Evaluation of Strip Meniscometry and Association with Clinical and Demographic Variables in a Community Eye Study (in Bangladesh)

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Participants
2.3. Study Procedures
2.3.1. Questionnaire
2.3.2. Strip Meniscometry
2.3.3. Fluorescein Breakup Time (TBUT)
2.3.4. Schirmer’s I Test
2.3.5. Meibomian Gland Dysfunction Examination
2.3.6. Slit-Lamp Examination
2.4. Statistical Analysis
3. Results
3.1. Clinical and Characteistics of Participants
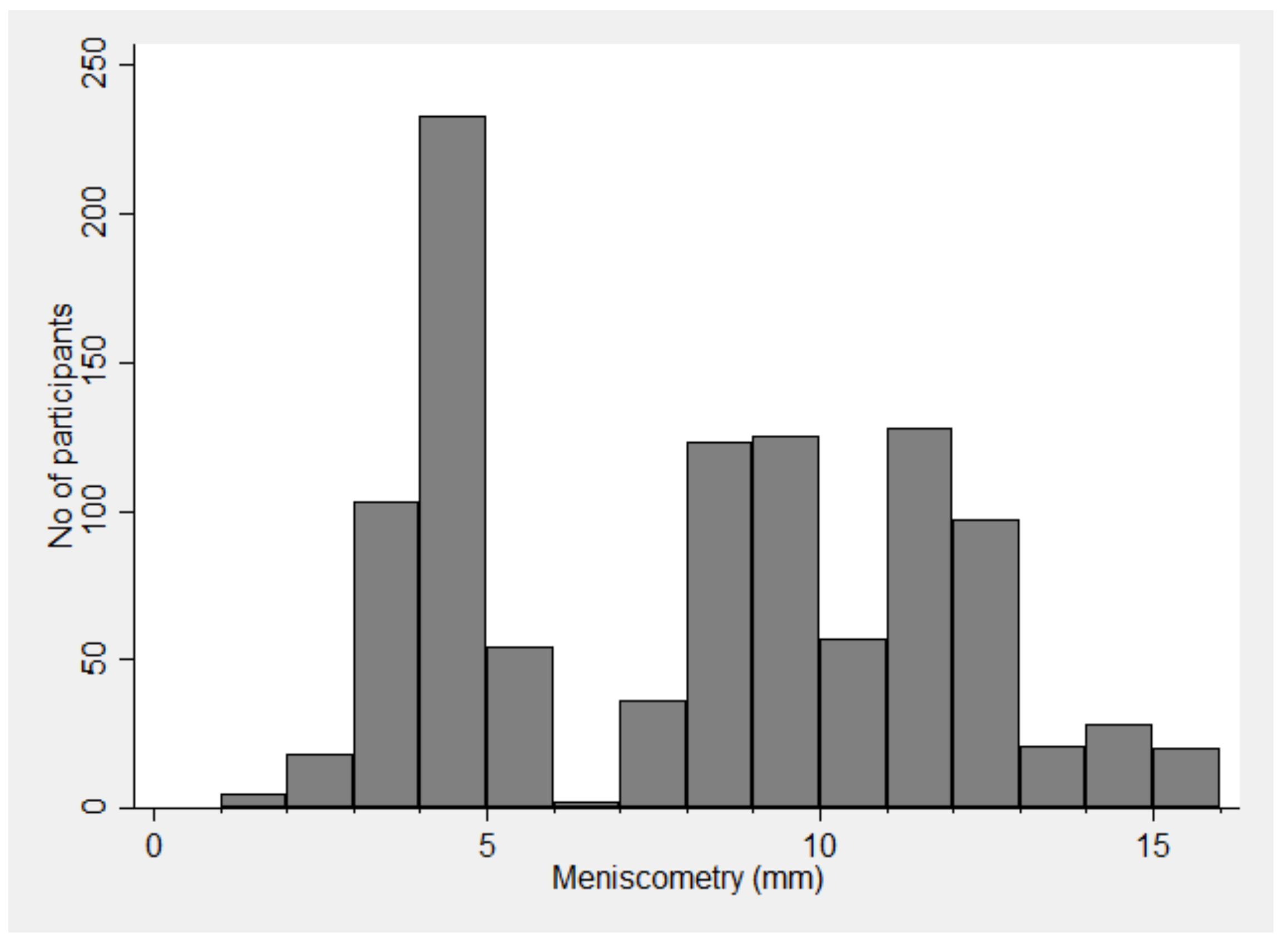
3.2. Distribution of Strip Meniscometry Readings
3.3. Factors Affecting Strip Meniscometry
3.4. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Nelson, J.D.; Azar, D.T.; Belmonte, C.; Bron, A.J.; Chauhan, S.K.; de Paiva, C.S.; Gomes, J.A.; Hammitt, K.M.; Jones, L.; et al. TFOS DEWS II Report Executive Summary. Ocul. Surf. 2017, 15, 802–812. [Google Scholar] [CrossRef]
- Stapleton, F.; Alves, M.; Bunya, V.Y.; Jalbert, I.; Lekhanont, K.; Malet, F.; Na, K.S.; Schaumberg, D.; Uchino, M.; Vehof, J.; et al. TFOS DEWS II Epidemiology Report. Ocul. Surf. 2017, 15, 334–365. [Google Scholar] [CrossRef]
- Clegg, J.P.; Guest, J.F.; Lehman, A.; Smith, A.F. The annual cost of dry eye syndrome in France, Germany, Italy, Spain, Sweden and the United Kingdom among patients managed by ophthalmologists. Ophthalmic Epidemiol. 2006, 13, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Wlodarczyk, J.; Fairchild, C. United States cost-effectiveness study of two dry eye ophthalmic lubricants. Ophthalmic Epidemiol. 2009, 16, 22–30. [Google Scholar] [CrossRef]
- Sullivan, R.M.; Cermak, J.M.; Papas, A.S.; Dana, M.R.; Sullivan, D.A. Economic and quality of life impact of dry eye symptoms in women with Sjogren’s syndrome. Adv. Exp. Med. Biol. 2002, 506, 1183–1188. [Google Scholar]
- Yu, J.; Asche, C.V.; Fairchild, C.J. The economic burden of dry eye disease in the United States: A decision tree analysis. Cornea 2011, 30, 379–387. [Google Scholar] [CrossRef]
- Reddy, P.; Grad, O.; Rajagopalan, K. The economic burden of dry eye: A conceptual framework and preliminary assessment. Cornea 2004, 23, 751–761. [Google Scholar] [CrossRef]
- Chhadva, P.; Goldhardt, R.; Galor, A. Meibomian Gland Disease: The Role of Gland Dysfunction in Dry Eye Disease. Ophthalmology 2017, 124, S20–S26. [Google Scholar] [CrossRef] [PubMed]
- Nichols, K.K.; Foulks, G.N.; Bron, A.J.; Glasgow, B.J.; Dogru, M.; Tsubota, K.; Lemp, M.A.; Sullivan, D.A. The international workshop on meibomian gland dysfunction: Executive summary. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1922–1929. [Google Scholar] [CrossRef]
- Osae, A.E.; Gehlsen, U.; Horstmann, J.; Siebelmann, S.; Stern, M.E.; Kumah, D.B.; Steven, P. Epidemiology of dry eye disease in Africa: The sparse information, gaps and opportunities. Ocul. Surf. 2017, 15, 159–168. [Google Scholar] [CrossRef]
- Lee, A.J.; Lee, J.; Saw, S.M.; Gazzard, G.; Koh, D.; Widjaja, D.; Tan, D.T. Prevalence and risk factors associated with dry eye symptoms: A population based study in Indonesia. Br. J. Ophthalmol. 2002, 86, 1347–1351. [Google Scholar] [CrossRef]
- Sutradhar, I.; Gayen, P.; Hasan, M.; Gupta RDas Roy, T.; Sarker, M. Eye diseases: The neglected health condition among urban slum population of Dhaka, Bangladesh. BMC Ophthalmol. 2019, 19, 38. [Google Scholar] [CrossRef]
- Ibrahim, O.M.A.; Dogru, M.; Ward, S.K.; Matsumoto, Y.; Wakamatsu, T.H.; Ishida, K.; Tsuyama, A.; Kojima, T.; Shimazaki, J.; Tsubota, K. The efficacy, sensitivity, and specificity of strip meniscometry in conjunction with tear function tests in the assessment of tear meniscus. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2194–2198. [Google Scholar] [CrossRef]
- Dogru, M.; Ishida, K.; Matsumoto, Y.; Goto, E.; Ishioka, M.; Kojima, T.; Goto, T.; Saeki, M.; Tsubota, K. Strip meniscometry: A new and simple method of tear meniscus evaluation. Investig. Ophthalmol. Vis. Sci. 2006, 47, 1895–1901. [Google Scholar] [CrossRef]
- Rashid, M.A.K.M.; Teo, C.H.Y.; Mamun, S.; Ong, H.S.; Tong, L. Prevalence and Risk Factors of Severe Dry Eye in Bangladesh-Based Factory Garment Workers. Diagnostics 2020, 10, 634. [Google Scholar] [CrossRef]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef]
- Foong, A.W.; Saw, S.M.; Loo, J.L.; Shen, S.; Loon, S.C.; Rosman, M.; Aung, T.; Tan, D.T.; Tai, E.S.; Wong, T.Y. Rationale and methodology for a population-based study of eye diseases in Malay people: The Singapore Malay eye study (SiMES). Ophthalmic Epidemiol. 2007, 14, 25–35. [Google Scholar] [CrossRef]
- Koh, S.; Watanabe, H.; Hosohata, J.; Hori, Y.; Hibino, S.; Nishida, K.; Maeda, N.; Tano, Y. Diagnosing dry eye using a blue-free barrier filter. Am. J. Ophthalmol. 2003, 136, 513–519. [Google Scholar] [CrossRef]
- Peterson, R.C.; Wolffsohn, J.S. Objective grading of the anterior eye. Optom. Vis. Sci. 2009, 86, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Terry, R.L.; Schnider, C.M.; Holden, B.A.; Cornish, R.; Grant, T.; Sweeney, D.; La Hood, D.O.; Back, A.R. CCLRU standards for success of daily and extended wear contact lenses. Optom. Vis. Sci. 1993, 70, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Bruce, A.S. Preliminary Examination. Contact Lens Pract. 2018. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Participants N (%) | Strip Meniscometry Reading Mean± Standard Deviation (SD) Median (Min, Max) | p Value | |
|---|---|---|---|
| Overall | 1050 (100%) | 7.7 ± 3.6 8 (1, 16) | - |
| Gender | <0.001 | ||
| Male | 485 (46.19%) | 7.1 ± 3.8 7 (1, 16) | |
| Female | 565 (53.81%) | 8.1 ± 3.3 9 (2, 16) | |
| Age | <0.001 | ||
| <30 years | 371 (35.33%) | 8.4 ± 3.8 10 (2, 16) | |
| 30–40 years | 219 (20.86%) | 7.3 ± 3.1 8 (1, 16) | |
| 40–50 years | 347 (33.05%) | 6.9 ± 3.4 8 (2, 16) | |
| >50 years | 113 (10.76%) | 8.1 ± 3.6 9 (2, 14) | |
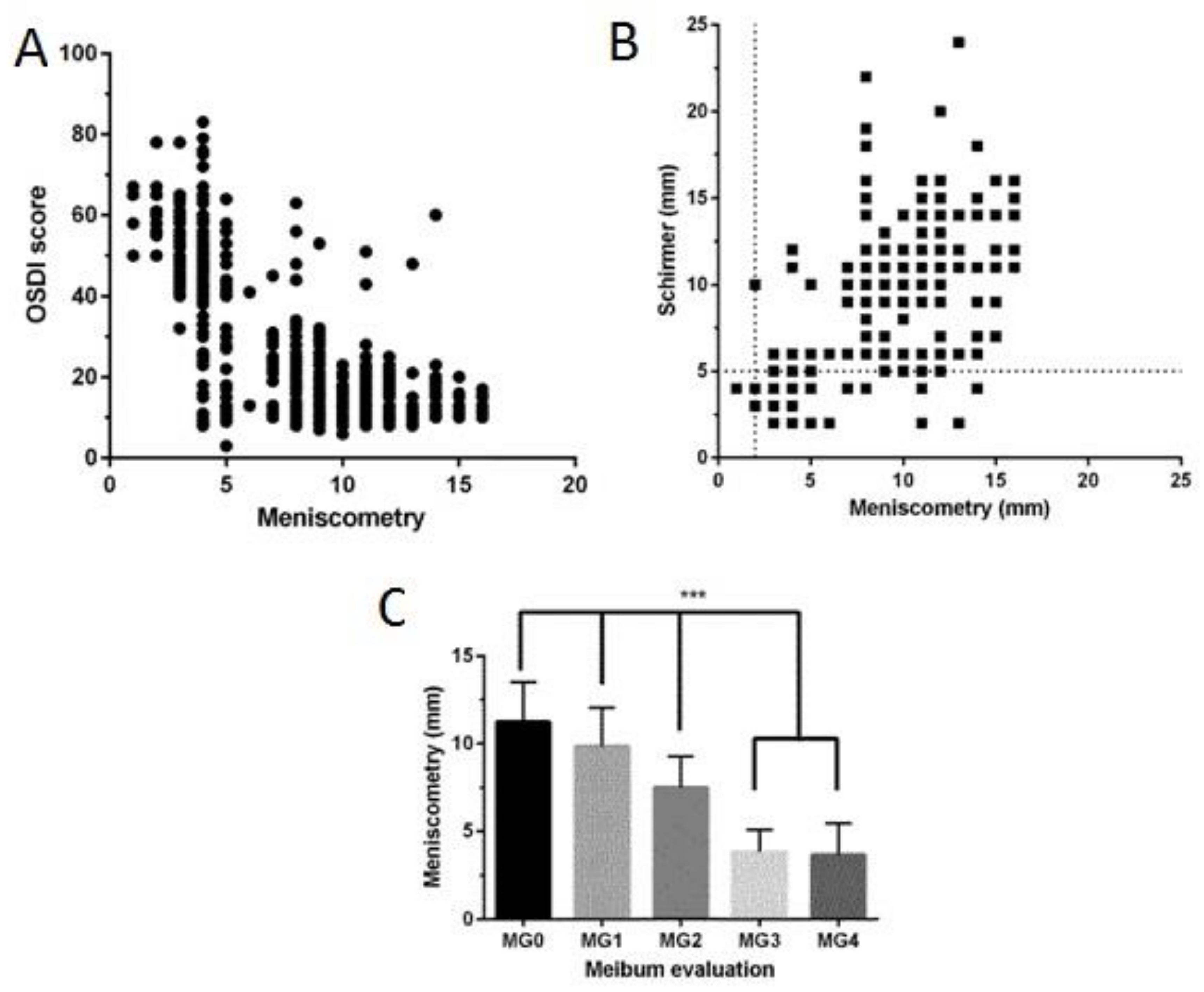
| Ocular Surface Disease Index (OSDI) | <0.001 | ||
| Low (<33) | 679 (64.67%) | 9.7 ± 2.5 10 (3, 16) | |
| High (≥33) | 371 (35.33%) | 3.9 ± 1.4 4 (1, 14) | |
| Schirmer I test | <0.001 | ||
| Low (<5 mm) | 413 (39.33%) | 4.0 ± 1.7 4 (1, 14) | |
| High (≥5 mm) | 637 (60.67%) | 10.0 ± 2.3 10 (2, 16) | |
| Tear Breakup Time (TBUT) | <0.001 | ||
| Low (<5 s) | 369 (35.14%) | 3.8 ± 1.3 4 (1, 14) | |
| High (≥5 s) | 681 (64.86%) | 9.8 ± 2.5 10 (3, 16) | |
| Meibomian Gland Dysfunction (MGD) Types | <0.001 | ||
| Type 0 | 275 (26.19%) | 11.2 ± 2.3 11 (3, 16) | |
| Type 1 | 182 (17.33%) | 9.8 ± 2.2 10 (4, 16) | |
| Type 2 | 593 (56.48%) | 5.3 ± 2.4 4 (1, 14) |
| Model 1 | Model 2 † | Model 3 †† | Model 4 ††† | |
|---|---|---|---|---|
| Parameters | Unadjusted Odds Ratio (95% Confidence Interval) | Adjusted Odds Ratio (95% Confidence Interval) | Adjusted Odds Ratio (95% Confidence Interval) | Adjusted Odds Ratio (95% Confidence Interval) |
| Age | 1.01 (1.00–1.02) * | 1.00 (0.99–1.02) | 0.97 (0.95–0.99) * | 0.97 (0.94–1.00) |
| Gender | 1.85 (1.44–2.38) * | 1.83 (1.42–2.35) * | 1.67 (1.06–2.63) * | 1.09 (0.61–1.94) |
| OSDI | 1.16 (1.15–1.18) * | 1.17 (1.15–1.19) * | 1.05 (1.02–1.08) * | |
| TBUT | 0.43 (0.39–0.47) * | 0.87 (0.72–1.05) | ||
| Schirmers | 0.17 (0.13–0.23) * | 0.43 (0.35–0.54) * | ||
| MGD | 12.15 (8.96–16.48) * | 1.42 (0.79–2.57) |
| Model 1 | Model 2 † | Model 3 †† | Model 4 ††† | |
|---|---|---|---|---|
| Parameters | Unadjusted Odds Ratio (95% Confidence Interval) | Adjusted Odds Ratio (95% Confidence Interval) | Adjusted Odds Ratio (95% Confidence Interval) | Adjusted Odds Ratio (95% Confidence Interval) |
| Age | 1.04 (1.00–1.08) | 1.03 (1.00–1.08) | 1.02 (0.98–1.07) | 1.04 (0.99–1.09) |
| Gender | 2.72 (1.11–6.67) * | 2.52 (1.02–6.19) * | 1.84 (0.70–4.89) | 1.37 (0.49–3.82) |
| OSDI | 1.13 (1.09–1.18) * | 1.13 (1.08–1.18) * | 1.11 (1.06–1.17) * | |
| TBUT | 0.41 (0.29–0.60) * | 0.48 (0.30–0.77) * | ||
| Schirmers | 0.59 (0.44–0.78) * | 1.33 (0.94–1.86) | ||
| MGD grading | 4.80 (2.63–8.77) * | 1.67 (0.60–4.68) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rashid, M.A.K.M.; Thia, Z.Z.; Teo, C.H.Y.; Mamun, S.; Ong, H.S.; Tong, L. Evaluation of Strip Meniscometry and Association with Clinical and Demographic Variables in a Community Eye Study (in Bangladesh). J. Clin. Med. 2020, 9, 3366. https://doi.org/10.3390/jcm9103366
Rashid MAKM, Thia ZZ, Teo CHY, Mamun S, Ong HS, Tong L. Evaluation of Strip Meniscometry and Association with Clinical and Demographic Variables in a Community Eye Study (in Bangladesh). Journal of Clinical Medicine. 2020; 9(10):3366. https://doi.org/10.3390/jcm9103366
Chicago/Turabian StyleRashid, Mamunur A.K.M., Zhang Zhe Thia, Calesta Hui Yi Teo, Sumaiya Mamun, Hon Shing Ong, and Louis Tong. 2020. "Evaluation of Strip Meniscometry and Association with Clinical and Demographic Variables in a Community Eye Study (in Bangladesh)" Journal of Clinical Medicine 9, no. 10: 3366. https://doi.org/10.3390/jcm9103366
APA StyleRashid, M. A. K. M., Thia, Z. Z., Teo, C. H. Y., Mamun, S., Ong, H. S., & Tong, L. (2020). Evaluation of Strip Meniscometry and Association with Clinical and Demographic Variables in a Community Eye Study (in Bangladesh). Journal of Clinical Medicine, 9(10), 3366. https://doi.org/10.3390/jcm9103366