Cystocele Repair by a Modified Surgical Technique of Bilateral Pubococcygeus Plication: Long-Term Surgical and Functional Results




Abstract
1. Introduction
2. Experimental Section
2.1. Data Acquisition
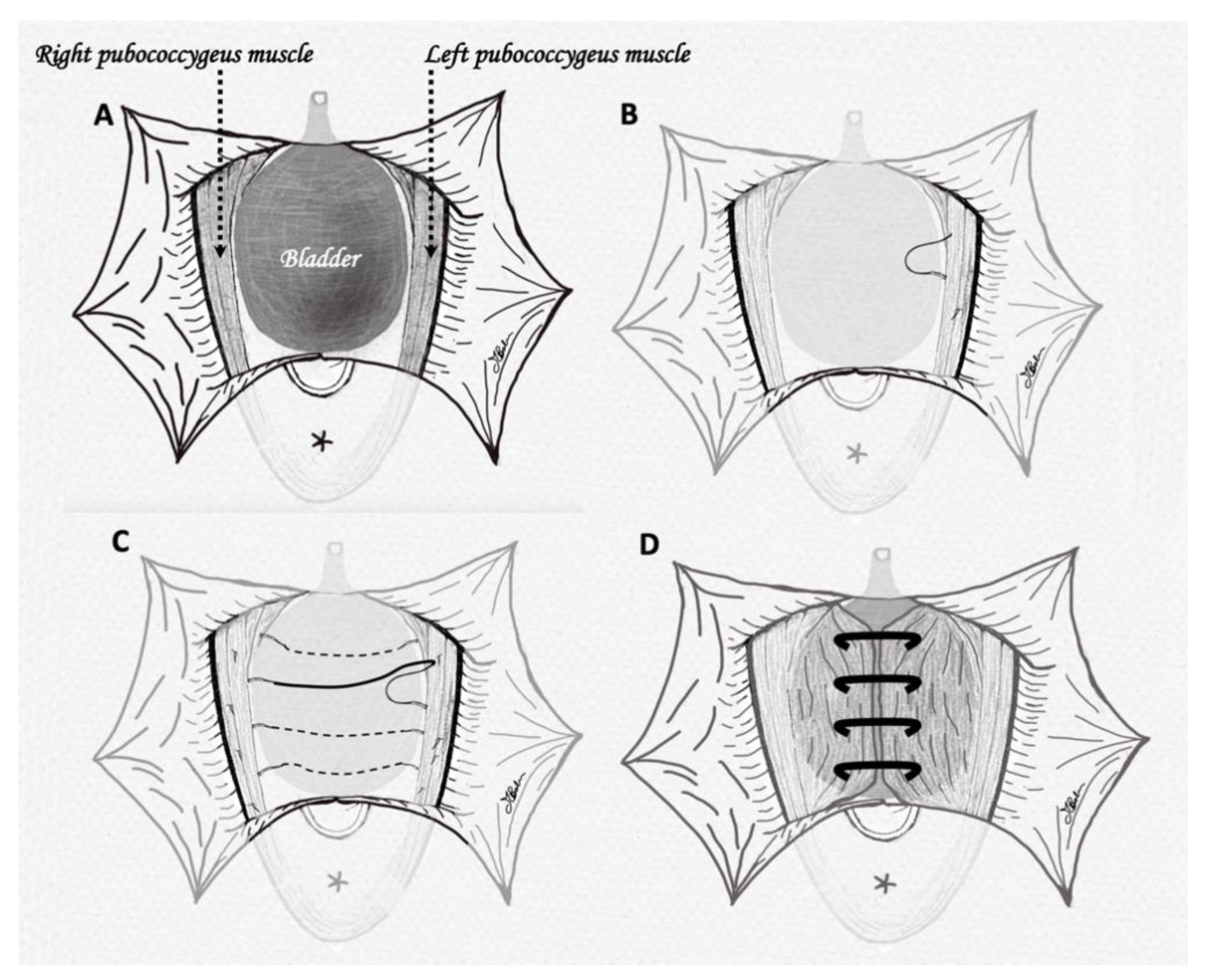
2.2. Surgical Technique
3. Results
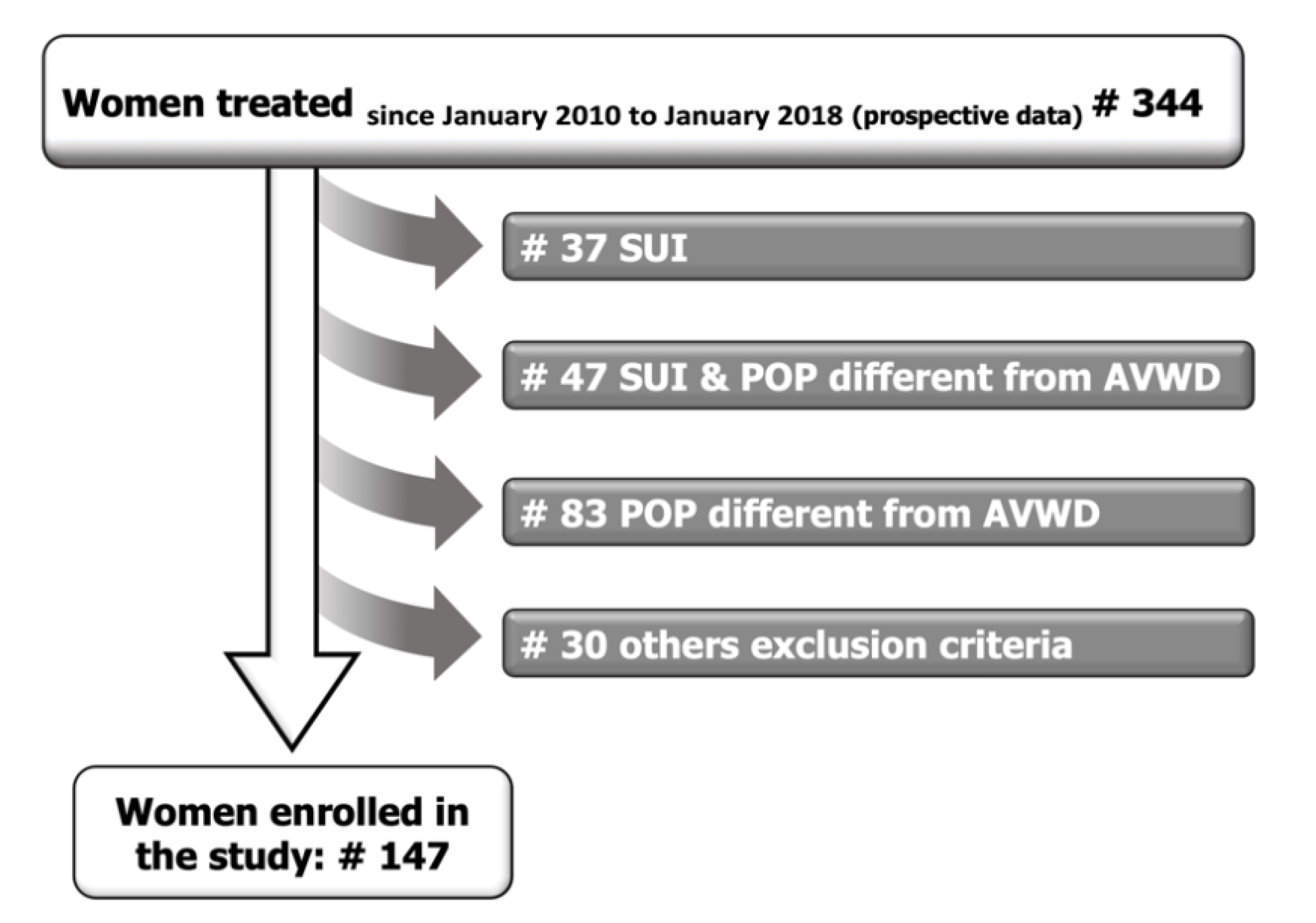
3.1. Demographics and Indication for Surgery
3.2. Preoperative Functional and Urodynamic Characteristics
3.3. Outcomes
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shek, K.L.; Dietz, H.P. Assessment of pelvic organ prolapse: A review. Ultrasound Obstet. Gynecol. 2016, 48, 681–692. [Google Scholar] [CrossRef] [PubMed]
- Srikrishna, S.; Robinson, D.; Cardozo, L. Validation of the Patient Global Impression of Improvement (PGI-I) for urogenital prolapse. Int. Urogynecol. J. 2009, 21, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Coyne, K.S.; Matza, L.S.; Kopp, Z.; Abrams, P. The Validation of the Patient Perception of Bladder Condition (PPBC): A Single-Item Global Measure for Patients with Overactive Bladder. Eur. Urol. 2006, 49, 1079–1086. [Google Scholar] [CrossRef] [PubMed]
- Filocamo, M.T.; Serati, M.; Marzi, V.L.; Giannantoni, A.; Milanesi, M.; Pietropaolo, A.; Polledro, P.; Gentile, B.; Maruccia, S.; Fornia, S.; et al. The Female Sexual Function Index (FSFI): Linguistic Validation of the Italian Version. J. Sex. Med. 2014, 11, 447–453. [Google Scholar] [CrossRef]
- Balzarro, M.; Rubilotta, E.; Goss, C.; Costantini, E.; Artibani, W.; Sand, P. Counseling in urogynecology: A difficult task, or simply good surgeon–patient communication? Int. Urogynecol. J. 2018, 29, 943–948. [Google Scholar] [CrossRef]
- Handel, L.N.; Frenkl, T.L.; Kim, Y.H. Results of Cystocele Repair: A Comparison of Traditional Anterior Colporrhaphy, Polypropylene Mesh and Porcine Dermis. J. Urol. 2007, 178, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Walter, S.; Olesen, K.P.; Hald, T.; Jensen, H.K.; Pedersen, P.H. Urodynamic Evaluation after Vaginal Repair and Colposuspension. Br. J. Urol. 1982, 54, 377–380. [Google Scholar] [CrossRef]
- Balzarro, M.; Rubilotta, E.; Porcaro, A.B.; Trabacchin, N.; Sarti, A.; Cerruto, M.A.; Siracusano, S.; Artibani, W. Long-term follow-up of anterior vaginal repair: A comparison among colporrhaphy, colporrhaphy with reinforcement by xenograft, and mesh. Neurourol. Urodyn. 2017, 37, 278–283. [Google Scholar] [CrossRef]
- Glazener, C.M.; Breeman, S.; Elders, A.; Hemming, C.; Cooper, K.G.; Freeman, R.M.; Smith, A.R.; Reid, F.; Hagen, S.; Montgomery, I.; et al. Mesh, graft, or standard repair for women having primary transvaginal anterior or posterior compartment prolapse surgery: Two parallel-group, multicentre, randomised, controlled trials (PROSPECT). Lancet 2017, 389, 381–392. [Google Scholar] [CrossRef]
- Weber, A.M.; Walters, M.D.; Piedmonte, M.R.; Ballard, L.A. Anterior colporrhaphy: A randomized trial of three surgical techniques. Am. J. Obstet. Gynecol. 2001, 185, 1299–1306. [Google Scholar] [CrossRef]
- Sand, P.K.; Koduri, S.; Lobel, R.W.; Winkler, H.A.; Tomezsko, J.; Culligan, P.; Goldberg, R. Prospective randomized trial of polyglactin 910 mesh to prevent recurrence of cystoceles and rectoceles. Am. J. Obstet. Gynecol. 2001, 184, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Allègre, L.; Callewaert, G.; Alonso, S.; Cornille, A.; Fernandez, H.; Eglin, G.; De Tayrac, R. Long-term outcomes of a randomized controlled trial comparing trans-obturator vaginal mesh with native tissue repair in the treatment of anterior vaginal wall prolapse. Int. Urogynecol. J. 2019, 31, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Palmerola, R.; Rosenblum, N. Prolapse Repair Using Non-synthetic Material: What is the Current Standard? Curr. Urol. Rep. 2019, 20, 70. [Google Scholar] [CrossRef] [PubMed]
- Colombo, M.; Vitobello, D.; Proietti, F.; Milani, R. Randomised comparison of Burch colposuspension versus anterior colporrhaphy in women with stress urinary incontinence and anterior vaginal wall prolapse. BJOG Int. J. Obstet. Gynaecol. 2000, 107, 544–551. [Google Scholar] [CrossRef]
- Haylen, B.T.; Maher, C.F.; Barber, M.D.; Camargo, S.; Dandolu, V.; Digesu, G.A.; Goldman, H.B.; Huser, M.; Milani, A.L.; Moran, P.A.; et al. An International Urogynecological Association (IUGA) / International Continence Society (ICS) Joint Report on the Terminology for Female Pelvic Organ Prolapse (POP). Neurourol. Urodyn. 2016, 35, 137–168. [Google Scholar] [CrossRef]
- Urogynecologic Surgical Mesh Implants. Available online: https://www.fda.gov/medical-devices/implants-and-prosthetics/urogynecologic-surgical-mesh-implants (accessed on 8 August 2020).
- Dmochowski, R.R.; Zimmern, P.; Ganabathi, K.; Sirls, L.; Leach, G.E. Role of the four-corner bladder neck suspension to correct stress incontinence with a mild to moderate cystocele. Urology 1997, 49, 35–40. [Google Scholar] [CrossRef]
- Cormio, L.; Mancini, V.; Liuzzi, G.; Lucarelli, G.; Carrieri, G. Cystocele Repair by Autologous Rectus Fascia Graft: The Pubovaginal Cystocele Sling. J. Urol. 2015, 194, 721–727. [Google Scholar] [CrossRef]
- Paparella, P.; Ercoli, A.; Groutz, A.; Falconi, G.; Marturano, M.; Paparella, R.; Ortiz, O.C. Clinical and urodynamic effects of anterior colporraphy and approximation of pubococcygeus muscles in patients with severe cystocele. Arch. Gynecol. Obstet. 2004, 271, 195–199. [Google Scholar] [CrossRef]
- Chen, K.; Wang, F.; Liu, S.; Wu, X.; Xu, L.; Zhang, D. In situ reduction of silver nanoparticles by sodium alginate to obtain silver-loaded composite wound dressing with enhanced mechanical and antimicrobial property. Int. J. Biol. Macromol. 2020, 148, 501–509. [Google Scholar] [CrossRef]
- Balzarro, M.; Rubilotta, E.; Trabacchin, N.; Soldano, A.; Cerrato, C.; Migliorini, F.; Mancini, V.; Pastore, A.L.; Carbone, A.; Cormio, L.; et al. Early and Late Efficacy on Wound Healing of Silver Nanoparticle Gel in Males after Circumcision. J. Clin. Med. 2020, 9, 1822. [Google Scholar] [CrossRef]
- Foster, R.T.; Barber, M.D.; Parasio, M.F.R.; Walters, M.D.; Weidner, A.C.; Amundsen, C.L. A prospective assessment of overactive bladder symptoms in a cohort of elderly women who underwent transvaginal surgery for advanced pelvic organ prolapse. Am. J. Obstet. Gynecol. 2007, 197, 82.e1–82.e4. [Google Scholar] [CrossRef] [PubMed]
- Malanowska, E.; Starczewski, A.; Bielewicz, W.; Balzarro, M. Assessment of Overactive Bladder after Laparoscopic Lateral Suspension for Pelvic Organ Prolapse. Biomed Res. Int. 2019, 2019, 9051963. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N° Pts. | 147 |
|---|---|
| POP-Q stage, % (n) | |
| 2 | 49% (72/147) |
| 3 | 51% (75/147) |
| Ba mean (SD) | 1.2 (1.0) |
| Aa mean (SD) | 1.4 (1.2) |
| Follow-Up, Months Mean | 82.4 Months (Range 24–120) | |
|---|---|---|
| Objective success | ||
| POP-Q <2 stage, % (n) | 89.8% (132/147) | |
| Aa mean (SD) | −2.4 (0.9) | |
| Ba mean (SD) | −2.1 (1.1) | |
| Recurrences, % (n) | Pre-operative POP-Q stage | Follow-up POP-Q stage |
| Tot 10.2% (15/147) | ||
| 11.1% (8/72) | 2 | 2 |
| 8.0% (6/75) | 3 | 2 |
| 1.3% (1/75) | 3 | 3 |
| Patients Affected by OAB Symptoms | p Value | |
|---|---|---|
| OAB before surgery | 36.7% (54/147) | <0.05 * |
| OAB after surgery | ||
| In overall population | 14.3 (21/147) | |
| In OAB patients | 38.9% (21/54) | |
| De Novo OAB | 3.2% (3/93) | |
| OAB-screener | ||
| Before surgery | 23.1 (8.8) | <0.05 * |
| After surgery | 13.1 (5.9) |
| PRE | POST | p Value | |
|---|---|---|---|
| FSFI | Mean (SD) | Mean (SD) | |
| Total score | 17.1 (4.1) | 18.2 (4.5) | >0.05 * |
| Desire | 2.5 (0.9) | 3.2 (1.0) | >0.05 * |
| Arousal | 2.3 (1.4) | 2.9 (1.6) | >0.05 * |
| Lubrication | 2.6 (1.6) | 2.9 (1.9) | >0.05 * |
| Orgasm | 2.5 (1.3) | 2.7 (1.9) | >0.05 * |
| Satisfaction | 2.2 (1.5) | 3.1 (2.0) | <0.05 * |
| Pain | 2.6 (1.6) | 3.4 (2.1) | >0.05 * |
| Complications | ||
| Intraoperative bladder injury | 2 (1.4%) | |
| Hematoma | 3 (2.0%) | |
| Pain | 2 (1.4%) | |
| Clavien-Dindo Classification | ||
| Grade I | None | |
| Grade II | None | |
| Grade IIIa | 1 | Percutaneous drainage of hematoma |
| Grade IIIb | 1 | Surgical (trans vaginal) drainage of hematoma and blood transfusion |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balzarro, M.; Rubilotta, E.; Antonelli, A. Cystocele Repair by a Modified Surgical Technique of Bilateral Pubococcygeus Plication: Long-Term Surgical and Functional Results. J. Clin. Med. 2020, 9, 3318. https://doi.org/10.3390/jcm9103318
Balzarro M, Rubilotta E, Antonelli A. Cystocele Repair by a Modified Surgical Technique of Bilateral Pubococcygeus Plication: Long-Term Surgical and Functional Results. Journal of Clinical Medicine. 2020; 9(10):3318. https://doi.org/10.3390/jcm9103318
Chicago/Turabian StyleBalzarro, Matteo, Emanuele Rubilotta, and Alessandro Antonelli. 2020. "Cystocele Repair by a Modified Surgical Technique of Bilateral Pubococcygeus Plication: Long-Term Surgical and Functional Results" Journal of Clinical Medicine 9, no. 10: 3318. https://doi.org/10.3390/jcm9103318
APA StyleBalzarro, M., Rubilotta, E., & Antonelli, A. (2020). Cystocele Repair by a Modified Surgical Technique of Bilateral Pubococcygeus Plication: Long-Term Surgical and Functional Results. Journal of Clinical Medicine, 9(10), 3318. https://doi.org/10.3390/jcm9103318