The Role of COVID-19 in the Death of SARS-CoV-2–Positive Patients: A Study Based on Death Certificates

 , , ,
, , , 
Abstract
1. Introduction
2. Experimental Section
Ethical Issues
3. Results
3.1. Deaths Due to COVID-19
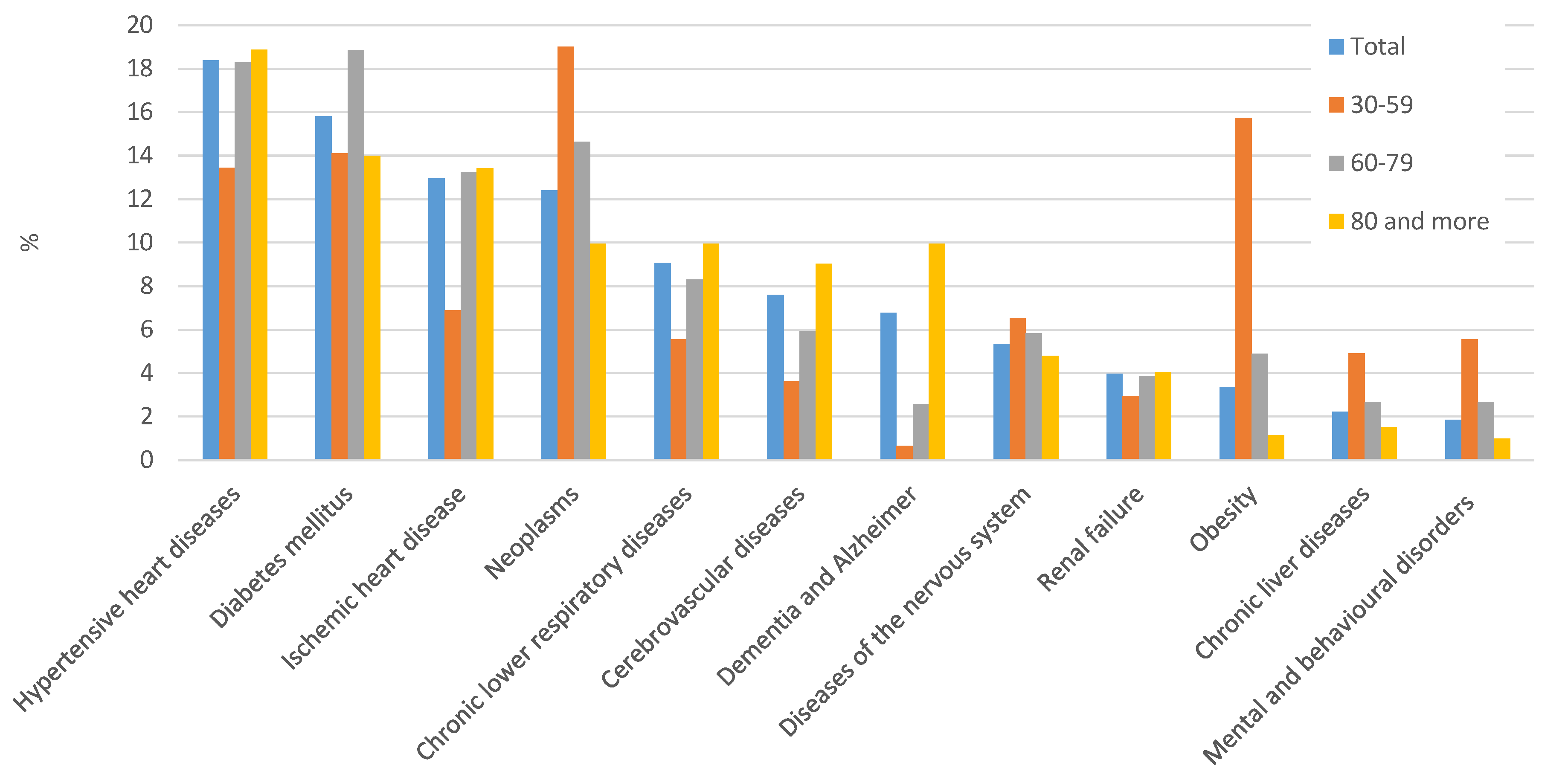
3.2. Comorbidities
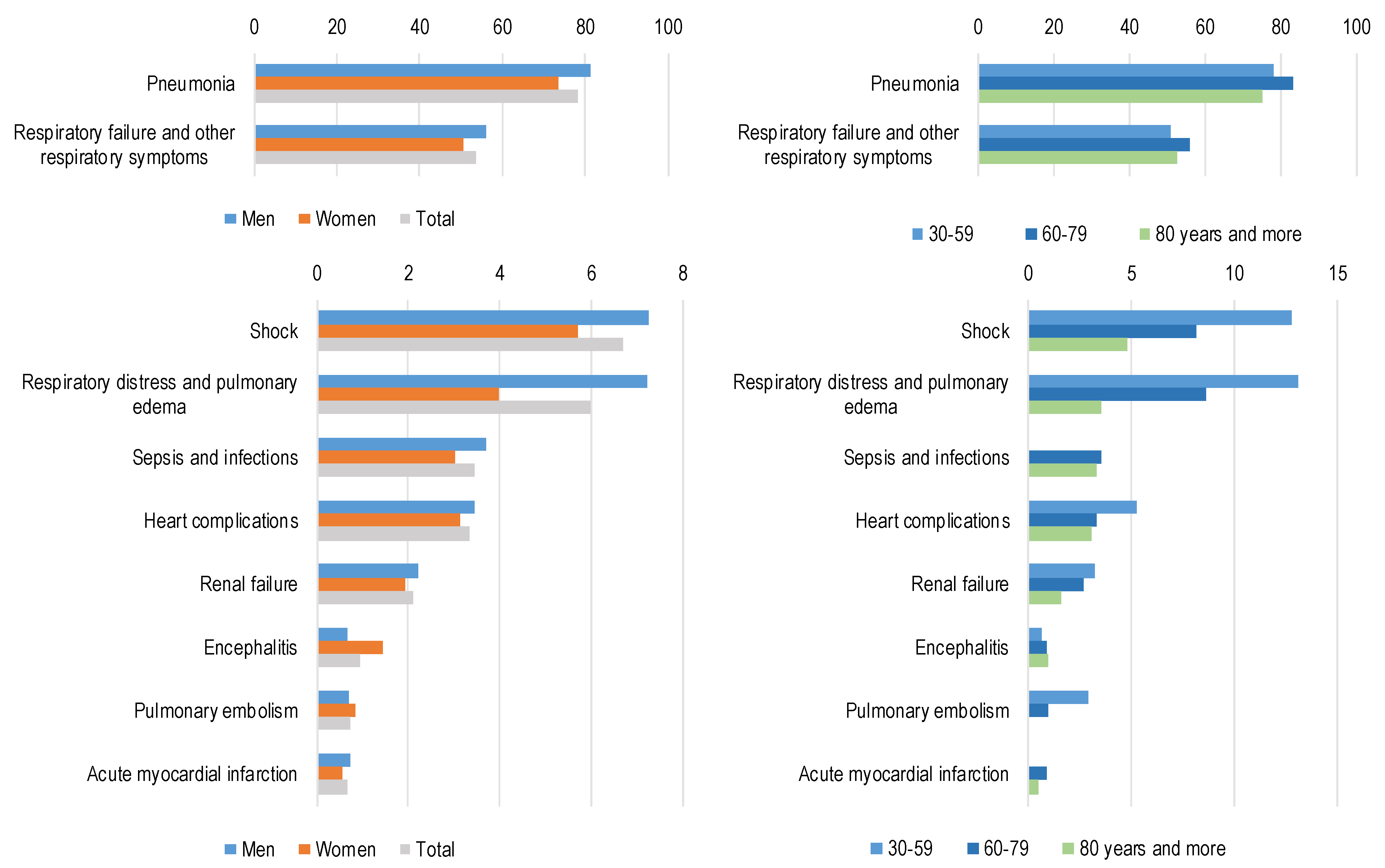
3.3. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Procedure for the Selection of Comorbidities
Appendix A.2. Detailed Description
- -
- “originating cause”—the originating causes of the sequences reported on the death certificate. If there is a single sequence.
- -
- “precipitating condition”—a code that can be considered a complication of another on the death certificate.
- -
- “associated cause”—the independent codes in Part 2.
- -
- “ill-defined codes”—codes at the origin of a sequence or reported as associated causes that are considered ill-defined by the ICD-10.
- -
- “deleted codes”—it is possible that during the process, two or more codes are condensed together in a single code; those codes including others are marked as “deleted”.
- (1)
- All codes in Part 1 are initially marked as “originating”, and all codes in Part 2 are marked as “associated cause”.
- (2)
- Check for “due to” relation in Part 1: starting from line a to line f, each code is compared with any other in lower lines, if the first code can be due to the second (according to Iris Decision Tables), the first code will be identified as “precipitating condition”.
- (3)
- Check for obvious causes: if any “originating” code is an obvious consequence (according to Iris Decision Tables) of another code, then the first code is marked as “precipitating” and the second as “originating”.
- (4)
- Check for Ill-defined causes, if an “originating” code is an ill-defined condition (the list of ill-defined codes is provided by ICD-10 and included in Iris Decision Tables), the code will be marked as “ill-defined”.
- (5)
- Check for linkages: if two or more codes are linked together (according to Iris Decision Tables), the first code is marked as “deleted” and the second is preferred (and sometimes modified).
- (6)
- Check for specificity: if one code is considered less specific than another (according to Iris Decision Tables), the first code is marked as “deleted” and the second is preferred (and sometimes modified).
Appendix B
Appendix B.1. Selection of Complications
Appendix B.1.1. Example 1
- P1
- a. Respiratory failure;b. Pneumonia;c. COVID-19.
Appendix B.1.2. Example 2
- P1
- a. Respiratory failure;b. Pneumonia.
- P2
- COVID-19.
Appendix B.1.3. Example 3
- P1
- a. Liver failure;b. Liver metastasis;c. Lung cancer, positive to SARS-CoV-2 (by swamp).

{kind=link}
{kind=link}
{kind=link}
| Observed | Expected | |
|---|---|---|
| Frequency of condition c reported as “due to” COVID-19 (in a line of Part 1 above the line where COVID-19 is reported) | Dtc | ½ Fc |
| Frequency of condition c reported as “cause of” COVID-19 (in a line of Part 1 below the line where COVID-19 is reported) | Coc | ½ Fc |
| Total frequency of the condition c reported in Part 1 together with COVID-19 but in a different line | Fc | Fc |
| ICD10 | (Fc) Observed Total in “Due to” or “Cause of” with COVID-19 (A) | (Dtc) Observed in Due to Position | (½ Fc) Expected in Due to (=1/2 A) | Chi-Square Value | Total Number Considered as Complication of COVID-19: Due to and Obvious Consequence | ||
|---|---|---|---|---|---|---|---|
| N | N | N | |||||
| A00-A09 | Intestinal infections | 6 | 3 | 3 | 0.0 | 3 | |
| A00-B99 | Some infectious diseases | 12 | 6 | 6 | 0.0 | 6 | |
| A40-A41, A49, B34, B37, B44, B99 | Sepsis and bacterial infections of unspecified site | 144 | 120 | 72 | 64.0 * | 187 | |
| C00-D48 | Neoplasms | 140 | 19 | 70 | 74.3 § | 25 | |
| D50-D99 | Diseases of blood and blood forming organs | 27 | 13 | 13.5 | 0.0 | 13 | |
| E10-E14 | Endocrine diseases | 67 | 13 | 33.5 | 25.1 § | 13 | |
| E40-E46 | Nutritional disorders | 2 | 2 | 1 | 0.0 | 2 | |
| E66 | Obesity | 12 | 2 | 6 | 5.3 § | 2 | |
| E70-E90 | Other diseases of the metabolism | 33 | 25 | 16.5 | 8.8 * | 26 | |
| F00-F99 | Mental and behavioural disorders | 73 | 13 | 36.5 | 30.3 § | 13 | |
| G00-H99 | other diseases of the nervous system | 58 | 8 | 29 | 30.4 § | 8 | |
| G04, G93 | Encephalitis, myelitis and encephalomyelitis | 46 | 39 | 23 | 22.3 * | 51 | |
| I00-I09, I27-I45, I47, I52 | Specified cardiac diseases | 36 | 20 | 18 | 0.4 | 21 | |
| I10-I5 | Hypertensive heart diseases | 73 | 13 | 36.5 | 30.3 * | 12 | |
| I20-I24 | Myocardial infarction | 47 | 35 | 23.5 | 11.3 * | 35 | |
| I25 | Chronic ischaemic heart disease | 76 | 22 | 38 | 13.5 § | 22 | |
| I26 | Pulmonary embolism | 31 | 28 | 15.5 | 20.2 * | 40 | |
| I70-I79, I83-I89, I95-I99 | Other circulatory diseases | 40 | 21 | 20 | 0.1 | 21 | |
| I46 | Cardiac arrest | 713 | 698 | 356.5 | 654.3 * | 698 | |
| I48-I49 | Atrial fibrillation and other arrhythmias | 59 | 29 | 29.5 | 0.0 | 29 | |
| I50-I51 | Heart complications (heart failure and unspecified cardiac disease) | 242 | 177 | 121 | 51.8 * | 183 | |
| I60-I64 | Acute cerebrovascular accidents | 48 | 20 | 24 | 1.3 | 31 | |
| I80-I82 | Phlebitis, thrombophlebitis and thrombosis of peripheral vessels | 7 | 7 | 3.5 | 0.0 | 7 | |
| J00-J99 | Other respiratory diseases | 98 | 32 | 49 | 11.8 § | 43 | |
| J12-J18, J84, J98 | Pneumonia | 1277 | 1198 | 638.5 | 980.5 * | 4207 | |
| J80-J81 | ARDS and pulmonary oedema | 278 | 273 | 139 | 258.4 * | 318 | |
| J96, R04, R06, R09 | Respiratory failure and related symptoms | 2952 | 2824 | 1476 | 2462.2 * | 3007 | |
| Tutte le altre intestinali | Other diseases of digestive system | 18 | 10 | 9 | 0.2 | 15 | |
| K50-K67 | Other diseases of intestine and peritoneum | 17 | 4 | 8.5 | 4.8 § | 4 | |
| K70-K77 | Chronic liver diseases | 21 | 11 | 10.5 | 0.0 | 11 | |
| M00-M99 | Diseases of the musculoskeletal system and connective tissue | 10 | 3 | 5 | 1.6 | 3 | |
| N00, N04, N17, N19 | Kidney failure | 142 | 112 | 71 | 47.4 * | 112 | |
| N00-N99 | Other diseases of the genitourinary system | 44 | 15 | 22 | 4.5 § | 15 | |
| R57 | Shock | 319 | 311 | 159.5 | 287.8 * | 364 | |
| S00-T98, V01-Y98 | External causes | 55 | 14 | 27.5 | 13.3 § | 59 |
Appendix C. Age and Gender Distribution of Death Certificates

References
- Riccardo, F.; Ajelli, M.; Andrianou, X.D.; Bella, A.; Del Manso, M.; Fabiani, M.; Bellino, S.; Boros, S.; Urdiales, A.M.; Marziano, V.; et al. Epidemiological characteristics of COVID-19 cases in Italy and estimates of the reproductive numbers one month into the epidemic. medRxiv 2020. preprint. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, L.; Vanacore, N.; Donfrancesco, C.; Lo Noce, C.; Canevelli, M.; Punzo, O.; Raparelli, V.; Pezzotti, P.; Riccardo, F.; Bella, A.; et al. Clinical characteristics of hospitalized individuals dying with COVID-19 by age group in Italy. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1796–1800. [Google Scholar] [CrossRef] [PubMed]
- ONS. Measuring Pre-Existing Health Conditions in Death Certification—Deaths Involving COVID-19: March 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/methodologies/measuringpreexistinghealthconditionsindeathcertificationdeathsinvolvingcovid19march2020 (accessed on 27 August 2020).
- WHO. International Classification of Diseases and Related Health Problems, 5th ed.; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Iss, Istat, Inail. Rapporto ad Interim su Definizione, Certificazione e Classificazione Delle Cause di Morte. Versione dell’8 Giugno 2020, ISS COVID-19 n. 49/2020. Available online: https://www.iss.it/documents/20126/0/Rapporto+ISS+COVID-19++49_2020+%281%29.pdf/9378da12-76ae-f51f-9666-14c7c2078a17?t=1592583825077 (accessed on 27 August 2020).
- Grippo, F.; Désesquelles, A.; Pappagallo, M.; Frova, L.; Egidi, V.; Meslé, F. Multi-morbidity and frailty at death: A new classification of death records for an aging world. Popul. Stud. 2019, in press. [Google Scholar]
- Available online: https://www.gazzettaufficiale.it/eli/id/2020/02/28/20A01348/SG (accessed on 27 August 2020).
- Agrawal, H.; Das, N.; Nathani, S.; Saha, S.; Saini, S.; Kakar, S.S.; Roy, P. An assessment on impact of COVID-19 infection in a gender specific manner. Stem Cell Rev. Rep. 2020, 838, 3. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.N. Coding and classifying causes of death: Trends and international differences. In International Handbook of Adult Mortality; Rogers, R.G., Crimmins, E.M., Eds.; Springer: Dordrech, The Netherlands, 2011; pp. 467–489. [Google Scholar]
- Dietz, W.; Santos-Burgoa, C. Obesity and its implications for COVID-19 mortality. Obesity 2020, 28, 1005. [Google Scholar] [CrossRef] [PubMed]
- Onder, G.; Palmieri, L.; Vanacore, N.; Giuliano, M.; Brusaferro, S.; Italian National Institute of Health COVID-19 mortality group. Non-respiratory complications and obesity in patients dying with COVID-19 in Italy. Obesity 2020. [Google Scholar] [CrossRef]


| ICD-10 | Underlying Cause of Death | Whole Sample | Gender | Age Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Men | Women | 30–59 | 60–79 | 80 and Older | |||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | ||
| U07.1 | COVID-19 | 4691 | 88.3 | 2950 | 89.4 | 1737 | 86.5 | 263 | 86.2 | 1754 | 90.4 | 2590 | 87.3 |
| A00-B99 | Infectious and parasitic diseases | 12 | 0.2 | 7 | 0.2 | 5 | 0.2 | 0 | 0.0 | 4 | 0.2 | 6 | 0.2 |
| C00-D48 | Neoplasms | 137 | 2.6 | 87 | 2.6 | 50 | 2.5 | 21 | 6.9 | 54 | 2.8 | 57 | 1.9 |
| E00-E99 | Endocrine, nutritional and metabolic diseases | 46 | 0.9 | 28 | 0.8 | 18 | 0.9 | 7 | 2.3 | 13 | 0.7 | 25 | 0.8 |
| of which | |||||||||||||
| E10-E14 | Diabetes | 37 | 0.7 | 22 | 0.7 | 15 | 0.7 | 6 | 2.0 | 11 | 0.6 | 19 | 0.6 |
| F01-F03, G30 | Dementia and Alzheimer | 38 | 0.7 | 13 | 0.4 | 25 | 1.2 | 0 | 0.0 | 3 | 0.2 | 35 | 1.2 |
| G00-H99 | Diseases of the nervous system (excluding Alzheimer) | 15 | 0.3 | 12 | 0.4 | 3 | 0.1 | 0 | 0.0 | 8 | 0.4 | 7 | 0.2 |
| I00-I99 | Diseases of the circulatory system | 235 | 4.4 | 131 | 4.0 | 104 | 5.2 | 8 | 2.6 | 61 | 3.1 | 161 | 5.4 |
| of which | |||||||||||||
| I10-I15 | Hypertensive diseases | 40 | 0.8 | 16 | 0.5 | 24 | 1.2 | 1 | 0.3 | 8 | 0.4 | 28 | 0.9 |
| I20-I25 | Ischaemic heart diseases | 87 | 1.6 | 58 | 1.8 | 29 | 1.4 | 1 | 0.3 | 33 | 1.7 | 52 | 1.8 |
| I48 | Atrial fibrillation | 12 | 0.2 | 5 | 0.2 | 7 | 0.3 | 0 | 0.0 | 2 | 0.1 | 10 | 0.3 |
| I60-I69 | Cerebrovascular diseases | 55 | 1.0 | 29 | 0.9 | 26 | 1.3 | 2 | 0.7 | 11 | 0.6 | 41 | 1.4 |
| J00-J99 | Diseases of the respiratory system | 58 | 1.1 | 33 | 1.0 | 25 | 1.2 | 0 | 0.0 | 18 | 0.9 | 39 | 1.3 |
| of which | |||||||||||||
| J40-J47 | Chronic lower-respiratory diseases | 55 | 1.0 | 33 | 1.0 | 22 | 1.1 | 0 | 0.0 | 17 | 0.9 | 37 | 1.2 |
| K00-K99 | Diseases of the digestive system | 36 | 0.7 | 18 | 0.5 | 18 | 0.9 | 2 | 0.7 | 15 | 0.8 | 17 | 0.6 |
| S00-T98 | External causes of death | 26 | 0.5 | 12 | 0.4 | 14 | 0.7 | 1 | 0.3 | 6 | 0.3 | 18 | 0.6 |
| Other causes | 28 | 0.6 | 13 | 0.4 | 15 | 0.7 | 4 | 1.3 | 9 | 0.5 | 15 | 0.5 | |
| Total | 5311 | 100.0 | 3298 | 100.0 | 2009 | 100.0 | 305 | 100.0 | 1940 | 100.0 | 2966 | 100.0 | |
| Number of Comorbidities Besides COVID-19 | Total | Gender | Age Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Men | Women | 30–59 | 60–79 | 80 and More | ||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | |
| None | 1469 | 27.7 | 911 | 27.6 | 554 | 27.6 | 80 | 26.2 | 550 | 28.4 | 819 | 27.6 |
| at least 1 | 3842 | 72.3 | 2387 | 72.4 | 1455 | 72.4 | 225 | 73.8 | 1390 | 71.6 | 2147 | 72.4 |
| of which: | ||||||||||||
| 1 | 1699 | 32.0 | 1059 | 32.1 | 640 | 31.9 | 124 | 40.7 | 621 | 32.0 | 920 | 31.0 |
| 2 | 1422 | 26.8 | 866 | 26.3 | 556 | 27.7 | 66 | 21.6 | 494 | 25.5 | 841 | 28.4 |
| 3 or more | 721 | 13.6 | 462 | 14.0 | 259 | 12.9 | 35 | 11.5 | 275 | 14.2 | 386 | 13.0 |
| Total | 5311 | 100.0 | 3298 | 100.0 | 2009 | 100.0 | 305 | 100.0 | 1940 | 100.0 | 2966 | 100.0 |
| Mean number | 1.3 | 1.3 | 1.3 | 1.2 | 1.3 | 1.3 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grippo, F.; Navarra, S.; Orsi, C.; Manno, V.; Grande, E.; Crialesi, R.; Frova, L.; Marchetti, S.; Pappagallo, M.; Simeoni, S.; et al. The Role of COVID-19 in the Death of SARS-CoV-2–Positive Patients: A Study Based on Death Certificates. J. Clin. Med. 2020, 9, 3459. https://doi.org/10.3390/jcm9113459
Grippo F, Navarra S, Orsi C, Manno V, Grande E, Crialesi R, Frova L, Marchetti S, Pappagallo M, Simeoni S, et al. The Role of COVID-19 in the Death of SARS-CoV-2–Positive Patients: A Study Based on Death Certificates. Journal of Clinical Medicine. 2020; 9(11):3459. https://doi.org/10.3390/jcm9113459
Chicago/Turabian StyleGrippo, Francesco, Simone Navarra, Chiara Orsi, Valerio Manno, Enrico Grande, Roberta Crialesi, Luisa Frova, Stefano Marchetti, Marilena Pappagallo, Silvia Simeoni, and et al. 2020. "The Role of COVID-19 in the Death of SARS-CoV-2–Positive Patients: A Study Based on Death Certificates" Journal of Clinical Medicine 9, no. 11: 3459. https://doi.org/10.3390/jcm9113459
APA StyleGrippo, F., Navarra, S., Orsi, C., Manno, V., Grande, E., Crialesi, R., Frova, L., Marchetti, S., Pappagallo, M., Simeoni, S., Di Pasquale, L., Carinci, A., Donfrancesco, C., Lo Noce, C., Palmieri, L., Onder, G., Minelli, G., & Group, I. N. I. o. H. C.-1. M. (2020). The Role of COVID-19 in the Death of SARS-CoV-2–Positive Patients: A Study Based on Death Certificates. Journal of Clinical Medicine, 9(11), 3459. https://doi.org/10.3390/jcm9113459