Association between Carotid Artery Calcification and Periodontal Disease Progression in Japanese Men and Women: A Cross-Sectional Study

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Patient Setting
2.2. Assessment of Alveolar Bone Resorption Using Panoramic Radiographs
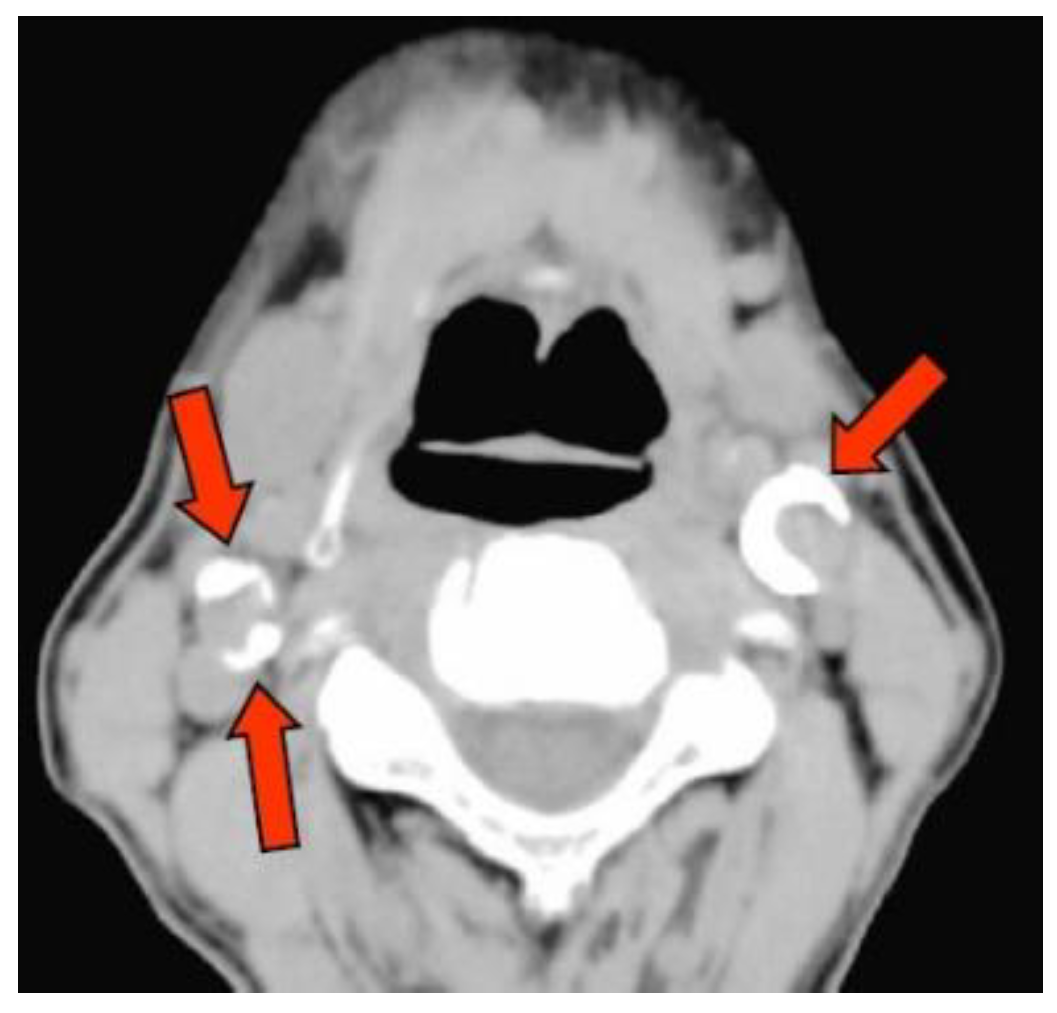
2.3. Detection of CAC on CT
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vital Statistics of Japan—The Latest Trends. 2018. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/jinkou/kakutei18/dl/11_h7.pdf (accessed on 14 September 2020).
- Data of Patient Survey 2017. Available online: https://www.estat.go.jp/statsearch/database?page=1&layout=datalist&toukei=00450022&tstat=000001031167&cycle=7&tclass1=000001124800&tclass2=000001124803&toukei_kind=6&statdisp_id=0003315901&result_page=1 (accessed on 14 September 2020).
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef]
- Dye, B.A. Global periodontal disease epidemiology. Periodontol 2000 2012, 58, 10–25. [Google Scholar] [CrossRef]
- Data of Survey of Dental Diseases 2016. Available online: https://www.mhlw.go.jp/toukei/list/dl/62-28-02.pdf (accessed on 14 September 2020).
- Beck, J.D.; Elter, J.R.; Heiss, G.; Couper, D.; Mauriello, S.M.; Offenbacher, S. Relationship of periodontal disease to carotid artery intima-media wall thickness: The atherosclerosis risk in communities (ARIC) study. Arter. Thromb. Vasc. Biol. 2001, 21, 1816–1822. [Google Scholar] [CrossRef]
- Beck, J.D.; Eke, P.; Lin, D.; Madianos, P.; Couper, D.; Moss, K.; Elter, J.; Heiss, G.; Offenbacher, S. Associations between IgG antibody to oral organisms and carotid intima-medial thickness in community-dwelling adults. Atherosclerosis 2005, 183, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Desvarieux, M.; Schwahn, C.; Volzke, H.; Demmer, R.T.; Ludemann, J.; Kessler, C.; Jacobs, D.R., Jr.; John, U.; Kocher, T. Gender differences in the relationship between periodontal disease, tooth loss, and atherosclerosis. Stroke 2004, 35, 2029–2035. [Google Scholar] [CrossRef] [PubMed]
- Desvarieux, M.; Demmer, R.T.; Rundek, T.; Boden-Albala, B.; Jacobs, D.R., Jr.; Sacco, R.L.; Papapanou, P.N. Periodontal microbiota and carotid intima-media thickness: The Oral Infections and Vascular Disease Epidemiology Study (INVEST). Circulation 2005, 111, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Seinost, G.; Wimmer, G.; Skerget, M.; Thaller, E.; Brodmann, M.; Gasser, R.; Bratschko, R.O.; Pilger, E. Periodontal treatment improves endothelial dysfunction in patients with severe periodontitis. Am. Heart J. 2005, 149, 1050–1054. [Google Scholar] [CrossRef] [PubMed]
- Elter, J.R.; Hinderliter, A.L.; Offenbacher, S.; Beck, J.D.; Caughey, M.; Brodala, N.; Madianos, P.N. The effects of periodontal therapy on vascular endothelial function: A pilot trial. Am. Heart J. 2006, 151, 47. [Google Scholar] [CrossRef]
- Tonetti, M.S.; D’Aiuto, F.; Nibali, L.; Donald, A.; Storry, C.; Parkar, M.; Suvan, J.; Hingorani, A.D.; Vallance, P.; Deanfield, J. Treatment of periodontitis and endothelial function. N. Engl. J. Med. 2007, 356, 911–920. [Google Scholar] [CrossRef]
- Orlandi, M.; Suvan, J.; Petrie, A.; Donos, N.; Masi, S.; Hingorani, A.; Deanfield, J.; D’Aiuto, F. Association between periodontal disease and its treatment, flow-mediated dilatation and carotid intima-media thickness: A systematic review and meta-analysis. Atherosclerosis 2014, 236, 39–46. [Google Scholar] [CrossRef]
- Nicoll, R.; Henein, M.Y. The predictive value of arterial and valvular calcification for mortality and cardiovascular events. Int. J. Cardiol. Heart Vessel. 2014, 3, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Ibrahimi, P.; Jashari, F.; Nicoll, R.; Bajraktari, G.; Wester, P.; Henein, M.Y. Coronary and carotid atherosclerosis: How useful is the imaging? Atherosclerosis 2013, 231, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.S.; Obst, C.; Zehaczek, S.; Geenen, C. Detection of bone loss with different X-ray techniques in periodontal patients. J. Periodontol. 2008, 79, 1141–1149. [Google Scholar] [CrossRef]
- Bassiouny, M.A.; Grant, A.A. The accuracy of the Schei ruler: A laboratory investigation. J. Periodontol. 1975, 46, 748–752. [Google Scholar] [CrossRef]
- Ryden, L.; Buhlin, K.; Ekstrand, E.; de Faire, U.; Gustafsson, A.; Holmer, J.; Kjellstrom, B.; Lindahl, B.; Norhammar, A.; Nygren, A.; et al. Periodontitis Increases the Risk of a First Myocardial Infarction: A Report From the PAROKRANK Study. Circulation 2016, 133, 576–583. [Google Scholar]
- Swets, J.A. Measuring the accuracy of diagnostic systems. Science 1988, 240, 1285–1293. [Google Scholar] [CrossRef]
- Mattila, K.J.; Nieminen, M.S.; Valtonen, V.V.; Rasi, V.P.; Kesaniemi, Y.A.; Syrjala, S.L.; Jungell, P.S.; Isoluoma, M.; Hietaniemi, K.; Jokinen, M.J. Association between dental health and acute myocardial infarction. BMJ 1989, 298, 779–781. [Google Scholar] [CrossRef] [PubMed]
- Bahekar, A.A.; Singh, S.; Saha, S.; Molnar, J.; Arora, R. The prevalence and incidence of coronary heart disease is significantly increased in periodontitis: A meta-analysis. Am. Heart J. 2007, 154, 830–837. [Google Scholar] [CrossRef]
- Lockhart, P.B.; Bolger, A.F.; Papapanou, P.N.; Osinbowale, O.; Trevisan, M.; Levison, M.E.; Taubert, K.A.; Newburger, J.W.; Gornik, H.L.; Gewitz, M.H.; et al. Periodontal disease and atherosclerotic vascular disease: Does the evidence support an independent association?: A scientific statement from the American Heart Association. Circulation 2012, 125, 2520–2544. [Google Scholar] [CrossRef]
- Hujoel, P.P.; Drangsholt, M.; Spiekerman, C.; DeRouen, T.A. Periodontal disease and coronary heart disease risk. JAMA 2000, 284, 1406–1410. [Google Scholar] [CrossRef]
- Peacock, M.E.; Carson, R.E. Frequency of self-reported medical conditions in periodontal patients. J. Periodontol. 1995, 66, 1004–1007. [Google Scholar] [CrossRef]
- Lafon, A.; Pereira, B.; Dufour, T.; Rigouby, V.; Giroud, M.; Bejot, Y.; Tubert-Jeannin, S. Periodontal disease and stroke: A meta-analysis of cohort studies. Eur. J. Neurol. 2014, 21, 1155-e67. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, A.; Miki, M.; Muto, A.; Kubokawa, K.; Migita, K.; Higashi, Y.; Yoshinari, N. Association between oral health and the risk of lacunar infarction in Japanese adults. Gerontology 2013, 59, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Howell, T.H.; Ridker, P.M.; Ajani, U.A.; Hennekens, C.H.; Christen, W.G. Periodontal disease and risk of subsequent cardiovascular disease in U.S. male physicians. J. Am. Coll Cardiol. 2001, 37, 445–450. [Google Scholar] [CrossRef]
- Boillot, A.; Demmer, R.T.; Mallat, Z.; Sacco, R.L.; Jacobs, D.R.; Benessiano, J.; Tedgui, A.; Rundek, T.; Papapanou, P.N.; Desvarieux, M. Periodontal microbiota and phospholipases: The Oral Infections and Vascular Disease Epidemiology Study (INVEST). Atherosclerosis 2015, 242, 418–423. [Google Scholar] [CrossRef]
- Slowik, J.; Wnuk, M.A.; Grzech, K.; Golenia, A.; Turaj, W.; Ferens, A.; Jurczak, A.; Chomyszyn-Gajewska, M.; Loster, B.; Slowik, A. Periodontitis affects neurological deficit in acute stroke. J. Neurol. Sci. 2010, 297, 82–84. [Google Scholar] [CrossRef]
- Holmlund, A.; Lampa, E.; Lind, L. Oral health and cardiovascular disease risk in a cohort of periodontitis patients. Atherosclerosis 2017, 262, 101–106. [Google Scholar] [CrossRef]
- Guidelines for Non-Invasive Vascular Function Test (JCS 2013). 2013. Available online: https://www.j-circ.or.jp/old/guideline/pdf/JCS2013_yamashina_h.pdf (accessed on 14 September 2020).
- Almog, D.M.; Horev, T.; Illig, K.A.; Green, R.M.; Carter, L.C. Correlating carotid artery stenosis detected by panoramic radiography with clinically relevant carotid artery stenosis determined by duplex ultrasound. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2002, 94, 768–773. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, O.S.; Chung, H.J.; Kim, Y.J.; Kweon, S.S.; Lee, Y.H.; Shin, M.H.; Yoon, S.J. The prevalence and correlation of carotid artery calcification on panoramic radiographs and peripheral arterial disease in a population from the Republic of Korea: The Dong-gu study. Dentomaxillofac Radiol. 2013, 42, 29725099. [Google Scholar] [CrossRef]
- Garoff, M.; Johansson, E.; Ahlqvist, J.; Jaghagen, E.L.; Arnerlov, C.; Wester, P. Detection of calcifications in panoramic radiographs in patients with carotid stenoses >/=50%. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2014, 117, 385–391. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, O.S.; Chung, H.J.; Kim, Y.J.; Kweon, S.S.; Lee, Y.H.; Shin, M.H.; Yoon, S.J. The correlation of carotid artery calcification on panoramic radiographs and determination of carotid artery atherosclerosis with ultrasonography. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2014, 118, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, A.H.; Lande, A. Panoramic radiographic identification of carotid arterial plaques. Oral. Surg. Oral. Med. Oral. Pathol. 1981, 52, 102–104. [Google Scholar] [CrossRef]
- Cohen, S.N.; Friedlander, A.H.; Jolly, D.A.; Date, L. Carotid calcification on panoramic radiographs: An important marker for vascular risk. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2002, 94, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Bilgin Çetin, M.; Sezgin, Y.; Nisancı Yilmaz, M.N.; Köseoğlu Seçgin, C. Assessment of carotid artery calcifications on digital panoramic radiographs and their relationship with periodontal condition and cardiovascular risk factors. Int. Dent. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Paju, S.; Pietiäinen, M.; Liljestrand, J.M.; Lahdentausta, L.; Salminen, A.; Kopra, E.; Mäntylä, P.; Buhlin, K.; Hörkkö, S.; Sinisalo, J.; et al. Carotid artery calcification in panoramic radiographs associates with oral infections and mortality. Int. Endod. J. 2020. [Google Scholar] [CrossRef]
- Thanakun, S.; Pornprasertsuk-Damrongsri, S.; Izumi, Y. C-reactive protein levels and the association of carotid artery calcification with tooth loss. Oral. Dis. 2017, 23, 69–77. [Google Scholar] [CrossRef]
- Otawara, H.; Jinbu, Y.; Shinozaki, Y.; Hayasaka, J.; Tsuchiya, Y.; Itoh, H.; Noguchi, T.; Mori, Y.; Iida, Y.; Katsumata, A. Carotid calcification in panoramic Radiography. J. Jpn.Oral. Med. 2015, 21, 33–37. [Google Scholar] [CrossRef]
- Anderson, K.M.; Odell, P.M.; Wilson, P.W.; Kannel, W.B. Cardiovascular disease risk profiles. Am. Heart J. 1991, 121, 293–298. [Google Scholar] [CrossRef]
- Kaimenyi, J.T.; Ashley, F.P. Assessment of bone loss in periodontitis from panoramic radiographs. J. Clin. Periodontol. 1988, 15, 170–174. [Google Scholar] [CrossRef]
- Rohlin, M.; Kullendorff, B.; Ahlqwist, M.; Henrikson, C.O.; Hollender, L.; Stenström, B. Comparison between panoramic and periapical radiography in the diagnosis of periapical bone lesions. Dento Maxillo Facial Radiol. 1989, 18, 151–155. [Google Scholar] [CrossRef]
- Kiliç, A.R.; Efeoglu, E.; Yilmaz, S.; Orgun, T. The relationship between probing bone loss and standardized radiographic analysis. Periodontal. Clin. Investig. 1998, 20, 25–32. [Google Scholar] [PubMed]
- Eickholz, P.; Hausmann, E. Accuracy of radiographic assessment of interproximal bone loss in intrabony defects using linear measurements. Eur. J. Oral. Sci. 2000, 108, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Graetz, C.; Plaumann, A.; Wiebe, J.-F.; Springer, C.; Sälzer, S.; Dörfer, C.E. Periodontal probing versus radiographs for the diagnosis of furcation involvement. J. Periodontol. 2014, 85, 1371–1379. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age | ||||||||
|---|---|---|---|---|---|---|---|---|
| 30–39 y (n = 2) | 40–49 y (n = 32) | 50–59 y (n = 65) | 60–69 y (n = 85) | 70–79 y (n = 82) | 80–89 y (n = 24) | 90–95 y (n = 5) | p-Value | |
| Male | 1 (50.0) | 16 (50.0) | 40 (61.5) | 54 (63.5) | 42 (51.2) | 11 (45.8) | 3 (60.0) | 0.40 |
| Female | 1 (50.0) | 6 (50.0) | 25 (38.5) | 31 (36.5) | 40 (48.8) | 13 (54.2) | 2 (40.0) | |
| Calcification | 0 (0.0) | 2 (6.3) | 11 (16.9) | 28 (32.9) | 55 (67.1) | 20 (83.3) | 5 (100.0) | <0.001 |
| Not Calcification | 2 (100.0) | 30 (93.8) | 54 (83.1) | 57 (67.1) | 27 (32.9) | 4 (16.7) | 0 (0.0) | |
| Hypertension Yes | 0 (0.0) | 3 (9.4) | 14 (21.5) | 31 (36.5) | 37 (45.1) | 15 (62.5) | 4 (80.0) | 0.15 |
| No | 2 (100.0) | 29 (90.6) | 51 (78.5) | 54 (63.5) | 45 (54.9) | 9 (37.5) | 1 (20.0) | |
| Dyslipidemia Yes | 0 (0.0) | 1 (3.1) | 10 (15.4) | 12 (14.1) | 10 (12.2) | 2 (8.3) | 1 (20.0) | 0.68 |
| No | 2 (100.0) | 31 (96.9) | 55 (84.6) | 73 (85.9) | 72 (87.8) | 22 (91.7) | 4 (80.0) | |
| Diabetes mellitus Yes | 0 (0.0) | 1 (3.1) | 6 (9.2) | 14 (16.5) | 13 (15.9) | 2 (8.3) | 2 (40.0) | 0.58 |
| No | 2 (100.0) | 31 (96.9) | 59 (90.8) | 71 (83.5) | 69 (84.1) | 22 (91.7) | 3 (60.0) | |
| Osteoporosis Yes | 0 (0.0) | 0 (0.0) | 2 (3.1) | 1 (16.5) | 13 (15.9) | 2 (8.3) | 1 (20.0) | 0.02 |
| No | 2 (100.0) | 32 (100.0) | 63 (96.9) | 84 (83.5) | 69 (84.1) | 22 (91.7) | 4 (80.0) | |
| Cancer Yes | 0 (0.0) | 1 (3.1) | 3 (9.2) | 14 (1.2) | 7 (8.5) | 5 (20.8) | 0 (0.0) | 0.38 |
| No | 2 (100.0) | 31 (96.9) | 62 (90.8) | 71 (98.8) | 75 (91.5) | 19 (79.2) | 5 (100.0) | |
| Number of present teeth | 27.5 ± 0.7 | 25.0 ± 4.6 | 23.9 ± 4.3 | 21.9 ± 5.7 | 17.7 ± 7.8 | 14.5 ± 6.5 | 11.4 ± 8.8 | <0.001 a |
| 1–9 | 0 (0.0) | 1 (3.1) | 1 (1.5) | 3 (3.5) | 16 (19.5) | 7 (29.2) | 2 (40.0) | 0.002 |
| 10–19 | 0 (0.0) | 3 (9.4) | 7 (10.8) | 20 (23.5) | 22 (26.8) | 9 (37.5) | 1 (20.0) | |
| ≥20 | 2 (100.0) | 28 (87.5) | 57 (87.7) | 62 (72.9) | 44 (53.7) | 8 (33.3) | 2 (40.0) | |
| ABL | 19.8 ± 12.4 | 17.2 ± 7.7 | 19.4 ± 9.7 | 21.1 ± 9.3 | 29.5 ± 12.3 | 29.6 ± 9.2 | 35.7 ± 7.4 | <0.001 a |
| ≤20% | 1 (50.0) | 26 (81.3) | 44 (67.7) | 49 (57.6) | 19 (23.2) | 5 (20.8) | 0 (0.0) | <0.001 |
| >20%, ≤34% | 1 (50.0) | 5 (15.6) | 15 (23.1) | 28 (32.9) | 38 (46.3) | 11 (45.8) | 2 (40.0) | |
| >34% | 0 (0.0) | 1 (3.1) | 6 (9.2) | 8 (9.4) | 25 (30.5) | 8 (33.3) | 3 (60.0) | |
| Group C | Group NC | p-Value | |
|---|---|---|---|
| (n = 121) Male: 68, Female: 53 | (n = 174) Male: 99, Female: 75 | ||
| Age (Year) | 72.0 ± 9.7 | 59.4 ± 10.3 | <0.001 a |
| 30–49 y | 2 (5.9) | 32 (94.1) | <0.001 |
| 50–59 y | 11 (16.9) | 54 (83.1) | |
| 60–69 y | 28 (32.9) | 57 (67.1) | |
| 70–79 y | 55 (67.1) | 27 (32.9) | |
| 80–95 y | 25 (86.2) | 4 (13.8) | |
| Male | 68 (56.2) | 99 (56.9) | 0.91 |
| Hypertension | 69 (57.0) | 35 (20.1) | <0.001 |
| Dyslipidemia | 14 (11.6) | 22 (12.6) | 0.78 |
| Osteoporosis | 12 (9.9) | 4 (2.3) | 0.004 |
| Diabetes Mellitus | 19 (15.7) | 19 (10.9) | 0.23 |
| Cancer | 13 (10.7) | 19 (10.9) | 0.96 |
| Number of Present Teeth | 17.1 ± 7.9 | 23.3 ± 4.8 | <0.001 a |
| 1–9 | 27 (90.0) | 3 (10.0) | <0.001 |
| 10–19 | 31 (50.0) | 31 (50.0) | |
| ≥20 | 63 (31.0) | 140 (69.0) | |
| ABL (%) | 32.7 ± 9.7 | 17.2 ± 7.0 | <0.001 a |
| ≤20% | 8 (5.6) | 136 (94.4) | <0.001 |
| >20%, ≤34% | 67 (67.0) | 33 (33.0) | |
| >34% | 46 (90.2) | 5 (9.8) |
| Partial Regression Coefficient | Standard Error | Odds Ratio (95% CI) | p-Value | ||
|---|---|---|---|---|---|
| Step 1 | ABL | 0.231 | 0.026 | 1.260 (1.197–1.325) | <0.001 |
| constant | −5.744 | 0.614 | 0.003 | <0.001 | |
| Step 2 | Age | 0.099 | 0.020 | 1.105 (1.062–1.149) | <0.001 |
| ABL | 0.214 | 0.028 | 1.239 (1.173–1.308) | <0.001 | |
| Constant | −11.916 | 1.572 | 0.000 | <0.001 | |
| Step 3 | Age | 0.092 | 0.021 | 1.096 (1.051–1.143) | <0.001 |
| Hypertension | 1.321 | 0.389 | 3.748 (1.748–8.037) | 0.001 | |
| ABL | 0.210 | 0.028 | 1.233 (1.167–1.303) | <0.001 | |
| Constant | −11.883 | 1.658 | 0.000 | <0.001 | |
| Step 1 | ABL ≤20% | 1.000 | <0.001 | ||
| >20%, ≤34% | 3.541 | 0.421 | 34.515 (15.112–78.833) | <0.001 | |
| >34% | 5.052 | 0.595 | 156.400 (48.722–502.053) | <0.001 | |
| Constant | −5.744 | 0.614 | 0.003 | <0.001 | |
| Step 2 | Age 30–49 y | 1.000 | <0.001 | ||
| 50–59 y | 0.872 | 0.924 | 2.392 (0.391–14.617) | 0.345 | |
| 60–69 y | 1.937 | 0.883 | 6.940 (1.128–39.206) | 0.028 | |
| 70–79 y | 2.598 | 0.882 | 13.437 (2.387–75.654) | 0.003 | |
| 80–95 y | 4.188 | 1.102 | 65.902 (7.606–571.037) | <0.001 | |
| ABL ≤20% | 1.000 | <0.001 | |||
| >20%, ≤34% | 3.367 | 0.460 | 28.988 (11.759–71.456) | <0.001 | |
| >34% | 4.747 | 0.643 | 115.220 (32.686–406.154) | <0.001 | |
| Constant | −4.705 | 0.905 | 0.009 | <0.001 | |
| Step 3 | Age 30–49 y | 1.000 | <0.001 | ||
| 50–59 y | 0.534 | 0.934 | 1.705 (0.273–10.638) | 0.568 | |
| 60–69 y | 1.498 | 0.893 | 4.471 (0.776–25.758) | 0.094 | |
| 70–79 y | 2.194 | 0.889 | 8.974 (1.571–51.274) | 0.014 | |
| 80–95 y | 3.747 | 1.130 | 42.410 (4.626–388.797) | 0.001 | |
| Hypertension | 1.026 | 0.399 | 2.790 (1.275–6.104) | 0.001 | |
| ABL ≤20% | 1.000 | <0.001 | |||
| >20%, ≤34% | 3.164 | 0.466 | 23.676 (9.494–59.035) | <0.001 | |
| >34% | 4.717 | 0.649 | 111.848 (31.322–399.398) | <0.001 | |
| Constant | −11.883 | 1.658 | 0.000 | <0.001 | |
| Covariance | AUROC | Standard Error | p-Value (95% CI) |
|---|---|---|---|
| ABL | 0.932 | 0.014 | <0.001 (0.904–0.960) |
| Age | 0.815 | 0.025 | <0.001 (0.767–0.864) |
| Hypertension | 0.685 | 0.032 | <0.001 (0.621–0.748) |
| Number of Present Teeth | 0.749 | 0.029 | <0.001 (0.692–0.806) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dewake, N.; Ishioka, Y.; Uchida, K.; Taguchi, A.; Higashi, Y.; Yoshida, A.; Yoshinari, N. Association between Carotid Artery Calcification and Periodontal Disease Progression in Japanese Men and Women: A Cross-Sectional Study. J. Clin. Med. 2020, 9, 3365. https://doi.org/10.3390/jcm9103365
Dewake N, Ishioka Y, Uchida K, Taguchi A, Higashi Y, Yoshida A, Yoshinari N. Association between Carotid Artery Calcification and Periodontal Disease Progression in Japanese Men and Women: A Cross-Sectional Study. Journal of Clinical Medicine. 2020; 9(10):3365. https://doi.org/10.3390/jcm9103365
Chicago/Turabian StyleDewake, Nanae, Yasuaki Ishioka, Keiichi Uchida, Akira Taguchi, Yukihito Higashi, Akihiro Yoshida, and Nobuo Yoshinari. 2020. "Association between Carotid Artery Calcification and Periodontal Disease Progression in Japanese Men and Women: A Cross-Sectional Study" Journal of Clinical Medicine 9, no. 10: 3365. https://doi.org/10.3390/jcm9103365
APA StyleDewake, N., Ishioka, Y., Uchida, K., Taguchi, A., Higashi, Y., Yoshida, A., & Yoshinari, N. (2020). Association between Carotid Artery Calcification and Periodontal Disease Progression in Japanese Men and Women: A Cross-Sectional Study. Journal of Clinical Medicine, 9(10), 3365. https://doi.org/10.3390/jcm9103365