The New ELN Recommendations for Treating CML

Abstract
1. Introduction
2. Initial Diagnostic Workup
3. Treatment Monitoring
4. First-Line Treatment
5. Second- and Higher-Line Treatment
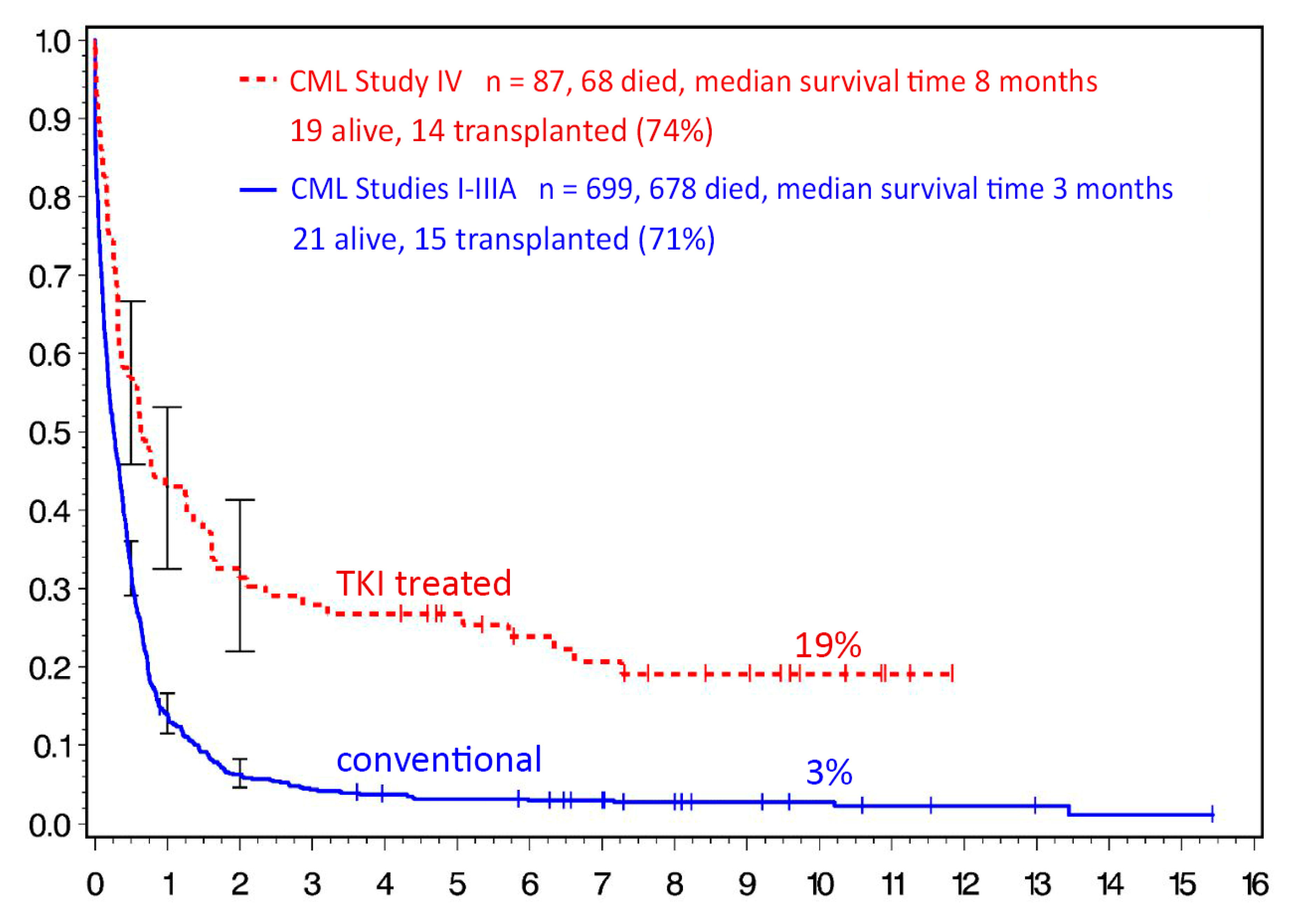
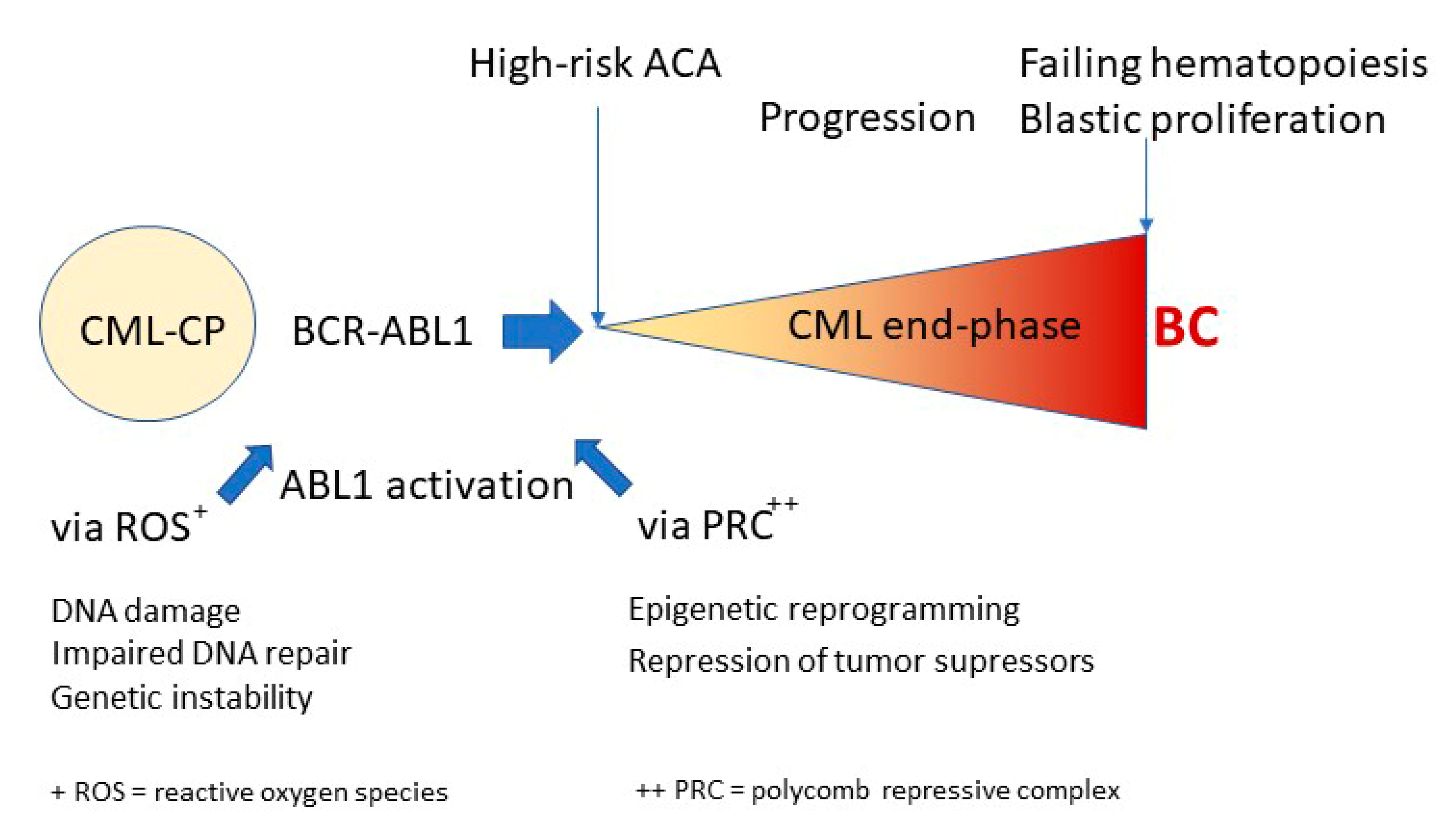
6. CML End-Phase and Blast Crisis
7. Treatment Discontinuation and Treatment-Free Remission
8. Pregnancy
9. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Sasaki, K.; Strom, S.S.; O’Brien, S.; Jabbour, E.; Ravandi, F.; Konopleva, M.; Borthakur, G.; Pemmaraju, N.; Daver, N.; Jain, P.; et al. Relative survival in patients with chronic-phase chronic myeloid leukaemia in the tyrosine-kinase inhibitor era: Analysis of patient data from six prospective clinical trials. Lancet Haematol. 2015, 2, e186–e193. [Google Scholar] [CrossRef]
- Hehlmann, R.; Lauseker, M.; Saußele, S.; Pfirrmann, M.; Krause, S.; Kolb, H.J.; Neubauer, A.; Hossfeld, D.K.; Nerl, C.; Gratwohl, A.; et al. Assessment of imatinib as first-line treatment of chronic myeloid leukemia: 10-year survival results of the randomized CML study IV and impact of non-CML determinants. Leukemia 2017, 31, 2398–2406. [Google Scholar] [CrossRef] [PubMed]
- Thielen, N.; Visser, O.; Ossenkoppele, G.J.; Janssen, J. Chronic myeloid leukemia in the Netherlands: A population-based study on incidence, treatment, and survival in 3585 patients from 1989 to 2012. Eur. J. Haematol. 2015, 97, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Bower, H.; Björkholm, M.; Dickman, P.W.; Höglund, M.; Lambert, P.C.; Andersson, T.M.-L. Life expectancy of patients with chronic myeloid leukemia approaches the life expectancy of the general population. J. Clin. Oncol. 2016, 34, 2851–2857. [Google Scholar] [CrossRef] [PubMed]
- Welch, H.G.; Kramer, B.S.; Black, W.C. Epidemiologic signatures in cancer. N. Engl. J. Med. 2019, 381, 1378–1386. [Google Scholar] [CrossRef] [PubMed]
- Baccarani, M.; Saglio, G.; Goldman, J.; Hochhaus, A.; Simonsson, B.; Appelbaum, F.; Apperley, J.; Cervantes, F.; Cortes, J.; Deininger, M.; et al. Evolving concepts in the management of chronic myeloid leukemia: Recommendations from an expert panel on behalf of the European LeukemiaNet. Blood 2006, 108, 1809–1820. [Google Scholar] [CrossRef]
- Baccarani, M.; Cortes, J.; Pane, F.; Niederwieser, D.; Saglio, G.; Apperley, J.; Cervantes, F.; Deininger, M.; Gratwohl, A.; Guilhot, F.; et al. Chronic myeloid leukemia: An update of concepts and management recommendations of European LeukemiaNet. J. Clin. Oncol. 2009, 27, 6041–6051. [Google Scholar] [CrossRef]
- Baccarani, M.; Deininger, M.W.; Rosti, G.; Hochhaus, A.; Soverini, S.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Guilhot, F.; et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013. Blood 2013, 122, 872–884. [Google Scholar] [CrossRef]
- Hehlmann, R. Chronic myeloid leukemia in 2020. HemaSphere 2020, 4, e468. [Google Scholar] [CrossRef]
- Hochhaus, A.; Baccarani, M.; Silver, R.T.; Schiffer, C.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Deininger, M.W.; Guilhot, F.; et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia 2020, 34, 966–984. [Google Scholar] [CrossRef]
- Pfirrmann, M.; Baccarani, M.; Saussele, S.; Guilhot, J.; Cervantes, F.; Ossenkoppele, G.; Hoffmann, V.S.; Castagnetti, F.; Hasford, J.; Hehlmann, R.; et al. Prognosis of long-term survival considering disease-specific death in patients with chronic myeloid leukemia. Leukemia 2016, 30, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Pfirrmann, M.; Clark, R.E.; Prejzner, W.; Lauseker, M.; Baccarani, M.; Saussele, S.; Guilhot, F.; Heibl, S.; Hehlmann, R.; Faber, E.; et al. The EUTOS long-term survival (ELTS) score is superior to the Sokal score for predicting survival in chronic myeloid leukemia. Leukemia 2020, 34, 2138–2149. [Google Scholar] [CrossRef] [PubMed]
- Cross, N.C.P.; White, H.E.; Muller, M.C.; Saglio, G.; Hochhaus, A. Standardized definitions of molecular response in chronic myeloid leukemia. Leukemia 2012, 26, 2172–2175. [Google Scholar] [CrossRef] [PubMed]
- Cross, N.C.P.; White, H.E.; Colomer, D.; Ehrencrona, H.; Foroni, L.; Gottardi, E.; Lange, T.; Lion, T.; Polakova, K.M.; Dulucq, S.; et al. Laboratory recommendations for scoring deep molecular responses following treatment for chronic myeloid leukemia. Leukemia 2015, 29, 999–1003. [Google Scholar] [CrossRef]
- Hehlmann, R.; Lauseker, M.; Jung-Munkwitz, S.; Leitner, A.; Müller, M.C.; Pletsch, N.; Proetel, U.; Haferlach, C.; Schlegelberger, B.; Balleisen, L.; et al. Tolerability-adapted imatinib 800 mg/d versus 400 mg/d versus 400 mg/d plus interferon-α in newly diagnosed chronic myeloid leukemia. J. Clin. Oncol. 2011, 29, 1634–1642. [Google Scholar] [CrossRef]
- Hehlmann, R.; Müller, M.C.; Lauseker, M.; Hanfstein, B.; Fabarius, A.; Schreiber, A.; Proetel, U.; Pletsch, N.; Pfirrmann, M.; Haferlach, C.; et al. Deep molecular response is reached by the majority of patients treated with imatinib, predicts survival, and is achieved more quickly by optimized high-dose imatinib: Results from the randomized CML-study IV. J. Clin. Oncol. 2014, 32, 415–423. [Google Scholar] [CrossRef]
- Hochhaus, A.; Larson, R.A.; Guilhot, F.; Radich, J.P.; Branford, S.; Hughes, T.P.; Baccarani, M.; Deininger, M.W.; Cervantes, F.; Fujihara, S.; et al. Long-term outcomes of imatinib treatment for CML. N. Engl. J. Med. 2017, 376, 917–927. [Google Scholar] [CrossRef]
- Lauseker, M.; Hanfstein, B.; Haferlach, C.; Schnittger, S.; Pfirrmann, M.; Fabarius, A. Equivalence of BCR-ABL transcript levels with complete cytogenetic remission in patients with chronic myeloid leukemia in chronic phase. J. Cancer Res. Clin. Oncol. 2014, 140, 1965–1969. [Google Scholar] [CrossRef]
- Kalmanti, L.; Saussele, S.; Lauseker, M.; Müller, M.C.; Dietz, C.T.; Heinrich, L. Safety and efficacy of imatinib in CML over a period of 10 years: Data from the randomized CML-study IV. Leukemia 2015, 29, 1123–1132. [Google Scholar] [CrossRef]
- Steegmann, J.L.; Baccarani, M.; Breccia, M.; Casado, L.F.; García-Gutiérrez, V.; Hochhaus, A.; Kim, D.-W.; Kim, T.D.; Khoury, H.J.; Le Coutre, P.; et al. European LeukemiaNet recommendations for the management and avoidance of adverse events of treatment in chronic myeloid leukaemia. Leukemia 2016, 30, 1648–1671. [Google Scholar] [CrossRef]
- Cortes, J.E.; Saglio, G.; Kantarjian, H.M.; Baccarani, M.; Mayer, J.; Boqué, C.; Shah, N.P.; Chuah, C.; Casanova, L.; Bradley-Garelik, B.; et al. Final 5-year study results of DASISION: The dasatinib versus imatinib study in treatment-naïve chronic myeloid leukemia patients trial. J. Clin. Oncol. 2016, 34, 2333–2340. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, A.; Saglio, G.; Hughes, T.P.; Larson, A.R.; Kim, D.-W.; Issaragrisil, S.; Le Coutre, P.D.; Etienne, G.; Dorlhiac-Llacer, E.P.; Clark, E.R.; et al. Long-term benefits and risks of frontline nilotinib vs. imatinib for chronic myeloid leukemia in chronic phase: 5-year update of the randomized ENESTnd trial. Leukemia 2016, 30, 1044–1054. [Google Scholar] [CrossRef] [PubMed]
- Padula, W.V.; Larson, R.A.; Dusetzina, S.B.; Apperley, J.F.; Hehlmann, R.; Baccarani, M.; Eigendorff, E.; Guilhot, J.; Guilhot, F.; Mahon, F.-X.; et al. Cost-effectiveness of tyrosine kinase inhibitor treatment strategies for chronic myeloid leukemia in chronic phase after generic entry of imatinib in the united states. J. Natl. Cancer Inst. 2016, 108, 003. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.-C.T.; Cortes, J.E.; Kantarjian, H.M. Treatment value of second-generation BCR-ABL1 tyrosine kinase inhibitors compared with imatinib to achieve treatment-free remission in patients with chronic myeloid leukaemia: A modelling study. Lancet Haematol. 2019, 6, e398–e408. [Google Scholar] [CrossRef]
- Yamamoto, C.; Nakashima, H.; Ikeda, T.; Kawaguchi, S.-I.; Toda, Y.; Ito, S.; Mashima, K.; Nagayama, T.; Umino, K.; Minakata, D.; et al. Analysis of the cost-effectiveness of treatment strategies for CML with incorporation of treatment discontinuation. Blood Adv. 2019, 3, 3266–3277. [Google Scholar] [CrossRef]
- Naqvi, K.; Jabbour, E.; Skinner, J.; Bs, K.A.; Bs, S.D.; Yilmaz, M.; Ferrajoli, A.; Bose, P.; Thompson, P.; Alvarado, Y.; et al. Long-term follow-up of lower dose dasatinib (50 mg daily) as frontline therapy in newly diagnosed chronic-phase chronic myeloid leukemia. Cancer 2020, 126, 67–75. [Google Scholar] [CrossRef]
- Hughes, T.P.; Saglio, G.; Larson, R.A.; Kantarjian, H.M.; Kim, D.N.-W.; Issaragrisil, S.; Le Coutre, P.; Etienne, G.; Boquimpani, C.; Clark, R.E.; et al. Long-term outcomes in patients with chronic myeloid leukemia in chronic phase receiving frontline nilotinib versus imatinib: Enestnd 10-year analysis. Blood 2019, 134, 2924. [Google Scholar] [CrossRef]
- Saußele, S.; Krauß, M.-P.; Hehlmann, R.; Lauseker, M.; Proetel, U.; Kalmanti, L.; Hanfstein, B.; Fabarius, A.; Kraemer, D.; Berdel, W.E.; et al. Impact of comorbidities on overall survival in patients with chronic myeloid leukemia: Results of the randomized CML study IV. Blood 2015, 126, 42–49. [Google Scholar] [CrossRef]
- Cortes, J.E.; Gambacorti-Passerini, C.; Deininger, M.W.; Mauro, M.J.; Chuah, C.; Kim, D.-W.; Dyagil, I.; Glushko, N.; Milojkovic, D.; Le Coutre, P.; et al. Bosutinib versus imatinib for newly diagnosed chronic myeloid leukemia: Results from the randomized BFORE trial. J. Clin. Oncol. 2018, 36, 231–237. [Google Scholar] [CrossRef]
- Soverini, S.; Bavaro, L.; De Benedittis, C.; Martelli, M.; Iurlo, A.; Orofino, N.; Sica, S.; Sora, F.; Lunghi, F.; Ciceri, F.; et al. Prospective assessment of NGS-detectable mutations in CML patients with non-optimal response: The NEXT-in-CML study. Blood J. Am. Soc. Hematol. 2020, 135, 534–541. [Google Scholar]
- Kizilors, A.; Crisà, E.; Lea, N.; Passera, R.; Mian, S.; Anwar, J.; Best, S.; Nicolini, F.E.; Ireland, R.; Aldouri, M.; et al. Effect of low-level BCR-ABL1 kinase domain mutations identified by next-generation sequencing in patients with chronic myeloid leukaemia: A population-based study. Lancet Haematol. 2019, 6, e276–e284. [Google Scholar] [CrossRef]
- Cortes, J.E.; Kim, D.-W.; Pinilla-Ibarz, J.L.; Le Coutre, P.; Paquette, R.; Chuah, C.; Nicolini, F.; Apperley, J.; Khoury, H.; Talpaz, M.; et al. A phase 2 trial of ponatinib in philadelphia chromosome–positive leukemias. N. Engl. J. Med. 2013, 369, 1783–1796. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Lomaia, E.; Turkina, A.; Moiraghi, B.; Sutton, U.M.; Pavlovsky, C.; Kim, D.W. Interim analysis from the OPTIC trial-A dose-ranging study of 3 starting doses of ponatinib. Clin. Lymphoma Myeloma Leuk. 2020, 20, S234. [Google Scholar]
- Lichtin, A.E.; Woolf, S.H.; Silver, R.T.; Hehlmann, R. Chronic myeloid leukemia—ASH practice guideline and beyond. Hematol. Am. Soc. Hematol. Educ. Prog. 1998, 435–453. [Google Scholar]
- Gratwohl, A.; Pfirrmann, M.; Zander, A.; Kröger, N.; Beelen, D.; Novotny, J.; Nerl, C.; Scheid, C.; Spiekermann, K.; Mayer, J. Long-term outcome of patients with newly diagnosed chronic myeloid leukemia: A randomized comparison of stem cell transplantation with drug treatment. Leukemia 2016, 30, 562–569. [Google Scholar] [CrossRef]
- Saussele, S.; Lauseker, M.; Gratwohl, A.; Beelen, D.W.; Bunjes, D.; Schwerdtfeger, R.; Kolb, H.-J.; Ho, A.D.; Falge, C.; Holler, E.; et al. Allogeneic hematopoietic stem cell transplantation (allo SCT) for chronic myeloid leukemia in the imatinib era: Evaluation of its impact within a subgroup of the randomized German CML Study IV. Blood 2010, 115, 1880–1885. [Google Scholar] [CrossRef]
- Saussele, S.; Lauseker, M.; Müller, M.C.; Gratwohl, A.; Beelen, D.; Bunjes, D.W.; Schwerdtfeger, R.; Kolb, H.-J.; Ho, A.D.; Falge, C.; et al. Allogeneic hematopoietic stem cell transplantation (hsct) in the imatinib-era: Update on the survival outcome following allogeneic HSCT after imatinib failure; results of the german CML study IV. Blood 2014, 124, 2567. [Google Scholar] [CrossRef]
- Jiang, H.; Xu, L.-P.; Liu, D.-H.; Liu, K.-Y.; Chen, S.-S.; Jiang, B.; Jiang, Q.; Chen, H.; Chen, Y.-H.; Han, W.; et al. Allogeneic hematopoietic SCT in combination with tyrosine kinase inhibitor treatment compared with TKI treatment alone in CML blast crisis. Bone Marrow Transplant. 2014, 49, 1146–1154. [Google Scholar] [CrossRef]
- Oyekunle, A.; Zander, A.R.; Binder, M.; Ayuk, F.; Zabelina, T.; Christopeit, M.; Stübig, T.; Alchalby, H.; Schafhausen, P.; Lellek, H.; et al. Outcome of allogeneic SCT in patients with chronic myeloid leukemia in the era of tyrosine kinase inhibitor therapy. Ann. Hematol. 2013, 92, 487–496. [Google Scholar] [CrossRef]
- Hehlmann, R.; Voskanyan, A.; Lauseker, M.; Pfirrmann, M.; Kalmanti, L.; Rinaldetti, S.; Kohlbrenner, K.; Haferlach, C.; Schlegelberger, B.; Fabarius, A.; et al. High-risk additional chromosomal abnormalities at low blast counts herald death by CML. Leukemia 2020, 34, 2074–2086. [Google Scholar] [CrossRef]
- Fabarius, A.; Kalmanti, L.; Dietz, C.T.; Lauseker, M.; Rinaldetti, S.; Haferlach, C.; Göhring, G.; Schlegelberger, B.; Jotterand, M.; Hanfstein, B.; et al. Impact of unbalanced minor route versus major route karyotypes at diagnosis on prognosis of CML. Ann. Hematol. 2015, 94, 2015–2024. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Cortes, J.E.; Tang, G.; Khoury, J.D.; Wang, S.; Bueso-Ramos, C.E.; DiGiuseppe, J.A.; Chen, Z.; Kantarjian, H.M.; Medeiros, L.J.; et al. Risk stratification of chromosomal abnormalities in chronic myelogenous leukemia in the era of tyrosine kinase inhibitor therapy. Blood 2016, 127, 2742–2750. [Google Scholar] [CrossRef] [PubMed]
- Gong, Z.; Medeiros, L.J.; Cortes, J.E.; Chen, Z.; Zheng, L.; Li, Y.; Bai, S.; Lin, P.; Miranda, R.N.; Jorgensen, J.L.; et al. Cytogenetics-based risk prediction of blastic transformation of chronic myeloid leukemia in the era of TKI therapy. Blood Adv. 2017, 1, 2541–2552. [Google Scholar] [CrossRef] [PubMed]
- Grossmann, V.; Kohlmann, A.; Zenger, M.; Schindela, S.; Eder, C.; Weissmann, S.; Schnittger, S.; Kern, W.; Muller, M.C.; Hochhaus, A.; et al. A deep-sequencing study of chronic myeloid leukemia patients in blast crisis (BC-CML) detects mutations in 76.9% of cases. Leukemia 2011, 25, 557–560. [Google Scholar] [CrossRef]
- Branford, S.; Wang, P.; Yeung, D.T.; Thomson, D.; Purins, A.; Wadham, C.; Shahrin, N.H.; Marum, J.E.; Nataren, N.; Parker, W.T.; et al. Integrative genomic analysis reveals cancer-associated mutations at diagnosis of CML in patients with high-risk disease. Blood 2018, 132, 948–961. [Google Scholar] [CrossRef]
- Koptyra, M.; Falinski, R.; Nowicki, M.O.; Stoklosa, T.; Majsterek, I.; Nieborowska-Skorska, M.; Blasiak, J.; Skorski, T. BCR/ABL kinase induces self-mutagenesis via reactive oxygen species to encode imatinib resistance. Blood 2006, 108, 319–327. [Google Scholar] [CrossRef]
- Mohty, M.; Yong, A.S.M.; Szydlo, R.; Apperley, J.F.; Melo, J.V. The polycomb group BMI1 gene is a molecular marker for predicting prognosis of chronic myeloid leukemia. Blood 2007, 110, 380–383. [Google Scholar] [CrossRef]
- Ko, T.K.; Javed, A.; Lee, K.L.; Pathiraja, T.N.; Liu, X.; Malik, S.; Soh, S.X.; Heng, X.T.; Takahashi, N.; Tan, J.H.J.; et al. An integrative model of pathway convergence in genetically heterogeneous blast crisis chronic myeloid leukemia. Blood 2020, 135, 2337–2353. [Google Scholar] [CrossRef]
- Johansson, B.; Fioretos, T.; Mitelman, F. Cytogenetic and molecular genetic evolution of chronic myeloid leukemia. Acta Haematol. 2002, 107, 76–94. [Google Scholar] [CrossRef]
- Mitelman, F.; LeVan, G.; Nilsson, P.G.; Brandt, L. Non-random karyotypic evolution in chronic myeloid leukemia. Int. J. Cancer 1976, 18, 24–30. [Google Scholar] [CrossRef]
- Soverini, S.; Hochhaus, A.; Nicolini, F.E.; Gruber, F.; Lange, T.; Saglio, G.; Pane, F.; Müller, M.C.; Ernst, T.; Rosti, G.; et al. BCR-ABL kinase domain mutation analysis in chronic myeloid leukemia patients treated with tyrosine kinase inhibitors: Recommendations from an expert panel on behalf of European LeukemiaNet. Blood 2011, 118, 1208–1215. [Google Scholar] [CrossRef] [PubMed]
- Hehlmann, R. How I treat CML blast crisis. Blood 2012, 120, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Milojkovic, D.; Ibrahim, A.; Reid, A.; Foroni, L.; Apperley, J.; Marin, D. Efficacy of combining dasatinib and FLAG-IDA for patients with chronic myeloid leukemia in blastic transformation. Haematologica 2011, 97, 473–474. [Google Scholar] [CrossRef]
- Copland, M.; Slade, D.; Byrne, J.; Brock, K.; De Lacallade, H.; Craddock, C.; Clark, R.; Smith, M.; Bishiop, R.; Milojkovic, D.; et al. FLAG-IDA and ponatinib in patients with blast phase chronic myeloid leukemia: Results from the phase I/II UK trials acceleration program matchpoint trial. Blood 2017, 134, 497. [Google Scholar] [CrossRef]
- Strati, P.; Kantarjian, H.; Thomas, D.; O’Brien, S.; Konoplev, S.; Jorgensen, J.L.; Luthra, R.; Abruzzo, L.; Jabbour, E.; Quintas-Cardama, A.; et al. HCVAD plus imatinib or dasatinib in lymphoid blastic phase chronic myeloid leukemia. Cancer 2014, 120, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Rousselot, P.; Huguet, F.; Rea, D.; Legros, L.; Cayuela, J.-M.; Maarek, O.; Blanchet, O.; Marit, G.; Gluckman, E.; Reiffers, J.; et al. Imatinib mesylate discontinuation in patients with chronic myelogenous leukemia in complete molecular remission for more than 2 years. Blood 2007, 109, 58–60. [Google Scholar] [CrossRef]
- Mahon, F.X.; Réa, D.; Guilhot, J.; Guilhot, F.; Huguet, F.; Nicolini, F.; Lgros, L.; Charbonnier, A.; Guerci, A.; Varet, B.; et al. Discontinuation of imatinib in patients with chronic myeloid leukemia who have maintained complete molecular remission for at least 2 years: The prospective, multicenter Stop Imatinib (STIM) trial. Lancet. Oncol. 2010, 11, 1029–1035. [Google Scholar] [CrossRef]
- Saussele, S.; Richter, J.; Guilhot, J.; Gruber, F.X.; Hjorth-Hansen, H.; Almeida, A.; Janssen, J.J.W.M.; Mayer, P.J.; Koskenvesa, P.; Panayiotidis, P.; et al. Discontinuation of tyrosine kinase inhibitor therapy in chronic myeloid leukemia (EURO-SKI): A prespecified interim analysis of a prospective, multicenter, non-randomized, trial. Lancet Oncol. 2018, 19, 747–757. [Google Scholar] [CrossRef]
- Etienne, G.; Guilhot, J.; Rea, D.; Rigal-Huguet, F.; Nicolini, F.; Charbonnier, A.; Guerci-Bresler, A.; Legros, L.; Varet, B.; Gardembas, M.; et al. Long-term follow-up of the french stop imatinib (STIM1) study in patients with chronic myeloid leukemia. J. Clin. Oncol. 2017, 35, 298–305. [Google Scholar] [CrossRef]
- Ross, D.M.; Branford, S.; Seymour, J.F.; Schwarer, A.P.; Arthur, C.; Yeung, D.T.; Dang, P.; Goyne, J.M.; Slader, C.; Filshie, R.J.; et al. Safety and efficacy of imatinib cessation for CML patients with stable undetectable minimal residual disease: Results from the TWISTER study. Blood 2013, 122, 515–522. [Google Scholar] [CrossRef]
- Rousselot, P.; Charbonnier, A.; Cony-Makhoul, P.; Agape, P.; Nicolini, F.E.; Varet, B.; Gardembas, M.; Etienne, G.; Réa, D.; Roy, L.; et al. Loss of major molecular response as a trigger for restarting tyrosine kinase inhibitor therapy in patients with chronic-phase chronic myelogenous leukemia who have stopped imatinib after durable undetectable disease. J. Clin. Oncol. 2014, 32, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-E.; Choi, S.Y.; Song, H.-Y.; Kim, S.-H.; Choi, M.-Y.; Park, J.S.; Kim, H.-J.; Zang, D.Y.; Oh, S.; Do, Y.R.; et al. Imatinib withdrawal syndrome and longer duration of imatinib have a close association with a lower molecular relapse after treatment discontinuation: The KID study. Haematologica 2016, 101, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Zang, D.Y.; Lee, W.S.; Mun, Y.-C.; Do, Y.R.; Oh, S.; Lee, S.-E.; Choi, S.Y.; Kim, D.-W. Long-term follow-up after treatment discontinuation in patients with chronic myeloid leukemia: The korean imatinib discontinuation (KID) study. Blood 2018, 132, 4252. [Google Scholar] [CrossRef]
- Nicolini, F.E.; Dulucq, S.; Guilhot, J.; Etienne, G.; Mahon, F.-X. The evaluation of residual disease by digital PCR, and TKI duration are critical predictive factors for molecular recurrence after for stopping imatinib first-line in chronic phase CML patients: Results of the STIM2 study. Blood 2018, 132, 462. [Google Scholar] [CrossRef]
- Mori, S.; Vagge, E.; Le Coutre, P.; Abruzzese, E.; Martino, B.; Pungolino, E.; Elena, C.; Pierri, I.; Assouline, S.; D’Emilio, A.; et al. Age and dPCR can predict relapse in CML patients who discontinued imatinib: The ISAV study. Am. J. Hematol. 2015, 90, 910–914. [Google Scholar] [CrossRef]
- Mori, S.; Le Coutre, P.; Abruzzese, E.; Martino, B.; Pungolino, E.; Elena, C.; Bergamaschi, M.; Assouline, S.; Di Bona, E.; Gozzini, A.; et al. Imatinib suspension and validation (ISAV) study: Final results at 79 months. Blood 2018, 132, 461. [Google Scholar] [CrossRef]
- Rea, D.; Nicolini, F.E.; Tulliez, M.; Guilhot, F.; Guilhot, J.; Guerci-Bresler, A.; Gardembas, M.; Coiteux, V.; Guillerm, G.; Legros, L.; et al. Discontinuation of dasatinib or nilotinib in chronic myeloid leukemia: Interim analysis of the STOP 2G-TKI study. Blood 2017, 129, 846–854. [Google Scholar] [CrossRef]
- Imagawa, J.; Tanaka, H.; Okada, M.; Nakamae, H.; Hino, P.M.; Murai, K.; Ishida, P.Y.; Kumagai, T.; Sato, S.; Ohashi, K.; et al. Discontinuation of dasatinib in patients with chronic myeloid leukemia who have maintained deep molecular response for longer than 1 year (DADI trial): A multicenter phase 2 trial. Lancet Haematol. 2015, 2, e528–e535. [Google Scholar] [CrossRef]
- Kadowaki, N.; Kawaguchi, T.; Kuroda, J.; Nakamae, H.; Matsumura, I.; Miyamoto, T.; Ishikawa, J.; Nagafuji, K.; Imamura, Y.; Yamazaki, H.; et al. Discontinuation of nilotinib in patients with chronic myeloid leukemia who have maintained deep molecular responses for at least 2 years: A multicenter phase 2 stop nilotinib (nilst) trial. Blood 2016, 128, 790. [Google Scholar] [CrossRef]
- Kim, D.D.H.; Bence-Bruckler, F.I.; Forrest, D.L.; Savoie, M.L.; Couban, S.; Busque, P.F.L.; Delage, M.R.; Laneuville, F.P.; Liew, E.; Xenocostas, A.; et al. Treatment-free remission accomplished by dasatinib (TRAD): Preliminary results of the pan-canadian tyrosine kinase inhibitor discontinuation trial. Blood 2016, 128, 1922. [Google Scholar] [CrossRef]
- Shah, N.; García-Gutiérrez, J.V.; Jiménez-Velasco, A.; Larson, S.; Saussele, S.; Rea, D.; Mahon, F.-X.; Levy, M.; Gómez-Casares, M.; Luciano, L.; et al. PF408 dasfree 2-year update: Dasatinib discontinuation in patients (PTS) with chronic myeloid leukemia in chronic phase (CML-CP) and deep molecular response (DMR). HemaSphere 2019, 3, 156. [Google Scholar] [CrossRef]
- Hughes, F.T.P.; Boquimpani, C.M.; Takahashi, N.; Benyamini, N.; Clementino, N.C.D.; Shuvaev, V.; Ailawadhi, S.; Lipton, J.H.; Turkina, A.G.; Moiraghi, E.B.; et al. Treatment-free remission in patients with chronic myeloid leukemia in chronic phase according to reasons for switching from imatinib to nilotinib: Subgroup analysis from ENESTop. Blood 2016, 128, 792. [Google Scholar] [CrossRef]
- Takahashi, N.; Nishiwaki, K.; Nakaseko, C.; Aotsuka, N.; Sano, K.; Ohwada, C.; Kuroki, J.; Kimura, H.; Tokuhira, M.; Mitani, K.; et al. Treatment-free remission after two-year consolidation therapy with nilotinib in patients with chronic myeloid leukemia: STAT2 trial in Japan. Haematologica 2018, 103, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, A.; Masszi, T.; Giles, F.J.; Radich, J.P.; Ross, D.M.; Casares, M.T.G.; Hellmann, A.; Stentoft, J.; Conneally, E.; García-Gutiérrez, V.; et al. Treatment-free remission following frontline nilotinib in patients with chronic myeloid leukemia in chronic phase: Results from the ENESTfreedom study. Leukemia 2017, 31, 1525–1531. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, T.; Nakaseko, C.; Nishiwaki, K.; Yoshida, C.; Ohashi, K.; Takezako, N.; Takano, H.; Kouzai, Y.; Murase, T.; Matsue, K.; et al. Discontinuation of dasatinib after deep molecular response for over 2 years in patients with chronic myelogenous leukemia and the unique profiles of lymphocyte subsets for successful discontinuation: A prospective, multicenter Japanese trial (D-STOP Trial). Blood 2016, 128, 791. [Google Scholar] [CrossRef]
- Hernández-Boluda, J.C.; Pereira, A.; Pastor-Galán, I.; Alvarez-Larrán, A.; Savchuk, A.; Puerta, J.M.; Sánchez-Pina, J.M.; Collado, R.; Díaz-González, A.; Angona, A.; et al. Feasibility of treatment discontinuation in chronic myeloid leukemia in clinical practice: Results from a nationwide series of 236 patients. Blood Cancer J. 2018, 8, 1–8. [Google Scholar] [CrossRef]
- Clark, R.E.; Polydoros, F.; Apperley, J.F.; Milojkovic, D.; Rothwell, K.; Pocock, C. Initial reduction of therapy prior to complete treatment discontinuation in chronic myeloid leukaemia: Final results of the British DESTINY Study. Lancet Haematol. 2019, 6, e375–e383. [Google Scholar] [CrossRef]
- Rousselot, P.; Loiseau, C.; Delord, M.; Cayuela, J.M.; Spentchian, M. Late molecular recurrences in patients with chronic myeloid leukemia experiencing treatment-free remission. Blood Adv. 2020, 4, 3034–3040. [Google Scholar] [CrossRef]
- Legros, L.; Nicolini, F.E.; Etienne, G.; Rousselot, P.; Rea, D.; Giraudier, S.; Guerci-Bresler, A.; Huguet, F.; Gardembas, M.; Escoffre, M.; et al. Second tyrosine kinase inhibitor discontinuation attempt in patients with chronic myeloid leukemia. Cancer 2017, 123, 4403–4410. [Google Scholar] [CrossRef]
- Talpaz, M.; Hehlmann, R.; Quintás-Cardama, A.; Mercer, J.; Cortes, J. Re-emergence of interferon-α in the treatment of chronic myeloid leukemia. Leukemia 2012, 27, 803–812. [Google Scholar] [CrossRef]
- Machova-Polakova, K.; Zizkova, H.; Zuna, J.; Motlova, E.; Hovorkova, L.; Gottschalk, A.; Glauche, I.; Koblihova, J.; Pecherkova, P.; Klamova, H.; et al. Analysis of chronic myeloid leukaemia during deep molecular response by genomic PCR: A traffic light stratification model with impact on treatment-free remission. Leukemia 2020. [Google Scholar] [CrossRef] [PubMed]
- Abruzzese, E.; Trawinska, M.M.; De Fabritiis, P.; Perrotti, A.P. Tyrosine kinase inhibitors and pregnancy. Mediterr. J. Hematol. Infect. Dis. 2014, 6, e2014028. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.E.; Abruzzese, E.; Chelysheva, E.; Guha, M.; Wallis, N.; Apperley, J.F. The impact of dasatinib on pregnancy outcomes. Am. J. Hematol. 2015, 90, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Chelysheva, E.; Aleshin, S.; Polushkina, E.; Shmakov, R.; Shokhin, I.; Chilov, G.; Turkina, A. Breastfeeding in patients with chronic myeloid leukemia: Case series with measurements of drug concentrations in maternal milk and literature review. Mediterr. J. Hematol. Infect. Dis. 2018, 10, e2018027. [Google Scholar] [CrossRef] [PubMed]
- Nicolini, F.-E.; Alcazer, V.; Huguet, F.; Cony-Makhoul, P.; Heiblig, M.; Fort, M.-P.; Morisset, S.; Guerci-Bresler, A.; Soula, V.; Sobh, M.; et al. CML patients show sperm alterations at diagnosis that are not improved with imatinib treatment. Leuk. Res. 2016, 48, 80–83. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| (A) ELTS score calculation. | ||||||
|---|---|---|---|---|---|---|
| Calculation | Definition of Risk Groups | |||||
| 0.0025 × (age/10)3 + 0.0615 × spleen size + 0.1052 × peripheral blood blasts + 0.4104 × (platelet count/1000)−0.5 | Low risk: < 1.5680 Intermediate risk: 1.5680–2.2185 High risk: > 2.2185 | |||||
| (B) Risk strata proportions and outcome. | ||||||
| Low Risk | Intermediate Risk | High Risk | ||||
| n= 5154 | Sokal | ELTS | Sokal | ELTS | Sokal | ELTS |
| % | 38 | 55 | 38 | 28 | 23 | 13 |
| 10-year OS | 89% | 88% | 81% | 79% | 75% | 68% |
| 6-year LRD | 3% | 2% | 4% | 5% | 8% | 12% |
| Optimal | Warning | Failure | |
|---|---|---|---|
| Baseline | NA | High-risk ACA, high-risk ELTS score | NA |
| 3 months | ≤10% | >10% | >10% if confirmed within 1–3 months |
| 6 months | ≤1% | >1–10% | >10% |
| 12 months | ≤0.1% | >0.1–1% | >1% |
| Any time | ≤0.1% | >0.1% loss of ≤ 0.1% (MMR) * | >1%, resistance mutations high-risk ACA |
| Prevention of BC | Effective treatment, elimination of BCR-ABL1 |
| High-risk ACA | Observe closely, intensify treatment |
| AP | Treat as high-risk CML |
| Primary BC | Start with imatinib Assess for allo-SCT, initiate donor search |
| Resistance to 2G-TKI | Ponatinib |
| Failure to ponatinib | Early allo-SCT recommended |
| Progress to BC | Attempt at return to CP2 * For myeloid BC: AML regimens + TKI [53,54] For lymphoid BC: ALL regimens + TKI [55] After CP2: allo-SCT without delay |
| Study | 5 Years (%) | 10 Years (%) | |
|---|---|---|---|
| CML study IV * | Imatinib MR4 | 68 | 81 |
| Imatinib MR4.5 | 53 | 72 | |
| ENESTnd ** | Nilotinib MR4 | 66 | 73 |
| Nilotinib MR4.5 | 54 | 64 | |
| Imatinib MR4 | 42 | 56 | |
| Imatinib MR4.5 | 35 | 45 | |
| Dasision *** | Dasatinib MR4.5 | 42 | NA |
| Imatinib MR4.5 | 33 | NA |
| Study | TKI | Min. Treatment Duration (Years) | n | Depth of MR | Min. Duration of MR (Years) | RFS with at Least MMR | References |
|---|---|---|---|---|---|---|---|
| Euro-SKI | IM | 3 | 755 | MR4 | 1 | 49% at 2 years | Saußele et al., 2018 [58] |
| STIM | IM | 2 | 100 | MR5 | 2 | 37% at 10 years | Etienne et al., 2017 [59] Update at ESH 2019 |
| TWISTER | IM | 3 | 40 | MR4.5 | 2 | 45% at 42 months | Ross et al., 2013 [60] |
| A-STIM | IM | 3 | 80 | UMRD | 2 | 64% at 23 months | Rousselot et al., 2014 [61] |
| KID study | IM | 3 | 126 | MR4.5 | 2 | 58% at 2 years | Lee et al., 2016 [62] Update Zang 2018 ASH a. 4252 [63] |
| STIM2 | IM | 2 | 200 | MR4.5 | 2 | 46% at 2 years | Nicolini et al., 2018 [64] ASH a. 462 |
| ISAV | IM | 2 | 112 | UMRD | 1.5 | 52% at 22 months | Mori et al., 2015 [65] Update at ASH 2018 a. 461 [66] |
| STOP 2G-TKI | Dasa/Nilo | 2 | 60 | MR4.5 | 2 | ca. 55% at 4 years | Rea et al., 2017 [67] |
| DADI | Dasa 2nd line | ND | 63 | MR4 | 1 | 49% at 6 months | Imagawa et al., 2015 [68] |
| NILST | Nilo | 2 | 87 | MR4.5 | 2 | 59% at 1 year | Kadowaki et al., 2016 ASH a. 790 [69] |
| TRAD | IM/Dasa | 3 | 75 | MR4.5 | 2 | 58% at 6 months | Kim et al., 2016 ASH a. 1922 [70] |
| Dasfree | Dasa | 2 | 84 | MR4.5 | 1 | 46% at 2 years | Shah et al., 2019 [71] Update at ESH 2019 |
| ENESTop | Nilo 2nd line | 3 | 126 | MR4.5 | 1 | 58% at 4 years | Hughes et al., 2016 ASH a. 792 [72] |
| STAT2 | IM/Nilo | 2 | 96 | MR4.5 | 2 | 68% at 1 year | Takahashi et al., 2018 [73] |
| ENESTfreedom | Nilo | 2 | 190 | MR4.5 | 1 | 52% at 4 years | Hochhaus et al., 2017 [74] |
| D-STOP | IM/Dasa | ND | 54 | MR4 | 2 | 63% at 1 year | Kumagai et al., 2016 ASH a. 791 [75] |
| Spanish study | IM/Nilo/Dasa | 3 | 236 | MR4.5 | 2 | 64% at 4 years | Boluda et al., 2018 ASH a. 47 [76] |
| DESTINY | IM/Nilo/Dasa | 6.9 (median) | 125 | MR4 | 3 | 72% at 3 years | Clark et al., 2019 [77] |
| Routine Care | TKI | 7.1 | 128 | MR4 | 4 | 67% at 2.9 years | Rousselot et al., 2020 [78] |
| Swedish CML-Registry | TKI (53% IM) | 7.7 | 131 | DMR | 2.9 (median) | 61% outside, 35% inside a study at 2 years | Richter, ESH 2020 |
| RE-STIM | (2nd stop) | 3.1 (median) | 106 | MR4.5 | 1.7 (median) | 33% at 4 years | Legros et al., 2017 [79] Update at EHA 2019 |
| Total: 21 | 2974 | 33–72% at 0.5–10 years | |||||
| Mandatory | CML in first CP only (data are lacking outside this setting) |
| Motivated patient with structured communication | |
| Access to high-quality quantitative PCR using the International Scale (IS), with rapid turn-around of PCR test results | |
| Patient’s agreement to more frequent monitoring after stopping treatment. This means monthly for the first 6 months, every 2 months for months 6–12, and every 3 months thereafter | |
| Minimal (stop allowed) | First-line therapy or second-line, if intolerance was the only reason for changing TKI |
| Typical e13a2 or e14a2 BCR-ABL1 transcripts | |
| Duration of TKI therapy > 5 years (>4 years for 2G-TKI) | |
| Duration of DMR (MR4 or better) > 2 years | |
| No prior treatment failure | |
| Optimal (stop recommended for consideration) | Duration of TKI therapy > 5 years |
| Duration of DMR > 3 years if MR4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hehlmann, R. The New ELN Recommendations for Treating CML. J. Clin. Med. 2020, 9, 3671. https://doi.org/10.3390/jcm9113671
Hehlmann R. The New ELN Recommendations for Treating CML. Journal of Clinical Medicine. 2020; 9(11):3671. https://doi.org/10.3390/jcm9113671
Chicago/Turabian StyleHehlmann, Rüdiger. 2020. "The New ELN Recommendations for Treating CML" Journal of Clinical Medicine 9, no. 11: 3671. https://doi.org/10.3390/jcm9113671
APA StyleHehlmann, R. (2020). The New ELN Recommendations for Treating CML. Journal of Clinical Medicine, 9(11), 3671. https://doi.org/10.3390/jcm9113671