Short-Term Effects of Different Types of Anti-Glaucoma Eyedrop on the Sclero-Conjunctival Vasculature Assessed Using Anterior Segment OCTA in Normal Human Eyes: A Pilot Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Protocol for Eye Drop Instillation
2.3. Anterior Segment Optical Coherence Tomography Angiography (AS-OCTA) Examination
2.4. OCTA Image Acquisition and Processing
2.5. Quantitative Measurements
2.6. Statistical Analysis
3. Results
3.1. Participants and Intraocular Pressure (IOP) Measurements
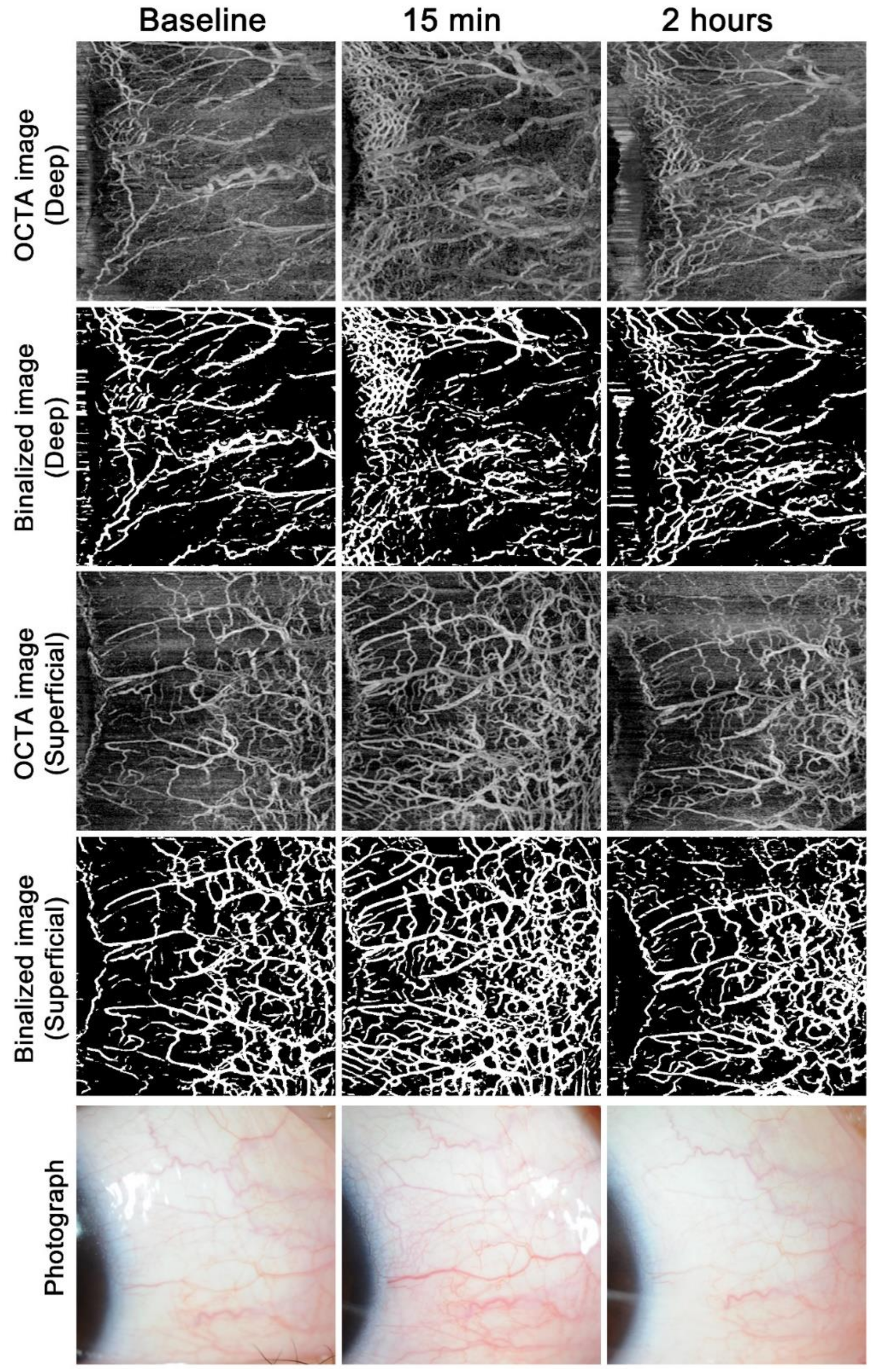
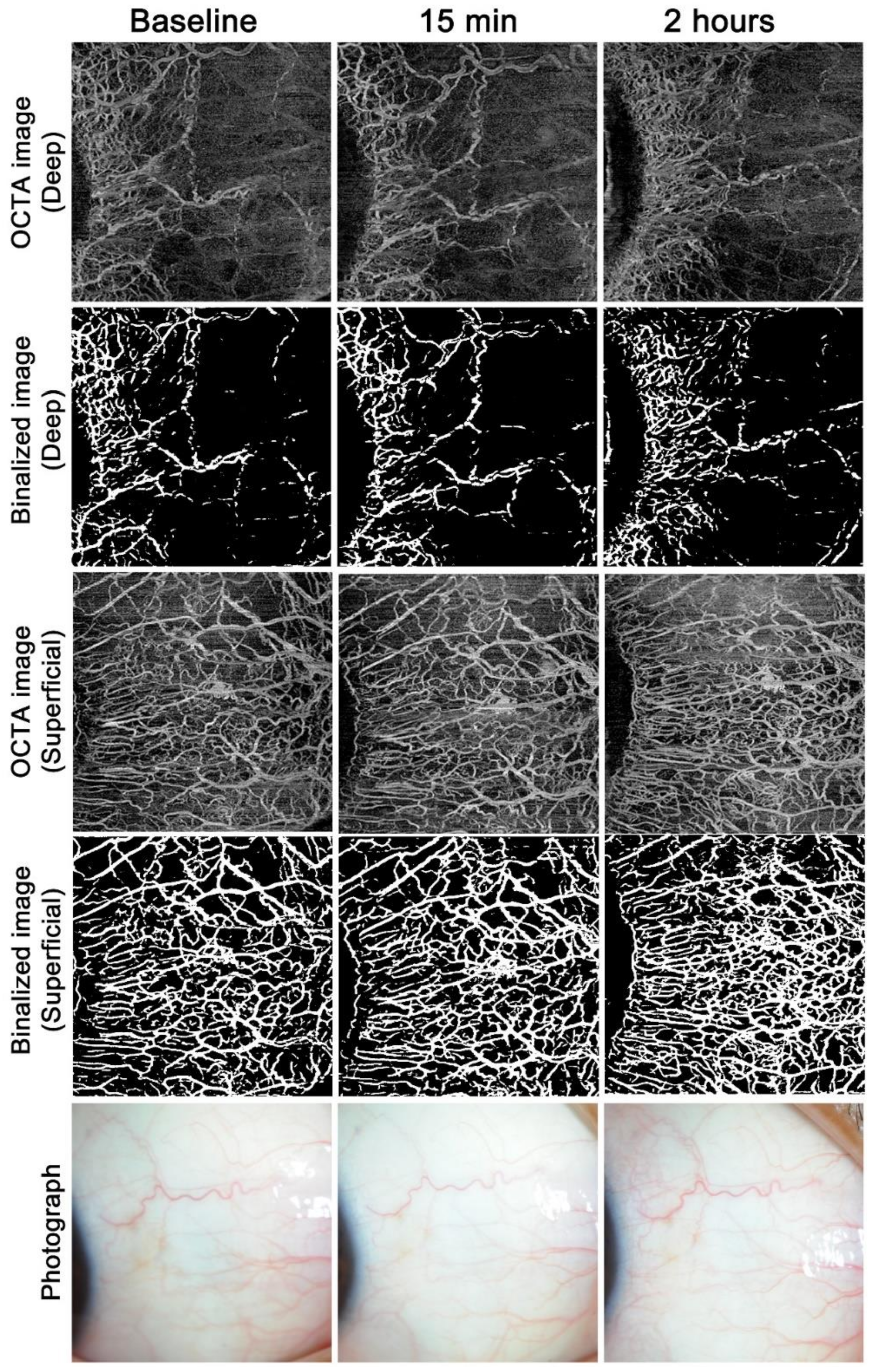
3.2. Time Course of Vasculature Findings in the Superficial and Deep Layers
3.3. Association between IOP Reduction and AS-OCTA Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Friedman, D.S.; Hahn, S.R.; Gelb, L.; Tan, J.; Shah, S.N.; Kim, E.E.; Zimmerman, T.J.; Quigley, H.A. Doctor-patient communication, health-related beliefs, and adherence in glaucoma results from the Glaucoma Adherence and Persistency Study. Ophthalmology 2008, 115, 1320–1327. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.C.; Kolker, A.E.; Stewart, J.A.; Leech, J.; Jackson, A.L. Conjunctival hyperemia in healthy subjects after short-term dosing with latanoprost, bimatoprost, and travoprost. Am. J. Ophthalmol. 2003, 135, 314–320. [Google Scholar] [CrossRef]
- Sakata, R.; Sakisaka, T.; Matsuo, H.; Miyata, K.; Aihara, M. Time Course of Prostaglandin Analog-related Conjunctival Hyperemia and the Effect of a Nonsteroidal Anti-inflammatory Ophthalmic Solution. J. Glaucoma 2016, 25, e204–e208. [Google Scholar] [CrossRef] [PubMed]
- Terao, E.; Nakakura, S.; Fujisawa, Y.; Fujio, Y.; Matsuya, K.; Kobayashi, Y.; Tabuchi, H.; Yoneda, T.; Fukushima, A.; Kiuchi, Y. Time Course of Conjunctival Hyperemia Induced by a Rho-kinase Inhibitor Anti-glaucoma Eye Drop: Ripasudil 0.4. Curr. Eye Res. 2017, 42, 738–742. [Google Scholar] [CrossRef]
- Terao, E.; Nakakura, S.; Fujisawa, Y.; Nagata, Y.; Ueda, K.; Kobayashi, Y.; Oogi, S.; Dote, S.; Shiraishi, M.; Tabuchi, H.; et al. Time course of conjunctival hyperemia induced by omidenepag isopropyl ophthalmic solution 0.002%: A pilot, comparative study versus ripasudil 0.4. BMJ Open Ophthalmol. 2020, 5, e000538. [Google Scholar] [CrossRef]
- Carreon, T.; van der Merwe, E.; Fellman, R.L.; Johnstone, M.; Bhattacharya, S.K. Aqueous outflow—A continuum from trabecular meshwork to episcleral veins. Prog. Retin. Eye Res. 2017, 57, 108–133. [Google Scholar] [CrossRef]
- Honjo, M.; Tanihara, H.; Inatani, M.; Kido, N.; Sawamura, T.; Yue, B.Y.; Narumiya, S.; Honda, Y. Effects of rho-associated protein kinase inhibitor Y-27632 on intraocular pressure and outflow facility. Investig. Ophthalmol. Vis. Sci. 2001, 42, 137–144. [Google Scholar]
- Tanihara, H.; Inatani, M.; Honjo, M.; Tokushige, H.; Azuma, J.; Araie, M. Intraocular pressure-lowering effects and safety of topical administration of a selective ROCK inhibitor, SNJ-1656, in healthy volunteers. Arch. Ophthalmol. 2008, 126, 309–315. [Google Scholar] [CrossRef]
- Prum, B.E., Jr.; Rosenberg, L.F.; Gedde, S.J.; Mansberger, S.L.; Stein, J.D.; Morot, S.E.; Herndon, L.W., Jr.; Lim, M.C.; Williams, R.D. Primary Open-Angle Glaucoma Preferred Practice Pattern((R)) Guidelines. Ophthalmology 2016, 123, 41–111. [Google Scholar] [CrossRef]
- Yanagi, M.; Kiuchi, Y.; Yuasa, Y.; Yoneda, T.; Sumi, T.; Hoshikawa, Y.; Kobayashi, M.; Fukushima, A. Association between glaucoma eye drops and hyperemia. Jpn. J. Ophthalmol. 2016, 60, 72–77. [Google Scholar] [CrossRef]
- Li, P.; An, L.; Reif, R.; Shen, T.T.; Johnstone, M.; Wang, R.K. In vivo microstructural and microvascular imaging of the human corneo-scleral limbus using optical coherence tomography. Biomed. Opt. Express 2011, 2, 3109–3118. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Akagi, T.; Uji, A.; Huang, A.S.; Weinreb, R.N.; Yamada, T.; Miyata, M.; Kameda, T.; Ikeda, H.O.; Tsujikawa, A. Conjunctival and Intrascleral Vasculatures Assessed Using Anterior Segment Optical Coherence Tomography Angiography in Normal Eyes. Am. J. Ophthalmol. 2018, 196, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Akagi, T.; Uji, A.; Okamoto, Y.; Suda, K.; Kameda, T.; Nakanishi, H.; Ikeda, H.O.; Miyake, M.; Nakano, E.; Motozawa, N.; et al. Anterior Segment Optical Coherence Tomography Angiography Imaging of Conjunctiva and Intrasclera in Treated Primary Open-Angle Glaucoma. Am. J. Ophthalmol. 2019, 208, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Guler, M.; Bilak, S.; Bilgin, B.; Simsek, A.; Capkin, M.; Reyhan, A.H. Comparison of Intraocular Pressure Measurements Obtained by Icare PRO Rebound Tonometer, Tomey FT-1000 Noncontact Tonometer, and Goldmann Applanation Tonometer in Healthy Subjects. J. Glaucoma 2015, 24, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Akagi, T.; Okamoto, Y.; Tsujikawa, A. Anterior Segment OCT Angiography Images of Avascular Bleb after Trabeculectomy. Ophthalmol. Glaucoma 2019, 2, 102. [Google Scholar] [CrossRef] [PubMed]
- Akagi, T.; Fujimoto, M.; Ikeda, H.O. Anterior Segment Optical Coherence Tomography Angiography of Iris Neovascularization After Intravitreal Ranibizumab and Panretinal Photocoagulation. JAMA Ophthalmol. 2020, 138, e190318. [Google Scholar] [CrossRef]
- Zhang, A.; Zhang, Q.; Wang, R.K. Minimizing projection artifacts for accurate presentation of choroidal neovascularization in OCT micro-angiography. Biomed. Opt. Express 2015, 6, 4130–4143. [Google Scholar] [CrossRef]
- Chu, Z.; Lin, J.; Gao, C.; Xin, C.; Zhang, Q.; Chen, C.-L.; Roisman, L.; Gregori, G.; Rosenfeld, P.J.; Wang, R.K. Quantitative assessment of the retinal microvasculature using optical coherence tomography angiography. J. Biomed. Opt. 2016, 21, 66008. [Google Scholar] [CrossRef]
- Trainable Weka Segmentation. Available online: https://imagej.net/Trainable_Weka_Segmentation (accessed on 1 July 2020).
- ImageJ. Available online: http://rsb.info.nih.gov/ij/index.html (accessed on 1 July 2020).
- Arganda-Carreras, I.; Kaynig, V.; Rueden, C.; Eliceiri, K.W.; Schindelin, J.E.; Cardona, A.; Seung, H.S. Trainable Weka Segmentation: A machine learning tool for microscopy pixel classification. Bioinformatics 2017, 33, 2424–2426. [Google Scholar] [CrossRef]
- Ren, R.; Li, G.; Le, T.D.; Kopczynski, C.; Stamer, W.D.; Gong, H. Netarsudil Increases Outflow Facility in Human Eyes Through Multiple Mechanisms. Investig. Ophthalmol. Vis. Sci. 2016, 57, 6197–6209. [Google Scholar] [CrossRef]
- Selbach, J.M.; Rohen, J.W.; Steuhl, K.P.; Lutjen-Drecoll, E. Angioarchitecture and innervation of the primate anterior episclera. Curr. Eye Res. 2005, 30, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Funk, R.H.; Gehr, J.; Rohen, J.W. Short-term hemodynamic changes in episcleral arteriovenous anastomoses correlate with venous pressure and IOP changes in the albino rabbit. Curr. Eye Res. 1996, 15, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Robinson, M.R.; Weinreb, R.N. Episcleral Venous Pressure and the Ocular Hypotensive Effects of Topical and Intracameral Prostaglandin Analogs. J. Glaucoma 2019, 28, 846–857. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.; Wei, E.; Wang, X.; Zhang, X.; Morrison, J.C.; Parikh, M.; Lombardi, L.H.; Gattey, D.M.; Armour, R.L.; Edmunds, B.; et al. Optical coherence tomography angiography of optic disc perfusion in glaucoma. Ophthalmology 2014, 121, 1322–1332. [Google Scholar] [CrossRef]
- Chen, J.; Dinh, T.; Woodward, D.F.; Holland, J.M.; Yuan, Y.-D.; Lin, T.-H.; Wheeler, L.A. Bimatoprost: Mechanism of ocular surface hyperemia associated with topical therapy. Cardiovasc. Drug Rev. 2005, 23, 231–246. [Google Scholar] [CrossRef]
- Alm, A.; Nilsson, S.F. Uveoscleral outflow—A review. Exp. Eye Res. 2009, 88, 760–768. [Google Scholar] [CrossRef]
- Winkler, N.S.; Fautsch, M.P. Effects of prostaglandin analogues on aqueous humor outflow pathways. J. Ocul. Pharmacol. Ther. 2014, 30, 102–109. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Ripasudil Group | Bimatoprost Group | |||
|---|---|---|---|---|
| Age, mean (SD), y | 30.1 (7.8) | 27.6 (5.4) | ||
| Sex, n, male/female | 5/5 | 4/6 | ||
| Right eye | Left eye | Right eye | Left eye | |
| Axial length, mean (SD), mm | 24.81 (1.24) | 24.87 (1.23) | 24.77 (1.04) | 24.76 (0.92) |
| Central corneal thickness, mean (SD), μm | 550.2 (32.3) | 551.2 (29.5) | 547.4 (31.2) | 546.6 (31.0) |
| Baseline IOP, mean (SD), mm Hg | 13.9 (2.9) | 14.0 (2.5) | 12.8 (2.2) | 13.0 (2.4) |
| IOP 15 min, mean (SD), mm Hg | 12.3 (2.6) | 13.6 (2.3) | 11.9 (1.7) | 12.6 (1.2) |
| IOP 2 h, mean (SD), mm Hg | 11.3 (3.1) | 13.2 (2.6) | 11.7 (0.9) | 12.6 (1.5) |
| Eye Drop and Side | Median (25th Percentile, 75th Percentile) | p Value ab | p Value ac | ||
|---|---|---|---|---|---|
| At Baseline | At 15 min | At 2 h | |||
| Ripasudil group Right eye | |||||
| Deep VD, % | 13.11% (11.52%, 15.92%) | 19.91% (14.82%, 24.07%) | 14.80% (12.03%, 19.98%) | <0.001 | 0.009 |
| Superficial VD, % | 28.46% (25.08%, 35.43%) | 37.29% (33.2%, 40.90%) | 31.64% (27.42%, 36.75%) | <0.001 | 0.015 |
| Ripasudil group Left eye | |||||
| Deep VD, % | 14.28% (11.83%, 16.45%) | 13.49% (10.61%, 18.16%) | 13.52% (10.41%, 16.94%) | 0.33 | 0.85 |
| Superficial VD, % | 29.45% (25.04%, 33.64%) | 27.27% (23.16%, 33.69%) | 29.56% (26.78%, 33.90%) | 0.093 | 0.91 |
| Bimatoprost group Right eye | |||||
| Deep VD, % | 24.21% (16.96%, 27.43%) | 19.34% (15.19%, 25.06%) | 22.07% (17.50%, 26.16%) | 0.037 | 0.48 |
| Superficial VD, % | 42.64% (39.49%, 46.84%) | 39.53% (35.23%, 47.19%) | 48.19% (45.02%, 53.95%) | 0.010 | 0.011 |
| Bimatoprost group Left eye | |||||
| Deep VD, % | 20.55% (17.01%, 25.87%) | 23.41% (16.24%, 31.80%) | 22.40% (18.68%, 30.80%) | 0.18 | 0.10 |
| Superficial VD, % | 42.73% (38.25%, 46.25%) | 42.28% (37.09%, 48.51%) | 46.46% (39.54%, 49.09%) | 0.85 | 0.067 |
| Ripasudil | Percent IOP Change at 15 min | Percent IOP Change at 2 h | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariable Analysis a | Univariate Analysis | Multivariable Analysis a | |||||||||
| B | β | p | B | β | p | B | β | p | B | β | p | |
| Use of eye drop | −8.677 | −0.657 | <0.001 | −8.191 | −0.620 | <0.001 | −13.034 | −0.521 | 0.001 | −11.822 | −0.473 | 0.001 |
| Baseline IOP | −0.419 | −0.163 | 0.32 | - | - | - | −0.018 | −0.004 | 0.98 | - | - | - |
| Baseline deep VD | 0.366 | 0.34 | 0.032 | 0.267 | 0.248 | 0.044 | 0.808 | 0.396 | 0.011 | 0.665 | 0.326 | 0.018 |
| Baseline superficial VD | 0.064 | 0.077 | 0.64 | - | - | - | 0.486 | 0.308 | 0.053 | 0.72 | ||
| Change in deep VD at 15 min | −0.031 | −0.36 | 0.023 | 0.70 | −0.025 | −0.155 | 0.34 | - | - | - | ||
| Change in deep VD at 2 h | −0.014 | −0.086 | 0.60 | - | - | - | 0.033 | 0.106 | 0.51 | - | - | - |
| Change in superficial VD at 15 min | −0.094 | −0.468 | 0.002 | 0.61 | −0.151 | −0.398 | 0.011 | 0.61 | ||||
| Change in superficial VD at 2 h | −0.053 | −0.236 | 0.14 | - | - | - | −0.109 | −0.254 | 0.11 | - | - | - |
| Bimatoprost | Percent IOP Change at 15 min | Percent IOP Change at 2 h | ||||||||||
| Univariate Analysis | Multivariable Analysis a | Univariate Analysis | Multivariable Analysis a | |||||||||
| B | β | p | B | β | p | B | β | p | B | β | p | |
| Use of eye drop | −4.274 | −0.092 | 0.57 | 0.070 | −6.715 | −0.12 | 0.46 | −9.587 | −0.171 | 0.004 | ||
| Baseline IOP | −9.363 | −0.878 | <0.001 | −9.363 | −0.878 | <0.001 | −11.844 | −0.927 | <0.001 | −11.964 | −0.936 | <0.001 |
| Baseline deep VD | −1.03 | −0.304 | 0.056 | 0.74 | −1.416 | −0.349 | 0.027 | 0.89 | ||||
| Baseline superficial VD | 0.167 | 0.054 | 0.74 | - | - | - | 0.628 | 0.170 | 0.29 | - | - | - |
| Change in deep VD at 15 min | 0.014 | 0.024 | 0.89 | - | - | - | −0.013 | −0.019 | 0.91 | - | - | - |
| Change in deep VD at 2 h | 0.063 | 0.086 | 0.60 | - | - | - | 0.054 | 0.062 | 0.70 | - | - | - |
| Change in superficial VD at 15 min | 0.265 | 0.194 | 0.23 | - | - | - | 0.283 | 0.173 | 0.29 | - | - | - |
| Change in superficial VD at 2 h | −0.185 | −0.110 | 0.50 | - | - | - | −0.187 | −0.093 | 0.57 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akagi, T.; Okamoto, Y.; Kameda, T.; Suda, K.; Nakanishi, H.; Miyake, M.; Ikeda, H.O.; Yamada, T.; Kadomoto, S.; Uji, A.; et al. Short-Term Effects of Different Types of Anti-Glaucoma Eyedrop on the Sclero-Conjunctival Vasculature Assessed Using Anterior Segment OCTA in Normal Human Eyes: A Pilot Study. J. Clin. Med. 2020, 9, 4016. https://doi.org/10.3390/jcm9124016
Akagi T, Okamoto Y, Kameda T, Suda K, Nakanishi H, Miyake M, Ikeda HO, Yamada T, Kadomoto S, Uji A, et al. Short-Term Effects of Different Types of Anti-Glaucoma Eyedrop on the Sclero-Conjunctival Vasculature Assessed Using Anterior Segment OCTA in Normal Human Eyes: A Pilot Study. Journal of Clinical Medicine. 2020; 9(12):4016. https://doi.org/10.3390/jcm9124016
Chicago/Turabian StyleAkagi, Tadamichi, Yoko Okamoto, Takanori Kameda, Kenji Suda, Hideo Nakanishi, Masahiro Miyake, Hanako Ohashi Ikeda, Tatsuya Yamada, Shin Kadomoto, Akihito Uji, and et al. 2020. "Short-Term Effects of Different Types of Anti-Glaucoma Eyedrop on the Sclero-Conjunctival Vasculature Assessed Using Anterior Segment OCTA in Normal Human Eyes: A Pilot Study" Journal of Clinical Medicine 9, no. 12: 4016. https://doi.org/10.3390/jcm9124016
APA StyleAkagi, T., Okamoto, Y., Kameda, T., Suda, K., Nakanishi, H., Miyake, M., Ikeda, H. O., Yamada, T., Kadomoto, S., Uji, A., & Tsujikawa, A. (2020). Short-Term Effects of Different Types of Anti-Glaucoma Eyedrop on the Sclero-Conjunctival Vasculature Assessed Using Anterior Segment OCTA in Normal Human Eyes: A Pilot Study. Journal of Clinical Medicine, 9(12), 4016. https://doi.org/10.3390/jcm9124016