The Performance of Vascular Age in the Assessment of Cardiovascular Risk of Patients with Rheumatoid Arthritis

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Included in the Study
2.2. Laboratory Assessment and Data Collection
2.3. Carotid Ultrasound Evaluation
2.4. Statistical Analysis
3. Results
3.1. Demographic, Laboratory and Disease-Related Data
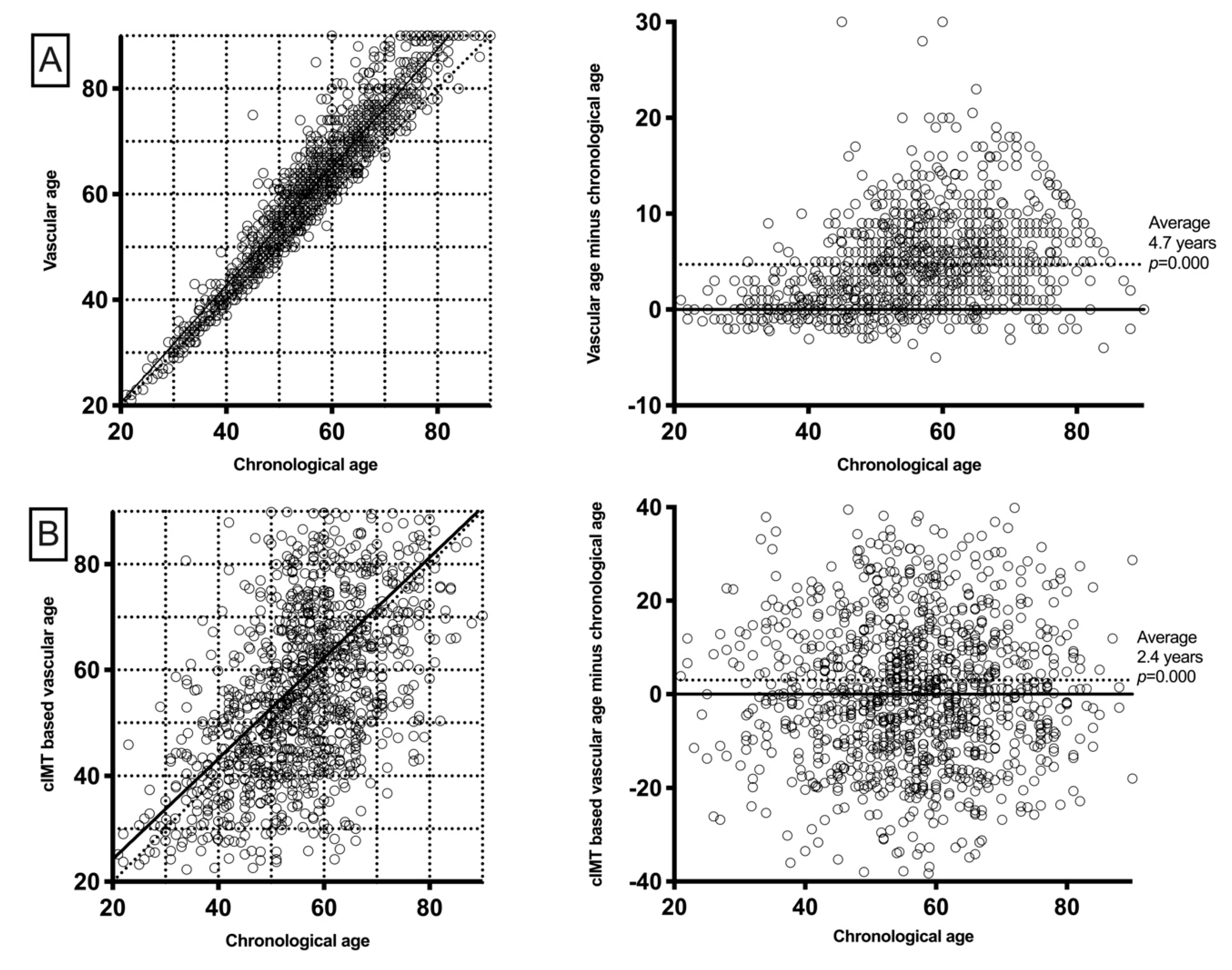
3.2. Vascular Age and cIMT-Based Vascular Age Relation to Chronological Age
3.3. VA Performance for the Presence of Carotid Plaque
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Aviña-Zubieta, J.A.; Choi, H.K.; Sadatsafavi, M.; Etminan, M.; Esdaile, J.M.; Lacaille, D. Risk of cardiovascular mortality in patients with rheumatoid arthritis: A meta-analysis of observational studies. Arthritis Care Res. 2008, 59, 1690–1697. [Google Scholar] [CrossRef] [PubMed]
- Arts, E.E.A.; Popa, C.; Den Broeder, A.A.; Semb, A.G.; Toms, T.; Kitas, G.D.; van Riel, P.L.; Fransen, J. Performance of four current risk algorithms in predicting cardiovascular events in patients with early rheumatoid arthritis. Ann. Rheum. Dis. 2015, 74, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Kawai, V.K.; Chung, C.P.; Solus, J.F.; Oeser, A.; Raggi, P.; Stein, C.M. The ability of the 2013 American College of Cardiology/American Heart Association cardiovascular risk score to identify rheumatoid arthritis patients with high coronary artery calcification scores. Arthritis Rheumatol. 2015, 67, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Cuende, J.I.; Cuende, N.; Calaveras-Lagartos, J. How to calculate vascular age with the SCORE project scales: A new method of cardiovascular risk evaluation. Eur. Heart J. 2010, 31, 2351–2358. [Google Scholar] [CrossRef]
- Cooney, M.T.; Vartiainen, E.; Laatikainen, T.; De Bacquer, D.; McGorrian, C.; Dudina, A.; Graham, I. Cardiovascular risk age: Concepts and practicalities. Heart 2012, 98, 941–946. [Google Scholar] [CrossRef]
- Stein, J.H. Carotid intima-media thickness and vascular age: You are only as old as your arteries look. J. Am. Soc. Echocardiogr. 2004, 17, 686–689. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Prevoo, M.L.; van ’t Hof, M.A.; Kuper, H.H.; van Leeuwen, M.A.; van de Putte, L.B.; van Riel, P.L. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995, 38, 44–48. [Google Scholar] [CrossRef]
- Smolen, J.S.; Breedveld, F.C.; Schiff, M.H.; Kalden, J.R.; Emery, P.; Eberl, G.; van Riel, P.L.; Tugwell, P. A simplified disease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology 2003, 42, 244–257. [Google Scholar] [CrossRef]
- Aletaha, D.; Smolen, J. The Simplified Disease Activity Index (SDAI) and the Clinical Disease Activity Index (CDAI): A review of their usefulness and validity in rheumatoid arthritis. Clin. Exp. Rheumatol. 2005, 23, S100–S108. [Google Scholar]
- Aletaha, D.; Ward, M.M.; Machold, K.P.; Nell, V.P.K.; Stamm, T.; Smolen, J.S. Remission and active disease in rheumatoid arthritis: Defining criteria for disease activity states. Arthritis Rheum. 2005, 52, 2625–2636. [Google Scholar] [CrossRef] [PubMed]
- Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef]
- Grau, M.; Subirana, I.; Marrugat, J.; Elosua, R. Percentiles of Carotid Intima-media Thickness in a Spanish Population With and Without Cardiovascular Risk Factors. Rev. Española Cardiol. 2013, 66, 749–751. [Google Scholar] [CrossRef]
- Corrales, A.; González-Juanatey, C.; Peiró, M.E.; Blanco, R.; Llorca, J.; González-Gay, M.A. Carotid ultrasound is useful for the cardiovascular risk stratification of patients with rheumatoid arthritis: Results of a population-based study. Ann. Rheum. Dis. 2014, 73, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Corrales, A.; Parra, J.A.; González-Juanatey, C.; Rueda-Gotor, J.; Blanco, R.; Llorca, J.; González-Gay, M.A. Cardiovascular risk stratification in rheumatic diseases: Carotid ultrasound is more sensitive than coronary artery calcification score to detect subclinical atherosclerosis in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2013, 72, 1764–1770. [Google Scholar] [CrossRef]
- Touboul, P.-J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Fatar, M.; et al. Mannheim carotid intima-media thickness consensus (2004–2006). An update on behalf of the Advisory Board of the 3rd and 4th Watching the Risk Symposium, 13th and 15th European Stroke Conferences, Mannheim, Germany, 2004, and Brussels, Belgium, 2006. Cerebrovasc. Dis. 2007, 23, 75–80. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Wibetoe, G.; Sexton, J.; Ikdahl, E.; Rollefstad, S.; Kitas, G.D.; Van Riel, P.; Gabriel, S.; Kvien, T.K.; Douglas, K.; Sandoo, A.; et al. Prediction of cardiovascular events in rheumatoid arthritis using risk age calculations: Evaluation of concordance across risk age models. Arthritis Res. Ther. 2020, 22. [Google Scholar] [CrossRef]
- Chambless, L.E.; Heiss, G.; Folsom, A.R.; Rosamond, W.; Szklo, M.; Sharrett, A.R.; Clegg, L.X. Association of coronary heart disease incidence with carotid arterial wall thickness and major risk factors: The Atherosclerosis Risk in Communities (ARIC) study, 1987–1993. Am. J. Epidemiol. 1997, 146, 483–494. [Google Scholar] [CrossRef]
- Gonzalez-Juanatey, C.; Llorca, J.; Martin, J.; Gonzalez-Gay, M.A. Carotid Intima-Media Thickness Predicts the Development of Cardiovascular Events in Patients with Rheumatoid Arthritis. Semin. Arthritis Rheum. 2009, 38, 366–371. [Google Scholar] [CrossRef]
- Adolphe, A.B.; Huang, X.; Cook, L.S. Carotid intima-media thickness determined vascular age and the framingham risk score. Crit. Pathw. Cardiol. 2011, 10, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Cuende, J.I. Vascular Age Versus Cardiovascular Risk: Clarifying Concepts. Rev. Española Cardiol. 2016, 69, 243–246. [Google Scholar] [CrossRef]
- Lopez-Gonzalez, A.A.; Aguilo, A.; Frontera, M.; Bennasar-Veny, M.; Campos, I.; Vicente-Herrero, T.; Tomas-Salva, M.; De Pedro-Gomez, J.; Tauler, P. Effectiveness of the Heart Age tool for improving modifiable cardiovascular risk factors in a Southern European population: A randomized trial. Eur. J. Prev. Cardiol. 2015, 22, 389–396. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| RA Patients | |
|---|---|
| (n = 1173) | |
| Age, years | 57 ± 12 |
| Female, n (%) | 917 (78) |
| Body mass index, kg/m2 | 28 ± 5 |
| Cardiovascular co-morbidity | |
| Smoking, n (%) | 307 (26) |
| Diabetes, n (%) | 0 (0) |
| Hypertension, n (%) | 285 (24) |
| Dyslipidemia, n (%) | 290 (25) |
| Obesity, n (%) | 327 (28) |
| Statins, n (%) | 252 (21) |
| Laboratory and lipid profile | |
| ESR, mm/1st h | 13 (6–25) |
| CRP, mg/L | 2.6 (0.9–6.3) |
| Cholesterol, mg/dL | 205 ± 36 |
| Triglycerides, mg/dL | 112 ± 63 |
| HDL cholesterol, mg/dL | 61 ± 17 |
| LDL cholesterol, mg/dL | 121 ± 31 |
| Atherogenic index | 3.57 ± 1.06 |
| Rheumatoid arthritis related data | |
| Disease duration, years | 4 (1–10) |
| Age of onset, years | 49 ± 14 |
| DAS28 | 3.05 ± 1.47 |
| DAS28-PCR | 2.81 ± 1.37 |
| SDAI | 10 (5–18) |
| CDAI | 9 (4–16) |
| Rheumatoid factor, n (%) | 694 (59) |
| ACPA, n (%) | 634 (54) |
| Prednisone intake, n (%) | 562 (48) |
| Current prednisone dose *, mg/day | 5 (3–6) |
| NSAIDs intake, n (%) | 471 (40) |
| DMARDs, n (%) | 909 (77) |
| Methotrexate, n (%) | 683 (58) |
| Leflunomide, n (%) | 131 (11) |
| Hydroxychloroquine, n (%) | 254 (22) |
| Anti TNF therapy, n (%) | 158 (13) |
| Abatacept, n (%) | 14 (1) |
| Tocilizumab, n (%) | 59 (5) |
| Rituximab, n (%) | 21 (2) |
| Tofacitinib, n (%) | 11 (1) |
| Baricitinib, n (%) | 9 (1) |
| Carotid assessment | |
| cIMT, microns | 690 ± 140 |
| Carotid plaque, n (%) | 587 (50) |
| cIMT Based Vascular Age | |||||
|---|---|---|---|---|---|
| Age | n | cIMT, Microns | cIMT Vascular Age, Years | Age Difference, Years | p |
| <40 | 115 | 538 | 36 ± 13 | 1 (−5–10) | 0.055 |
| 40–50 | 223 | 619 | 49 ± 15 | 1 (−6–10) | 0.005 |
| 50–60 | 393 | 690 | 60 ± 19 | 2 (−8–14) | 0.000 |
| 60–70 | 273 | 725 | 65 ± 19 | −1 (−14–11) | 0.916 |
| >80 | 168 | 811 | 78 ± 20 | −1 (−12–15) | 0.270 |
| SCORE-based vascular age | |||||
| Age | n | SCORE, % | Vascular age, years | Age difference, years | p |
| <40 | 115 | 0.0 (0.0–0.0) | 35 ± 7 | 0 (−1–2) | 0.030 |
| 40–50 | 223 | 0.2 (0.1–0.4) | 49 ± 5 | 2 (0–5) | 0.000 |
| 50–60 | 393 | 1.0 (0.6–1.7) | 61 ± 6 | 5 (2–8) | 0.000 |
| 60–70 | 273 | 3.0 (1.8–4.2) | 71 ± 6 | 5 (3–9) | 0.000 |
| >80 | 168 | 8.0 (5.1–12.8) | 83 ± 6 | 6 (3–9) | 0.000 |
| Age | n | SCORE, % | Carotid Plaque, n | SCORE AUC for Carotid Plaque | Vascular Age AUC for Carotid Plaque | p | OR (95% CI), p |
|---|---|---|---|---|---|---|---|
| <40 | 115 | 0.0 (0.0–0.0) | 4 | - | - | - | |
| 40–50 | 223 | 0.2 (0.1–0.4) | 45 | 0.711 (0.624–0.797) | 0.690 (0.605–0.776) | 0.40 | 1.19 (1.09–1.30), 0.000 |
| 50–60 | 393 | 1.0 (0.6–1.7) | 201 | 0.597 (0.541–0.653) | 0.596 (0.541–0,652) | 0.97 | 1.07 (1.02–1.12), 0.006 |
| 60–70 | 273 | 3.0 (1.8–4.2) | 188 | 0.590 (0.520–0.660) | 0.581 (0.510–0.651) | 0.49 | 1.04 (0.98–1.10), 0.16 |
| >80 | 168 | 8.0 (5.1–12.8) | 149 | 0.690 (0.588–0.794) | 0.710 (0.607–0.813) | 0.24 | 1.07 (0.96–1.20), 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferraz-Amaro, I.; Corrales, A.; Quevedo-Abeledo, J.C.; Atienza-Mateo, B.; Prieto-Peña, D.; Blanco, R.; Llorca, J.; González-Gay, M.Á. The Performance of Vascular Age in the Assessment of Cardiovascular Risk of Patients with Rheumatoid Arthritis. J. Clin. Med. 2020, 9, 4065. https://doi.org/10.3390/jcm9124065
Ferraz-Amaro I, Corrales A, Quevedo-Abeledo JC, Atienza-Mateo B, Prieto-Peña D, Blanco R, Llorca J, González-Gay MÁ. The Performance of Vascular Age in the Assessment of Cardiovascular Risk of Patients with Rheumatoid Arthritis. Journal of Clinical Medicine. 2020; 9(12):4065. https://doi.org/10.3390/jcm9124065
Chicago/Turabian StyleFerraz-Amaro, Iván, Alfonso Corrales, Juan Carlos Quevedo-Abeledo, Belén Atienza-Mateo, Diana Prieto-Peña, Ricardo Blanco, Javier Llorca, and Miguel Á. González-Gay. 2020. "The Performance of Vascular Age in the Assessment of Cardiovascular Risk of Patients with Rheumatoid Arthritis" Journal of Clinical Medicine 9, no. 12: 4065. https://doi.org/10.3390/jcm9124065
APA StyleFerraz-Amaro, I., Corrales, A., Quevedo-Abeledo, J. C., Atienza-Mateo, B., Prieto-Peña, D., Blanco, R., Llorca, J., & González-Gay, M. Á. (2020). The Performance of Vascular Age in the Assessment of Cardiovascular Risk of Patients with Rheumatoid Arthritis. Journal of Clinical Medicine, 9(12), 4065. https://doi.org/10.3390/jcm9124065