Anterior Scleral Regional Variation between Asian and Caucasian Populations



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Exportation and Processing
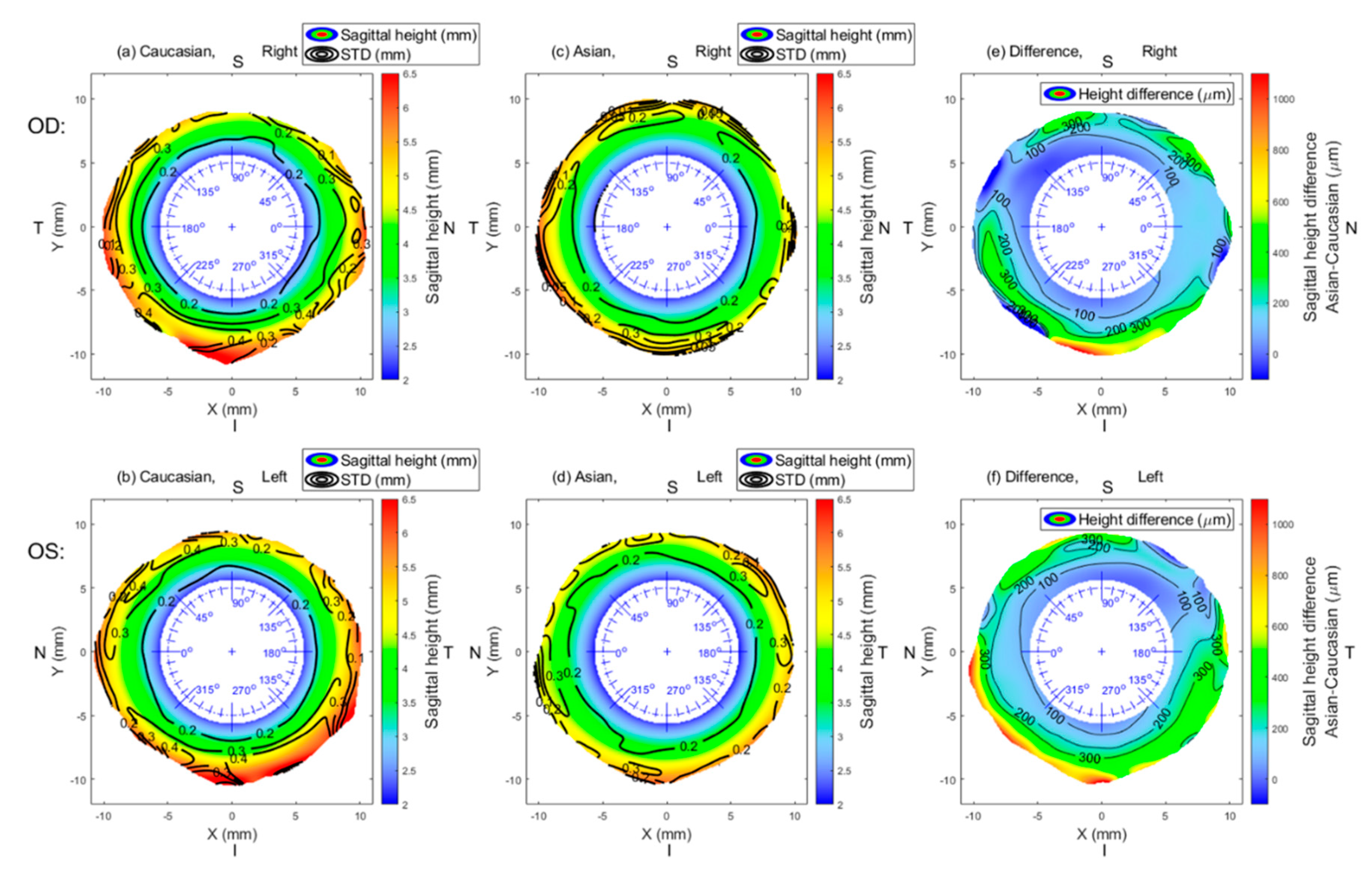
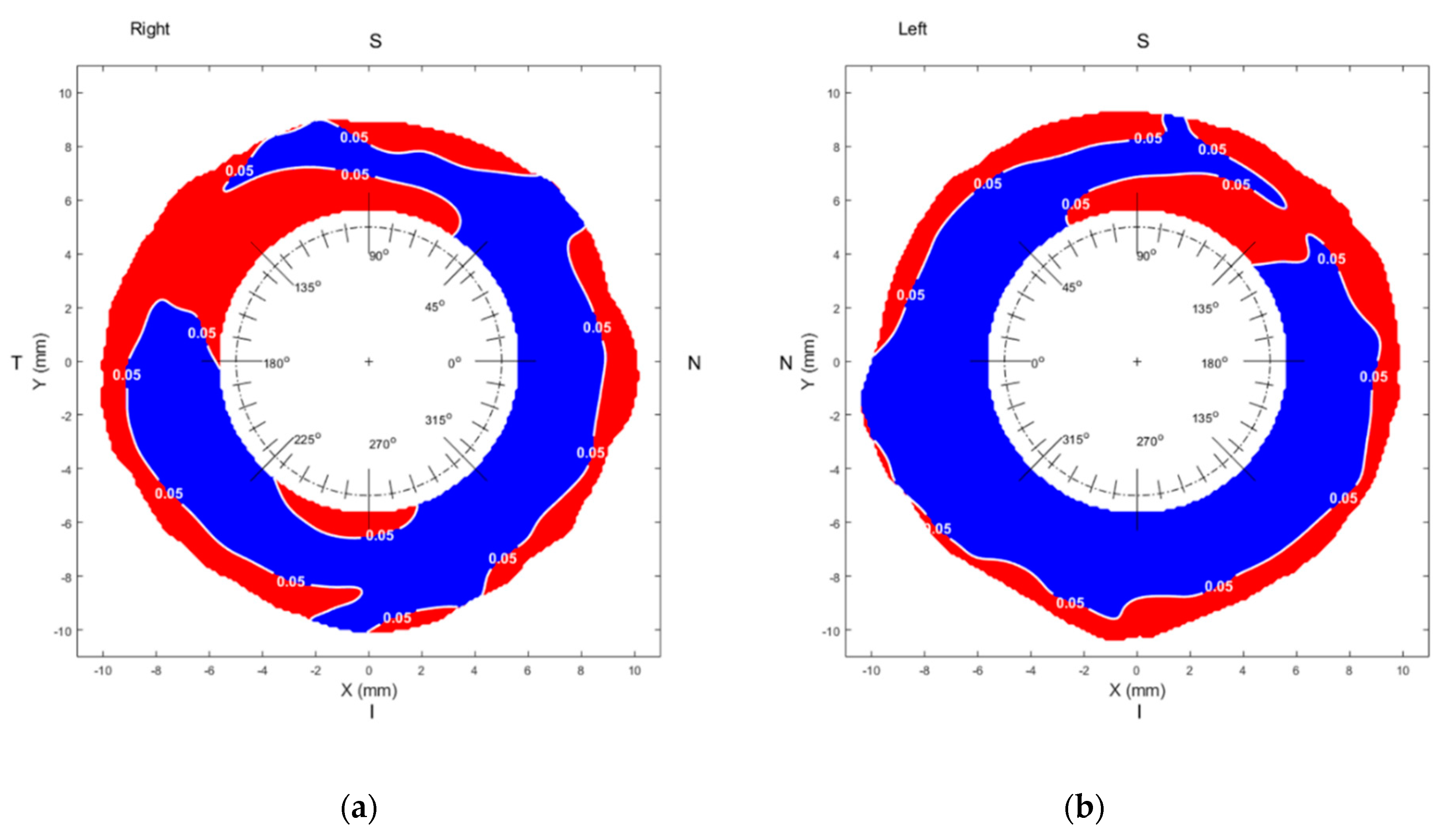
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Efron, N.; Morgan, P.B.; Woods, C.A.; International Contact Lens Prescribing Survey Consortium. An international survey of daily disposable contact lens prescribing. Clin. Exp. Optom. 2013, 96, 58–64. [Google Scholar] [CrossRef]
- Haddad, M.F.; Bakkar, M.; Gammoh, Y.; Morgan, P. Trends of contact lens prescribing in Jordan. Contact Lens Anterior Eye 2016, 39, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Efron, N.; Morgan, P.B.; Woods, C.A. International survey of contact lens prescribing for extended wear. Optom. Vis. Sci. 2012, 89, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Itoi, M.; Itoi, M.; Efron, N.; Morgan, P.; Woods, C. Trends in Contact Lens Prescribing in Japan (2003–2016). Contact Lens Anterior Eye 2018, 41, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Vincent, S.J. The rigid lens renaissance: A surge in sclerals. Contact Lens Anterior Eye 2018, 41, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Woods, C.A.; Efron, N.; Morgan, P. Are eye-care practitioners fitting scleral contact lenses? Clin. Exp. Optom. 2020, 103, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Consejo, A.; Llorens-Quintana, C.; Bartuzel, M.M.; Iskander, D.R.; Rozema, J.J. Rotation asymmetry of the human sclera. Acta Ophthalmol. 2018, 97. [Google Scholar] [CrossRef]
- Ritzmann, M.; Caroline, P.J.; Borret, R.; Korszen, E. An analysis of anterior scleral shape and its role in the design and fitting of scleral contact lenses. Contact Lens Anterior Eye 2018, 41, 205–213. [Google Scholar] [CrossRef]
- DeNaeyer, G.; Sanders, D.; van der Worp, E.; Jedlicka, J.; Michaud, L.; Morrison, S. Qualitative Assessment of Scleral Shape Patterns Using a New Wide Field Ocular Surface Elevation Topographer. J. Contact Lens Res. Sci. 2017, 1, 12–22. [Google Scholar] [CrossRef]
- Van Nuffel, S.; Consejo, A.; Koppen, C.; Kreps, E.O. The corneoscleral shape in keratoconus patients with and without specialty lens wear. Contact Lens Anterior Eye 2020. [Google Scholar] [CrossRef]
- Alonso-Caneiro, D.; Vincent, S.J.; Collins, M.J. Morphological changes in the conjunctiva, episclera and sclera following short-term miniscleral contact lens wear in rigid lens neophytes. Contact Lens Anterior Eye 2016, 39, 53–61. [Google Scholar] [CrossRef]
- Consejo, A.; Bartuzel, M.M.; Iskander, D.R. Corneo-scleral limbal changes following short-term soft contact lens wear. Contact Lens Anterior Eye 2017, 40, 293–300. [Google Scholar] [CrossRef]
- Consejo, A.; Behaegel, J.; Van Hoey, M.; Wolffsohn, J.S.; Rozema, J.J.; Iskander, D.R. Anterior eye surface changes following miniscleral contact lens wear. Contact Lens Anterior Eye 2019, 42, 70–74. [Google Scholar] [CrossRef]
- Walker, M.K.; Schornack, M.M.; Vincent, S.J. Anatomical and physiological considerations in scleral lens wear: Conjunctiva and sclera. Contact Lens Anterior Eye 2020. [Google Scholar] [CrossRef] [PubMed]
- Hickson-Curran, S.; Young, G.; Brennan, N.; Hunt, C. Chinese and Caucasian ocular topography and soft contact lens fit. Clin. Exp. Optom. 2016, 99, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Guillon, M.; Dumbleton, K.; Theodoratos, P.; Patel, T.; Karkkainen, T.; Moody, K. Objective Assessment of Ocular Surface Response to Contact Lens Wear in Presbyopic Contact Lens Wearers of Asian Descent. Eye Contact Lens 2018, 44, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Vincent, S.J.; Alonso-Caneiro, D.; Collins, M.J. Miniscleral lens wear influences corneal curvature and optics. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. 2016, 36, 100–111. [Google Scholar] [CrossRef]
- Chan, S.M.; Svitova, T.F.; Lin, M.C. Accounting for Ethnicity-Related Differences in Ocular Surface Integrity as a Step toward Understanding Contact Lens Discomfort. Eye Contact Lens 2017, 43, 23–31. [Google Scholar] [CrossRef]
- Patel, S.; Virhia, S.K.; Farrell, P. Stability of the precorneal tear film in Chinese, African, Indian, and Caucasian eyes. Optom. Vis. Sci. 1995, 72, 911–915. [Google Scholar] [CrossRef] [PubMed]
- Cho, P.; Brown, B. Review of the tear break-up time and a closer look at the tear break-up time of Hong Kong Chinese. Optom. Vis. Sci. 1993, 70, 30–38. [Google Scholar] [CrossRef]
- Abass, A.; Vinciguerra, R.; Lopes, B.T.; Bao, F.; Vinciguerra, P.; Ambrósio, R.; Elsheikh, A. Positions of Ocular Geometrical and Visual Axes in Brazilian, Chinese and Italian Populations. Curr. Eye Res. 2018, 43, 1404–1414. [Google Scholar] [CrossRef]
- Blake, C.R.; Lai, W.W.; Edward, D.P. Racial and ethnic differences in ocular anatomy. Int. Ophthalmol. Clin. 2003, 43, 9–25. [Google Scholar] [CrossRef] [PubMed]
- Hickson-Curran, S.; Brennan, N.A.; Igarashi, Y.; Young, G. Comparative evaluation of Asian and white ocular topography. Optom. Vis. Sci. 2014, 91, 1396–1405. [Google Scholar] [CrossRef] [PubMed]
- Qin, B.; Tang, M.; Li, Y.; Zhang, X.; Chu, R.; Huang, D. Anterior Segment Dimensions in Asian and Caucasian Eyes Measured by Optical Coherence Tomography. Ophthalmic Surg. Lasers Imaging Retin. 2012, 43, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Consejo, A.; Llorens-Quintana, C.; Radhakrishnan, H.; Iskander, D.R. Mean shape of the human limbus. J. Cataract Refract. Surg. 2017, 43, 667–672. [Google Scholar] [CrossRef]
- Abass, A.; Lopes, B.T.; Eliasy, A.; Wu, R.; Jones, S.; Clamp, J.; Ambrósio, R., Jr.; Elsheikh, A. Three-dimensional non-parametric method for limbus detection. PLoS ONE 2018, 13, e0207710. [Google Scholar] [CrossRef]
- Consejo, A.; Radhakrishnan, H.; Iskander, D.R. Scleral changes with accommodation. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. 2017, 37, 263–274. [Google Scholar] [CrossRef]
- Abass, A.; Lopes, B.T.; Eliasy, A.; Salomao, M.; Wu, R.; White, L.; Jones, S.; Clamp, J.; Ambrósio, R., Jr.; Elsheikh, A. Artefact-free topography based scleral-asymmetry. PLoS ONE 2019, 14, e0219789. [Google Scholar] [CrossRef]
- Iskander, D.R.; Wachel, P.; Simpson, P.N.; Consejo, A.; Jesus, D.A. Principles of operation, accuracy and precision of an Eye Surface Profiler. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. 2016, 36, 266–278. [Google Scholar] [CrossRef]
- Applegate, R.A.; Thibos, L.N.; Twa, M.D.; Sarver, E.J. Importance of fixation, pupil center, and reference axis in ocular wavefront sensing, videokeratography, and retinal image quality. J. Cataract Refract. Surg. 2009, 35, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Kolb, H.F.E.; Nelson, R. Facts and Figures Concerning the Human Retina; University of Utah Health Sciences Center: Salt Lake City, UT, USA, 1995. [Google Scholar]
- Gross, H. Handbook of Optical Systems; Wiley-VCH: Weinheim, Germany, 2005; Volume 4. [Google Scholar]
- Arvo, J. Fast random rotation matrices. In Graphics Gems III; David, K., Ed.; Academic Press Professional, Inc.: Cambridge, MA, USA, 1992; pp. 117–120. [Google Scholar]
- Choi, H.J.; Lee, S.-M.; Lee, J.Y.; Lee, S.Y.; Kim, M.K.; Wee, W.R. Measurement of Anterior Scleral Curvature Using Anterior Segment OCT. Optom. Vis. Sci. 2014, 91, 793–802. [Google Scholar] [CrossRef] [PubMed]
- Kasahara, M.; Shoji, N.; Morita, T.; Shimizu, K. Comparative optical coherence tomography study of differences in scleral shape between the superonasal and superotemporal quadrants. Jpn. J. Ophthalmol. 2014, 58, 396–401. [Google Scholar] [CrossRef]
- Bandlitz, S.; Baumer, J.; Conrad, U.; Wolffsohn, J. Scleral topography analysed by optical coherence tomography. Contact Lens Anterior Eye 2017, 40, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.; Lemke, B.N.; Dortzbach, R.K.; Park, Y.G.; Kang, H.K. The Asian upper eyelid: An anatomical study with comparison to the Caucasian eyelid. Arch. Ophthalmol. 1999, 117, 907–912. [Google Scholar] [CrossRef]
- Most, S.P.; Mobley, S.R.; Larrabee, W.F., Jr. Anatomy of the eyelids. Facial Plast. Surg. Clin. North Am. 2005, 13, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.J.; Collins, M.J.; Davis, B.A.; Carney, L.G. Eyelid pressure and contact with the ocular surface. Investig. Ophthalmol. Vis. Sci. 2010, 51, 1911–1917. [Google Scholar] [CrossRef] [PubMed]
- Song, W.C.; Kim, S.J.; Kim, S.H.; Hu, K.S.; Kim, H.J.; Koh, K.S. Asymmetry of the palpebral fissure and upper eyelid crease in Koreans. J. Plast. Reconstr. Aesthetic Surg. 2007, 60, 251–255. [Google Scholar] [CrossRef]
- Lam, B.L.; Lam, S.; Walls, R.C. Prevalence of Palpebral Fissure Asymmetry in White Persons. Am. J. Ophthalmol. 1995, 120, 518–522. [Google Scholar] [CrossRef]
- McCurdy, J.A., Jr. Upper blepharoplasty in the Asian patient: The “double eyelid” operation. Facial Plast. Surg. Clin. North Am. 2005, 13, 47–64. [Google Scholar] [CrossRef]
- Consejo, A.; Rozema, J.J. In vivo anterior scleral morphometry, axial length and myopia. Contact Lens Anterior Eye 2020, 43, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Niyazmand, H.; Read, S.A.; Atchison, D.A.; Collins, M.J. Anterior eye shape in emmetropes, low to moderate myopes, and high myopes. Contact Lens Anterior Eye 2020. [Google Scholar] [CrossRef] [PubMed]
- Zhao, K.K.; Yang, Y.; Wang, H.; Li, L.; Wang, Z.Y.; Jiang, F.; Qu, J.F. Axial length/corneal radius of curvature ratio and refractive development evaluation in 3- to 4-year-old children: The Shanghai Pudong Eye Study. Int. J. Ophthalmol. 2019, 12, 1021–1026. [Google Scholar] [CrossRef]
- Lam, C.S.; Goh, W.S. The incidence of refractive errors among school children in Hong Kong and its relationship with the optical components. Clin. Exp. Optom. 1991, 74, 97–103. [Google Scholar] [CrossRef]
- Congdon, N.G.; Youlin, Q.; Quigley, H.; Hung, P.T.; Wang, T.H.; Ho, T.C.; Tielsch, J.M. Biometry and primary angle-closure glaucoma among Chinese, white, and black populations. Ophthalmology 1997, 104, 1489–1495. [Google Scholar] [CrossRef]
- Garaszczuk, I.K.; Iskander, D.R. Qualitative assessment of tear dynamics with fluorescein profilometry. Contact Lens Anterior Eye 2017, 40, 208–212. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Q.; Xiang, M.; Zou, H.; Liu, B.; Zhou, H.; Han, Z.; Fu, Z.; Zhang, Z.; Wang, H. Bulbar Conjunctival Thickness Measurements with Optical Coherence Tomography in Healthy Chinese Subjects. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4705–4709. [Google Scholar] [CrossRef]
- Walker, M.K.; Bergmanson, J.P.; Miller, W.L.; Marsack, J.D.; Johnson, L.A. Complications and fitting challenges associated with scleral contact lenses: A review. Contact Lens Anterior Eye 2016, 39, 88–96. [Google Scholar] [CrossRef]
- Kowalski, L.P.; Collins, M.J.; Vincent, S.J. Scleral lens centration: The influence of centre thickness, scleral topography, and apical clearance. Contact Lens Anterior Eye 2019, 42, 63–69. [Google Scholar] [CrossRef]
- Consejo, A.; Behaegel, J.; Van Hoey, M.; Iskander, D.R.; Rozema, J.J. Scleral asymmetry as a potential predictor for scleral lens compression. Ophthalmic Physiol. Opt. 2018, 38, 609–616. [Google Scholar] [CrossRef]
- DeNaeyer, G.; Sanders, D.R.; Farajian, T.S. Surface coverage with single vs. multiple gaze surface topography to fit scleral lenses. Contact Lens Anterior Eye 2017, 40, 162–169. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Angular position | Distance from the Corneal Centre | |||||
| 6 mm | 7 mm | 8 mm | 9 mm | |||
| 0° | N | 2.43 (0.14) | 3.16 (0.20) | 3.84 (0.23) | 4.55 (0.28) | |
| 45° | S-N | 2.46 (0.17) | 3.18 (0.24) | 3.95 (0.31) | 4.78 (0.40) | |
| 90° | S | 2.47 (0.17) | 3.31 (0.21) | 4.18 (0.26) | 5.07 (0.29) | |
| 135° | S-T | 2.46 (0.16) | 3.28 (0.22) | 4.16 (0.27) | 5.07 (0.32) | |
| 180° | T | 2.49 (0.16) | 3.36 (0.22) | 4.21 (0.25) | 5.03 (0.20) | |
| 225° | I-T | 2.55 (0.17) | 3.40 (0.20) | 4.28 (0.29) | 5.29 (0.48) | |
| 270° | I | 2.52 (0.14) | 3.33 (0.20) | 4.19 (0.33) | 5.20 (0.46) | |
| 315° | I-N | 2.50 (0.14) | 3.22 (0.18) | 3.95 (0.26) | 4.89 (0.38) | |
| Angular position | Distance from the Corneal Centre | |||||
| 6 mm | 7 mm | 8 mm | 9 mm | |||
| 0° | N | 2.34 (0.13) | 3.04 (0.18) | 3.68 (0.21) | 4.27 (0.28) | |
| 45° | S-N | 2.39 (0.13) | 3.08 (0.17) | 3.75 (0.20) | 4.42 (0.26) | |
| 90° | S | 2.46 (0.13) | 3.20 (0.17) | 3.99 (0.23) | 4.71 (0.27) | |
| 135° | S-T | 2.44 (0.12) | 3.24 (0.18) | 4.02 (0.28) | 4.93 (0.35) | |
| 180° | T | 2.35 (0.13) | 3.16 (0.20) | 3.97 (0.25) | 4.73 (0.36) | |
| 225° | I-T | 2.41 (0.13) | 3.20 (0.18) | 3.97 (0.21) | 4.85 (0.26) | |
| 270° | I | 2.46 (0.13) | 3.19 (0.17) | 3.93 (0.22) | 4.82 (0.27) | |
| 315° | I-N | 2.41 (0.14) | 3.07 (0.18) | 3.71 (0.24) | 4.40 (0.25) | |
| Angular position | Distance from the Corneal Centre | |||||
| 6 mm | 7 mm | 8 mm | 9 mm | |||
| 0° | N | 88 (57) | 128 (91) | 157 (96) | 280 (24) | |
| 45° | S-N | 63 (116) | 94 (171) | 199 (238) | 360 (298) | |
| 90° | S | 13 (111) | 112 (110) | 194 (124) | 368 (120) | |
| 135° | S-T | 21 (111) | 37 (138) | 133 (33) | 144 (137) | |
| 180° | T | 142 (94) | 196 (94) | 246 (45) | 299 (297) | |
| 225° | I-T | 136 (110) | 203 (99) | 306 (200) | 438 (404) | |
| 270° | I | 59 (46) | 142 (102) | 255 (250) | 380 (372) | |
| 315° | I-N | 91 (0) | 150 (27) | 241(92) | 493 (289) | |
| Angular position | Caucasians | Asians | ||||||||||
| Distance from the Corneal Centre | Distance from the Corneal Centre | |||||||||||
| 6 mm | 7 mm | 8 mm | 9 mm | 6 mm | 7 mm | 8 mm | 9 mm | |||||
| 0° | N | 0.12 | 0.14 | 0.49 | 0.77 | 0° | N | 0.00 * | 0.01 * | 0.04 * | 0.75 | |
| 45° | S-N | 0.89 | 0.83 | 0.73 | 0.56 | 45° | S-N | 0.00 * | 0.12 | 0.38 | 0.94 | |
| 90° | S | 0.68 | 0.70 | 0.68 | n/a | 90° | S | 0.99 | 0.98 | 0.68 | 0.67 | |
| 135° | S-T | 0.91 | 0.85 | 0.72 | 0.75 | 135° | S-T | 0.99 | 0.99 | 0.99 | 0.52 | |
| 180° | T | 0.27 | 0.63 | 0.52 | 0.63 | 180° | T | 0.69 | 0.60 | 0.58 | 0.40 | |
| 225° | I-T | 0.08 | 0.13 | 0.57 | 0.70 | 225° | I-T | 0.97 | 0.40 | 0.62 | 0.85 | |
| 270° | I | 0.17 | 0.48 | 0.47 | 0.70 | 270° | I | 0.99 | 0.77 | 0.95 | 0.74 | |
| 315° | I-N | 0.85 | 0.85 | 0.77 | 0.28 | 315° | I-N | 0.01 * | 0.27 | 0.44 | 0.95 | |
| Angular position | Caucasians | Asians | ||||||||||
| Distance from the Corneal Centre | Distance from the Corneal Centre | |||||||||||
| 6 mm | 7 mm | 8 mm | 9 mm | 6 mm | 7 mm | 8 mm | 9 mm | |||||
| 0° | N | 117/118 | 102/112 | 80/94 | 36/58 | 0° | N | 125/125 | 116/115 | 82/96 | 33/41 | |
| 45° | S-N | 99/108 | 60/75 | 26/29 | 16/11 | 45° | S-N | 115/125 | 88/115 | 27/96 | 10/41 | |
| 90° | S | 69/82 | 40/43 | 15/15 | 0/16 | 90° | S | 114/111 | 79/74 | 34/33 | 12/10 | |
| 135° | S-T | 95/108 | 65/74 | 31/33 | 10/11 | 135° | S-T | 120/120 | 98/93 | 57/44 | 14/18 | |
| 180° | T | 118/114 | 95/93 | 63/56 | 18/20 | 180° | T | 124/125 | 120/119 | 83/93 | 12/16 | |
| 225° | I-T | 115/109 | 82/86 | 49/50 | 12/15 | 225° | I-T | 125/125 | 118/115 | 97/93 | 31/33 | |
| 270° | I | 83/90 | 54/65 | 28/34 | 9/12 | 270° | I | 116/116 | 86/90 | 44/52 | 12/16 | |
| 315° | I-N | 105/114 | 79/84 | 37/49 | 14/16 | 315° | I-N | 122/123 | 114/116 | 73/87 | 23/33 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Consejo, A.; Wu, R.; Abass, A. Anterior Scleral Regional Variation between Asian and Caucasian Populations. J. Clin. Med. 2020, 9, 3419. https://doi.org/10.3390/jcm9113419
Consejo A, Wu R, Abass A. Anterior Scleral Regional Variation between Asian and Caucasian Populations. Journal of Clinical Medicine. 2020; 9(11):3419. https://doi.org/10.3390/jcm9113419
Chicago/Turabian StyleConsejo, Alejandra, Richard Wu, and Ahmed Abass. 2020. "Anterior Scleral Regional Variation between Asian and Caucasian Populations" Journal of Clinical Medicine 9, no. 11: 3419. https://doi.org/10.3390/jcm9113419
APA StyleConsejo, A., Wu, R., & Abass, A. (2020). Anterior Scleral Regional Variation between Asian and Caucasian Populations. Journal of Clinical Medicine, 9(11), 3419. https://doi.org/10.3390/jcm9113419