Incidence and Risk Factors of Alcohol Relapse after Liver Transplantation: Analysis of Pre-Transplant Abstinence and Psychosocial Features

 , , ,
, , ,
Abstract
1. Introduction
2. Study Design
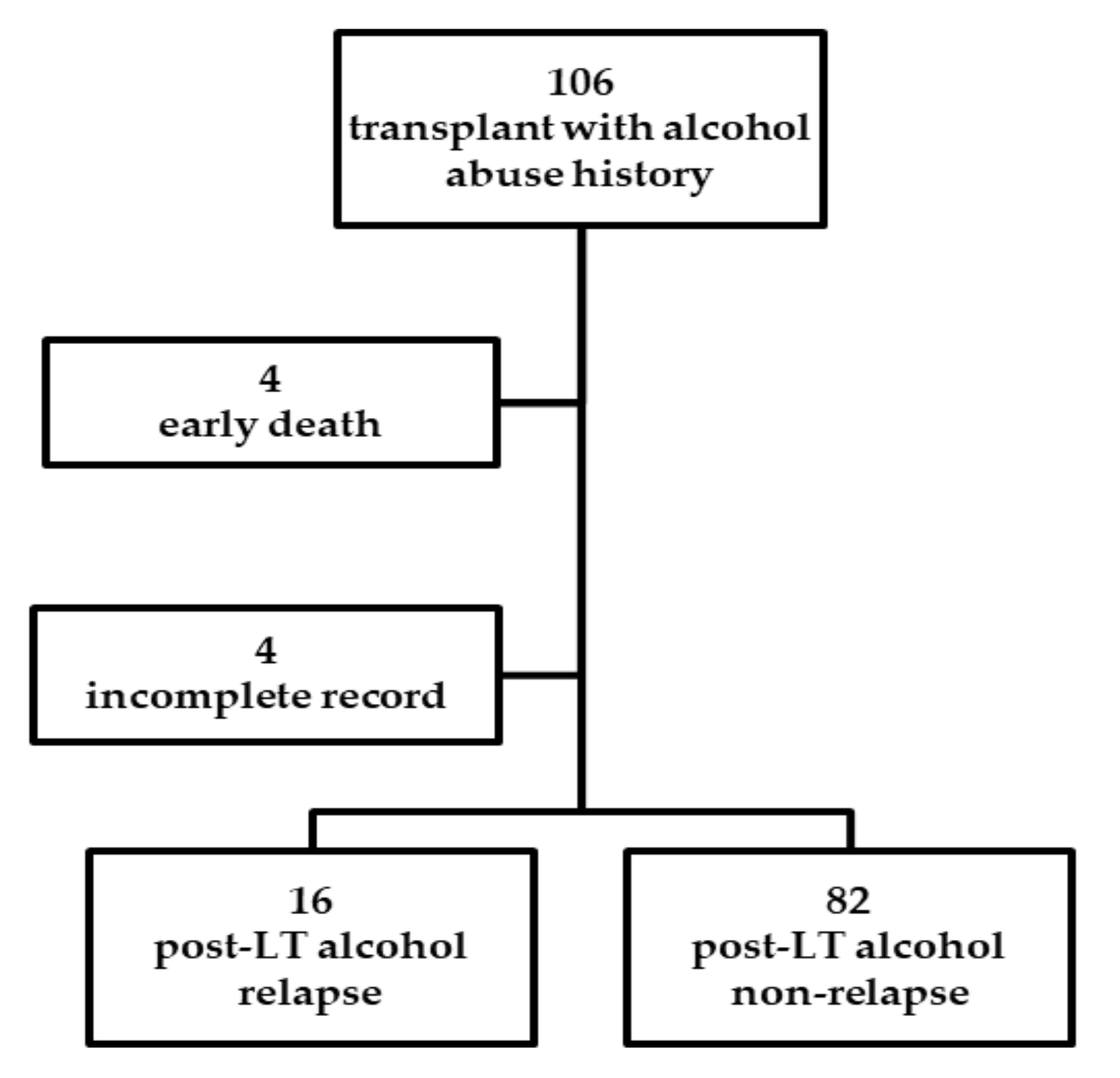
2.1. Study Participants
2.2. Statistics
3. Results
3.1. Demographic and Clinical Characteristics in LT Recipients
3.2. Predictors of Alcohol Relapse
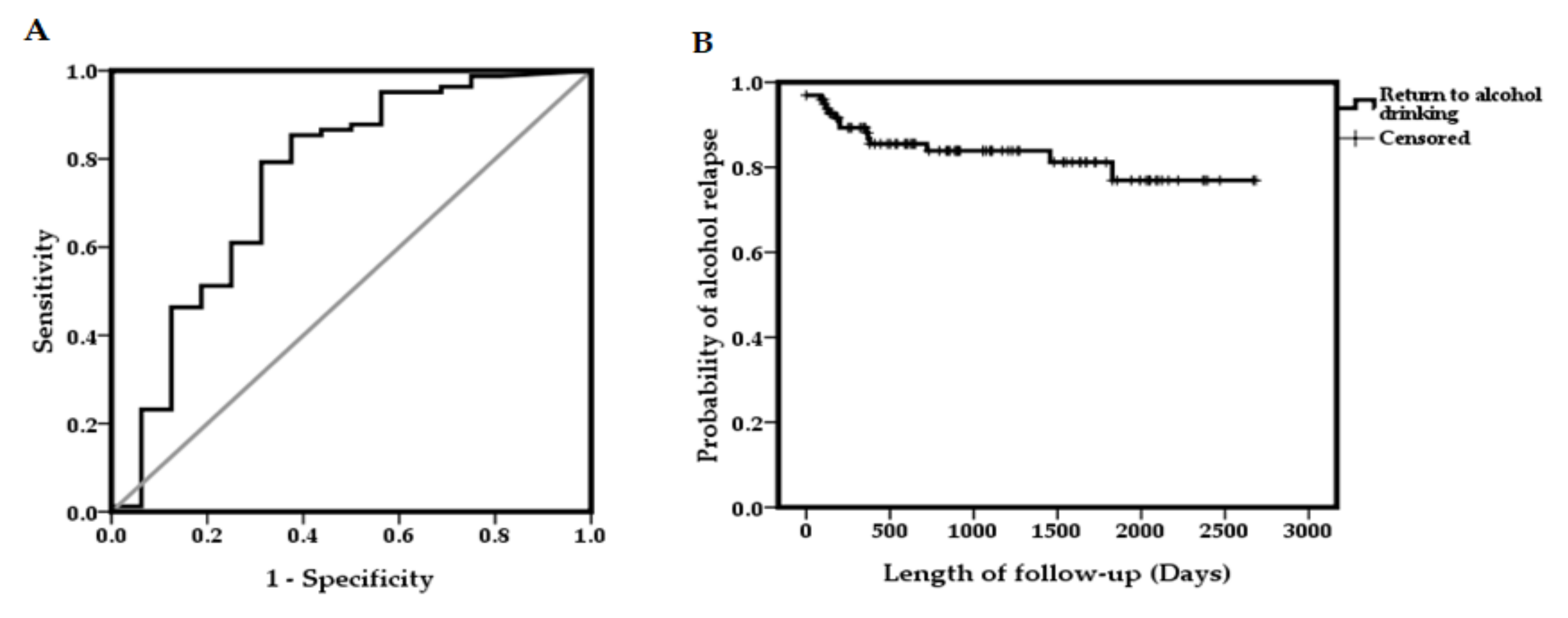
3.3. ROC Curve of Alcohol Abstinence Durations for Alcohol Relapse
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The Organ Procurement and Transplantation Network/The Scientific Registry of Transplant Recipients (OPTN/SRTR). Annual Data Report. 2017. Available online: https://srtr.transplant.hrsa.gov/annual_reports/2017/Liver.aspx (accessed on 1 January 2020).
- Marroni, C.A.; Fleck, A.M., Jr.; Fernandes, S.A.; Galant, L.H.; Mucenic, M.; de Mattos Meine, M.H.; Mariante-Neto, G.; Brandao, A.B.M. Liver transplantation and alcoholic liver disease: History, controversies, and considerations. World J. Gastroenterol. 2018, 24, 2785–2805. [Google Scholar] [CrossRef] [PubMed]
- DiMartini, A.; Day, N.; Dew, M.A.; Javed, L.; Fitzgerald, M.G.; Jain, A.; Fung, J.J.; Fontes, P. Alcohol consumption patterns and predictors of use following liver transplantation for alcoholic liver disease. Liver Transpl. 2006, 12, 813–820. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of, L. EASL clinical practical guidelines: Management of alcoholic liver disease. J. Hepatol. 2012, 57, 399–420. [Google Scholar] [CrossRef] [PubMed]
- Deruytter, E.; Van Steenkiste, C.; Trepo, E.; Geerts, A.; Van Vlierberghe, H.; Berrevoet, F.; de Hemptinne, B.; Rogiers, X.; Troisi, R.; Colle, I. Liver transplantation for alcoholic liver disease: A retrospective analysis of recidivism, survival and risk factors predisposing to alcohol relapse. Acta Gastroenterol. Belg. 2013, 76, 282–290. [Google Scholar]
- Fleming, M.F.; Smith, M.J.; Oslakovic, E.; Lucey, M.R.; Vue, J.X.; Al-Saden, P.; Levitsky, J. Phosphatidylethanol Detects Moderate-to-Heavy Alcohol Use in Liver Transplant Recipients. Alcohol Clin. Exp. Res. 2017, 41, 857–862. [Google Scholar] [CrossRef]
- Lee, B.P.; Mehta, N.; Platt, L.; Gurakar, A.; Rice, J.P.; Lucey, M.R.; Im, G.Y.; Therapondos, G.; Han, H.; Victor, D.W.; et al. Outcomes of Early Liver Transplantation for Patients With Severe Alcoholic Hepatitis. Gastroenterology 2018, 155, 422–430. [Google Scholar] [CrossRef]
- Lucey, M.R. Liver transplantation in patients with alcoholic liver disease. Liver Transpl. 2011, 17, 751–759. [Google Scholar] [CrossRef]
- Egawa, H.; Nishimura, K.; Teramukai, S.; Yamamoto, M.; Umeshita, K.; Furukawa, H.; Uemoto, S. Risk factors for alcohol relapse after liver transplantation for alcoholic cirrhosis in Japan. Liver Transpl. 2014, 20, 298–310. [Google Scholar] [CrossRef]
- Dumortier, J.; Dharancy, S.; Cannesson, A.; Lassailly, G.; Rolland, B.; Pruvot, F.R.; Boillot, O.; Faure, S.; Guillaud, O.; Rigole-Donnadieu, H.; et al. Recurrent alcoholic cirrhosis in severe alcoholic relapse after liver transplantation: A frequent and serious complication. Am. J. Gastroenterol. 2015, 110, 1160–1166. [Google Scholar] [CrossRef]
- Satapathy, S.K.; Eason, J.D.; Nair, S.; Dryn, O.; Sylvestre, P.B.; Kocak, M.; Vanatta, J.M. Recidivism in Liver Transplant Recipients with Alcoholic Liver Disease: Analysis of Demographic, Psychosocial, and Histology Features. Exp. Clin. Transpl. 2015, 13, 430–440. [Google Scholar]
- Lombardo-Quezada, J.; Colmenero, J.; Lopez-Pelayo, H.; Gavotti, C.; Lopez, A.; Crespo, G.; Lopez, E.; Gual, A.; Lligona, A.; Navasa, M. Prediction of Alcohol Relapse Among Liver Transplant Candidates with Less Than 6 Months of Abstinence Using the High-Risk Alcoholism Relapse Score. Liver Transpl. 2019, 25, 1142–1154. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.T.; Said, A.; Agni, R.; Tome, S.; Hughes, S.; Dureja, P.; Lucey, M.R. The impact of acute alcoholic hepatitis in the explanted recipient liver on outcome after liver transplantation. Liver Transpl. 2007, 13, 1728–1735. [Google Scholar] [CrossRef] [PubMed]
- Grat, M.; Lewandowski, Z.; Grat, K.; Wronka, K.M.; Krasnodebski, M.; Barski, K.; Zborowska, H.; Patkowski, W.; Zieniewicz, K.; Krawczyk, M. Negative outcomes after liver transplantation in patients with alcoholic liver disease beyond the fifth post-transplant year. Clin. Transplant. 2014, 28, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- Lindenger, C.; Castedal, M.; Schult, A.; Aberg, F. Long-term survival and predictors of relapse and survival after liver transplantation for alcoholic liver disease. Scand. J. Gastroenterol. 2018, 53, 1553–1561. [Google Scholar] [CrossRef] [PubMed]
- Potts, S.G. Transplant psychiatry. J. R. Coll. Physicians Edinb. 2009, 39, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Karim, Z.; Intaraprasong, P.; Scudamore, C.H.; Erb, S.R.; Soos, J.G.; Cheung, E.; Cooper, P.; Buzckowski, A.K.; Chung, S.W.; Steinbrecher, U.P.; et al. Predictors of relapse to significant alcohol drinking after liver transplantation. Can. J. Gastroenterol. 2010, 24, 245–250. [Google Scholar] [CrossRef]
- Mathurin, P.; Bataller, R. Trends in the management and burden of alcoholic liver disease. J. Hepatol. 2015, 62, S38–S46. [Google Scholar] [CrossRef]
- Leon, M.; Varon, J.; Surani, S. When a liver transplant recipient goes back to alcohol abuse: Should we be more selective? World J. Gastroenterol. 2016, 22, 4789–4793. [Google Scholar] [CrossRef]
- Sliedrecht, W.; de Waart, R.; Witkiewitz, K.; Roozen, H.G. Alcohol use disorder relapse factors: A systematic review. Psychiatry Res. 2019, 278, 97–115. [Google Scholar] [CrossRef]
- Bianchi, G.; Marchesini, G.; Nicolino, F.; Graziani, R.; Sgarbi, D.; Loguercio, C.; Abbiati, R.; Zoli, M. Psychological status and depression in patients with liver cirrhosis. Dig. Liver Dis. 2005, 37, 593–600. [Google Scholar] [CrossRef]
- Grover, S.; Sarkar, S. Liver transplant-psychiatric and psychosocial aspects. J. Clin. Exp. Hepatol. 2012, 2, 382–392. [Google Scholar] [CrossRef] [PubMed]
- De Gottardi, A.; Spahr, L.; Gelez, P.; Morard, I.; Mentha, G.; Guillaud, O.; Majno, P.; Morel, P.; Hadengue, A.; Paliard, P.; et al. A simple score for predicting alcohol relapse after liver transplantation: Results from 387 patients over 15 years. Arch. Intern. Med. 2007, 167, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Chuncharunee, L.; Yamashiki, N.; Thakkinstian, A.; Sobhonslidsuk, A. Alcohol relapse and its predictors after liver transplantation for alcoholic liver disease: A systematic review and meta-analysis. BMC Gastroenterol. 2019, 19, 150. [Google Scholar] [CrossRef] [PubMed]
- Pillai, V.G.; Chen, C.L. Living donor liver transplantation in Taiwan-challenges beyond surgery. Hepatobiliary Surg. Nutr. 2016, 5, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.H.; Lu, C.L.; Strong, C.; Lin, Y.J.; Chen, Y.L.; Li, C.Y.; Tsai, C.C. Demographic and Urbanization Disparities of Liver Transplantation in Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 177. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-S. Alcoholic Liver Disease in the Asian–Pacific Region with High Prevalence of Chronic Viral Hepatitis. J. Med. Ultrasound 2016, 24, 93–100. [Google Scholar] [CrossRef]
- American Psychological Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR, 4th ed.; APA: Washington, DC, USA, 2000. [Google Scholar]
- Wu, M.K.; Hsu, L.W.; Huang, K.T.; Lin, C.C.; Wang, C.C.; Lin, T.L.; Li, W.F.; Goto, S.; Chen, C.L.; Chen, C.C. Assessment of relevant factors with respect to psychosocial properties in potential living donor candidates before liver transplantation. Neuropsychiatr. Dis. Treat. 2018, 14, 1999–2005. [Google Scholar] [CrossRef]
- Yates, W.R.; Booth, B.M.; Reed, D.A.; Brown, K.; Masterson, B.J. Descriptive and predictive validity of a high-risk alcoholism relapse model. J. Stud. Alcohol 1993, 54, 645–651. [Google Scholar] [CrossRef]
- DiMartini, A.; Magill, J.; Fitzgerald, M.G.; Jain, A.; Irish, W.; Khera, G.; Yates, W. Use of a high-risk alcohol relapse scale in evaluating liver transplant candidates. Alcohol Clin. Exp. Res. 2000, 24, 1198–1201. [Google Scholar] [CrossRef]
- Chen, G.H.; Yang, Y.; Lu, M.Q.; Cai, C.J.; Zhang, Q.; Zhang, Y.C.; Xu, C.; Li, H.; Wang, G.S.; Yi, S.H.; et al. Liver transplantation for end-stage alcoholic liver disease: A single-center experience from mainland China. Alcohol 2010, 44, 217–221. [Google Scholar] [CrossRef]
- Koob, G.F.; Volkow, N.D. Neurobiology of addiction: A neurocircuitry analysis. Lancet Psychiatry 2016, 3, 760–773. [Google Scholar] [CrossRef]
- Faure, S.; Herrero, A.; Jung, B.; Duny, Y.; Daures, J.P.; Mura, T.; Assenat, E.; Bismuth, M.; Bouyabrine, H.; Donnadieu-Rigole, H.; et al. Excessive alcohol consumption after liver transplantation impacts on long-term survival, whatever the primary indication. J. Hepatol. 2012, 57, 306–312. [Google Scholar] [CrossRef]
- Hendershot, C.S.; Witkiewitz, K.; George, W.H.; Marlatt, G.A. Relapse prevention for addictive behaviors. Subst. Abuse Treat Prev. Policy 2011, 6, 17. [Google Scholar] [CrossRef] [PubMed]
- Hingson, R.W.; Heeren, T.; Winter, M.R. Age at drinking onset and alcohol dependence: Age at onset, duration, and severity. Arch. Pediatr. Adolesc. Med. 2006, 160, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Perney, P.; Bismuth, M.; Sigaud, H.; Picot, M.C.; Jacquet, E.; Puche, P.; Jaber, S.; Rigole, H.; Navarro, F.; Eledjam, J.J.; et al. Are preoperative patterns of alcohol consumption predictive of relapse after liver transplantation for alcoholic liver disease? Transpl. Int. 2005, 18, 1292–1297. [Google Scholar] [CrossRef] [PubMed]
- Quigley, L.A.; Marlatt, G.A. Drinking Among Young Adults: Prevalence, Patterns, and Consequences. Alcohol Health Res. World 1996, 20, 185–191. [Google Scholar] [PubMed]
- De Wever, E.; Quaglino, V. Risk factors and psychological vulnerabilities to binge-drinking in youth. Encephale 2017, 43, 486–490. [Google Scholar] [CrossRef]
- Stein, E.; Witkiewitz, K. Trait self-control predicts drinking patterns during treatment for alcohol use disorder and recovery up to three years following treatment. Addict. Behav. 2019, 99, 106083. [Google Scholar] [CrossRef]
- Soravia, L.M.; Schlafli, K.; Stutz, S.; Rosner, S.; Moggi, F. Resistance to temptation: The interaction of external and internal control on alcohol use during residential treatment for alcohol use disorder. Alcohol Clin. Exp. Res. 2015, 39, 2209–2214. [Google Scholar] [CrossRef]
- Kelly, M.; Chick, J.; Gribble, R.; Gleeson, M.; Holton, M.; Winstanley, J.; McCaughan, G.W.; Haber, P.S. Predictors of relapse to harmful alcohol after orthotopic liver transplantation. Alcohol Alcohol. 2006, 41, 278–283. [Google Scholar] [CrossRef]
- Chen, C.L.; Kabiling, C.S.; Concejero, A.M. Why does living donor liver transplantation flourish in Asia? Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 746–751. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total (n = 98, n%) | Variable | Total (n = 98, n%) |
|---|---|---|---|
| Gender (n %) | Diagnosis | ||
| Male | 93 (94.9) | Alcoholic cirrhosis | 46 (46.9) |
| Female | 5 (5.1) | Alcohol + HCC 1 | 52 (53.1) |
| Age (y/o, mean ± SD (range)) | 51.5 ± 7.0 (36–68) | Alcohol start age (y/o, mean ± SD (range)) | 20.1 ± 4.4 (12–30) |
| Male | 51.8 ± 6.9 (37–68) | Pre-LT abstinence (months, mean ± SD(range))2 | 20.7 ± 27.9 (0–122.2) |
| Female | 47.0 ± 6.5 (36–53) | Pre-LT abstinence duration | |
| MELD score3 | 16.4 ± 6.9 (6–36) | >6 months | 68 (69.4) |
| Donation type | <6 months | 30 (30.6) | |
| Children (son/daughter) | 39 (39.8)/30 (30.6) | HAMD score (mean ± SD (range))4 | 3.6 ± 2.7 (0–13) |
| Siblings | 10 (10.2) | Family APGARindex (mean ± SD (range))5 | 8.8 ± 1.5 (3–10) |
| Spouse | 8 (8.2) | Family history of alcoholism | |
| Other relatives | 6 (6.1) | None | 48 (49.0) |
| Cadaveric donor | 5 (5.1) | Immediate family | 30 (30.6) |
| Marital status | Siblings | 20 (20.4) | |
| Single | 3 (3.1) | Previous diagnosis of mental illness | |
| Married | 87 (88.8) | No | 86 (87.8) |
| Separated/divorced | 8 (8.2) | Yes | 12 (12.2) |
| Educational level | Current diagnosis of mental illness | ||
| Primary school | 16 (16.3) | No | 81 (82.7) |
| Junior high school | 27 (27.6) | Yes | 17 (17.3) |
| Senior high school | 46 (46.9) | Alcohol use disorder | |
| College or above | 9 (9.2) | Alcohol abuse | 8 (8.2) |
| Occupation | Alcohol dependence | 90 (91.8) | |
| Housewife/Unemployed | 11 (11.2) | Alcohol relapse | |
| Retired | 76 (77.6) | No | 82 (83.7) |
| Employed | 11 (11.2) | Yes | 16 (16.3) |
| Smoke | |||
| No | 11 (11.2) | ||
| Yes | 87 (88.8) |
| Variable | Non-Relapse (n = 82) | Relapse (n = 16) | Univariate Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|
| Gender | ||||
| Female | 3 | 2 | 1 | |
| Male | 79 | 14 | 0.266 (0.041–1.737) | 0.167 |
| Age (y/o) (mean ± SD) | 51.5 ± 7.0 | 51.6 ± 7.0 | 1. 002 (0.927–1.082) | 0.963 |
| Donation type | ||||
| Children (son/daughter) | 32/26 | 7/4 | 1 | |
| Siblings | 7 | 3 | 2.260 (0.505–10.110) | 0.286 |
| Spouse | 8 | 0 | 0.000 (0.000–2.000) | 0.999 |
| Other relatives | 6 | 0 | 0.000 (0.000–2.000) | 0.999 |
| Cadaveric donor | 3 | 2 | 3.515 (0.525–23.543) | 0.195 |
| Marital status | ||||
| Single | 2 | 1 | 1 | |
| Married | 75 | 12 | 0.320 (0.027–3.808) | 0.367 |
| Separated/divorced | 5 | 3 | 1.200 (0.073–19.631) | 0.898 |
| Educational level | ||||
| Primary school | 11 | 5 | 1 | |
| Junior high school | 24 | 3 | 0.275 (0.056–1.361) | 0.114 |
| Senior high school | 38 | 8 | 0.463 (0.126–1.705) | 0.274 |
| College or above | 9 | 0 | 0.000 (0.000–0.000) | 0.999 |
| Occupation | ||||
| Housewife/Unemployed | 9 | 2 | 1 | |
| Retired | 63 | 13 | 0.929 (0.179–4.808) | 0.930 |
| Employed | 10 | 1 | 0.450 (0.035–5.843) | 0.542 |
| Smoke | ||||
| No | 10 | 1 | 1 | |
| Yes | 72 | 15 | 2.083 (0.248–17.523) | 0.499 |
| Diagnosis | ||||
| Alcohol | 36 | 10 | 1 | |
| Alcohol + HCC | 46 | 6 | 0.470 (0.156–1.414) | 0.179 |
| Alcohol start age (y/o) (mean ± SD) | 20.6 ± 4.4 | 17.4 ± 3.1 | 0.781 (0.647–942) | 0.010 * |
| Pre-LT abstinence (months) (mean ± SD) | 22.1 ± 27.5 | 13.0 ± 29.6 | 0.982 (0.951–1.013) | 0.257 |
| Pre-LT abstinence duration | ||||
| <6 months | 19 | 11 | 1 | |
| >6 months | 63 | 5 | 0.137 (0.042–4.444) | 0.001 * |
| HAMD scores (mean ± SD) | 3.5 ± 2.6 | 4.1 ± 3.5 | 1.074 (0.895–1.289) | 0.443 |
| APGAR scores | 8.8 ± 1.4 | 8.6 ± 1.9 | 0.896 (0.638–1.258) | 0.526 |
| Family history of alcoholism | ||||
| None | 41 | 7 | 1 | |
| Immediate family | 25 | 5 | 1.171 (0.335–4.092) | 0.804 |
| Siblings | 16 | 4 | 1.464 (0.377–5.691) | 0.582 |
| Previous diagnosis of mental illness | ||||
| No | 73 | 13 | 1 | |
| Yes | 9 | 3 | 1.872 (0.446–7.850) | 0.391 |
| Current diagnosis of mental illness | ||||
| No | 69 | 12 | 1 | |
| Yes | 13 | 4 | 1.769 (0.493–6.347) | 0.381 |
| Alcohol use disorders | ||||
| Alcohol abuse | 7 | 1 | 1 | |
| Alcohol dependence | 75 | 15 | 1.400 (0.160–12.230) | 0.761 |
| Variable | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Younger age at starting alcohol | 1.261 | 1.039–1.531 | 0.019 |
| Abstinent <6 months pre-transplant | 7.045 | 2.059–24.106 | 0.002 |
| Pre-LT Abstinence Duration | Non-Relapse | Relapse | Total (n) |
|---|---|---|---|
| <6 months | 19 | 11 | 30 |
| >6 months | 63 | 5 | 68 |
| 82 | 16 | 98 | |
| Sensitivity: 0.783 | Specificity: 0.688 | PPV 1: 0.688 | NPV 2: 0.768 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, T.-W.; Chen, Y.-M.; Wang, C.-C.; Lin, C.-C.; Huang, K.-T.; Liu, Y.-W.; Hsu, L.-W.; Li, W.-F.; Chan, Y.-C.; Chen, C.-L.; et al. Incidence and Risk Factors of Alcohol Relapse after Liver Transplantation: Analysis of Pre-Transplant Abstinence and Psychosocial Features. J. Clin. Med. 2020, 9, 3716. https://doi.org/10.3390/jcm9113716
Yu T-W, Chen Y-M, Wang C-C, Lin C-C, Huang K-T, Liu Y-W, Hsu L-W, Li W-F, Chan Y-C, Chen C-L, et al. Incidence and Risk Factors of Alcohol Relapse after Liver Transplantation: Analysis of Pre-Transplant Abstinence and Psychosocial Features. Journal of Clinical Medicine. 2020; 9(11):3716. https://doi.org/10.3390/jcm9113716
Chicago/Turabian StyleYu, Tien-Wei, Yu-Ming Chen, Chih-Chi Wang, Chih-Che Lin, Kuang-Tzu Huang, Yueh-Wei Liu, Li-Wen Hsu, Wei-Feng Li, Yi-Chai Chan, Chao-Long Chen, and et al. 2020. "Incidence and Risk Factors of Alcohol Relapse after Liver Transplantation: Analysis of Pre-Transplant Abstinence and Psychosocial Features" Journal of Clinical Medicine 9, no. 11: 3716. https://doi.org/10.3390/jcm9113716
APA StyleYu, T.-W., Chen, Y.-M., Wang, C.-C., Lin, C.-C., Huang, K.-T., Liu, Y.-W., Hsu, L.-W., Li, W.-F., Chan, Y.-C., Chen, C.-L., & Chen, C.-C. (2020). Incidence and Risk Factors of Alcohol Relapse after Liver Transplantation: Analysis of Pre-Transplant Abstinence and Psychosocial Features. Journal of Clinical Medicine, 9(11), 3716. https://doi.org/10.3390/jcm9113716