Prognostic Value of Troponin Elevation in COVID-19 Hospitalized Patients

 , , , ,
, , , ,  and
and 
Abstract
1. Introduction
2. Experimental Section
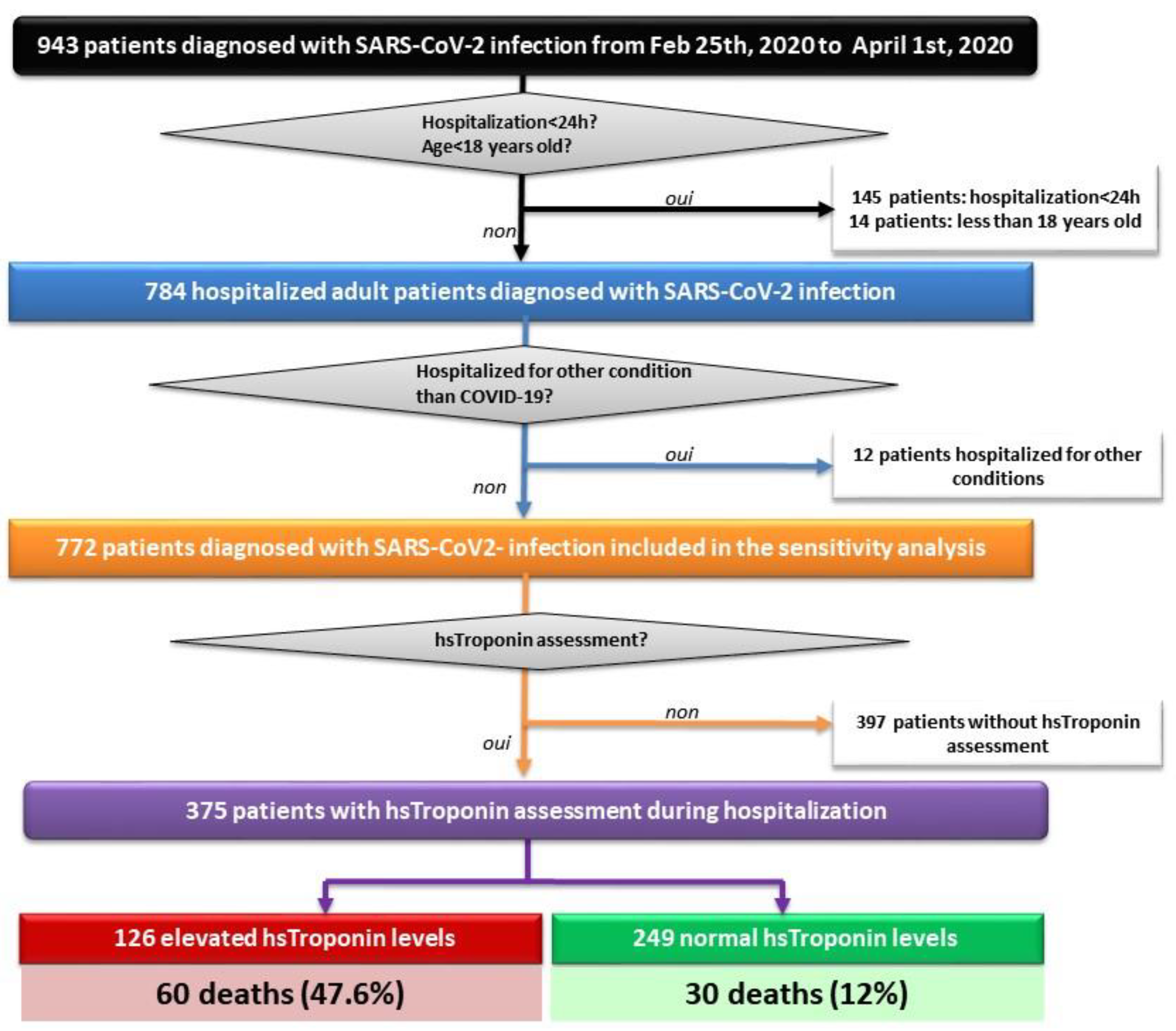
2.1. Study Design and Patient Selection
2.2. Baseline Variables
2.3. Outcome Assessment
2.4. Statistical Analysis
3. Results
3.1. Patients Characteristics at Baseline
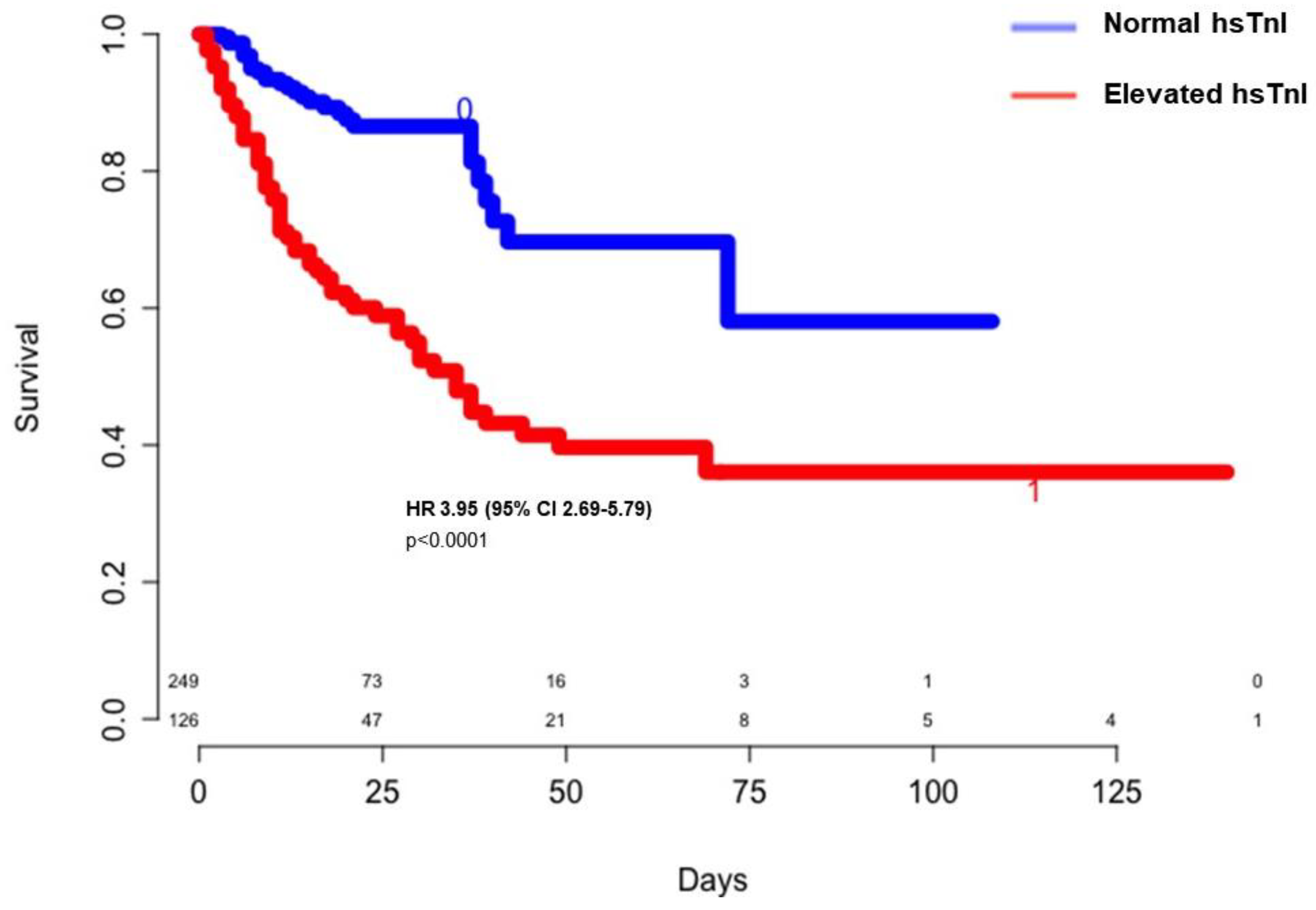
3.2. Troponin Elevation and in Hospital Outcomes
3.3. Mortality Predictors
4. Discussion
4.1. Troponin Elevation and in-Hospital Mortality
4.2. Myocardial Injury in COVID-19: Definition and Potential Mechanisms
4.3. Limitations
4.4. Further Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Li, B.; Yang, J.; Zhao, F.; Zhi, L.; Wang, X.; Liu, L.; Bi, Z.; Zhao, Y. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin. Res. Cardiol. 2020, 109, 531–538. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, Y.; Wu, L.; Niu, S.; Song, C.; Zhang, Z.; Lu, G.; Qiao, C.; Hu, Y.; Yuen, K.-Y.; et al. Structural and Functional Basis of SARS-CoV-2 Entry by Using Human ACE2. Cell 2020, 181, 894–904.e9. [Google Scholar] [CrossRef] [PubMed]
- Yan, R.; Zhang, Y.; Li, Y.; Xia, L.; Guo, Y.; Zhou, Q. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science 2020, 367, 1444–1448. [Google Scholar] [CrossRef]
- Samavati, L.; Uhal, B.D. ACE2, Much More Than Just a Receptor for SARS-COV-2. Front. Cell. Infect. Microbiol. 2020, 10. [Google Scholar] [CrossRef]
- Chen, L.; Li, X.; Chen, M.; Feng, Y.; Xiong, C. The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2. Cardiovasc. Res. 2020, 116, 1097–1100. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Januzzi, J.L. Troponin and BNP Use in COVID-19. 2020. Available online: https://www.acc.org/latest-incardiology/articles/2020/03/18/15/25/troponin-and-bnp-use-in-covid19 (accessed on 8 November 2020).
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811. [Google Scholar] [CrossRef]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury with Mortality in Hospitalized Patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef]
- Lala, A.; Johnson, K.W.; Januzzi, J.L.; Russak, A.J.; Paranjpe, I.; Richter, F.; Zhao, S.; Somani, S.; Van Vleck, T.; Vaid, A.; et al. Prevalence and Impact of Myocardial Injury in Patients Hospitalized with COVID-19 Infection. J. Am. Coll. Cardiol. 2020, 76, 533–546. [Google Scholar] [CrossRef] [PubMed]
- Zou, F.; Qian, Z.; Wang, Y.; Zhao, Y.; Bai, J. Cardiac Injury and COVID-19: A Systematic Review and Meta-analysis. CJC Open 2020, 2, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Majure, D.T.; Gruberg, L.; Saba, S.G.; Kvasnovsky, C.; Hirsch, J.S.; Jauhar, R. Usefulness of Elevated Troponin to Predict Death in Patients with COVID-19 and Myocardial Injury. Am. J. Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Manocha, K.K.; Kirzner, J.; Ying, X.; Yeo, I.; Peltzer, B.; Ang, B.; Li, H.A.; Lerman, B.B.; Safford, M.M.; Goyal, P.; et al. Troponin and Other Biomarker Levels and Outcomes Among Patients Hospitalized with COVID-19: Derivation and Validation of the HA 2 T 2 COVID-19 Mortality Risk Score. J. Am. Hear. Assoc. 2020, e018477. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.B.; Mikkelsen, E.M.; Cronin-Fenton, D.P.; Kristensen, N.R.; Pham, T.M.; Pedersen, L.; Petersen, I. Missing data and multiple imputation in clinical epidemiological research. Clin. Epidemiol. 2017, 9, 157–166. [Google Scholar] [CrossRef] [PubMed]
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–68. [Google Scholar] [CrossRef]
- De Almeida, G.L.G.; Braga, F.; Jorge, J.K.; Nobre, G.F.; Kalichsztein, M.; Faria, P.D.M.P.D.; Bussade, B.; Penna, G.L.; Alves, V.O.; Pereira, M.A.; et al. Valor Prognóstico da Troponina T e do Peptídeo Natriurético Tipo B em Pacientes Internados por COVID-19. Arq. Bras. Cardiol. 2020, 115, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Kavsak, P.A.; Hammarsten, O.; Worster, A.; Smith, S.W.; Apple, F.S. OUP accepted manuscript. Clin. Chem. 2020. [Google Scholar] [CrossRef]
- Bangalore, S.; Sharma, A.; Slotwiner, A.; Yatskar, L.; Harari, R.; Shah, B.; Ibrahim, H.; Friedman, G.H.; Thompson, C.; Alviar, C.L.; et al. ST-Segment Elevation in Patients with Covid-19—A Case Series. N. Engl. J. Med. 2020, 382, 2478–2480. [Google Scholar] [CrossRef] [PubMed]
- Giustino, G.; Croft, L.B.; Stefanini, G.G.; Bragato, R.; Silbiger, J.J.; Vicenzi, M.; Danilov, T.; Kukar, N.; Shaban, N.; Kini, A.; et al. Characterization of Myocardial Injury in Patients with COVID-19. J. Am. Coll. Cardiol. 2020, 76, 2043–2055. [Google Scholar] [CrossRef] [PubMed]
- Chapman, A.R.; Bularga, A.; Mills, N.L. High-Sensitivity Cardiac Troponin Can Be an Ally in the Fight against COVID-19. Circulation 2020, 141, 1733–1735. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall Cohort N (%)/M(IQR) | Elevated hsTnI N (%)/M(IQR) | Normal hsTnI N (%)/M(IQR) | p-Value | SMD | |
|---|---|---|---|---|---|
| n | 375 | 126 | 249 | ||
| Age (years) | 66 (55.5–74) | 71.5 (64.2–79) | 63 (51–71) | <0.001 | 0.627 |
| Age ≥ 65 years old | 210 (56) | 94 (74.6) | 116 (46.6) | <0.001 | 0.598 |
| Male | 252 (67.2) | 82 (65.1) | 170 (68.3) | 0.61 | 0.076 |
| BMI (kg/m2) (n = 337) | 28 (25–32) | 29 (26–34) | 28 (25–31) | 0.04 | 0.035 |
| eGFR (mL/min/1.73 m2) on admission | 81 (50–96) | 55.5 (28–84) | 86 (70–100) | <0.001 | 0.816 |
| Cardiovascular risk factors | |||||
| Hypertension (n = 374) | 221 (58.9) | 96 (76.2) | 125 (50.2) | <0.001 | 0.575 |
| Diabetes (n = 374) | 126 (33.6) | 59 (46.8) | 67 (26.9) | <0.001 | 0.430 |
| Dyslipidemia (n = 374) | 144 (38.4) | 66 (52.4) | 78 (31.3) | <0.001 | 0.446 |
| Smoking (history or current) (n = 330) | 80 (21.3) | 30 (23.8) | 50 (20.1) | 0.36 | 0.121 |
| Obesity (n = 347) | 134 (35.7) | 51 (40.5) | 83 (33.3) | 0.20 | 0.122 |
| Medical history | |||||
| Heart disease (n = 374) | 65 (17.3) | 31 (24.6) | 34 (13.7) | 0.007 | 0.305 |
| Ischemic heart disease | 48 (12.8) | 21 (16.7) | 27 (10.8) | 0.15 | 0.173 |
| Chronic heart failure | 20 (5.3) | 12 (9.5) | 8 (3.2) | 0.009 | 0.263 |
| HFrEF | 13 (3.5) | 7 (5.5) | 6 (2.4) | 0.20 | 0.478 |
| Chronic kidney disease (n = 374) | 65 (17.3) | 32 (25.4) | 33 (13.2) | 0.003 | 0.316 |
| Chronic respiratory disease (n = 374) | 45 (12) | 16 (12.7) | 29 (11.6) | 0.73 | 0.305 |
| Active cancer | 18 (4.8) | 9 (7.1) | 9 (3.6) | 0.20 | 0.157 |
| Cognitive impairment (n = 374) | 15 (4) | 7 (5.5) | 8 (3.2) | 0.19 | 0.117 |
| VTE (n = 374) | 22 (5.9) | 11 (8.7) | 11 (4.4) | 0.07 | 0.177 |
| Admission treatment | |||||
| Antithrombotic treatment | 121 (32.3) | 55 (43.7) | 66 (26.5) | <0.001 | 0.387 |
| Antiplatelet | 89 (23.7) | 37 (29.4) | 52 (20.9) | 0.007 | 0.212 |
| Anticoagulation | 41 (10.9) | 23 (18.3) | 18 (7.2) | <0.001 | 0.351 |
| Antihypertensive drugs | |||||
| RASi | 150 (40) | 63 (50) | 87 (34.9) | 0.006 | 0.308 |
| Diuretics | 83 (22.1) | 41 (32.5) | 42 (16.9) | <0.001 | 0.387 |
| Beta-blockers | 103 (27.5) | 47 (37.3) | 56 (22.5) | <0.001 | 0.354 |
| Admission Low-dose chest CT * | 320 (85.3) | 102 (81) | 218 (87.6) | 1 | 0.009 |
| abnormal | 314 (98.1) | 100 (98) | 245 (98.4) | 1 | |
| COVID-19 infection severity indicators | |||||
| Oxygen therapy flow rate of >5 L/min | 231 (67.9) | 82 (77.4) | 149 (63.7) | 0.01 | 0.304 |
| ICU admission | 215 (57.6) | 85 (67.5) | 130 (52.6) | 0.008 | 0.307 |
| Intubation | 205 (54.8) | 84 (66.7) | 121 (48.8) | 0.001 | 0.353 |
| HFNO therapy/NIV | 10 (2.7) | 1 (0.8) | 9 (3.6) | 0.17 | |
| CT scan extension > 25% (n = 320) | 179 (47.7) | 69 (54.8) | 110 (44.2) | 0.052 | 0.655 |
| CRP ≥ 100 mg/L (n = 371) | 270 (72) | 106 (84.1) | 164 (65.9) | <0.001 | 0.458 |
| D-dimer count ≥ 3000 µg/L (n = 292) | 170 (45.3) | 77 (61.1) | 93 (37.3) | <0.001 | 0.546 |
| Lymphopenia < 1000/µL (n = 371) | 284 (75.7) | 104 (82.5) | 180 (72.2) | 0.026 | 0.276 |
| In-hospital treatment | |||||
| Prophylactic/therapeutic anticoagulation | 329 (88.2) | 108 (86.4) | 221 (89.1) | 0.55 | |
| Antibiotics | 331 (88.3) | 109 (86.5) | 222 (89.2) | 0.49 | |
| Antiviral $ | 199 (53.1) | 60 (47.6) | 139 (55.8) | 1 | |
| In-hospital outcomes | |||||
| Death | 90 (24) | 60 (47.6) | 30 (12) | <0.001 | 0.844 |
| Severe sepsis or septic shock | 98 (27.2) | 47 (37.9) | 51 (21.6) | <0.001 | 0.389 |
| Acute renal impairment | 136 (36.3) | 77 (61.1) | 59 (23.7) | <0.001 | 0.851 |
| VTE | 57 (15.2) | 25 (19.8) | 32 (12.9) | 0.10 | 0.190 |
| Stroke/TIA | 16 (4.3) | 10 (7.9) | 6 (2.4) | 0.026 | 0.289 |
| Hospital length of stay (days) | 15 (8–29) | 16.5 (8–35) | 15 (8–27) | 0.26 | 0.277 |
| Risk Factor | Unadjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age ≥ 65 years old | 5.55 (3.12–10.47) | <0.001 | 3.17 (1.45–7.18) | 0.004 |
| High blood pressure | 2.08 (1.25–3.55) | 0.005 | 0.78 (0.28–2.10) | 0.63 |
| Diabetes mellitus | 1.66 (1.01–2.71) | 0.04 | 0.95 (0.40–2.15) | 0.90 |
| Dyslipidemia | 1.60 (0.98–2.59) | 0.054 | 0.54 (0.22–1.25) | 0.16 |
| Tobacco consumption | 2.33 (1.33–4.04) | 0.002 | 1.99 (0.89–4.49) | 0.09 |
| Active Cancer | 5.52 (2.10–15.47) | <0.001 | 2.80 (0.67–11.65) | 0.15 |
| Chronic kidney disease | 3.07 (1.74–5.41) | <0.001 | 2.30 (0.84–6.41) | 0.10 |
| Ischemic heart disease | 2.39 (1.25–4.50) | 0.007 | 1.02 (0.30–3.36) | 0.96 |
| Chronic heart failure | 5.39 (2.15–14.22) | <0.001 | 0.93 (0.17–4.86) | 0.94 |
| Previous antithrombotic drug | 2.52 (1.54–4.13) | <0.001 | 1.72 (0.70–4.26) | 0.23 |
| Previous RASi | 1.61 (1.00–2.60) | 0.049 | 1.40 (0.55–3.61) | 0.47 |
| Lymphopenia | 2.35 (1.25–4.77) | 0.011 | 3.05 (0.90–14.35) | 0.10 |
| CRP ≥ 100 mg/L (max) | 3.26 (1.71–6.76) | <0.001 | 3.62 (1.12–13.98) | 0.042 |
| D-dimer count (max) ≥ 3000 µg/L | 2.52 (1.42–4.62) | 0.002 | 1.55 (0.70–3.55) | 0.28 |
| hsTroponin elevation | 6.63 (3.98–11.25) | <0.001 | 3.12 (1.49–6.65) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cordeanu, E.-M.; Duthil, N.; Severac, F.; Lambach, H.; Tousch, J.; Jambert, L.; Mirea, C.; Delatte, A.; Younes, W.; Frantz, A.-S.; et al. Prognostic Value of Troponin Elevation in COVID-19 Hospitalized Patients. J. Clin. Med. 2020, 9, 4078. https://doi.org/10.3390/jcm9124078
Cordeanu E-M, Duthil N, Severac F, Lambach H, Tousch J, Jambert L, Mirea C, Delatte A, Younes W, Frantz A-S, et al. Prognostic Value of Troponin Elevation in COVID-19 Hospitalized Patients. Journal of Clinical Medicine. 2020; 9(12):4078. https://doi.org/10.3390/jcm9124078
Chicago/Turabian StyleCordeanu, Elena-Mihaela, Nicolas Duthil, Francois Severac, Hélène Lambach, Jonathan Tousch, Lucas Jambert, Corina Mirea, Alexandre Delatte, Waël Younes, Anne-Sophie Frantz, and et al. 2020. "Prognostic Value of Troponin Elevation in COVID-19 Hospitalized Patients" Journal of Clinical Medicine 9, no. 12: 4078. https://doi.org/10.3390/jcm9124078
APA StyleCordeanu, E.-M., Duthil, N., Severac, F., Lambach, H., Tousch, J., Jambert, L., Mirea, C., Delatte, A., Younes, W., Frantz, A.-S., Merdji, H., Schini-Kerth, V., Bilbault, P., Ohlmann, P., Andres, E., & Stephan, D. (2020). Prognostic Value of Troponin Elevation in COVID-19 Hospitalized Patients. Journal of Clinical Medicine, 9(12), 4078. https://doi.org/10.3390/jcm9124078