The Role of Autoimmune Diseases in the Prognosis of Lymphoma



Abstract
1. Introduction
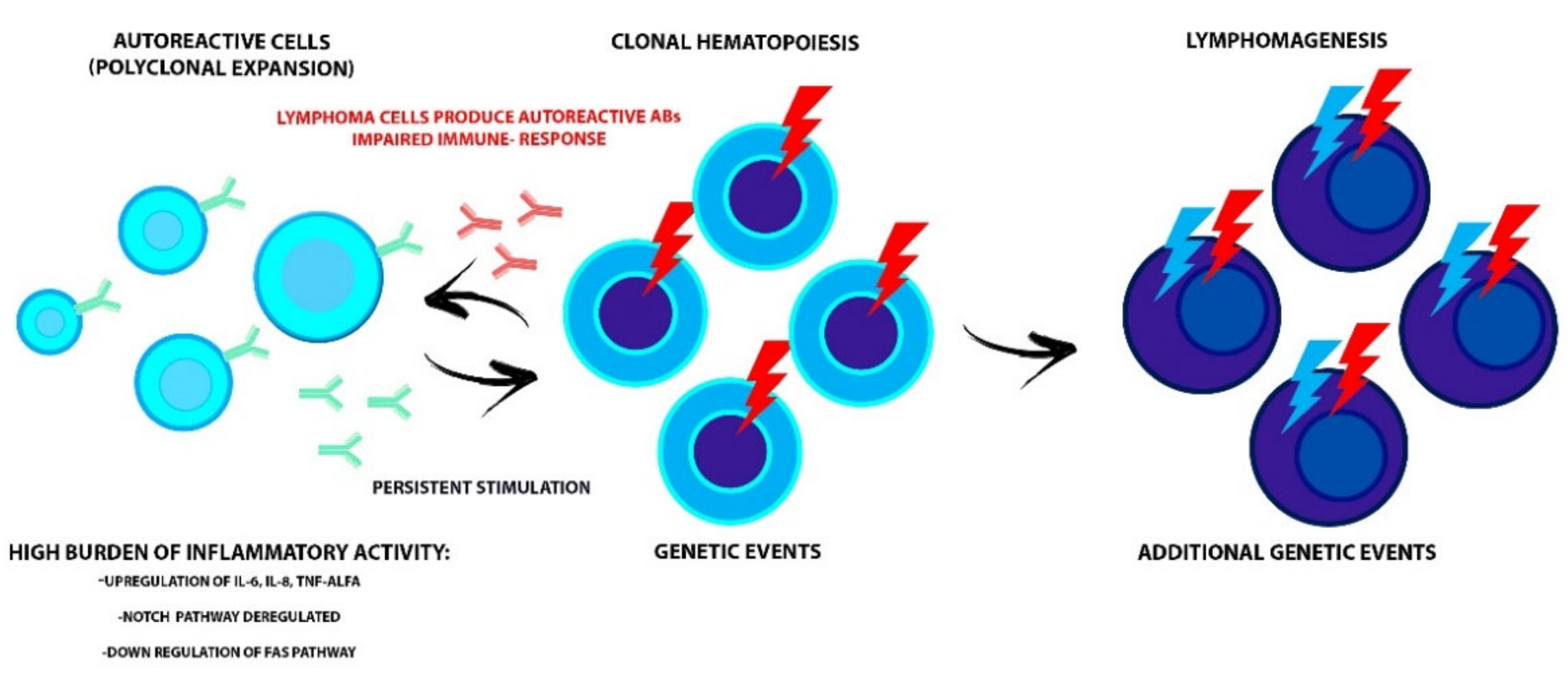
2. Pathophysiology of the Connection between AID and Lymphoma
3. Timing of AID in the Lymphoma Course
4. Lymphoma, AID, and Outcome
5. Outcome in Patients with HL and Pre-Existing AID
6. DLBCL and Autoimmunity
7. Mantle Cell Lymphoma and Autoimmunity
8. Marginal Zone Lymphoma and Autoimmunity
9. T- Cell Lymphoma and Autoimmunity
10. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lim, M.S.; Bailey, N.G.; King, R.L.; Piris, M. Molecular Genetics in the Diagnosis and Biology of Lymphoid Neoplasms. Am. J. Clin. Pathol. 2019, 152, 277–301. [Google Scholar] [CrossRef] [PubMed]
- Hayter, S.M.; Cook, M.C. Updated assessment of the prevalence, spectrum and case definition of autoimmune disease. Autoimmun. Rev. 2012, 11, 754–765. [Google Scholar] [CrossRef] [PubMed]
- Fattizzo, B.; Barcellini, W. Autoimmune Cytopenias in Chronic Lymphocytic Leukemia: Focus on Molecular Aspects. Front. Oncol. 2020, 9, 1435. [Google Scholar] [CrossRef] [PubMed]
- Smedby, K.E.; Vajdic, C.M.; Falster, M.; Engels, E.A.; Martinez-Maza, O.; Turner, J.; Hjalgrim, H.; Vineis, P.; Costantini, A.S.; Bracci, P.M.; et al. Autoimmune disorders and risk of non-Hodgkin lymphoma subtypes: A pooled analysis within the InterLymph Consortium. Blood 2008, 111, 4029–4038. [Google Scholar] [CrossRef] [PubMed]
- Smedby, K.E.; Hjalgrim, H.; Askling, J.; Chang, E.T.; Gregersen, H.; Porwit-MacDonald, A.; Sundström, C.; Åkerman, M.; Melbye, M.; Glimelius, B.; et al. Autoimmune and chronic inflammatory disorders and risk of non-Hodgkin lymphoma by subtype. J. Natl. Cancer Inst. 2006, 98, 51–60. [Google Scholar] [CrossRef]
- Hu, S.; Zhou, D.; Wu, Y.; Zhao, Y.; Wang, S.; Han, B.; Duan, M.; Li, J.; Zhu, T.; Zhuang, J.; et al. Autoimmune disease-associated non-Hodgkin’s lymphoma—A large retrospective study from China. Ann. Hematol. 2019, 98, 445–455. [Google Scholar] [CrossRef]
- Landgren, O.; Pfeiffer, R.M.; Kristinsson, S.Y.; Björkholm, M. Survival patterns in patients with Hodgkin’s lymphoma with a pre-existing hospital discharge diagnosis of autoimmune disease. J. Clin. Oncol. 2010, 28, 5081–5087. [Google Scholar] [CrossRef]
- Kleinstern, G.; Averbuch, M.; Abu Seir, R.; Perlman, R.; Ben Yehuda, D.; Paltiel, O. Presence of autoimmune disease affects not only risk but also survival in patients with B-cell non-Hodgkin lymphoma. Hematol. Oncol. 2018, 36, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Baecklund, E.; Iliadou, A.; Askling, J.; Ekbom, A.; Backlin, C.; Granath, F.; Catrina, A.I.; Rosenquist, R.; Feltelius, N.; Sundström, C.; et al. Association of chronic inflammation, not its treatment, with increased lymphoma risk in rheumatoid arthritis. Arthritis Rheum. 2006, 54, 692–701. [Google Scholar] [CrossRef]
- Khanmohammadi, S.; Shabani, M.; Tabary, M.; Rayzan, E.; Rezaei, N. Lymphoma in the setting of autoimmune diseases: A review of association and mechanisms. Crit. Rev. Oncol. Hematol. 2020, 150. [Google Scholar] [CrossRef]
- Baecklund, E.; Smedby, K.E.; Sutton, L.A.; Askling, J.; Rosenquist, R. Lymphoma development in patients with autoimmune and inflammatory disorders—What are the driving forces? Semin. Cancer Biol. 2014, 24, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Mariette, X.; Cazals-Hatem, D.; Warszawki, J.; Liote, F.; Balandraud, N.; Sibilia, J. Lymphomas in rheumatoid arthritis patients treated with methotrexate: A 3-year prospective study in France. Blood 2002, 99, 3909–3915. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.N.; Mikhail, I.S.; Landgren, O. Autoimmunity and hematologic malignancies: Associations and mechanisms. Leuk. Lymphoma 2009, 50, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Kuksin, C.A.; Minter, L.M. The link between autoimmunity and lymphoma: Does NOTCH signaling play a contributing role? Front. Oncol. 2015, 5, 51. [Google Scholar] [CrossRef]
- Libby, P.; Sidlow, R.; Lin, A.E.; Gupta, D.; Jones, L.W.; Moslehi, J.; Zeiher, A.; Jaiswal, S.; Schulz, C.; Blankstein, R.; et al. Clonal Hematopoiesis: Crossroads of Aging, Cardiovascular Disease, and Cancer: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 567–577. [Google Scholar] [CrossRef]
- Husby, S.; Favero, F.; Nielsen, C.; Sørensen, B.S.; Bæch, J.; Grell, K.; Hansen, J.W.; Rodriguez-Gonzalez, F.G.; Haastrup, E.K.; Fischer-Nielsen, A.; et al. Clinical impact of clonal hematopoiesis in patients with lymphoma undergoing ASCT: A national population-based cohort study. Leukemia 2020. [Google Scholar] [CrossRef]
- Cook, E.K.; Luo, M.; Rauh, M.J. Clonal hematopoiesis and inflammation: Partners in leukemogenesis and comorbidity. Exp. Hematol. 2020, 83, 85–94. [Google Scholar] [CrossRef]
- Teke, H.U.; Gulbas, Z.; Bal, C. Serum levels of cytokines and prevalence of autoantibodies in lymphoma patients and their prognostic value. JBUON 2014, 19, 191–197. [Google Scholar]
- Váróczy, L.; Gergely, L.; Zeher, M.; Szegedi, G.; Illés, A. Malignant lymphoma-associated autoimmune diseases--a descriptive epidemiological study. Rheumatol. Int. 2002, 22, 233–237. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Lebwohl, B.; Rubio-Tapia, A.; Murray, J.A.; Green, P.H.R.; Ekbom, A.; Granath, F. Does celiac disease influence survival in lymphoproliferative malignancy? Eur. J. Epidemiol. 2013, 28, 475–483. [Google Scholar] [CrossRef]
- Simard, J.F.; Baecklund, F.; Chang, E.T.; Baecklund, E.; Hjalgrim, H.; Olov Adami, H.; Glimelius, B.; Smedby, K.E. Lifestyle factors, autoimmune disease and family history in prognosis of non-hodgkin lymphoma overall and subtypes. Int. J. Cancer 2013, 132, 2659–2666. [Google Scholar] [CrossRef]
- Jachiet, V.; Mekinian, A.; Carrat, F.; Grignano, E.; Retbi, A.; Boffa, J.J.; Ronco, P.; Rondeau, E.; Sellam, J.; Berenbaum, F.; et al. Autoimmune manifestations associated with lymphoma: Characteristics and outcome in a multicenter retrospective cohort study. Leuk. Lymphoma 2018, 59, 1399–1405. [Google Scholar] [CrossRef]
- Mikuls, T.R.; Endo, J.O.; Puumala, S.E.; Aoun, P.A.; Black, N.A.; O’Dell, J.R.; Stoner, J.A.; Boilesen, E.C.; Bast, M.A.; Bergman, D.A.; et al. Prospective study of survival outcomes in non-Hodgkin’s lymphoma patients with rheumatoid arthritis. J. Clin. Oncol. 2006, 24, 1597–1602. [Google Scholar] [CrossRef]
- Fallah, M.; Liu, X.; Ji, J.; Försti, A.; Sundquist, K.; Hemminki, K. Hodgkin lymphoma after autoimmune diseases by age at diagnosis and histological subtype. Ann. Oncol. 2014, 25, 1397–1404. [Google Scholar] [CrossRef] [PubMed]
- Lechner, K.; Chen, Y.-A. Paraneoplastic autoimmune cytopenias in Hodgkin lymphoma. Leuk. Lymphoma 2010, 51, 469–474. [Google Scholar] [CrossRef]
- Dimou, M.; Angelopoulou, M.K.; Pangalis, G.A.; Georgios, G.; Kalpadakis, C.; Pappi, V.; Tsopra, O.; Koutsoukos, K.; Zografos, E.; Boutsikas, G.; et al. Autoimmune hemolytic anemia and autoimmune thrombocytopenia at diagnosis and during follow-up of Hodgkin lymphoma. Leuk. Lymphoma 2012, 53, 1481–1487. [Google Scholar] [CrossRef]
- Koff, J.L.; Rai, A.; Flowers, C.R. Characterizing Autoimmune Disease-associated Diffuse Large B-cell Lymphoma in a SEER–Medicare Cohort. Clin. Lymphoma Myeloma Leuk. 2018, 18, e115–e121. [Google Scholar] [CrossRef]
- Mörth, C.; Valachis, A.; Abu Sabaa, A.; Marshall, K.; Hedström, G.; Flogegård, M.; Baecklund, E.; Enblad, G. Autoimmune disease in patients with diffuse large B-cell lymphoma: Occurrence and impact on outcome. Acta Oncol. 2019, 58, 1170–1177. [Google Scholar] [CrossRef] [PubMed]
- Baecklund, E.; Backlin, C.; Iliadou, A.; Granath, F.; Ekbom, A.; Amini, R.M.; Feltelius, N.; Enblad, G.; Sundström, C.; Klareskog, L.; et al. Characteristics of diffuse large B cell lymphomas in rheumatoid arthritis. Arthritis Rheum. 2006, 54, 3774–3781. [Google Scholar] [CrossRef] [PubMed]
- García-Muñoz, R.; Panizo, C.; Bendandi, M.; Llorente, L. Autoimmunity and lymphoma: Is mantle cell lymphoma a mistake of the receptor editing mechanism? Leuk. Res. 2009, 33, 1437–1439. [Google Scholar] [CrossRef]
- Doni, E.; Carli, G.; Di Rocco, A.; Sassone, M.; Gandolfi, S.; Patti, C.; Falisi, E.; Salemi, C.; Visco, C. Autoimmune haemolytic anaemia in mantle cell lymphoma: An insidious complication associated with leukemic disease. Hematol. Oncol. 2017, 35, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Bernatsky, S.; Ramsey-Goldman, R.; Joseph, L.; Boivin, J.F.; Costenbader, K.H.; Urowitz, M.B.; Gladman, D.D.; Fortin, P.R.; Nived, O.; Petri, M.A.; et al. Lymphoma risk in systemic lupus: Effects of disease activity versus treatment. Ann. Rheum. Dis. 2014, 73, 138–142. [Google Scholar] [CrossRef]
- Wöhrer, S.; Troch, M.; Streubel, B.; Zwerina, J.; Skrabs, C.; Formanek, M.; Hauff, W.; Hoffmann, M.; Müllauer, L.; Chott, A.; et al. MALT lymphoma in patients with autoimmune diseases: A comparative analysis of characteristics and clinical course. Leukemia 2007, 21, 1812–1818. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Teixeira Mendes, L.S.; Wotherspoon, A. Marginal zone lymphoma: Associated autoimmunity and autoimmune disorders. Best Pract. Res. Clin. Haematol. 2017, 30, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Murakami, H.; Irisawa, H.; Saitoh, T.; Matsushima, T.; Tamura, J.; Sawamura, M.; Karasawa, M.; Hosomura, Y.; Kojima, M. Immunological abnormalities in splenic marginal zone cell lymphoma. Am. J. Hematol. 1997, 56, 173–178. [Google Scholar] [CrossRef]
- Fodor, A.; Molnar, M.Z.; Krenacs, L.; Bagdi, E.; Csomor, J.; Matolcsy, A.; Demeter, J. Autoimmune hemolytic anemia as a risk factor of poor outcome in patients with splenic marginal zone lymphoma. Pathol. Oncol. Res. 2009, 15, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Siegert, W.; Nerl, C.; Agthe, A.; Engelhard, M.; Brittinger, G.; Tiemann, M.; Lennert, K.; Huhn, D. Angioimmunoblastic lymphadenopathy (AILD)-type T-cell lymphoma: Prognostic impact of clinical observations and laboratory findings at presentation. Ann. Oncol. 1995, 6, 659–664. [Google Scholar] [CrossRef]
- Crickx, E.; Poullot, E.; Moulis, G.; Goulabchand, R.; Fieschi, C.; Galicier, L.; Meignin, V.; Coppo, P.; Delarue, R.; Casasnovas, O.; et al. Clinical spectrum, evolution, and management of autoimmune cytopenias associated with angioimmunoblastic T-cell lymphoma. Eur. J. Haematol. 2019, 103, 35–42. [Google Scholar] [CrossRef]
- Oka, S.; Nohgawa, M. Autoimmune Cytopenias Occurring after Treatment with Chemoimmunotherapy for Non-Hodgkin Lymphomas. Acta Haematol. 2019, 141, 79–83. [Google Scholar] [CrossRef]


{kind=link}
| Lymphoma Subtype | AID | Documented Role of Aid in Lymphoma Prognosis | Comments |
|---|---|---|---|
| HL | RA, SLE | Yes | HL patients with AID 5-y OS 46% (vs. 63.3%); 10-y OS 41% (vs. 51.9%). In female patients the most common cause of death was lymphoma (72% of cases) [13]. |
| Bechet’s disease, PA AHIA, ITP | No No | The mortality is increased due to lymphoma only in Bechet’s disease and pernicious anemia [24]. No difference in terms of OS came out from comparisons between HL patients with and without autoimmune cytopenia [26] | |
| DLBCL | Thyroid disease RA, B-cell mediated AIDs | Yes | No difference in EFS or OS between the two groups, but female patients with primary AID (thyroid disorders excluded) had a worse OS [20]. Post-rituximab era. |
| RA | Yes | The majority of RA-related DLBCLs belong to the non-GC subtype and had a worse prognosis than the GC subtype [29]. Pre-rituximab era. | |
| RA, SLE,SS | No | Low LRS in patients with SLE and DLBCL compared with other groups (but not statistically relevant) [5]. Pre-rituximab era. | |
| MCL | Autoimmune cytopenia | No | The contingency of AIHA in MCL is associated with early lymphoma progression, which is correlated with poor outcomes. (too small sample size) [28]. |
| MZL | RA, SLE, SS Autoimmune cytopenia | No No | The presence of AID has no significant influence on the long term clinical course of MALT lymphoma [33] The occurrence of autoimmune cytopenias during MZL is a sign of transformation to a high-grade lymphoma [30]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masciopinto, P.; Dell’Olio, G.; De Robertis, R.; Specchia, G.; Musto, P.; Albano, F. The Role of Autoimmune Diseases in the Prognosis of Lymphoma. J. Clin. Med. 2020, 9, 3403. https://doi.org/10.3390/jcm9113403
Masciopinto P, Dell’Olio G, De Robertis R, Specchia G, Musto P, Albano F. The Role of Autoimmune Diseases in the Prognosis of Lymphoma. Journal of Clinical Medicine. 2020; 9(11):3403. https://doi.org/10.3390/jcm9113403
Chicago/Turabian StyleMasciopinto, Pierluigi, Grazia Dell’Olio, Rosa De Robertis, Giorgina Specchia, Pellegrino Musto, and Francesco Albano. 2020. "The Role of Autoimmune Diseases in the Prognosis of Lymphoma" Journal of Clinical Medicine 9, no. 11: 3403. https://doi.org/10.3390/jcm9113403
APA StyleMasciopinto, P., Dell’Olio, G., De Robertis, R., Specchia, G., Musto, P., & Albano, F. (2020). The Role of Autoimmune Diseases in the Prognosis of Lymphoma. Journal of Clinical Medicine, 9(11), 3403. https://doi.org/10.3390/jcm9113403