Trajectories of Hospitalization in COVID-19 Patients: An Observational Study in France

 , , and
, , and 
Abstract
1. Introduction
2. Experimental Section
2.1. Data
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stoecklin, S.B.; Rolland, P.; Silue, Y.; Mailles, A.; Campese, C.; Simondon, A.; Mechain, M.; Meurice, L.; Nguyen, M.; Bassi, C.; et al. First cases of coronavirus disease 2019 (COVID-19) in France: Surveillance, investigations and control measures, January 2020. Eurosurveillance 2020, 25, 2000094. [Google Scholar]
- Boelle, P.-Y.; Souty, C.; Launay, T.; Guerrisi, C.; Turbelin, C.; Behillil, S.; Enouf, V.; Poletto, C.; Lina, B.; Van Der Werf, S.; et al. Excess cases of influenza-like illnesses synchronous with coronavirus disease (COVID-19) epidemic, France, March 2020. Eurosurveillance 2020, 25, 2000326. [Google Scholar] [CrossRef]
- Schoenfeld, D. Survival methods, including those using competing risk analysis, are not appropriate for intensive care unit outcome studies. Crit. Care 2005, 10, 103. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lescure, F.-X.; Bouadma, L.; Nguyen, D.; Parisey, M.; Wicky, P.-H.; Behillil, S.; Gaymard, A.; Bouscambert-Duchamp, M.; Donati, F.; Le Hingrat, Q.; et al. Clinical and virological data of the first cases of COVID-19 in Europe: A case series. Lancet Infect. Dis. 2020, 20, 697–706. [Google Scholar] [CrossRef]
- Argenziano, M.G.; Bruce, S.L.; Slater, C.L.; Tiao, J.R.; Baldwin, M.R.; Barr, R.G.; Chang, B.P.; Chau, K.H.; Choi, J.J.; Gavin, N.; et al. Characterization and clinical course of 1000 patients with coronavirus disease 2019 in New York: Retrospective case series. BMJ 2020, 369, m1996. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Riquelme, R.; Torres, A.; El-Ebiary, M.; Mensa, J.; Estruch, R.; Ruiz, M.; Angrill, J.; Soler, N. Community-acquired Pneumonia in the Elderly: Clinical and nutritional aspects. Am. J. Respir. Crit. Care Med. 1997, 156, 1908–1914. [Google Scholar] [CrossRef]
- Poissy, J.; Goutay, J.; Caplan, M.; Parmentier, E.; Duburcq, T.; Lassalle, F.; Jeanpierre, E.; Rauch, A.; Labreuche, J.; Susen, S.; et al. Pulmonary Embolism in Patients With COVID-19: Awareness of an Increased Prevalence. Circulation 2020, 142, 184–186. [Google Scholar] [CrossRef]
- Rauch, A.; Labreuche, J.; Lassalle, F.; Goutay, J.; Caplan, M.; Charbonnier, L.; Rohn, A.; Jeanpierre, E.; Dupont, A.; Duhamel, A.; et al. Coagulation biomarkers are independent predictors of increased oxygen requirements in COVID-19. J. Thromb. Haemost. 2020. ahead of print. [Google Scholar] [CrossRef]
- The RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, M.I.; Mortensen, E.M.; Rello, J.; Brody, J.; Anzueto, A. Late admission to the ICU in patients with community-acquired pneumonia is associated with higher mortality. Chest 2010, 137, 552–557. [Google Scholar] [CrossRef]
- Flaatten, H.; Van Heerden, V.; Jung, C.; Beil, M.; Leaver, S.; Rhodes, A.; Guidet, B.; Delange, D.W. The good, the bad and the ugly: Pandemic priority decisions and triage. J. Med. Ethics 2020. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Fuhrman, C.; Bonmarin, I.; Bitar, D.; Cardoso, T.; Duport, N.; Herida, M.; Isnard, H.; Guidet, B.; Mimoz, O.; Richard, J.C.M.; et al. Adult intensive-care patients with 2009 pandemic influenza A(H1N1) infection. Epidemiol. Infect. 2010, 139, 1202–1209. [Google Scholar] [CrossRef]
- Rees, E.M.; Nightingale, E.S.; Jafari, Y.; Waterlow, N.R.; Clifford, S.; Pearson, C.A.B.; CMMID Working Group; Jombart, T.; Procter, S.R.; Knight, G.M. COVID-19 length of hospital stay: A systematic review and data synthesis. BMC Med. 2020, 18, 270. [Google Scholar] [CrossRef]
- Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators; Cavalcanti, A.B.; Suzumura, E.A.; Laranjeira, L.N.; Paisani, D.D.M.; Damiani, L.P.; Guimarães, H.P.; Romano, E.R.; Regenga, M.D.M.; Taniguchi, L.N.T.; et al. Effect of Lung Recruitment and Titrated Positive End-Expiratory Pressure (PEEP) vs Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA 2017, 318, 1335–1345. [Google Scholar]
- Gupta, S.; Hayek, S.S.; Wang, W.; Chan, L.; Mathews, K.S.; Melamed, M.L.; Brenner, S.K.; Leonberg-Yoo, A.; Schenck, E.J.; Radbel, J.; et al. Factors Associated With Death in Critically Ill Patients With Coronavirus Disease 2019 in the US. JAMA Intern. Med. 2020. ahead of print. [Google Scholar] [CrossRef]
- Wood, R.M.; McWilliams, C.J.; Thomas, M.J.; Bourdeaux, C.P.; Vasilakis, C. COVID-19 scenario modelling for the mitigation of capacity-dependent deaths in intensive care. Health Care Manag. Sci. 2020, 23, 315–324. [Google Scholar] [CrossRef]
- Iannaccone, S.; Alemanno, F.; Houdayer, E.; Brugliera, L.; Castellazzi, P.; Cianflone, D.; Meloni, C.; Ambrosio, A.; Mortini, P.; Spina, A.; et al. COVID-19 rehabilitation units are twice as expensive as regular rehabilitation units. J. Rehabil. Med. 2020, 52, jrm00073. [Google Scholar] [CrossRef]
- Biased and Unbiased Estimation of the Average Lengths of Stay in Intensive Care Units in the COVID-19 Pandemic. Available online: https://www.medrxiv.org/content/10.1101/2020.04.21.20073916v2 (accessed on 14 September 2020).
- McLachlan, G.J.; McGiffin, D.C. On the role of finite mixture models in survival analysis. Stat. Methods Med. Res. 1994, 3, 211–226. [Google Scholar] [CrossRef] [PubMed]
- Lewnard, J.A.; Liu, V.X.; Jackson, M.L.; Schmidt, M.A.; Jewell, B.L.; Flores, J.P.; Jentz, C.; Northrup, G.R.; Mahmud, A.; Reingold, A.L.; et al. Incidence, clinical outcomes, and transmission dynamics of severe coronavirus disease 2019 in California and Washington: Prospective cohort study. BMJ 2020, 369, m1923. [Google Scholar] [CrossRef] [PubMed]
- Imam, Z.; Odish, F.; Gill, I.; O’Connor, D.; Armstrong, J.; Vanood, A.; Ibironke, O.; Hanna, A.; Ranski, A.; Halalau, A. Older age and comorbidity are independent mortality predictors in a large cohort of 1305 COVID-19 patients in Michigan, United States. J. Intern. Med. 2020, 288, 469–476. [Google Scholar] [CrossRef]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Al-Samkari, H.; Leaf, R.S.K.; Dzik, W.H.; Carlson, J.C.T.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID-19 and coagulation: Bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef]
- Patel, M.; Gangemi, A.; Marron, R.; Chowdhury, J.; Yousef, I.; Zheng, M.; Mills, N.; Tragesser, L.; Giurintano, J.; Gupta, R.; et al. Retrospective analysis of high flow nasal therapy in COVID-19-related moderate-to-severe hypoxaemic respiratory failure. BMJ Open Respir. Res. 2020, 7, e000650. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Gemelli against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Age Group (n) | Overall (n = 1321) | ||
|---|---|---|---|---|
| 18–65 (n = 523) | 66–80 (n = 400) | >80 (n = 398) | ||
| Male (% (n)) | 57% (300) | 60% (232) | 44% (168) | 55% (700) |
| Age (years) (median [IQR]) | 52.0 [43.9, 59.0] | 72.0 [68.0, 75.8] | 86.0 [83.0, 90.0] | 69.0 [55.8, 82.0] |
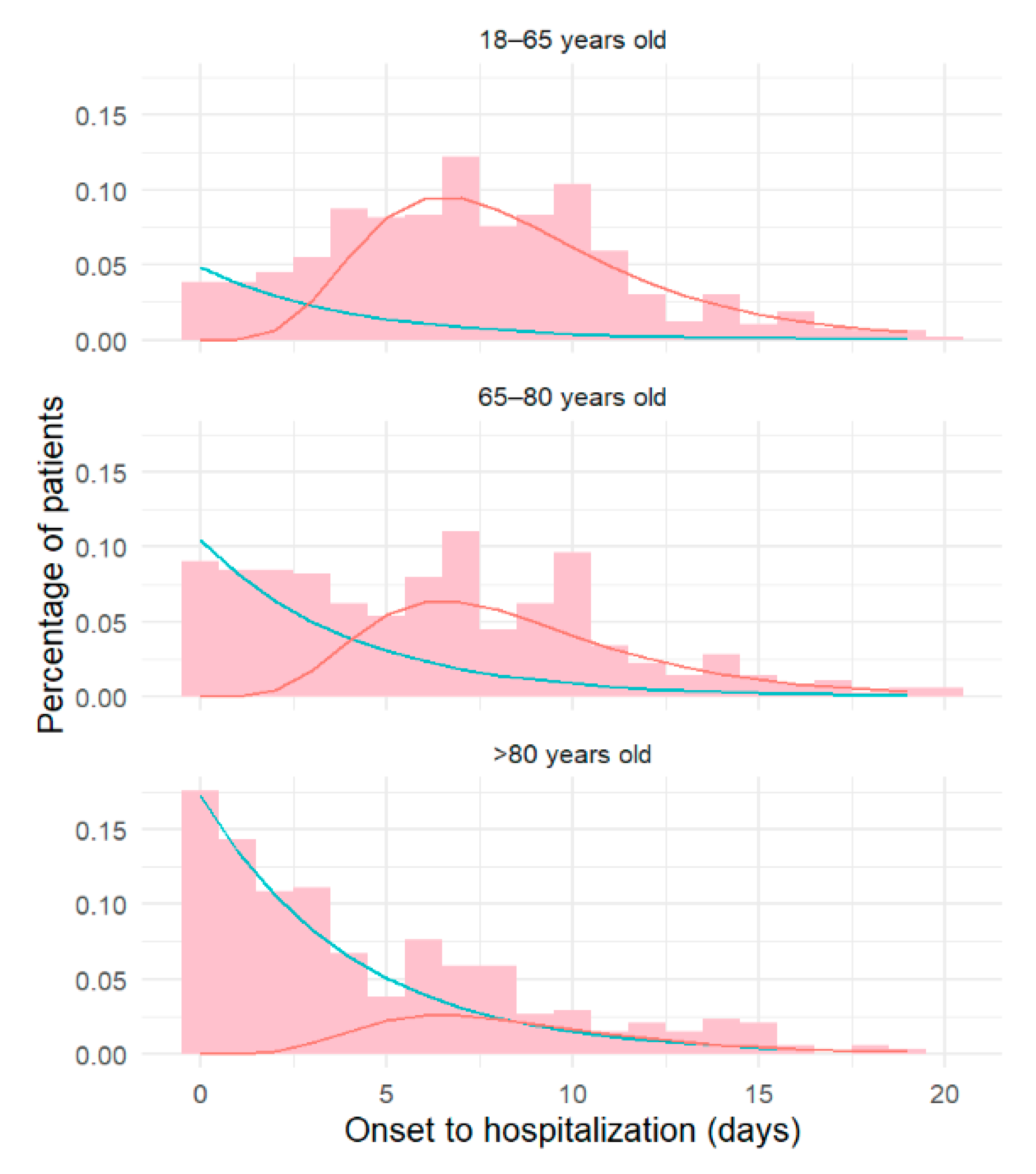
| Time from onset to hospitalization (days) (median [IQR]) | 8 [5, 11] | 7 [3, 10] | 4 [2, 8] | 7 [3, 10] |
| ICU < 24 h after admission (% (n)) | 17% (91) | 20% (78) | 6% (23) | 14% (192) |
| Age | ||||
|---|---|---|---|---|
| Trajectory Characteristics | 18–65 | 66–80 | >80 | Overall |
| (n = 523) | (n = 400) | (n = 398) | (n = 1321) | |
| Overall length of stay | 10 [6, 16] | 14 [9, 24] | 13 [8, 21] | 12 [7, 20] |
| Death (%) | 9 | 20 | 38 | 20 |
| Time to death (days) | 53 [31, 91] | 16 [9, 28] | 10 [6, 17] | 14 [8, 25] |
| Time to discharge (days) | 8 [5, 13] | 14 [9, 22] | 14 [9, 23] | 12 [7, 19] |
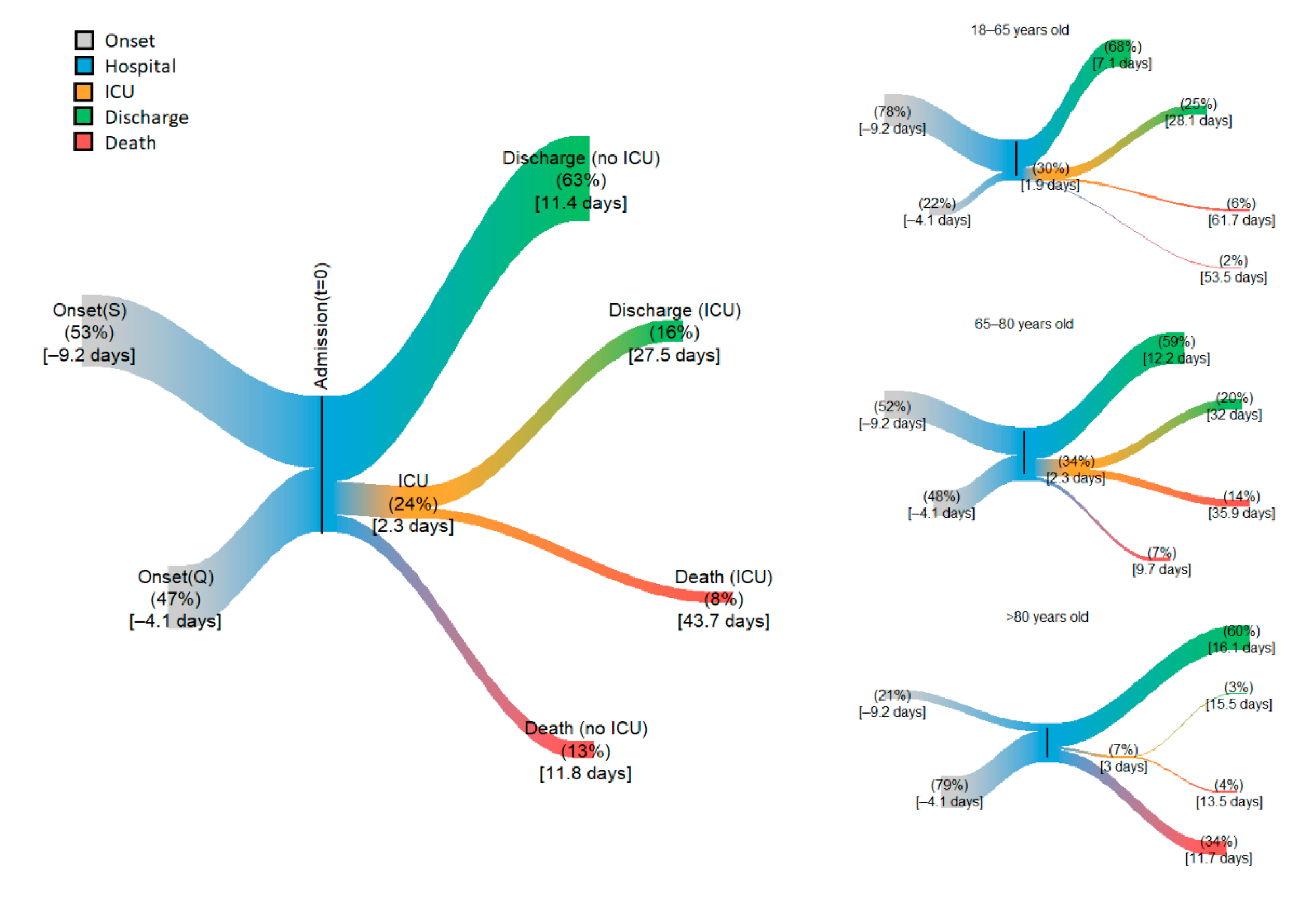
| ICU (%) | 30 | 34 | 7 | 24 |
| Time to ICU (days) | 1 [0, 2] | 1 [0, 3] | 1 [0, 3] | 1 [0, 2] |
| Time in the ICU (days) | 20 [10, 39] | 22 [11, 42] | 9 [5, 18] | 20 [10, 39] |
| Death in the ICU (%) | 18 | 42 | 62 | 33 |
| Time to death (days) | 40 [22, 75] | 23 [13, 44] | 9 [5, 16] | 27 [14, 52] |
| Discharge from the ICU (%) | 82 | 58 | 38 | 67 |
| Time to discharge (days) | 17 [9, 34] | 20.0 [10, 38] | 10 [5, 19] | 17 [9, 33] |
| No ICU (%) | 70 | 66 | 93 | 75 |
| Time in the hospital (days) | 6 [4, 10] | 9 [6, 15] | 11 [7, 17] | 9 [6, 14] |
| Death in hospital (%) | 3 | 11 | 36 | 13 |
| Time to death (days) | 41 [25, 67] | 8 [5, 12] | 9 [6, 15] | 9 [6, 15] |
| Discharge from hospital (%) | 97 | 89 | 64 | 63 |
| Time to discharge (days) | 6 [4, 9] | 10 [7, 15] | 13 [9, 20] | 9 [6, 14] |
| Period (n) | ||||
|---|---|---|---|---|
| >15 March (n = 158) | 15–30 March (n = 646) | 1–15 April (n = 370) | 1–15 April (n = 147) | |
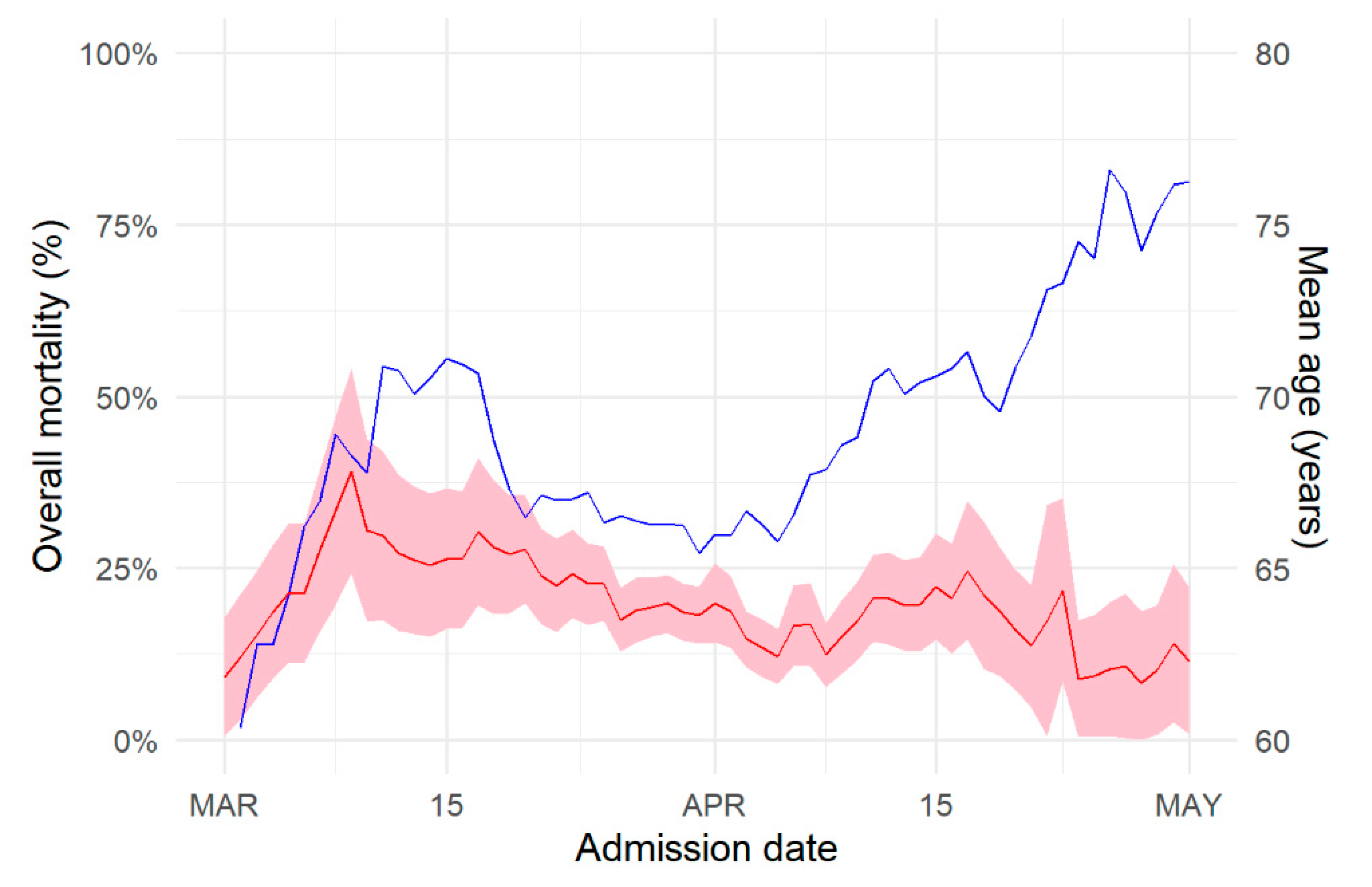
| Time from onset to hospitalization (days) (median [IQR]) | 5 [2, 9] | 6 [3, 9] | 6 [2, 10] | 4 [2, 8] |
| ICU < 24 h after admission (% (n)) | 20 (31) | 25 (159) | 24 (89) | 13 (19) |
| Length of stay (median [IQR]) | 13 [8, 21] | 11 [7, 18] | 12 [7, 20] | 17 [10, 27] |
| Death (%) | 22% | 21% | 17% | 12% |
| Time to discharge (median [IQR]) | 13 [8, 21] | 10 [6, 17] | 12 [7, 19] | 19 [12, 32] |
| Time to death (median [IQR]) | 13 [8, 21] | 14 [8, 24] | 13 [8, 22] | 8 [5, 12] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boëlle, P.-Y.; Delory, T.; Maynadier, X.; Janssen, C.; Piarroux, R.; Pichenot, M.; Lemaire, X.; Baclet, N.; Weyrich, P.; Melliez, H.; et al. Trajectories of Hospitalization in COVID-19 Patients: An Observational Study in France. J. Clin. Med. 2020, 9, 3148. https://doi.org/10.3390/jcm9103148
Boëlle P-Y, Delory T, Maynadier X, Janssen C, Piarroux R, Pichenot M, Lemaire X, Baclet N, Weyrich P, Melliez H, et al. Trajectories of Hospitalization in COVID-19 Patients: An Observational Study in France. Journal of Clinical Medicine. 2020; 9(10):3148. https://doi.org/10.3390/jcm9103148
Chicago/Turabian StyleBoëlle, Pierre-Yves, Tristan Delory, Xavier Maynadier, Cécile Janssen, Renaud Piarroux, Marie Pichenot, Xavier Lemaire, Nicolas Baclet, Pierre Weyrich, Hugues Melliez, and et al. 2020. "Trajectories of Hospitalization in COVID-19 Patients: An Observational Study in France" Journal of Clinical Medicine 9, no. 10: 3148. https://doi.org/10.3390/jcm9103148
APA StyleBoëlle, P.-Y., Delory, T., Maynadier, X., Janssen, C., Piarroux, R., Pichenot, M., Lemaire, X., Baclet, N., Weyrich, P., Melliez, H., Meybeck, A., Lanoix, J.-P., & Robineau, O. (2020). Trajectories of Hospitalization in COVID-19 Patients: An Observational Study in France. Journal of Clinical Medicine, 9(10), 3148. https://doi.org/10.3390/jcm9103148