Resveratrol-Based Multivitamin Supplement Increases Sperm Concentration and Motility in Idiopathic Male Infertility: A Pilot Clinical Study

 , ,
, ,
Abstract
1. Introduction
2. Material and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ADP | phosphorylate adenosine diphosphate |
| ATP | production of adenosine triphosphate |
| DP | mitochondrial membrane potential |
| ETC | electron transfer chain |
| FADH2 | dihydroflavine-adenine dinucleotide |
| FOXOs | forkhead box transcription factor, class O |
| FSH | follicle-stimulating hormone |
| HSF1 | heat shock factor 1 |
| LH | luteinizing hormone |
| MTHFR | polymorphisms of the tetrahydrofolate methylene |
| NADH | nicotinamide adenine dinucleotide |
| NF-kB | kB gene binding nuclear factor |
| OXPHOS | oxidative phosphorylation |
| PPARγ | peroxisome proliferator-activated receptor γ |
| SIRT1 | sirtuin 1 |
References
- World Health Organization. WHO Manual for the Standardized Investigation and Diagnosis of the Infertile Couple; Cambridge University Press: New York, NY, USA, 2000. [Google Scholar]
- National Institute for Health and Care Excellence. Fertility Problems: Assessment and Treatment; NICE: London, UK, 2013; Available online: www.nice.org.uk/guidance/cg156 (accessed on 12 July 2017).
- Winters, B.R.; Walsh, T.J. The epidemiology of male infertility. Urol. Clin. 2014, 41, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Nieschlag, E.; Behre, H.M.; Nieschlag, S. (Eds.) Andrology: Male Reproductive Health and Dysfunction; Springer: Berlin, Germany, 2010. [Google Scholar]
- Jungwirth, A.; Giwercman, A.; Tournaye, H.; Diemer, T.; Kopa, Z.; Dohle, G.; Krausz, C.; EAU Working Group on Male Infertility. European Association of Urology Guidelines on Male Infertility: The 2012 Update. Eur. Urol. 2012, 62, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Fisch, H.; Goluboff, E.T.; Olson, J.H.; Feldshuh, J.; Broder, S.J.; Barad, D.H. Semen analyses in 1283 men from the United States over a 25-year period: No decline in quality. Fertil. Steril. 1996, 65, 1009–1014. [Google Scholar] [CrossRef]
- Fisch, H.; Braun, S.R. Trends in global semen parameter values. Asian J. Androl. 2013, 15, 169–173. [Google Scholar] [CrossRef]
- Carlsen, E.; Giwercman, A.; Keiding, N.; Skakkebaek, N.E. Evidence for decreasing quality of semen during past 50 years. BMJ 1992, 305, 609–613. [Google Scholar] [CrossRef]
- Mohanty, G.; Samanta, L. Redox regulation & sperm function: A proteomic insight. Indian J. Med. Res. 2018, 148, S84–S91. [Google Scholar]
- Palmero, S.; Bottazzi, C.; Costa, M.; Leone, M.; Fugassa, E. Metabolic Effects of L-Carnitine on Prepubertal Rat Sertoli Cells. Horm. Metab. Res. 2007, 32, 87–90. [Google Scholar] [CrossRef]
- Oeda, T.; Henkel, R.; Ohmori, H.; Schill, W.-B. Scavenging effect of Nacetyl-L-cysteine against reactive oxygen species in human semen:a possible therapeutic modality for male factor infertility? Andrologia 1997, 29, 125–131. [Google Scholar] [CrossRef]
- Ebisch, I.M.W.; Thomas, C.M.G.; Peters, W.H.M.; Braat, D.D.M.; Steegers-Theunissen, R.P.M. The importance of folate, zinc and antioxidants in the pathogenesis and prevention of subfertility. Hum. Reprod. Update 2007, 13, 163–174. [Google Scholar] [CrossRef]
- Iacono, F.; Prezioso, D.; Ruffo, A.; Di Lauro, G.; Romis, L.; Illiano, E. Analyzing the efficacy of a new natural compound made of the alga Ecklonia bicyclis, Tribulus terrestris and BIOVIS® in order to improve male sexual function. J. Men’s Health 2011, 8, 282–287. [Google Scholar]
- Ghanim, H.; Sia, C.L.; Korzeniewski, K.; Lohano, T.; Abuaysheh, S.; Marumganti, A.; Chaudhuri, A.; Dandona, P. A resveratrol and polyphenol preparation suppresses oxidative and inflammatory stress response to a high-fat, high-carbohydrate meal. J. Clin. Endocrinol. Metab. 2011, 96, 1409–1414. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Sekhon, L.H. The role of antioxidant therapy in the treatment of male infertility. Hum. Fertil. 2010, 13, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Barati, E.; Nikzad, H.; Karimian, M. Oxidative stress and male infertility: Current knowledge of pathophysiology and role of antioxidant therapy in disease management. Cell. Mol. Life Sci. 2019, 77, 93–113. [Google Scholar] [CrossRef] [PubMed]
- Lanzafame, F.M.; La Vignera, S.; Vicari, E.; Calogero, A.E. Oxidative stress and medical antioxidant treatment in male infertility. Reprod. Biomed. Online 2009, 19, 638–659. [Google Scholar] [CrossRef] [PubMed]
- Amaral, A.; Lourenço, B.; Marques, M.; Ramalho-Santos, J. Mitochondria functionality and sperm quality. Reproduction 2013, 146, R163–R174. [Google Scholar] [CrossRef] [PubMed]
- Rajender, S.; Rahul, P.; Mahdi, A.A. Mitochondria, spermatogenesis and male infertility. Mitochondrion 2010, 10, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Price, N.L.; Gomes, A.P.; Ling, A.J.Y.; Duarte, F.V.; Martin-Montalvo, A.; North, B.J.; Agarwal, B.; Ye, L.; Ramadori, G.; Teodoro, J.S.; et al. SIRT1 Is Required for AMPK Activation and the Beneficial Effects of Resveratrol on Mitochondrial Function. Cell Metab. 2012, 15, 675–690. [Google Scholar] [CrossRef]
- Juan, E.M.; González-Pons, E.; Munuera, T.; Ballester, J.; Rodríguez-Gil, J.E.; Planas, J.M. Trans-Resveratrol, a natural antioxidant from grapes, increases sperm output in healthy rats. J. Nutr. 2005, 135, 757–760. [Google Scholar] [CrossRef]
- Shin, S.; Hee Jeon, J.; Park, D.; Jang, M.-J.; Choi, J.H.; Choi, B.-H.; Joo, S.S.; Nahm, S.-S.; Kim, J.-C.; Kim, Y.-B. Trans-Resveratrol relaxes the corpus cavernosum ex vivo and enhances testosterone levels and sperm quality in vivo. Arch. Pharm. Res. 2008, 31, 83–87. [Google Scholar] [CrossRef]
- Kasai, T.; Ogawa, K.; Mizuno, K.; Nagai, S.; Uchida, Y.; Ohta, S.; Fujie, M.; Suzuki, K.; Hirata, S.; Hoshi, K. Relationship between sperm mitochondrial membrane potential, sperm motility, and fertility potential. Asian J. Androl. 2002, 4, 97–103. [Google Scholar]
- Zhao, C.; Huo, R.; Wang, F.; Lin, M.; Zhou, Z.; Sha, J. Identification of several proteins involved in regulation of sperm motility by proteomic analysis. Fertil. Steril. 2007, 87, 436–438. [Google Scholar] [CrossRef] [PubMed]
- Bahmanzadeh, M.; Goodarzi, M.T.; Farimani, A.R.; Fathi, N.; Alizadeh, Z. Resveratrol supplementation improves DNA integrity and sperm parameters in streptozotocin–nicotinamide-induced type 2 diabetic rats. Andrologia 2019, 51, e13313. [Google Scholar] [CrossRef]
- Alamo, A.; Condorelli, R.A.; Mongioì, L.M.; Cannarella, R.; Giacone, F.; Calabrese, V.; La Vignera, S.; Calogero, A.E. Environment and Male Fertility: Effects of Benzo-α-Pyrene and Resveratrol on Human Sperm Function In Vitro. J. Clin. Med. 2019, 8, 561. [Google Scholar] [CrossRef] [PubMed]
- Takeo, S.; Sato, D.; Kimura, K.; Monji, Y.; Kuwayama, T.; Kawahara-Miki, R.; Iwata, H. Resveratrol Improves the Mitochondrial Function and Fertilization Outcome of Bovine Oocytes. J. Reprod. Dev. 2014, 60, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Barratt, C.L.; Björndahl, L.; De Jonge, C.J.; Lamb, D.J.; Martini, F.O.; McLachlan, R.; Oates, R.D.; Van Der Poel, S.; John, B.S.; Sigman, M.; et al. The diagnosis of male infertility: An analysis of the evidence to support the development of global WHO guidance—Challenges and future research opportunities. Hum. Reprod. Update 2017, 23, 660–680. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, P.S.; Gupta, A.S. Causes and Prevalence of Factors Causing Infertility in a Public Health Facility. J. Hum. Reprod. Sci. 2019, 12, 287–293. [Google Scholar] [PubMed]
- Durairajanayagam, D. Lifestyle causes of male infertility. Arab. J. Urol. 2018, 16, 10–20. [Google Scholar] [CrossRef]
- Banyra, O.; Nikitin, O.; Ventskivska, I. Acute epididymo-orchitis: Relevance of local classification and partner’s follow-up. Cent. Eur. J. Urol. 2019, 72, 324–329. [Google Scholar]
- La Vignera, S.; Vicari, E.; Condorelli, R.A.; D’Agata, R.; Calogero, A.E. Male accessory gland infection and sperm parameters (review). Int. J. Androl. 2011, 34, e330–e347. [Google Scholar] [CrossRef]
- Everaert, K.; Mahmoud, A.; Depuydt, C.; Maeyaert, M.; Comhaire, F. Chronic prostatitis and male accessory gland infection—Is there an impact on male infertility (diagnosis and therapy)? Andrologia 2003, 35, 325–330. [Google Scholar] [CrossRef]
- Spogli, R.; Bastianini, M.; Ragonese, F.; Ianninitti, R.G.; Monarca, L.; Bastioli, F.; Nakashidze, I.; Brecchia, G.; Menchetti, L.; Codini, M.; et al. Solid Dispersion of Resveratrol Supported on Magnesium DiHydroxide (Resv@MDH) Microparticles Improves Oral Bioavailability. Nutrients 2018, 10, 1925. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.; Ping, P.; Ma, Y.; Wu, Z.; Chen, X. Correlation between methylenetetrahydrofolate reductase gene polymorphism and oligoasthenospermia and the effects of folic acid supplementation on semen quality. Transl. Androl. Urol. 2019, 8, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Banihani, S.A.; Aljabali, S.M. Seminal plasma vitamin B 6 levels in men with asthenozoospermia and men with normal sperm motility, a measurement using liquid chromatography with tandem mass spectrometry. Andrologia 2020, 52, e13556. [Google Scholar] [CrossRef] [PubMed]
- Murphy, L.E.; Mills, J.L.; Molloy, A.M.; Qian, C.; Carter, T.C.; Strevens, H.; Wide-Swensson, D.; Giwercman, A.; Levine, R.J. Folate and vitamin B12 in idiopathic male infertility. Asian J. Androl. 2011, 13, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, I.M.; Costa, E.M.; Pariz, J.R.; Teixeira, T.A.; Drevet, J.R.; Gharagozloo, P.; Aitken, R.J.; Hallak, J. Serum vitamin D content is associated with semen parameters and serum testosterone levels in men. Asian J. Androl. 2020, 28. [Google Scholar] [CrossRef]
- Jueraitetibaike, K.; Ding, Z.; Wang, D.-D.; Peng, L.-P.; Jing, J.; Chen, L.; Ge, X.; Qiu, X.-H.; Yao, B. The effect of vitamin D on sperm motility and the underlying mechanism. Asian J. Androl. 2019, 21, 400–407. [Google Scholar]
- Rudnicka, A.; Adoamnei, E.; Noguera-Velasco, J.A.; Vioque, J.; Cañizares-Hernández, F.; Mendiola, J.; Jørgensen, N.; Chavarro, J.E.; Swan, S.H.; Torres-Cantero, A.M. Vitamin D status is not associated with reproductive parameters in young Spanish men. Andrologia 2020, 8, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Neto, F.T.L.; Bach, P.V.; Najari, B.B.; Lira, N.F.T.; Goldstein, M. Spermatogenesis in humans and its affecting factors. Semin. Cell Dev. Biol. 2016, 59, 10–26. [Google Scholar] [CrossRef]
- Grootegoed, J.A.; Jansen, R.; Van Der Molen, H.J. The role of glucose, pyruvate and lactate in ATP production by rat spermatocytes and spermatids. Biochim. Biophys. Acta Bioenerg. 1984, 767, 248–256. [Google Scholar] [CrossRef]
- Han, Y.; Luo, H.; Wang, H.; Cai, J.; Zhang, Y. SIRT1 induces resistance to apoptosis in human granulosa cells by activating the ERK pathway and inhibiting NF-κB signaling with anti-inflammatory functions. Apoptosis 2017, 22, 1260–1272. [Google Scholar] [CrossRef]
- Michan, S.; Sinclair, D. Sirtuins in mammals: Insights into their biological function. Biochem. J. 2007, 404, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Rato, L.; Alves, G.M.; Silva, M.B.; Sousa, M.; Oliveira, P.F. Sirtuins: Novel Players in Male Reproductive Health. Curr. Med. Chem. 2016, 23, 1084–1099. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Pesini, E.; Diez, C.; Lapeña, A.C.; Pérez-Martos, A.; Montoya, J.; Alvarez, E.; Arenas, J.; López-Pérez, M.J. Correlation of sperm motility with mitochondrial enzymatic activities. Clin. Chem. 1998, 44, 1616–1620. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Heredia, J.; de Mateo, S.; Vidal-Taboada, J.M.; Ballescà, J.L.; Oliva, R. Identification of proteomic differences in asthenozoospermic sperm samples. Hum. Reprod. 2008, 23, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Pesini, E.; Lapeña, A.C.; Díez, C.; Álvarez, E.; Enríquez, J.A.; López-Pérez, M.J. Seminal quality correlates with mitochondrial functionality. Clin. Chim. Acta 2000, 300, 97–105. [Google Scholar] [CrossRef]
- Mundy, A.J.; Ryder, T.A.; Edmonds, D.K. Asthenozoospermia and the human sperm mid-piece. Hum. Reprod. 1995, 10, 10116–10119. [Google Scholar] [CrossRef] [PubMed]
- Pelliccione, F.; Micillo, A.; Cordeschi, G.; D’Angeli, A.; Necozione, S.; Gandini, L.; Lenzi, A.; Francavilla, F.; Francavilla, F. Altered ultrastructure of mitochondrial membranes is strongly associated with unexplained asthenozoospermia. Fertil. Steril. 2011, 95, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Nakada, K.; Sato, A.; Yoshida, K.; Morita, T.; Tanaka, H.; Inoue, S.-I.; Yonekawa, H.; Hayashi, J.-I. Mitochondria-related male infertility. Proc. Natl. Acad. Sci. USA 2006, 103, 15148–15153. [Google Scholar] [CrossRef]
- Kao, S.H.; Chao, H.T.; Wei, Y.H. Multiple deletions of mitochondrial DNA are associated with the decline of motility and fertility of human spermatozoa. Mol. Hum. Reprod. 1998, 4, 657–666. [Google Scholar] [CrossRef]
- Tremellen, K. Oxidative stress and male infertility—A clinical perspective. Hum. Reprod. Update 2008, 14, 243–258. [Google Scholar] [CrossRef]


{kind=link}
| Patients | 20 |
|---|---|
| Age (mean ± SD) | 30.9 ± 3.28 |
| BMI (mean ± SD) | 27.9 ± 1.4 |
| Married n (%) | 10 (50) |
| Erectile Dysfunction n (%) | 0 (0) |
| Male hyopogonadism n (%) | 0 (0) |
| Oligozoospermia n (%) | 0 (0) |
| Asthenozoospermia n (%) | 6 (30) |
| Teratozoospermia n (%) | 7 (35) |
| Oligoasthenozoospermia n (%) | 7 (95) |
| Oligoteratozoospermia n (%) | 0 (0) |
| Asthenoteratozoospermia n (%) | 0 (0) |
| Oligosthenoteratozoospermia n (%) | 0 (0) |
| Normal scrotal ultrasound | 20 (100) |
| Normal prostatic transrectal ultrasound | 20 (100) |
| FSH mlU/mL (mean ± SD) | 4.60 ± 1.3 |
| LH mlU/mL (mean ± SD) | 3.87 ± 1.8 |
| Total Testosterone nmol/L (mean ± SD) | 14.89 ± 0.3 |
| Estradiol pg/mL (mean ± SD) | 25.2 ± 2.1 |
| Prolactin ng/mL (mean ± SD) | 11.17 ± 1.9 |
| 25-OH-Vitamin D3 ng/mL (mean ± SD) | 55.8 ± 2.8 |
| Parameters | Baseline | 1 Month | 3 Months | 6 Months | p-Value |
|---|---|---|---|---|---|
| Normal Viscosity n (%) | 20 (100) | 20 (100) | 20(100) | 20 (100) | nd |
| Complete Fludification n (%) | 11(100) | 11(100) | 11(100) | 11(100) | nd |
| PH (mean ± SD) | 8.1 ± 0.1 | 8.0 ± 0.3 | 8.0 ± 0.2 | 8.0 ± 0.3 | 0.219 |
| Semen volume (mL, mean ± SD) | 3.6 ± 0.7 | 3.61 ± 0.6 | 3.61 ± 0.5 | 3.7 ± 0.5 | 0.525 |
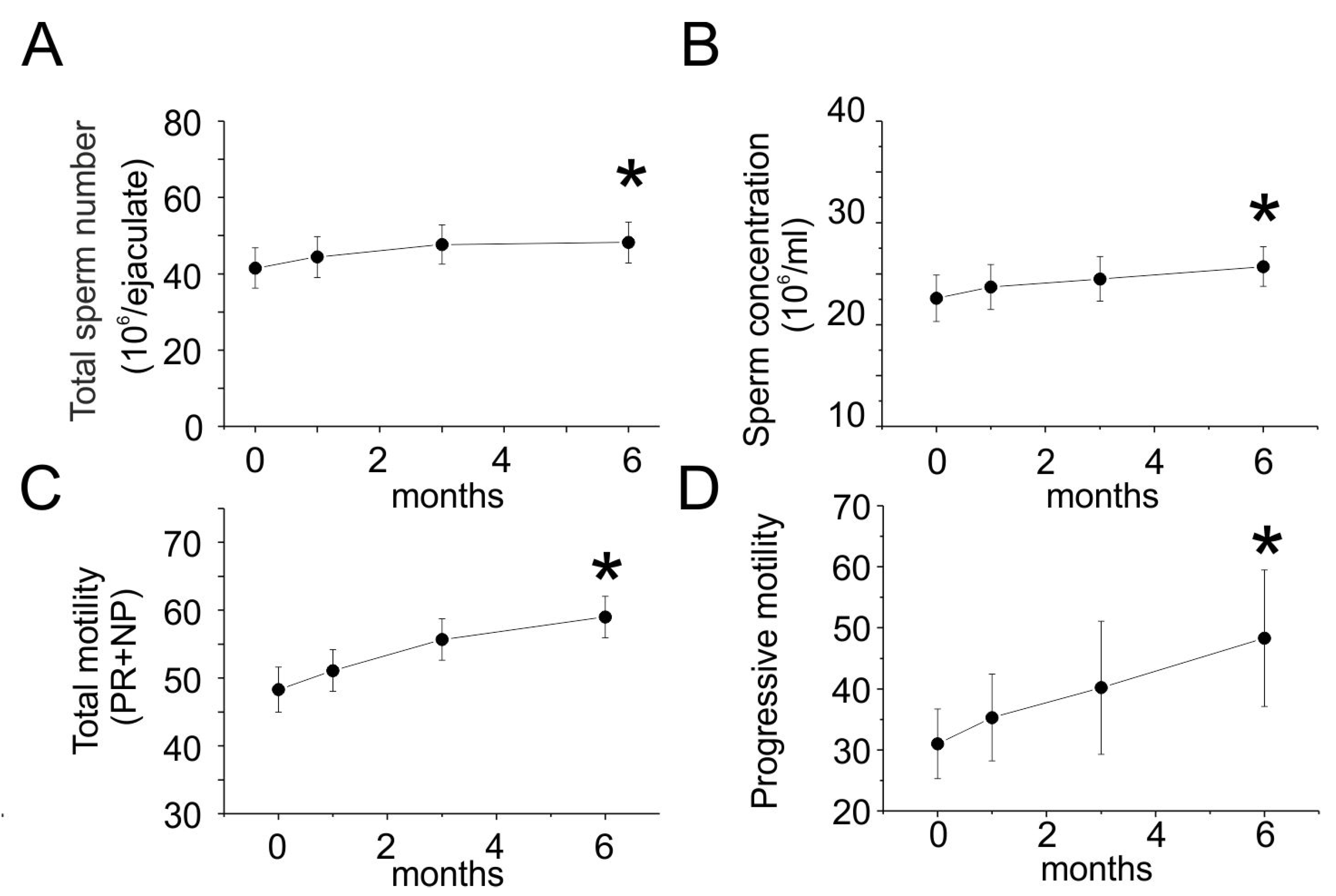
| Total sperm number (106/ejaculate, mean ± SD) | 41.5 ± 22.1 | 44.4 ± 22.4 | 47.7 ± 21.4 | 48.2 ± 22.4 | 0.002 * |
| Sperm concentration (106/mL, mean ± SD) | 22.6 ± 9.5 | 23.7 ±9.2 | 24.5 ± 9.1 | 25.7 ± 8.1 | 0.0001 * |
| Total motility (PR + NP, % mean ± SD) | 48.3 ± 13.8 | 51.1 ± 12.8 | 55.7 ± 12.7 | 59.0 ± 12.8 | 0.0001 * |
| Progressive motility (PR > 32% mean ± SD) | 31 ± 5.7 | 35.3 ± 7.1 | 40.2 ± 10.9 | 48.3 ± 11.2 | 0.0001 * |
| Sperm morphology (normal forms%) | 14 (66.7) | 14 (66.7) | 14 (66.7) | 14 (66.7) | nd |
| Parameters | Baseline | 1 Month | 3 Months | 6 Months | p Value |
|---|---|---|---|---|---|
| FSH mlU/mL (mean ± SD) | 4.60 ± 1.3 | 4.62 ± 1.2 | 4.61 ± 1.5 | 4.61 ± 1.7 | 0.9 |
| LH mlU/mL (mean ± SD) | 3.87 ± 1.8 | 3.85 ± 1.3 | 3.87 ± 1.4 | 3.88 ± 1.4 | 0.87 |
| Total Testosterone nmol/L (mean ± SD) | 14.89 ± 0.3 | 14.84 ± 0.7 | 14.82 ± 0.2 | 14.87 ± 0.2 | 0.9 |
| Estradiol pg/mL (mean ± SD) | 25.2 ± 2.1 | 25.8 ± 2.4 | 25.5 ± 2.3 | 25.6 ± 2.0 | 0.86 |
| Prolactin ng/mL (mean ± SD) | 11.17 ± 1.9 | 11.13 ± 1.5 | 11.15 ± 1.3 | 11.19 ± 1.2 | 0.9 |
| 25-OH-Vitamin D3 ng/mL (mean ± SD) | 55.8 ± 2.8 | 55.1 ± 2.2 | 55.7 ± 2.4 | 55.4 ± 2.1 | 0.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Illiano, E.; Trama, F.; Zucchi, A.; Iannitti, R.G.; Fioretti, B.; Costantini, E. Resveratrol-Based Multivitamin Supplement Increases Sperm Concentration and Motility in Idiopathic Male Infertility: A Pilot Clinical Study. J. Clin. Med. 2020, 9, 4017. https://doi.org/10.3390/jcm9124017
Illiano E, Trama F, Zucchi A, Iannitti RG, Fioretti B, Costantini E. Resveratrol-Based Multivitamin Supplement Increases Sperm Concentration and Motility in Idiopathic Male Infertility: A Pilot Clinical Study. Journal of Clinical Medicine. 2020; 9(12):4017. https://doi.org/10.3390/jcm9124017
Chicago/Turabian StyleIlliano, Ester, Francesco Trama, Alessandro Zucchi, Rossana Giulietta Iannitti, Bernard Fioretti, and Elisabetta Costantini. 2020. "Resveratrol-Based Multivitamin Supplement Increases Sperm Concentration and Motility in Idiopathic Male Infertility: A Pilot Clinical Study" Journal of Clinical Medicine 9, no. 12: 4017. https://doi.org/10.3390/jcm9124017
APA StyleIlliano, E., Trama, F., Zucchi, A., Iannitti, R. G., Fioretti, B., & Costantini, E. (2020). Resveratrol-Based Multivitamin Supplement Increases Sperm Concentration and Motility in Idiopathic Male Infertility: A Pilot Clinical Study. Journal of Clinical Medicine, 9(12), 4017. https://doi.org/10.3390/jcm9124017