes: The example of well-being indicators in the WHO ‘Health 2020’ framework. J. Scand. Public Health 2018, 46, 279–286. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Grp, P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement (Reprinted from Annals of Internal Medicine). Phys. Ther. 2009, 89, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Konrad, A.; Tucker, S.; Crane, J.; Whittaker, S. Technology and Reflection: Mood and Memory Mechanisms for Well-Being. Psychol. Well Being 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Villani, D.; Riva, G. Presence and relaxation: A preliminary controlled study. PsychNol. J. 2008, 6, 7–26. [Google Scholar]
- Tong, X.; Gromala, D.; Choo, A.; Amin, A.; Shaw, C. The Virtual Meditative Walk: An Immersive Virtual Environment for Pain Self-modulation Through Mindfulness-Based Stress Reduction Meditation. In Proceedings of the 7th International Conference, VAMR 2015, Held as Part of HCI International 2015, Los Angeles, CA, USA, 2–7 August 2015; Lecture Notes in Computer Science. Springer Int. Publ.: Cham, Switzerland, 2015; pp. 388–397. [Google Scholar] [CrossRef]
- Cikajlo, I.; Čižman-Štaba, U.; Vrhovac, S.; Larkin, F.; Roddy, M. Recovr: Realising collaborative virtual reality for wellbeing and self-healing. In Proceedings of the 3rd IASTED International Conference Telehealth Assistive Technology TAT 2016, Zurich, Switzerland, 5–7 October 2016; pp. 11–17. [Google Scholar] [CrossRef][Green Version]
- Hasan, H.; Linger, H. Enhancing the wellbeing of the elderly: Social use of digital technologies in aged care. Educ. Gerontol. 2016, 42, 749–757. [Google Scholar] [CrossRef]
- Baez, M.; Far, I.K.; Ibarra, F.; Ferron, M.; Didino, D.; Casati, F. Effects of online group exercises for older adults on physical, psychological and social wellbeing: A pilot trial Marcos. J. Chem. Inf. Model. 2017, 53, 1689–1699. [Google Scholar] [CrossRef]
- Singh, D.K.A.; Rahman, N.N.A.; Seffiyah, R.; Chang, S.Y.; Zainura, A.K.; Aida, S.R.; Rajwinder, K.H.S. Impact of virtual reality games on psychological well-being and upper limb performance in adults with physical disabilities: A pilot study. Med. J. Malays. 2017, 72, 119–121. [Google Scholar]
- Weerdmeester, J.; van Rooij, M.; Harris, O.; Smit, N.; Engels, R.C.M.E.; Granic, I. Exploring the role of self-efficacy in biofeedback video games. In Proceedings of the CHI Play 2017 Ext. Abstr.—Ext. Abstr. Publ. Annu. Symp. Comput. Interact. Play, Amsterdam, The Netherlands, 15–18 October 2017; pp. 453–461. [Google Scholar] [CrossRef]
- Bornioli, A. Psychological Wellbeing Benefits of Simulated Exposure to Five Urban Settings: An Experimental Study from the Pedestrian’s Perspective. Transp. Res. Part A Policy Pract. 2019, 123, 200–215. [Google Scholar] [CrossRef]
- Bornioli, A.; Parkhurst, G.; Morgan, P.L. Affective experiences of built environments and the promotion of urban walking. Transp. Res. Part. A Policy Pract. 2019, 123, 200–215. [Google Scholar] [CrossRef]
- Lorenzetti, V.; Bruno, M.; Rodrigo, B.; Chao, S.; Murat, Y.; Carlos, J.T.-C.; Jorge, M. Emotion regulation using virtual environments and real-time fMRI neurofeedback. Front. Neurol. 2018, 9, 1–15. [Google Scholar] [CrossRef]
- Turk, C.S.; Carstensen, L.L. Emotion Regulation and Aging. In Handbook of Emotion Regulation; Guilford: New York, NY, USA, 2007; pp. 307–325. [Google Scholar]
- Gross, J.J.; Carstensen, L.L.; Pasupathi, M.; Tsai, J.; Skorpen, C.G.; Hsu, A.Y.C. Emotion and aging: Experience, expression, and control. Psychol. Aging 1997, 12, 590–599. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.T.; Berntson, G.G.; Klein, D.J.; Poehlmann, K.M. The psychophysiology of emotion across the lifespan. Annu. Rev. Gerontol. Geriatr. 1998, 17, 27–65. [Google Scholar]
- Gross, J.J. Antecedent- and Response-Focused Emotion Regulation: Divergent Consequences for Experience, Expression, and Physiology. J. Personal. Soc. Psychol. 1998, 74, 224–237. [Google Scholar] [CrossRef]
- Singh, V.; Padmanabhan, B.; de Vreede, T.; de Vreede, G.-J.; Andel, S.; Spector, P.E.; Benfield, S.; Aslami, A. A content engagement score for online learning platforms. In Proceedings of the Fifth Annual ACM Conference Learning Scale—L@S ’18, London, UK, 26–28 June 2018; pp. 1–4. [Google Scholar] [CrossRef]
- Consedine, N.S.; Moskowitz, J.T. The role of discrete emotions in health outcomes: A critical review. Appl. Prev. Psychol. 2007, 12, 59–75. [Google Scholar] [CrossRef]
- Baños, R.M.; Castilla, D.; Etchemendy, E.; Garcia-Palacios, A. Positive mood induction procedures for virtual environments designed for elderly people. Interact. Comput. 2012, 24, 131–138. [Google Scholar] [CrossRef]
- Choi, N.G.; DiNitto, D.M. Internet Use Among Older Adults: Association with Health Needs, Psychological Capital, and Social Capital. J. Med. Internet Res. 2013, 15, e97. [Google Scholar] [CrossRef]
- Winstead, V.; Yost, E.A.; Cotten, S.R.; Berkowsky, R.W.; Anderson, W.A. The Impact of Activity Interventions on the Well-Being of Older Adults in Continuing Care Com. J. Appl. Gerontol. 2014, 33, 888–911. [Google Scholar] [CrossRef]
- Sander, D.; Grandjean, D.; Scherer, K.R. A systems approach to appraisal mechanisms in emotion. Neural Netw. 2005, 18, 317–352. [Google Scholar] [CrossRef]
- Scherer, K.R.; Schorr, A.; Johnstone, T. Appraisal Processes in Emotion: Theory, Methods, Research. In Handbook of Affective Sciences; Oxford University Press: Oxford, UK, 2003; pp. 92–120. [Google Scholar]
- Frank, D.L.; Khorshid, L.; Kiffer, J.; Moravec, C.S.; McKee Michael, G. Biofeedback in medicine: Who, when, why and how? Mental Health in Family Medicine. 2010, 7, 85–91. [Google Scholar]
- Wheat, A.L.; Larkin, K.T. Biofeedback of heart rate variability and related physiology: A critical review. Appl. Psychophysiol. Biofeedback 2010, 35, 229–242. [Google Scholar] [CrossRef]
- Gevirtz, R. The Promise of Heart Rate Variability Biofeedback: Evidence-Based Applications. Biofeedback 2013, 41, 110–120. [Google Scholar] [CrossRef]
- Gilbert, C.; Moss, D. Biofeedback and Biological Monitoring. In Handbook of Mind-Body Medicine for Primary Care: Behavioral and Physiological Tools; Sage Publications: Thousand Oaks, CA, USA, 2003; pp. 109–122. [Google Scholar]
- La Vaque, T.J. Neurofeedback, Neurotherapy, and Quantitative EEG. In Handbook of Mind-Body Medicine for Primary Care; Sage Publications: Thousand Oaks, CA, USA, 2003; pp. 123–136. [Google Scholar]
- Yucha, C.B.; Montgomery, D. Evidence-Based Practice in Biofeedback and Neurofeedback; Association for Applied Psychophysiology and Biofeedback: Wheat Ridge, CO, USA, 2008. [Google Scholar]
- Serino, S.; Cipresso, P.; Gaggioli, A.; Riva, G. The potential of pervasive sensors and computing for positive technology. In Pervasive and Mobile Sensing and Computing for Healthcare: Smart Sensors, Measurement and Instrumentation; Mukhopadhyay, S.C., Postolache, O.A., Eds.; Springer: New York, NY, USA, 2013. [Google Scholar]
- Realdon, O.; Rossetto, F.; Nalin, M.; Baroni, I.; Cabinio, M.; Fioravanti, R.; Saibene, F.L.; Alberoni, M.; Mantovani, F.; Romano, M.; et al. Technology-enhanced multi-domain at home continuum of care program with respect to usual care for people with cognitive impairment: The Ability- TelerehABILITation study protocol for a randomized controlled trial. BMC Psychiatry 2016, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Realdon, O.; Rossetto, F.; Nalin, M.; Baroni, I.; Romano, M.; Catania, F.; Frontini, D.; Mancastroppa, S.; Alberoni, M.; Zurloni, V.; et al. The Technology-Enhanced Ability Continuum-of-Care Home Program. for People with Cognitive Disorders: Concept Design and Scenario of Use. In Proceedings of the International Symposium on Pervasive Computing Paradigms for Mental Health, Buenos Aires, Argentina, 23–24 April 2018. [Google Scholar]
- Matamala-Gomez, M.; Donegan, T.; Bottiroli, S.; Sandrini, G.; Sanchez-Vives, M.V.; Tassorelli, C. Immersive virtual reality and virtual embodiment for pain relief. Front. Hum. Neurosci. 2019, 13, 279. [Google Scholar] [CrossRef] [PubMed]
- Matamala-Gomez, M.; Gonzalez, A.M.D.; Slater, M.; Sanchez-Vives, M.V. Decreasing Pain Ratings in Chronic Arm Pain Through Changing a Virtual Body: Different Strategies for Different Pain Types. J. Pain 2019, 20. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, H.G.; Patterson, D.R.; Carrougher, G.J.; Sharar, S.R. Effectiveness of virtual reality-based pain control with multiple treatments. Clin. J. Pain 2001, 17, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Baer, R.A. Mindfulness training as a clinical intervention: A conceptual and empirical review. Clin. Psychol. Pract. 2003, 10, 125–143. [Google Scholar] [CrossRef]
- Bingham, P.; Bates, J.H.T.; Thompson-Figueroa, T.; Lahiri, J. A breath biofeedback computer game for children with cystic fibrosis. Clin. Paediatr. 2010, 49, 337–342. [Google Scholar] [CrossRef]
- Fernández-Aranda, F.; Jiménez-Murcia, S.; Penelo, E. Video games as a complementary therapy tool in mental disorders: PlayMancer, a European multicentre study. J. Ment. Health 2012, 21, 364–374. [Google Scholar] [CrossRef]
- Lobel, A.; Gotsis, M.; Reynolds, E.; Annetta, M.; Engels, I.; Granic, R.C.M.E. Designing and utilizing biofeedback games for emotion regulation: The case of nevermind. In Proceedings of the 2016 CHI Conference Extended Abst, San Jose, CA, USA, 7–12 May 2016. [Google Scholar]
- Schwartz, M.S. Biofeedback: A Practitioner’s Guide, 2nd ed.; The Guilford Press: New York, NY, USA, 1995. [Google Scholar]
- Peper, E.; Harvey, R.; Takebayashi, N. Biofeedback an evidence based approach inclinical practice. Jpn. J. Biofeedback Res. 2009, 36, 3–10. [Google Scholar]
- Pham, Q.; Khatib, Y.; Fox, S.; Green, T. Feasibility and efficacy of an mHealth game for managing anxiety: ‘Flowy’ randomized controlled pilot trial and design evaluation. Games Health J. 2016, 5, 50–67. [Google Scholar] [CrossRef]
- Tyson, S.; Selley, A. A content analysis of physiotherapy for postural control in people with stroke: An observational study. Disabil. Rehabil. 2006, 28, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Thibaud, M.; Bloch, F.; Tournoux-Facon, C.; Brèque, C.; Rigaud, A.S.; Dugué, B.; Kemoun, G. Impact of physical activity and sedentary behaviour on fall risks in older people: A systematic review and meta-analysis of observational studies. Eur. Rev. Aging Phys. Act. 2012, 9, 5–15. [Google Scholar] [CrossRef]
- Stuart, M.; Chard, S.; Benvenuti, F.; Steinwachs, S. Community Exercise: A Vital Component to Healthy Aging. Healthcarepapers 2009, 10, 23–28. [Google Scholar] [CrossRef] [PubMed]
- El Khoury, F. The effect of fall prevention exercise programmes on fall induced injuries in community dwelling older adults: Systematic review and meta-analysis of randomised controlled trials. BMJ Res. 2013. [Google Scholar] [CrossRef]
- Mohr, D.C.; Cheung, K.; Schueller, S.M.; Brown, H.; Duan, N. Continuous Evaluation of Evolving Behavioral Intervention Technologies. Am. J. Prev. Med. 2013, 45, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Clore, G. Why emotions vary in intensity. In The Nature of Emotion: Fundamental Questions; Ekman, P., Davidson, R.J., Eds.; Oxford University Press: Oxford, UK, 1994; pp. 386–393. [Google Scholar]
- Richards, J.M.; Gross, J.J. Emotion regulation and memory: The cognitive costs of keeping one’s cool. J. Personal. Soc. Psychol. 2000, 79, 410–424. [Google Scholar] [CrossRef]
- Granic, I.; Lobel, A.; Engels, R.C.M.E. The Benefits of Playing Video Games. Am. Psychol. 2014, 69, 66–78. [Google Scholar] [CrossRef]
- Sherry, J.L. Flow and Media Enjoyment. Commun. Theory 2004, 14, 328–347. [Google Scholar] [CrossRef]
- Nakamura, J.; Csikszentmihalyi, M. The Concept of Flow. In Oxford Handbook of Positive Psychology; Snyder, U., Ed.; Oxford University Press: Oxford, UK, 2009; pp. 89–105. [Google Scholar]
- Riva, G.; Castelnuovo, G.; Mantovani, F. Transformation of flow in rehabilitation: The role of advanced communication technologies. Behav. Res. Methods 2006, 38, 237–244. [Google Scholar] [CrossRef]
- Riva, G.; Waterworth, J.A.; Waterworth, E.L. The layers of presence: A bio-cultural approach to understanding presence in natural and mediated environments. Cyberpsychol. Behav. Soc. Netw. 2004, 7, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Riva, G. From Virtual to Real Body. J. Cyberther. Rehabil. 2008, 1, 7–22. [Google Scholar]
- Steuer, J. Defining Virtual Reality: Characteristics Determining Telepresence. J. Commun. 1992, 42, 73–94. [Google Scholar] [CrossRef]
- Valmaggia, L.R.; Latifa, L.; Kempton, M.J.; Rus-Calafell, M. Virtual reality in the psychological treatment for mental health problems: An systematic review of recent evidence. Psychiatry Res. 2016, 236, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Slater, M.; Steed, A. Depth of Presence in Virtual Environments. Presence Teleoper. Virtual Environ. 1994. [Google Scholar] [CrossRef]
- Parsons, T.D. Virtual Reality for Enhanced Ecological Validity and Experimental Control in the Clinical, Affective and Social Neurosciences. Front. Hum. Neurosci. 2015, 9, 1–19. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion regulation: Conceptual and empirical foundations. In Handbook of emotion regulation; Gross, J.J., Ed.; Guilford Press: New York, NY, USA, 2014; pp. 3–20. [Google Scholar]
- Realdon, O.; Serino, S.; Savazzi, F.; Rossetto, F.; Cipresso, P.; Parsons, T.D.; Cappellini, G.; Mantovani, F.; Mendozzi, L.; Nemni, R.; et al. An ecological measure to screen executive functioning in MS: The Picture Interpretation Test (PIT). Sci. Rep. 2019, 1–8. [Google Scholar] [CrossRef]
- Ochsner, K.N.; Gross, J.J. The Neural Architecture of Emotion Regulation. In Handbook of Emotion Regulation; Guilford: New York, NY, USA, 2007; pp. 87–109. [Google Scholar]
- Linehan, M.M.; Bohus, M.; Lynch, T.R. Dialectical Behavior Therapy for Pervasive Emotion Dysregulation: Theoretical and Practical Underpinnings. In Handbook of Emotion Regulation; Guilford: New York, NY, USA, 2007; pp. 581–606. [Google Scholar]
- Boals, A.; Klein, K. Word Use in Emotional Narratives about Failed Romantic Relationships and Subsequent Mental Health. J. Lang. Soc. Psychol. 2005, 24, 252–268. [Google Scholar] [CrossRef]
- Petrie, K.J.; Booth, R.J.; Pennebaker, J.W. The Immunological Effects of Thought Suppression. J. Personal. Soc. Psychol. 1998, 75, 1264–1272. [Google Scholar] [CrossRef]
- Ryff, C.D.; Singer, B.H.; Love, G.D. Positive health: Connecting well-being with biology. Philos. Trans. R. Soc. B Biol. Sci. 2004, 359, 1383–1394. [Google Scholar] [CrossRef]
- Ryff, C.D. Psychological Well-Being in Adult Life. Curr. Dir. Psychol. Sci. 1995, 4, 99–104. [Google Scholar] [CrossRef]
- Kroll, C.; Kroll, C.; Delhey, J. A Happy Nation? Opportunities and Challenges of Using Subjective Indicators in Policymaking. Soc. Indic. Res. 2013, 114, 13–28. [Google Scholar] [CrossRef]


{kind=link}
| “virtual reality” OR “virtual environment*” OR “digital intervention*” OR “digital technologies.” | ||||||
|---|---|---|---|---|---|---|
| AND | PubMed | Embase | Scopus | Web of Science | ||
| “emotion regulation” | 17 | 20 | 40 | 54 | ||
| “affect regulation” | 1 | 1 | 2 | 104 | ||
| “wellbeing” | 14 | 25 | 124 | 128 | ||
| Sub total | 32 | 46 | 166 | 286 | Total | 530 |
| Without duplicates | 414 | |||||
| Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personal (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias | ||
|---|---|---|---|---|---|---|---|---|
| Villani and Riva | 2008 | low | unclear | unclear | low | low | low | low |
| Tong et al. | 2015 | low | unclear | low | unclear | low | low | low |
| Cikajlo et al. | 2016 | high | high | unclear | unclear | low | low | high: small sample size/no control group/\no homogeneous clinical sample |
| Hasan et al. | 2016 | high | high | unclear | unclear | high | high | high: no control group |
| Konrad et al. | 2016 | low | low | low | low | low | low | low |
| Baez et al. | 2017 | low | low | unclear | low | low | low | low |
| Singh et al. | 2017 | high | high | unclear | unclear | high | high | high: small sample size/no control group |
| Weerdmeester et al. | 2017 | high | high | unclear | unclear | low | low | high: no control group |
| Bornioli et al. | 2018 | high | high | unclear | unclear | low | low | high: no control group |
| Lorenzetti et al. | 2018 | low | low | unclear | unclear | low | low | high: small sample size/no control group |
| Bornioli et al. | 2019 | high | high | unclear | unclear | low | low | high: no control group |
| Authors | Year | Sample (N) | Sample Characteristics | Mean Age (SD or Range) | VR Task | VR Set-Up | Emotion Regulation/Wellbeing Assessment | Primary Outcomes | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Villani & Riva [42] | 2008 | 60 healthy adults | Experimental Group (EG) for three conditions 45 persons (15 for each condition) Control Group (CG) without treatment 15 persons | Range 21–28 years old | relaxation environment + relaxing narrative | Immersive VR Condition: Sony Glastron PLM S-700 with a head-tracker: Intersense Intertrax2 and Semi-immersive DVD Condition: pc (Fujitsu Siemens AMILO Processor, Pentium 4 | State-Trait Anxiety Inventory (STAI) and Positive And Negative Affect Scale (PANAS), Visual Analogue Scale (VAS), Coping Orientation to Problems Experienced Questionnaire (COPE) + Physiological Parameters: Respiration Rate, Respiration amplitude, Heart Rate, Heart Amplitude, Skin Conductance, Electromyography | Results show a significant reduction of anxiety and a significant improvement of positive emotional states—in particular, relaxation—measured through self-report questionnaires in all conditions. Physiological parameters showed some good changes related to respiration rate, heart rate, and skin conductance parameters, but less than expected. |
| 2 | Tong et al. [43] | 2015 | 13 patients with chronic pain | EG, 7 patients (3 male, 4 female) CG, 6 patients (3 male, 3 female) | Range 35–55 years old (mean = 49, SD = 8.2) | The Virtual Meditative Walk (VMW) + biofeedback | Immersive environment stereoscopic VR display | Numerical Rating Scale (NRS) for Self-Report Pain Levels (values 0–10) | These findings indicate that the VMW (VR paired with biofeedback for MBSR training) was significantly more effective than MBSR alone at reducing reported pain levels among participants. |
| 3 | Cikajlo et al. [44] | 2016 | 8 healthy adults and patients | EG, all participants (of which 4 patients with TBI, one with a brain tumor and 4 workers) | Healthy participants Range 27–40 years old; Patients participants Range 24–48 years old | Mindfulness-Based Stress Reduction VR | Immersive head-mounted display Samsung Gear + Samsung Smartphone S6 and Note4 | Mindfulness Attention Awareness Scale (MASS) Satisfaction With Life Scale (SWLS) Mini-Mental State Examination Test (MMSE) | Patients achieved very high level of satisfaction (SWLS) at the end of the study. A slight increase in MASS score is also noticeable. All patients had MMSE score 30, except one; his score was 19 at the beginning, 29 at midterm and 26 at the end of the study. |
| 4 | Hasan et al. [45] | 2016 | 27 older adults | Elderly group Seniors group | Older Range 70–98 years old; Seniors Range 50–70 years old | Weekly classes for developing ICT skills in aged-care facilities for 2 years | Non-immersive laptops and tablet | Social Care-Related Quality of Life (SCRQoL) | During the 2-year study, the participants developed various computing capabilities. The use of ICT appears to contribute positively to the wellbeing of the elderly: connection, self-worth/ esteem and personal development, productivity, occupation, self-sufficiency, being in control, and enjoyment. |
| 5 | Konrad et al. [41] | 2016 | 128 healthy adults | 34 in the Incongruent Negative group, 34 in the Congruent Negative group, 30 in the Incongruent Positive and 30 in the Congruent Positive group | Range 18–62 years old (M = 24.56, SD = 8.87); 91 female and 37 male | MoodAdaptor—a technology-mediated reflection (TMR) application | Non-immersive mobile app | Subjective Happiness Scale, Satisfaction With Life Scale, Ryff Scales of Psychological Well-Being and Personal Emotion Scale Participants. | Autobiographical memory enhances positive mood through well-documented self- enhancement biases. Negative thoughts when in a positive mood reduced current mood, while positive thoughts, when in a negative mood, enhances it. Selecting incongruent memories is useful for mood-regulation and consequently for improving wellbeing. |
| 6 | Baez et al. [46] | 2017 | 40 older adults | EG, 20 participants CG, 20 participants | Range 65–87 years old | OTAGO personalized exercise program for fall prevention | Non-immersive tablet-based application (10.1inch Sony Xperia tablet) | Physical Activity Enjoyment Scale (PACES), Wellbeing Scale of the Multidimensional Personality Questionnaire (MPQ), Trans Theoretical Model of Behavior Change (TTM), R-UCLA Loneliness Scale | In virtual group exercising, people with lesser physical skills improve to the level of the more fit participants. These results suggest that: the online group could overcome some of the major issues reported in the literature in terms of the negative effect of group-exercising in the motivation of heterogeneous groups; and it helped reduce the effect of the initial skill level and motivation levels of participants in comparison to the trainees complying with the group norm. |
| 7 | Singh et al. [47] | 2017 | 15 patients with motor disabilities | EG | Mean age = 22.7, SD = 4.2 | Physical activity task | Non-immersive Nintendo® Wii Fit | Depressive, Anxiety and Stress Scales (DASS) | The results of this study demonstrated that there was a significant difference in psychological well-being and reaction time after intervention using interactive VR games. |
| 8 | Weerdmeester et al. [48] | 2017 | 72 healthy adults | EG | Range 18–30 (M = 21.5, SD = 2.7); 31% male, 69% female | DEEP VR a virtual reality biofeedback game | Immersive VR game + biofeedback | Trier Social Stress Test | These results provide a promising outlook for using biofeedback video games such as DEEP to help individuals learn how to regulate their physiological arousal engagingly. |
| 9 | Bornioli et al. [49] | 2018 | 269 healthy adults and older adults | EG, all participants see five different environments | Range 18–67 years old (M = 31.69, SD = 13.63; 30.9% male, 69.1% females | exposure urban walking task | Non-immersive laptop | University of Wales Institute of Science and Technology Mood Adjective Checklist (UWIST MACL scale), Russell’s circumplex model of affect, Perceived Restorativeness Scale—Short Version (PRS scale) | This study sets out to investigate the immediate psychological wellbeing benefits of virtual exposure to different urban walking settings. The results suggest that walking in high-quality urban settings can have positive outcomes and highlight the negative role of traffic and the potential benefits of historical elements in the affective walking experience. |
| 10 | Lorenzetti et al. [51] | 2018 | 8 healthy adults | EG | Range 23–28 years old | exposure to an autumnal nature environment | Non-Immersive virtual environments in a brain-computer interface (BCI) + rrtfMRI-NFB | Beck Depression Inventory (BDI), Trait Anxiety Inventory (STAI) and Positive And Negative Affect Scale (PANAS), Emotion Regulation Questionnaire (ERQ) and Satisfaction with Life Scale (SLS) | The study provides a novel proof of concept and demonstrates the feasibility of the implementation of rtfMRI-NFB using virtual environment and music to elicit the neural activity and measure the neural correlates of specific, complex emotional states. Real-time up-regulation of tenderness engaged the hypothalamic septum area and other regions previously implicated in positive affiliative emotions (i.e., medial frontal cortex and temporal pole, precuneus). |
| 11 | Bornioli et al. [50] | 2019 | 384 healthy adults and older adults | EG, all participants see five different environments | Range 18–67 years old (M = 35.01, SD = 13.89) | exposure urban walking task | Non-immersive laptop | University of Wales Institute of Science and Technology Mood Adjective Checklist (UWIST MACL scale), Russell’s Circumplex Model of Affect, Perceived Restorativeness Scale—Short Version (PRS scale) | Results show the crucial features that make walking positive for psychological wellbeing and encourage walking intentions are perceived safety, comfort, and moderate stimulation. |
| Study | Sample (Type of) | VE Characteristics | VE Content | Aim of the VR Task |
|---|---|---|---|---|
| Virtual Environments for Healthy Participants | ||||
| Villani and Riva (2008) [42] | Healthy | Immersive | A waterfall and a beach of an island | Relaxation and enhancement of wellbeing |
| Konrad et al. (2016) [41] | Healthy | Non-immersive | Mood survey | Mood regulation and improvement wellbeing |
| Weerdmester et al. (2017) [48] | Healthy | Immersive | Underwater world | Regulation of physiological arousal |
| Bornioli et al. (2018) [49] | Healthy | Non-immersive | Five different pedestrian areas of a town | Enhancement of behavioral activation for wellbeing |
| Lorenzetti et al. (2018) [51] | Healthy | Non-immersive | A landscape of hills and cornfields | Regulation of physiological arousal |
| Bornioli et al. (2019) [50] | Healthy | Non-immersive | Five different pedestrian areas of a town | Enhancement of behavioral activation for wellbeing |
| Virtual Environments for Patients | ||||
| Tong et al. (2015) [43] | Clinical | Immersive | Walk in the forest | Mindfulness-based stress reduction |
| Cikajlo et al. (2016) [44] | Clinical | Immersive | A river and a mountain landscape | Mindfulness-based stress reduction |
| Singh et al. (2017) [47] | Clinical | Non-immersive | Three different sports: tennis, bowling, and boxing | Enhancement of behavioral activation for wellbeing |
| Study | Sample (Type of) | VE Characteristics | VE Content | Aim of the VR Task |
|---|---|---|---|---|
| Virtual Environments for healthy participants | ||||
| Hasan et al. (2016) [45] | Healthy | Non-immersive | Social networks, emails | Enhancement of ICT-skills for the improvement of social functioning and wellbeing |
| Baez et al. (2017) [46] | Healthy | Non-immersive | A gymnasium | Enhancement of behavioral activation for fall prevention and wellbeing |
| Bornioli et al. (2018) [49] | Healthy | Non-immersive | Five different pedestrian areas of a town | Enhancement of behavioral activation for wellbeing |
| Bornioli et al. (2019) [50] | Healthy | Non-immersive | Five different pedestrian areas of a town | Enhancement of behavioral activation for wellbeing |
| Scale | Description of Measure |
|---|---|
| State-Trait Anxiety Inventory (STAI) | A commonly used measure of trait and state anxiety. It can be used in clinical settings to diagnose anxiety and to distinguish it from depressive syndromes. Form Y, is its most popular version. It has 20 items for assessing trait anxiety and 20 for state anxiety. All items are rated on a 4-point scale (e.g., from “Almost Never” to “Almost Always”). Higher scores indicate greater anxiety. |
| Positive And Negative Affect Scale (PANAS) | A self-report questionnaire that consists of two 10-item scales to measure both positive and negative affect. Each item is rated on a 5-point scale of 1 (not at all) to 5 (very much). |
| Coping Orientation to Problems Experienced Questionnaire (COPE) | A self-reported questionnaire developed to assess a broad range of coping responses with a score on a 4-point scale (e.g., from “I usually don’t do this at all” to “I usually do this a lot”). There are two main components to the COPE inventory: problem-focused coping and emotion-focused coping. |
| Mindfulness Attention Awareness Scale (MASS) | A 15-item scale designed to assess a core characteristic of mindfulness, namely, a receptive state of mind in which attention, informed by a sensitive awareness of what is occurring in the present, simply observes what is taking place. |
| Satisfaction With Life Scale (SWLS) | A 5-item scale designed to measure global cognitive judgments of one’s life satisfaction (not a measure of either positive or negative affect). Participants indicate how much they agree or disagree with items on a 7-point scale (e.g., from 1 “strongly disagree” to 7 “strongly agree”). |
| Subjective Happiness Scale | A 4-item self-report measure developed to assess an individual’s overall happiness as measured through self-evaluation on a 7-point Likert-type scale. |
| Ryff Scales of Psychological Well-Being | A psychometric inventory in which respondents rate statements on a scale of 1 to 6 (e.g., from 1 “strong disagreement” to 6 “strong agreement”). It is based on six factors: autonomy, environmental mastery, personal growth, positive relations with others, purpose in life, and self-acceptance. Higher total scores indicate higher psychological well-being. |
| Wellbeing scale of the Multidimensional Personality Questionnaire (MPQ) | A personality test meant to measure personality that gives ratings on four broad traits: Positive Emotional Temperament, Negative Emotional Temperament, Constraint, and Absorption. High scorers on the specific wellbeing scale describe: having a cheerful happy disposition; feeling good about themselves; seeing a bright future ahead; being optimists; living interesting, exciting lives; enjoying the things they are doing. |
| Depressive, Anxiety and Stress Scales (DASS) | A 42-item self report instrument designed to measure the three related negative emotional states of depression, anxiety and tension/stress. The rating is based on a 0-3 point scale (e.g., from 0 “Did not apply to me at all” to 1 “Applied to me very much or most of the time”). |
| Emotion Regulation Questionnaire (ERQ) | A 10-item scale designed to measure respondents’ tendency to regulate their emotions in two ways: (1) Cognitive Reappraisal and (2) Expressive Suppression. Respondents answer each item on a 7-point Likert-type scale (e.g., from 1 “strongly disagree” to 7 “strongly agree”). |
| University of Wales Institute of Science and Technology Mood Adjective Checklist (UWIST MACL scale) | A scale that measures self-reported mood in the dimensions of energetic arousal, tense arousal, and hedonic tone. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montana, J.I.; Matamala-Gomez, M.; Maisto, M.; Mavrodiev, P.A.; Cavalera, C.M.; Diana, B.; Mantovani, F.; Realdon, O. The Benefits of emotion Regulation Interventions in Virtual Reality for the Improvement of Wellbeing in Adults and Older Adults: A Systematic Review. J. Clin. Med. 2020, 9, 500. https://doi.org/10.3390/jcm9020500
Montana JI, Matamala-Gomez M, Maisto M, Mavrodiev PA, Cavalera CM, Diana B, Mantovani F, Realdon O. The Benefits of emotion Regulation Interventions in Virtual Reality for the Improvement of Wellbeing in Adults and Older Adults: A Systematic Review. Journal of Clinical Medicine. 2020; 9(2):500. https://doi.org/10.3390/jcm9020500
Chicago/Turabian StyleMontana, Jessica Isbely, Marta Matamala-Gomez, Marta Maisto, Petar Aleksandrov Mavrodiev, Cesare Massimo Cavalera, Barbara Diana, Fabrizia Mantovani, and Olivia Realdon. 2020. "The Benefits of emotion Regulation Interventions in Virtual Reality for the Improvement of Wellbeing in Adults and Older Adults: A Systematic Review" Journal of Clinical Medicine 9, no. 2: 500. https://doi.org/10.3390/jcm9020500
APA StyleMontana, J. I., Matamala-Gomez, M., Maisto, M., Mavrodiev, P. A., Cavalera, C. M., Diana, B., Mantovani, F., & Realdon, O. (2020). The Benefits of emotion Regulation Interventions in Virtual Reality for the Improvement of Wellbeing in Adults and Older Adults: A Systematic Review. Journal of Clinical Medicine, 9(2), 500. https://doi.org/10.3390/jcm9020500