Ischemic and Bleeding Events Associated with Thrombocytopenia and Thrombocytosis after Percutaneous Coronary Intervention in Patients with Acute Myocardial Infarction

 , , ,
, , ,
Abstract
1. Introduction
2. Experimental Section
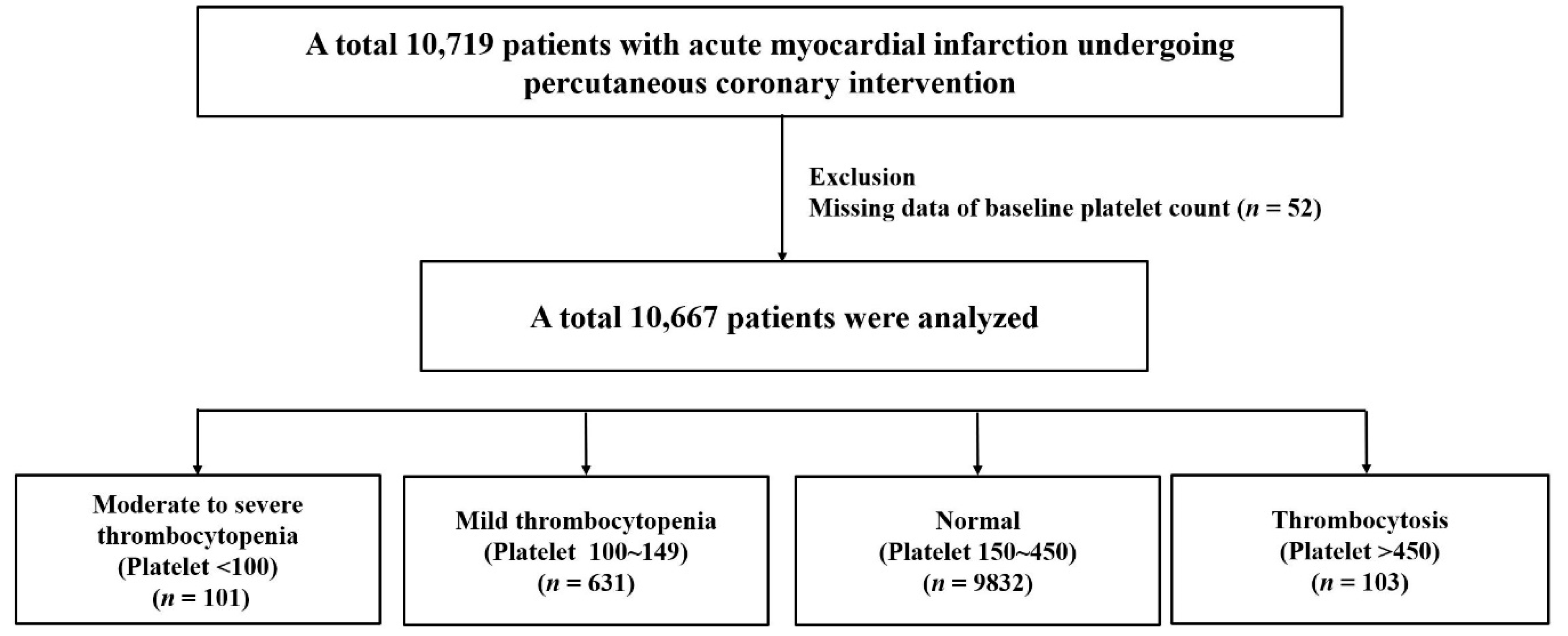
2.1. Study Population
2.2. Endpoints and Definitions
2.3. Stastical Analysis
3. Results
Baseline Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Badimon, L.; Badimon, J.J.; Vilahur, G.; Segales, E.; Llorente, V. Pathogenesis of the acute coronary syndromes and therapeutic implications. Pathophysiol. Haemost. Thromb. 2002, 32, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Frossard, M.; Fuchs, I.; Leitner, J.M.; Hsieh, K.; Vlcek, M.; Losert, H.; Domanovits, H.; Schreiber, W.; Laggner, A.N.; Jilma, B. Platelet function predicts myocardial damage in patients with acute myocardial infarction. Circulation 2004, 110, 1392–1397. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the world health organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- Cheng, W.J.; Yang, S.W.; Gao, F.; Guo, Y.H.; Wang, Z.J.; Zhou, Y.J. Association between baseline platelet count and severe adverse outcomes following percutaneous coronary intervention. J. Geriatr. Cardiol. 2018, 15, 346–355. [Google Scholar] [PubMed]
- Rubinfeld, G.D.; Smilowitz, N.R.; Berger, J.S.; Newman, J.D. Association of thrombocytopenia, revascularization, and in-hospital outcomes in patients with acute myocardial infarction. Am. J. Med. 2019, 132, 942–948.e945. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D. Third universal definition of myocardial infarction. Circulation 2012, 126, 2020–2035. [Google Scholar] [CrossRef]
- Cutlip, D.E.; Windecker, S.; Mehran, R.; Boam, A.; Cohen, D.J.; van Es, G.A.; Steg, P.G.; Morel, M.A.; Mauri, L.; Vranckx, P.; et al. Clinical end points in coronary stent trials: A case for standardized definitions. Circulation 2007, 115, 2344–2351. [Google Scholar] [CrossRef]
- Hicks, K.A.; Tcheng, J.E.; Bozkurt, B.; Chaitman, B.R.; Cutlip, D.E.; Farb, A.; Fonarow, G.C.; Jacobs, J.P.; Jaff, M.R.; Lichtman, J.H.; et al. 2014 acc/aha key data elements and definitions for cardiovascular endpoint events in clinical trials. Circulation 2015, 132, 302–361. [Google Scholar] [CrossRef] [PubMed]
- Ly, H.Q.; Kirtane, A.J.; Murphy, S.A.; Buros, J.; Cannon, C.P.; Braunwald, E.; Gibson, C.M.; TIMI Study Group. Association of platelet counts on presentation and clinical outcomes in st-elevation myocardial infarction (from the timi trials). Am. J. Cardiol. 2006, 98, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Mueller, C.; Neumann, F.J.; Hochholzer, W.; Trenk, D.; Zeller, T.; Perruchoud, A.P.; Buettner, H.J. The impact of platelet count on mortality in unstable angina/non-st-segment elevation myocardial infarction. Am. Heart J. 2006, 151, e1211–e1217. [Google Scholar] [CrossRef] [PubMed]
- Nikolsky, E.; Grines, C.L.; Cox, D.A.; Garcia, E.; Tcheng, J.E.; Sadeghi, M.; Mehran, R.; Lansky, A.J.; Na, Y.; Stone, G.W. Impact of baseline platelet count in patients undergoing primary percutaneous coronary intervention in acute myocardial infarction (from the cadillac trial). Am. J. Cardiol. 2007, 99, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Song, P.S.; Ahn, K.T.; Jeong, J.-O.; Jeon, K.-H.; Song, Y.B.; Gwon, H.-C.; Rha, S.-W.; Jeong, M.H.; Seong, I.-W. Association of baseline platelet count with all-cause mortality after acute myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2020, 2048872620925257. [Google Scholar] [CrossRef] [PubMed]
- Ndrepepa, G.; Guerra, E.; Schulz, S.; Fusaro, M.; Cassese, S.; Kastrati, A. Weight of the bleeding impact on early and late mortality after percutaneous coronary intervention. J. Thromb. Thrombolysis 2015, 39, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Watanabe, H.; Morimoto, T.; Yoshikawa, Y.; Shiomi, H.; Shizuta, S.; Ono, K.; Yamaji, K.; Soga, Y.; Hyodo, M.; et al. Impact of baseline thrombocytopenia on bleeding and mortality after percutaneous coronary intervention. Am. J. Cardiol. 2018, 121, 1304–1314. [Google Scholar] [CrossRef] [PubMed]
- Malyszczak, A.; Lukawska, A.; Dylag, I.; Lis, W.; Mysiak, A.; Kuliczkowski, W. Blood platelet count at hospital admission impacts long-term mortality in patients with acute coronary syndrome. Cardiology 2020, 145, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Skoda, R.C. Thrombocytosis. Hematol. Am. Soc. Hematol. Educ. Program 2009, 159–167. [Google Scholar] [CrossRef]
- Chistolini, A.; Mazzcooni, M.G.; Ferrari, A.; La Verde, G.; Ferrazza, G.; Dragoni, F.; Vitale, A.; Arcieri, R.; Mandelli, F. Essential, thrombocythemia: A retrospective study on the clinical course of 100 patients. Haematologica 1990, 75, 537–540. [Google Scholar] [PubMed]
- Budde, U.; Scharf, R.E.; Franke, P.; Hartmann-Budde, K.; Dent, J.; Ruggeri, Z. Elevated platelet count as a cause of abnormal von willebrand factor multimer distribution in plasma. Blood 1993, 82, 1749–1757. [Google Scholar] [CrossRef]
- Gawaz, M. Role of platelets in coronary thrombosis and reperfusion of ischemic myocardium. Cardiovasc. Res. 2004, 61, 498–511. [Google Scholar] [CrossRef] [PubMed]
- Martin-Garcia, A.C.; Arachchillage, D.R.; Kempny, A.; Alonso-Gonzalez, R.; Martin-Garcia, A.; Uebing, A.; Swan, L.; Wort, S.J.; Price, L.C.; McCabe, C.J.H. Platelet count and mean platelet volume predict outcome in adults with eisenmenger syndrome. Heart 2018, 104, 45–50. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Platelet < 100 K/μL (n = 101) | Platelet 100~149 K/μL (n = 631) | Platelet 150~450 K/μL (n = 9832) | Platelet > 450 K/μL (n = 103) | p Value | |
|---|---|---|---|---|---|
| Clinical Characteristics | |||||
| Age, years | 68.4 ± 11.2 | 68.9 ± 11.9 | 63.2 ± 12.8 | 67.1 ± 12.4 | <0.001 |
| Male | 77 (76.2%) | 491 (77.8%) | 6995 (71.1%) | 52 (50.5%) | <0.001 |
| Body mass index, kg/cm2 | 22.7 ± 3.1 | 23.6 ± 3.4 | 24.1 ± 3.2 | 23.1 ± 3.7 | <0.001 |
| Diabetes mellitus | 39 (38.6%) | 247 (39.1%) | 3048 (31.0%) | 39 (37.9%) | <0.001 |
| Hypertension | 54 (53.5%) | 369 (58.5%) | 5112 (52.0%) | 68 (66.0%) | 0001 |
| Dyslipidemia | 8 (7.9%) | 68 (10.8%) | 1597 (16.2%) | 9 (8.7%) | <0.001 |
| Current smoker | 24 (23.8%) | 195 (30.9%) | 4024 (40.9%) | 26 (25.2%) | <0.001 |
| Previous PCI | 15 (14.9%) | 68 (10.8%) | 686 (7.0%) | 8 (7.8%) | <0.001 |
| Previous MI | 7 (6.9%) | 36 (5.7%) | 396 (4.0%) | 5 (4.9%) | 0.099 |
| Previous stroke | 12 (11.9%) | 63 (10.0%) | 689 (7.0%) | 12 (11.7%) | 0.003 |
| Atrial fibrillation | 15(14.9%) | 60 (9.5%) | 498 (5.1%) | 2 (1.9%) | <0.001 |
| Chronic lung disease | 4 (4.0%) | 18 (2.9%) | 232 (2.4%) | 4 (3.9%) | 0.457 |
| Chronic liver disease | 3 (3.0%) | 15 (2.4%) | 78 (0.8%) | 2 (1.9%) | <0.001 |
| Clinical presentation | |||||
| STEMI NSTEMI | 43 (42.6%) | 309 (49.0%) | 5394 (54.9%) | 62 (60.2%) | 0.001 |
| 58 (57.4%) | 322 (51.0%) | 4438 (45.1%) | 41 (39.8%) | 0.001 | |
| Killip class III~IV | 28 (27.7%) | 140 (22.2%) | 1441 (14.7%) | 23 (22.3%) | <0.001 |
| Use of intravenous inotropics | 32 (31.7%) | 169 (26.8%) | 1666 (16.9%) | 24 (23.3%) | <0.001 |
| Left ventricular ejection fraction, % | 49.9 ± 11.1 | 51.5 ± 11.2 | 53.0 ± 10.9 | 49.8 ± 12.6 | <0.001 |
| Left ventricular ejection fraction < 40% | 18 (17.8%) | 88 (13.9%) | 1112 (11.3%) | 26 (25.2%) | <0.001 |
| White blood cell count, ×103/μL | 9.2 ± 4.8 | 9.2 ± 5.1 | 11.6 ± 6.4 | 13.6 ± 7.2 | <0.001 |
| Hemoglobin, mg/L | 11.8 ± 2.9 | 13.0 ± 2.3 | 13.6 ± 2.1 | 12.1 ± 2.6 | <0.001 |
| Anemia | 59 (58.4%) | 260 (41.2%) | 2834 (28.8%) | 52 (50.5%) | <0.001 |
| Serum creatinine, mg/dL | 1.7 ± 1.8 | 1.6 ± 1.6 | 1.2 ± 1.1 | 1.2 ± 1.2 | <0.001 |
| Estimated glomerular filtration rate, ml/min/1.73 m2 * | 61.9 ± 32.0 | 63.6 ± 28.3 | 76.3 ± 25.5 | 71.6 ± 27.7 | <0.001 |
| Renal insufficiency † | 57 (56.4%) | 355 (56.3%) | 3652 (37.1%) | 49 (47.6%) | <0.001 |
| End stage renal disease | 10 (9.9%) | 36 (5.7%) | 187 (1.9%) | 2 (1.9%) | <0.001 |
| Discharge medications‡ | |||||
| Aspirin | 76 (95.0%) | 544 (97.3%) | 9238 (98.4%) | 93 (95.9%) | 0.004 |
| P2Y12 inhibitor | 78 (97.5%) | 550 (98.4%) | 9318 (99.3%) | 97 (100%) | 0.021 |
| Statin | 70 (87.5%) | 492 (88.0%) | 8502 (90.6%) | 84 (86.6%) | 0.090 |
| Beta-blocker | 62 (77.5%) | 445 (79.6%) | 7831 (83.5%) | 70 (72.2%) | 0.001 |
| ACEI/ARB | 60 (75.0%) | 437 (78.2%) | 7333 (78.1%) | 70 (72.2%) | 0.485 |
| Anticoagulation | 2 (2.5%) | 21 (3.8%) | 222 (2.4%) | 5 (5.2%) | 0.067 |
| Angiographic characteristics | |||||
| Number of coronary arteries involved | 0.200 | ||||
| One | 38 (37.6%) | 257 (40.7%) | 4358 (44.3%) | 53 (51.5%) | |
| Two | 35 (34.7%) | 225 (35.7%) | 3244 (33.0%) | 26 (25.2%) | |
| Three | 28 (27.7%) | 149 (23.6%) | 2230 (22.7%) | 24 (23.3%) | |
| Multi vessel disease | 63 (62.4%) | 374 (59.3%) | 5474 (55.7%) | 50 (48.5%) | 0.079 |
| Culprit coronary artery | <0.001 | ||||
| Left anterior descending artery | 46 (45.5%) | 260 (41.2%) | 4720 (48.0%) | 62 (60.2%) | |
| Right coronary artery | 38 (37.6%) | 231 (36.6%) | 3168 (32.2%) | 27 (26.2%) | |
| Left circumflex artery | 15 (14.9%) | 103 (16.3%) | 1626 (16.5%) | 12 (11.7%) | |
| Left main artery | 2 (2.0%) | 33 (5.2%) | 307 (3.1%) | 2 (1.9%) | |
| Procedural characteristics | |||||
| Treated Coronary artery | |||||
| Left anterior descending artery | 62 (61.4%) | 333 (52.8%) | 5919 (60.2%) | 73 (70.9%) | <0.001 |
| Right coronary artery | 43 (42.6%) | 264 (41.8%) | 3880 (39.5%) | 36 (35.0%) | 0.440 |
| Left circumflex artery | 25 (24.8%) | 165 (26.1%) | 2608 (26.5%) | 22 (21.4%) | 0.664 |
| Left main artery | 4 (4.0%) | 36 (5.7%) | 397 (4.0%) | 5 (4.9%) | 0.232 |
| Number of treated coronary arteries | 0.403 | ||||
| One | 71 (70.3%) | 490 (77.7%) | 7218 (73.4%) | 75 (72.8%) | |
| Two or More | 30 (29.7%) | 141 (22.3%) | 261 4 (26.6%) | 2 (27.2%) | |
| Total stent number | 1.5 ± 1.0 | 1.5 ± 0.8 | 1.6 ± 0.9 | 1.5 ± 0.8 | 0.004 |
| Total stent number ≥ 3 | 17 (16.8%) | 69 (10.9%) | 1408 (14.3%) | 10 (9.7%) | 0.049 |
| Mean stent diameter (mm) | 3.1 ± 0.3 | 3.2 ± 0.4 | 3.2 ± 0.4 | 3.2 ± 0.5 | 0.083 |
| Total stent length (mm) | 35.4 ± 24.7 | 31.9 ± 17.5 | 34.2 ± 20.5 | 32.5 ± 19.2 | 0.035 |
| Thrombus aspiration | 9 (8.9%) | 93 (14.7%) | 1202 (12.2%) | 15 (14.6%) | 0.170 |
| Use of glycoproteins IIb/IIIa inhibitor | 12 (11.9%) | 109 (17.3%) | 1736 (17.7%) | 24 (23.3%) | 0.200 |
| Platelet < 100 K/μL (n = 101) | Platelet 100~149 K/μL (n = 631) | Platelet 150~450 K/μL (n = 9832) | Platelet > 450 K/μL (n = 103) | p Value | |
|---|---|---|---|---|---|
| 5-year outcomes | |||||
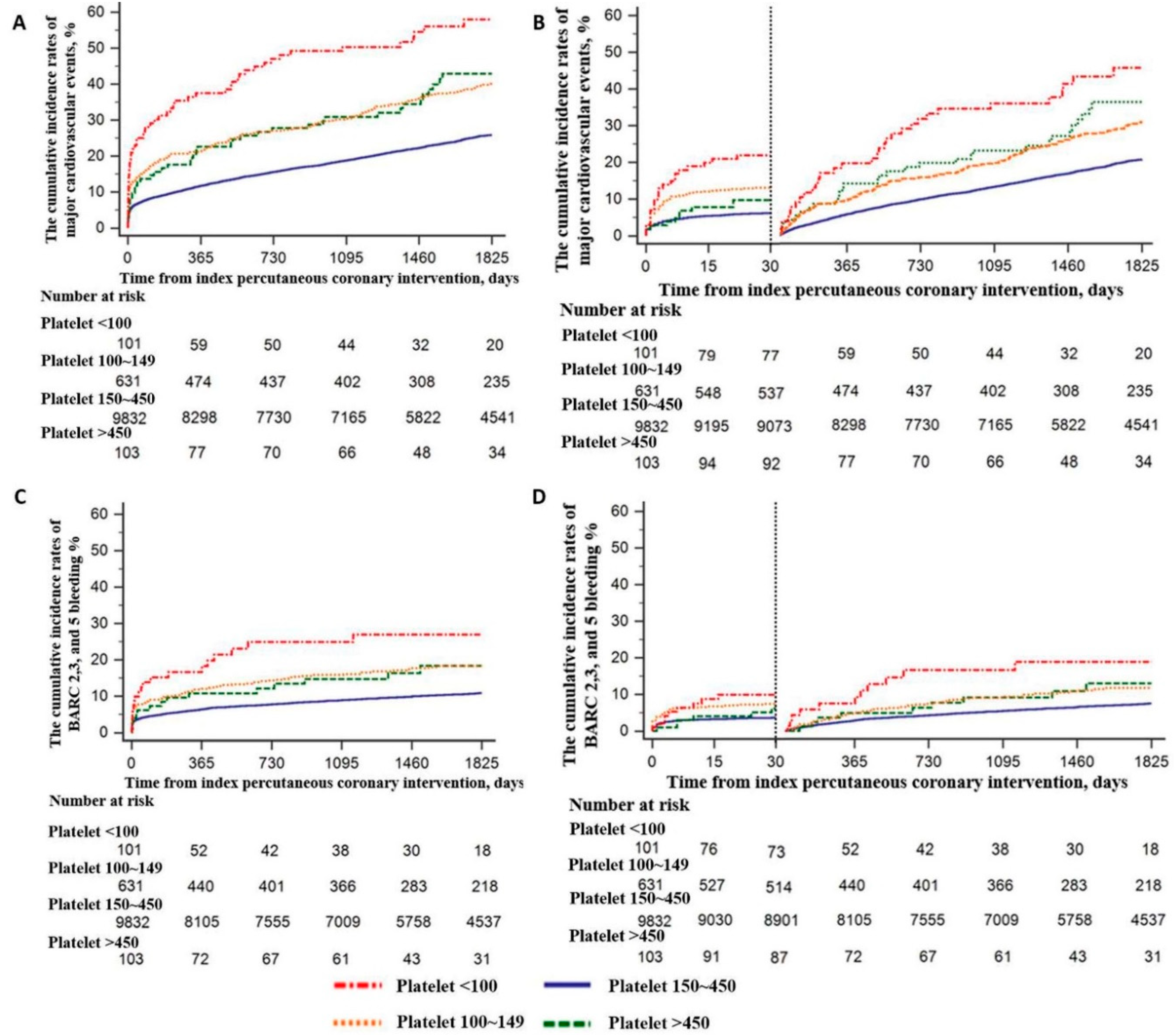
| MACE * | 54 (53.5%) | 235 (37.2%) | 2308 (23.5%) | 40 (38.8%) | <0.001 |
| All-cause death | 53 (52.5%) | 216 (34.2%) | 1786 (18.2%) | 38 (36.9%) | <0.001 |
| Recurrent myocardial infarction | 3 (3.0%) | 23 (3.6%) | 437 (4.4%) | 3 (2.9%) | 0.946 |
| Stroke | 4 (4.0%) | 22 (3.5%) | 325 (3.3%) | 3 (2.9%) | 0.683 |
| Cardiovascular death | 33 (32.7%) | 161 (25.5%) | 1410 (14.3%) | 31 (30.1%) | <0.001 |
| BARC 2, 3, and 5 bleeding | 20 (19.8%) | 96 (15.2%) | 929 (9.4%) | 15 (14.6%) | <0.001 |
| BARC 3 and 5 bleeding | 16 (15.8%) | 72 (11.4%) | 627 (6.4%) | 9 (8.7%) | <0.001 |
| 30-day outcomes | |||||
| MACE * | 22 (21.8%) | 82 (13.0%) | 609 (6.2%) | 10 (9.7%) | <0.001 |
| All-cause death | 21 (20.8%) | 73 (11.6%) | 491 (5.0%) | 9 (8.7%) | <0.001 |
| Recurrent myocardial infarction | 1 (1.0%) | 3 (0.5%) | 66 (0.7%) | 1 (1.0%) | 0.892 |
| Stroke | 2 (2.0%) | 8 (1.3%) | 88 (0.9%) | 0 (0.0%) | 0.268 |
| Cardiovascular death | 15 (14.9%) | 65 (10.3%) | 456 (4.6%) | 9 (8.7%) | <0.001 |
| BARC 2, 3, and 5 bleeding | 9 (8.9%) | 45 (7.1%) | 350 (3.6%) | 6 (5.8%) | <0.001 |
| BARC 3 and 5 bleeding | 8 (7.9%) | 41 (6.5%) | 320 (3.3%) | 5 (4.9%) | <0.001 |
| 30-day to 5-year outcomes | |||||
| MACE * | 32 (31.7%) | 153 (24.2%) | 1699 (17.3%) | 30 (29.1%) | <0.001 |
| All-cause death | 32 (31.7%) | 143 (22.6%) | 1295 (13.2%) | 29 (28.2%) | <0.001 |
| Recurrent myocardial infarction | 2 (2.0%) | 20 (3.1%) | 371 (3.7%) | 2 (1.9%) | 0.498 |
| Stroke | 2 (2.0%) | 14 (2.2%) | 237 (2.4%) | 3 (2.9%) | 0.963 |
| Cardiovascular death | 18 (17.8%) | 96 (15.2%) | 954 (9.7%) | 22 (21.4%) | <0.001 |
| BARC 2, 3, and 5 bleeding | 11(10.9%) | 51 (8.1%) | 579 (5.8%) | 9 (8.8%) | 0.015 |
| BARC 3 and 5 bleeding | 8 (7.9%) | 31 (4.9%) | 307 (3.1%) | 4 (4.8%) | 0.005 |
| Platelet < 100 K/μL (n = 101) | Platelet 100~149 K/μL (n = 631) | Platelet 150~450 K/μL (n = 9832) | Platelet > 450 K/μL (n = 103) | ||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | ||
| 5-year MACE | |||||||
| Univariate | 3.17 (2.42–4.16) | <0.001 | 1.78 (1.55–2.03) | <0.001 | Reference | 1.83 (1.34–2.50) | <0.001 |
| Model 1 * | 2.72 (2.07–3.56) | <0.001 | 1.35 (1.18–1.55) | <0.001 | Reference | 1.55 (1.13–2.12) | 0.006 |
| Model 2 † | 2.43 (1.84–3.20) | <0.001 | 1.31 (1.14–1.51) | <0.001 | Reference | 1.49 (1.09–2.04) | 0.013 |
| Model 3 ‡ | 2.03 (1.49–2.78) | <0.001 | 1.15 (1.01–1.34) | 0.045 | Reference | 1.47 (1.07–2.03) | 0.019 |
| 5-year BARC 2,3, and 5 bleeding | |||||||
| Univariate | 2.88 (1.85–4.49) | <0.001 | 1.83 (1.49–2.26) | <0.001 | Reference | 1.71(1.03–2.84) | 0.040 |
| Model 1 | 2.68 (1.72–4.18) | <0.001 | 1.66 (1.35–2.06) | <0.001 | Reference | 1.50 (0.90–2.51) | 0.117 |
| Model 2 | 2.45 (1.57–3.83) | <0.001 | 1.61 (1.29–2.01) | <0.001 | Reference | 1.42 (0.85–2.36) | 0.184 |
| Model 3 | 2.18 (1.36–3.49) | 0.001 | 1.41 (1.12–1.78) | 0.004 | Reference | 1.42 (0.85–2.37) | 0.180 |
| 30-day MACE | |||||||
| Univariate | 3.78 (2.47–5.79) | <0.001 | 2.18 (1.73–2.74) | <0.001 | Reference | 1.57 (0.84–2.94) | 0.155 |
| Model 1 | 3.26 (2.13–4.99) | <0.001 | 1.73 (1.37–2.19) | <0.001 | Reference | 1.27 (0.68–2.37) | 0.459 |
| Model 2 | 3.19 (2.04–5.02) | <0.001 | 1.84 (1.43–2.38) | <0.001 | Reference | 1.39 (0.74–2.61) | 0.304 |
| Model 3 | 2.22 (1.21–4.10) | 0.010 | 1.30 (1.03–1.81) | 0.012 | Reference | 1.43 (0.74–2.80) | 0.290 |
| 30-day BARC 2,3, and 5 bleeding | |||||||
| Univariate | 2.65 (1.37–5.13) | 0.004 | 2.09 (1.54–2.86) | <0.001 | Reference | 1.63 (0.73–3.66) | 0.233 |
| Model 1 | 2.47 (1.27–4.79) | 0.007 | 1.92 (1.40–2.63) | <0.001 | Reference | 1.36 (0.61–3.06) | 0.452 |
| Model 2 | 2.26 (1.16–4.41) | 0.016 | 1.94 (1.41–2.68) | <0.001 | Reference | 1.31 (0.58–2.95) | 0.509 |
| Model 3 | 1.99 (1.00–4.04) | 0.048 | 1.57 (1.11–2.23) | 0.012 | Reference | 1.22 (0.54–2.74) | 0.635 |
| 30-day to 5-year MACE | |||||||
| Univariate | 2.95 (2.10–4.15) | <0.001 | 1.64 (1.40–1.93) | <0.001 | Reference | 1.95 (1.37–2.79) | <0.001 |
| Model 1 | 2.55 (1.81–3.58) | <0.001 | 1.22 (1.04–1.44) | 0.016 | Reference | 1.69 (1.18–2.41) | 0.004 |
| Model 2 | 2.22 (1.58–3.12) | <0.001 | 1.17 (1.01–1.38) | 0.045 | Reference | 1.55 (1.09–2.22) | 0.016 |
| Model 3 | 1.93 (1.35–2.74) | <0.001 | 1.11 (1.00–1.32) | 0.049 | Reference | 1.54 (1.07–2.21) | 0.020 |
| 30-day to 5-year BARC 2,3, and 5 bleeding | |||||||
| Univariate | 2.88 (1.85–4.49) | <0.001 | 1.83 (1.49–2.26) | <0.001 | Reference | 1.71 (1.03–2.84) | 0.040 |
| Model 1 | 2.68 (1.72–4.18) | <0.001 | 1.66 (1.35–2.06) | <0.001 | Reference | 1.50 (0.90–2.51) | 0.117 |
| Model 2 | 2.45 (1.57–3.83) | <0.001 | 1.61 (1.29–2.01) | <0.001 | Reference | 1.42 (0.85–2.36) | 0.184 |
| Model 3 | 2.06 (1.29–3.31) | 0.003 | 1.39 (1.11–1.76) | 0.005 | Reference | 1.45 (0.87–2.43) | 0.154 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roh, J.W.; Lim, S.; Hwang, Y.; Lee, K.Y.; Choo, E.H.; Choi, I.J.; Hwang, B.-H.; Kim, C.J.; Park, M.-W.; Kim, D.-B.; et al. Ischemic and Bleeding Events Associated with Thrombocytopenia and Thrombocytosis after Percutaneous Coronary Intervention in Patients with Acute Myocardial Infarction. J. Clin. Med. 2020, 9, 3370. https://doi.org/10.3390/jcm9103370
Roh JW, Lim S, Hwang Y, Lee KY, Choo EH, Choi IJ, Hwang B-H, Kim CJ, Park M-W, Kim D-B, et al. Ischemic and Bleeding Events Associated with Thrombocytopenia and Thrombocytosis after Percutaneous Coronary Intervention in Patients with Acute Myocardial Infarction. Journal of Clinical Medicine. 2020; 9(10):3370. https://doi.org/10.3390/jcm9103370
Chicago/Turabian StyleRoh, Ji Woong, Sungmin Lim, Youngdeok Hwang, Kwan Yong Lee, Eun Ho Choo, Ik Jun Choi, Byung-Hee Hwang, Chan Joon Kim, Mahn-Won Park, Dong-Bin Kim, and et al. 2020. "Ischemic and Bleeding Events Associated with Thrombocytopenia and Thrombocytosis after Percutaneous Coronary Intervention in Patients with Acute Myocardial Infarction" Journal of Clinical Medicine 9, no. 10: 3370. https://doi.org/10.3390/jcm9103370
APA StyleRoh, J. W., Lim, S., Hwang, Y., Lee, K. Y., Choo, E. H., Choi, I. J., Hwang, B.-H., Kim, C. J., Park, M.-W., Kim, D.-B., Lee, J.-M., Park, C. S., Kim, H.-Y., Yoo, K.-D., Jeon, D. S., Youn, H. J., Chung, W. S., Kim, M. C., Jeong, M. H., ... Chang, K. (2020). Ischemic and Bleeding Events Associated with Thrombocytopenia and Thrombocytosis after Percutaneous Coronary Intervention in Patients with Acute Myocardial Infarction. Journal of Clinical Medicine, 9(10), 3370. https://doi.org/10.3390/jcm9103370