Characterizing Body Image Distortion and Bodily Self-Plasticity in Anorexia Nervosa via Visuo-Tactile Stimulation in Virtual Reality

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Pre-Experimental Session
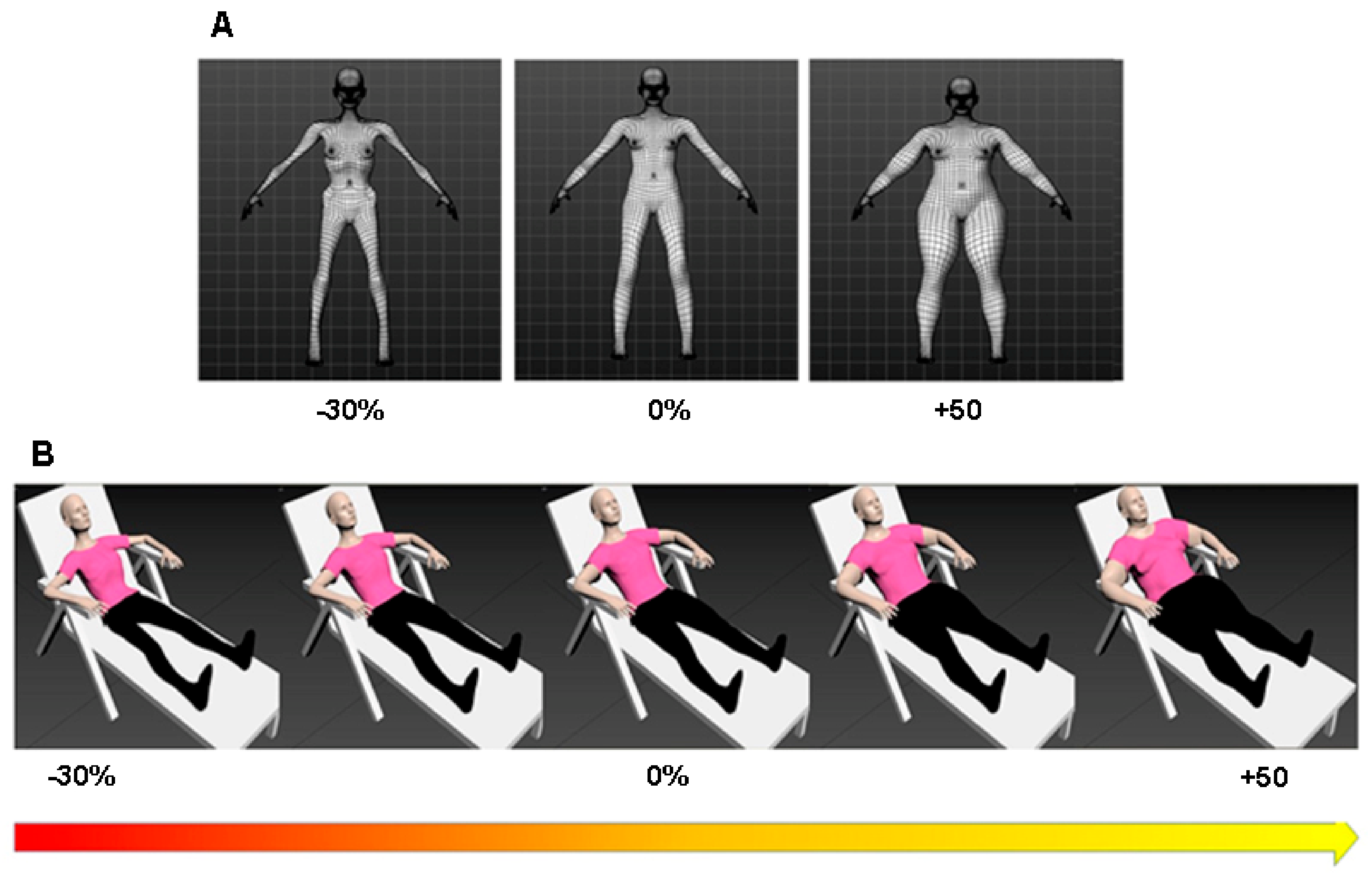
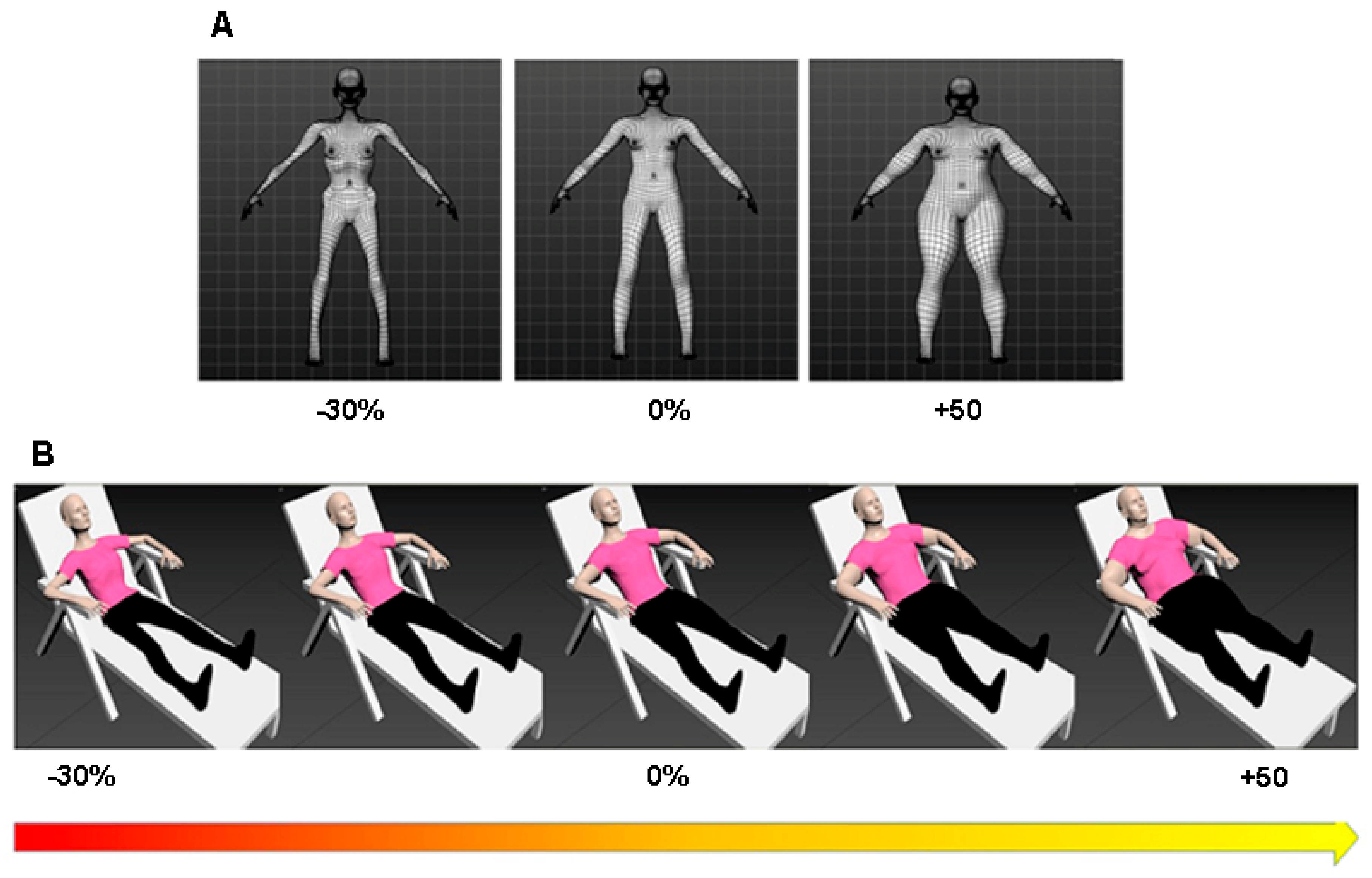
Avatars Modelling
2.4. Experimental Session
2.4.1. Avatar Selection Task
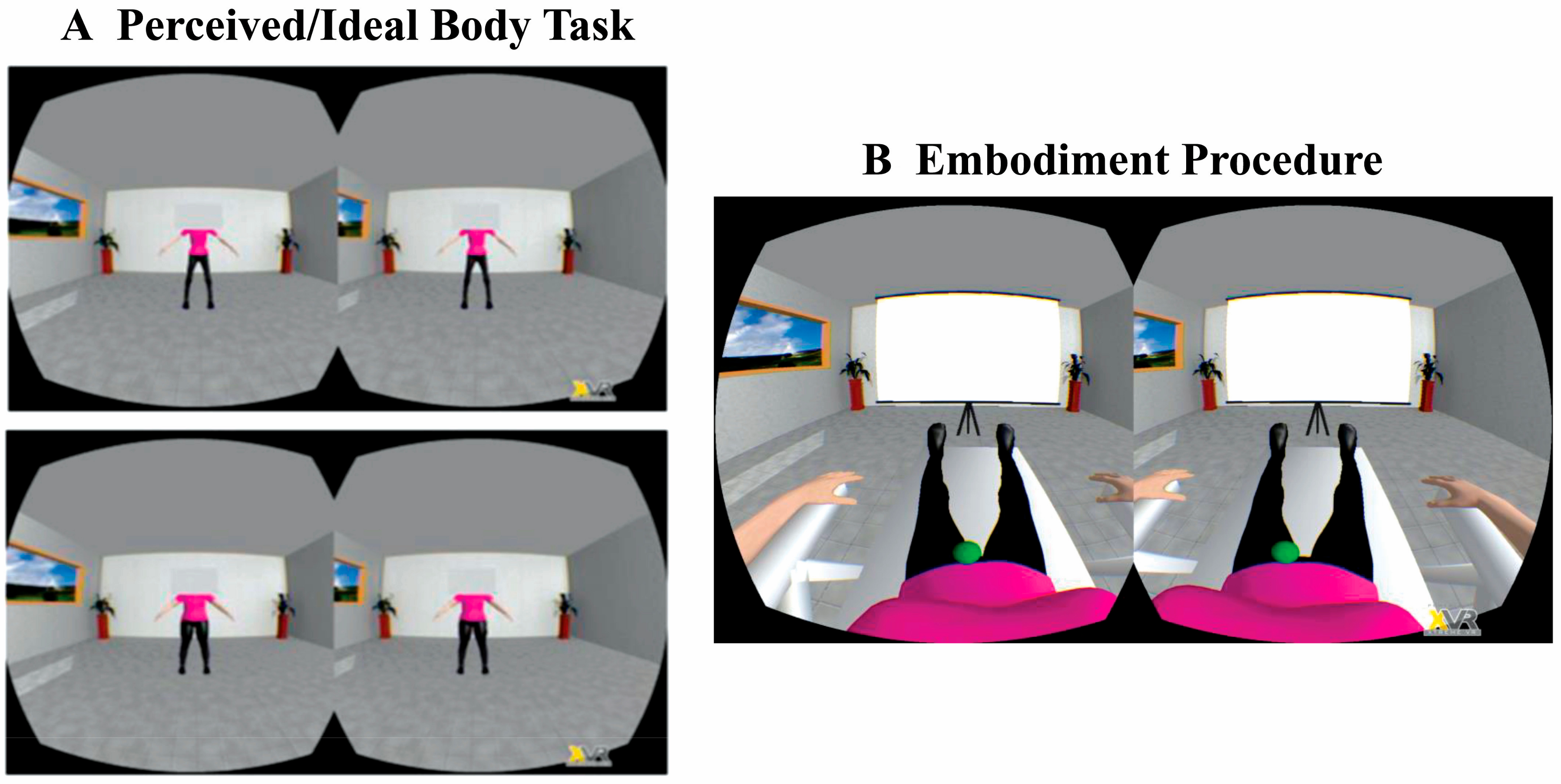
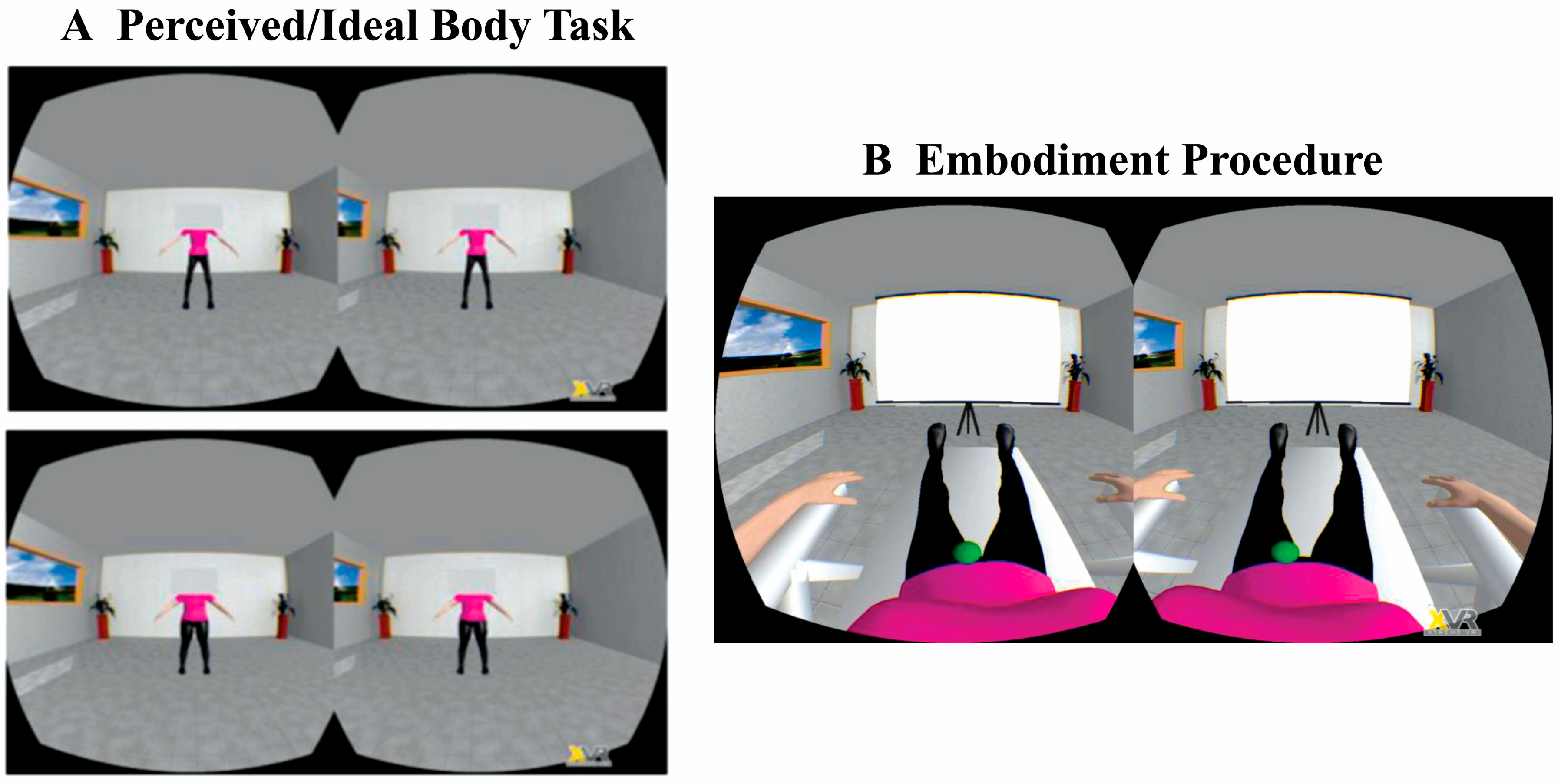
2.4.2. Perceived and Ideal Body Tasks: Body Dissatisfaction
2.4.3. Embodiment Procedure
2.4.4. Explicit and Implicit Measures of Embodiment
2.4.5. Measure of Emotional Response Induced by Embodiment
2.4.6. Similarity and Attractiveness Ratings of the Avatars
3. Results
3.1. Baseline Measures
3.2. Explicit and Implicit Measures of Embodiment
3.3. Body Dissatisfaction after Embodiment
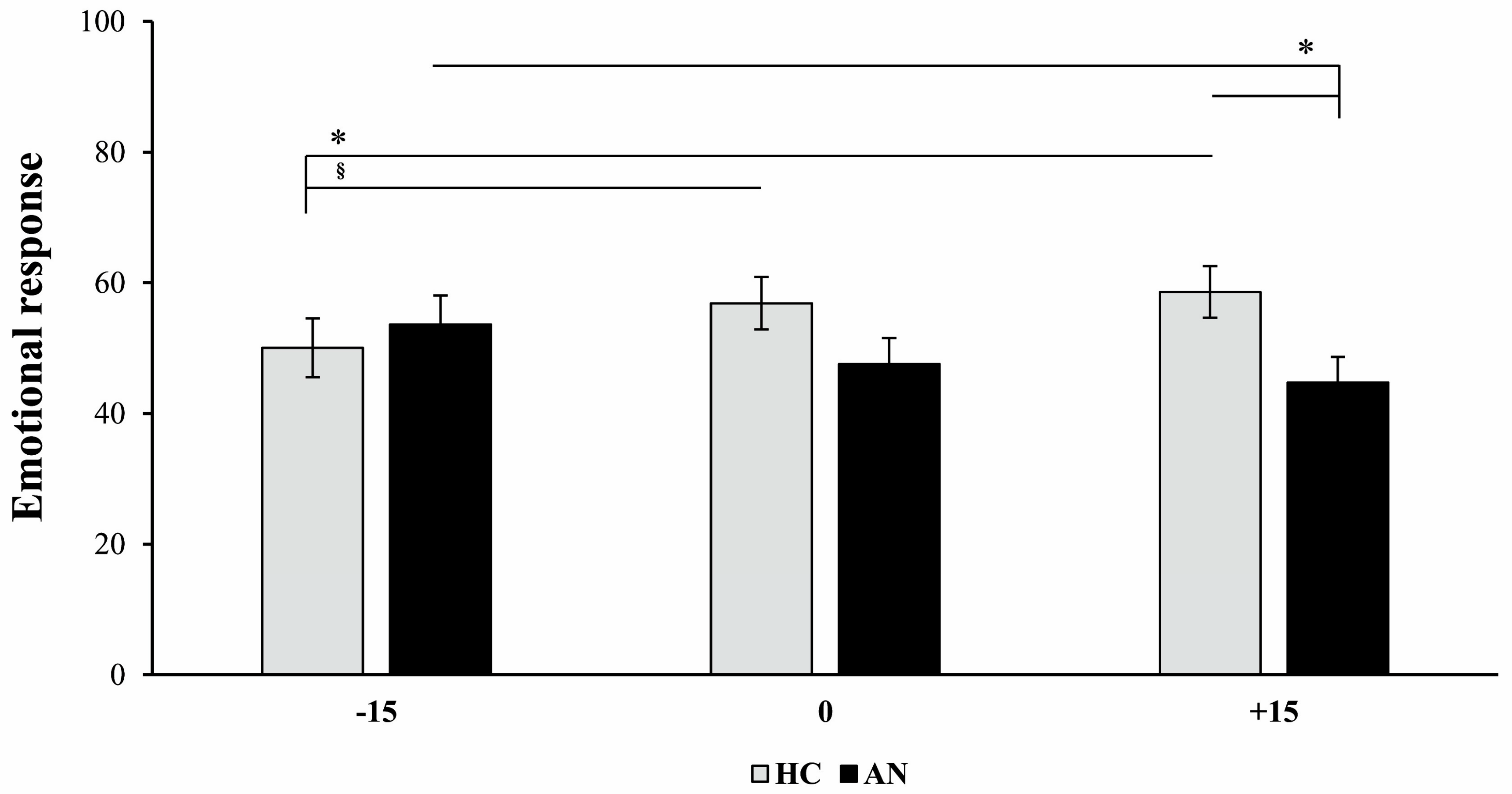
3.4. Emotional Response after Embodiment
3.5. Avatars’ Similarity and Attractiveness Ratings
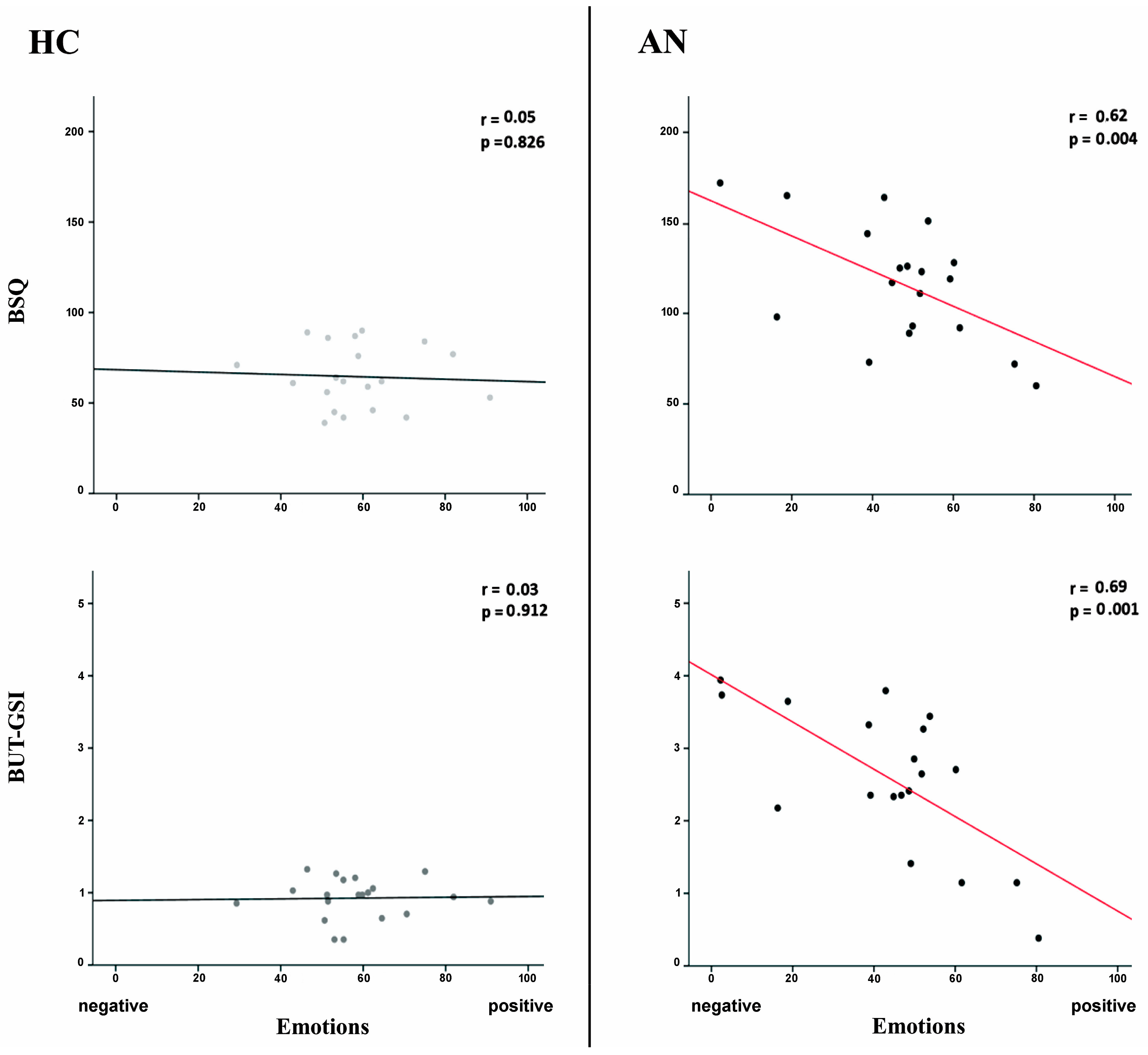
3.6. Correlations between +15% Avatar Emotional Response and Symptoms Severity
4. Discussion
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Gaudio, S.; Brooks, S.J.; Riva, G. Nonvisual multisensory impairment of body perception in anorexia nervosa: A systematic review of neuropsychological studies. PLoS ONE 2014, 9, e110087. [Google Scholar] [CrossRef] [PubMed]
- Arcelus, J. Mortality Rates in Patients with Anorexia Nervosa and Other Eating Disorders. Arch. Gen. Psychiatry 2011, 68, 724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornelissen, K.K.; Bester, A.; Cairns, P.; Tovée, M.J.; Cornelissen, P.L. The influence of personal BMI on body size estimations and sensitivity to body size change in anorexia spectrum disorders. Body Image 2015, 13, 75–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrell, C.; Lee, M.; Shafran, R. Assessment of body size estimation: A review. Eur. Eat. Disord. Rev. 2005, 13, 75–88. [Google Scholar] [CrossRef]
- Urgesi, C.; Fornasari, L.; Canalaz, F.; Perini, L.; Cremaschi, S.; Faleschini, L.; Thyrion, E.Z.; Zuliani, M.; Balestrieri, M.; Fabbro, F.; et al. Impaired configural body processing in anorexia nervosa: Evidence from the body inversion effect. Br. J. Psychol. 2014, 105, 486–508. [Google Scholar] [CrossRef]
- Cash, T.F. Body image: Past, present, and future. Body Image 2004, 1, 1–5. [Google Scholar] [CrossRef]
- Peelen, M.V.; Downing, P.E. The neural basis of visual body perception. Nat. Rev. Neurosci. 2007, 8, 636–648. [Google Scholar] [CrossRef]
- Gandolfo, M.; Downing, P.E. Causal Evidence for Expression of Perceptual Expectations in Category-Selective Extrastriate Regions. Curr. Biol. 2019, 29, 1–5. [Google Scholar] [CrossRef]
- Moreau, Q.; Pavone, E.F.; Aglioti, S.M.; Candidi, M. Theta synchronization over occipito-temporal cortices during visual perception of body parts. Eur. J. Neurosci. 2018, 48, 2826–2835. [Google Scholar] [CrossRef] [Green Version]
- Moreau, Q.; Parrotta, E.; Era, V.; Martelli, M.; Candidi, M. Role of the occipito-temporal Theta rhythm in hand visual identification. J. Neurophysiol. 2019. [Epub ahead of print]. [Google Scholar] [CrossRef]
- Cash, T.F.; Deagle, E.A. The nature and extent of body-image disturbances in anorexia nervosa and bulimia nervosa: A meta-analysis. Int. J. Eat. Disord. 1997, 22, 107–125. [Google Scholar] [CrossRef]
- Gardner, R.M.; Brown, D.L. Body size estimation in anorexia nervosa: A brief review of findings from 2003 through 2013. Psychiatry Res. 2014, 219, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Keel, P.K.; Dorer, D.J.; Franko, D.L.; Jackson, S.C.; Herzog, D.B. Postremission predictors of relapse in women with eating disorders. Am. J. Psychiatry 2005, 162, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mölbert, S.C.; Klein, L.; Thaler, A.; Mohler, B.J.; Brozzo, C.; Martus, P.; Karnath, H.O.; Zipfel, S.; Giel, K.E. Depictive and metric body size estimation in anorexia nervosa and bulimia nervosa: A systematic review and meta-analysis. Clin. Psychol. Rev. 2017, 57, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Piryankova, I.V.; Wong, H.Y.; Linkenauger, S.A.; Stinson, C.; Longo, M.R.; Bülthoff, H.H.; Mohler, B.J. Owning an overweight or underweight body: Distinguishing the physical, experienced and virtual body. PLoS ONE 2014, 9, e103428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berlucchi, G.; Aglioti, S.M. The body in the brain revisited. Exp. Brain Res. 2010, 200, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Porciello, G.; Bufalari, I.; Minio-Paluello, I.; Di Pace, E.; Aglioti, S.M. The ‘Enfacement’ illusion: A window on the plasticity of the self. Cortex 2018, 104, 261–275. [Google Scholar] [CrossRef]
- Botvinick, M.; Cohen, J. Rubber hands “feel” touch that eyes see. Nature 1998, 391, 756. [Google Scholar] [CrossRef]
- Lenggenhager, B.; Tadi, T.; Metzinger, T.; Blanke, O. Video ergo sum: Manipulating bodily self-consciousness. Science 2007, 317, 1096–1099. [Google Scholar] [CrossRef] [Green Version]
- Sforza, A.; Bufalari, I.; Haggard, P.; Aglioti, S.M. My face in yours: Visuo-tactile facial stimulation influences sense of identity. Soc. Neurosci. 2010, 5, 148–162. [Google Scholar] [CrossRef]
- Bufalari, I.; Sforza, A.L.; Di Russo, F.; Mannetti, L.; Aglioti, S.M. Malleability of the self: Electrophysiological correlates of the enfacement illusion. Sci. Rep. 2019, 9, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Fusaro, M.; Tieri, G.; Aglioti, S. Influence of cognitive stance and physical perspective on subjective and autonomic reactivity to observed pain and pleasure: An immersive virtual reality study. Conscious. Cogn. 2019, 67, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Porciello, G.; Holmes, B.S.; Liuzza, M.T.; Crostella, F.; Aglioti, S.M.; Bufalari, I. Interpersonal Multisensory Stimulation reduces the overwhelming distracting power of self-gaze. Sci. Rep. 2014, 4, 6669. [Google Scholar] [CrossRef] [PubMed]
- Mino-Paluello, I.; Porciello, G.; Gandolfo, M.; Boukarras, S.; Aglioti, S.M. The Enfacement illusion boosts facial mimicry. Cortex 2019, 123, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Maselli, A.; Slater, M. The building blocks of the full body ownership illusion. Front. Hum. Neurosci. 2013, 7, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Hoort, B.; Guterstam, A.; Ehrsson, H.H. Being barbie: The size of one’s own body determines the perceived size of the world. PLoS ONE 2011, 6, e20195. [Google Scholar] [CrossRef] [Green Version]
- Normand, J.M.; Giannopoulos, E.; Spanlang, B.; Slater, M. Multisensory stimulation can induce an illusion of larger belly size in immersive virtual reality. PLoS ONE 2011, 6, e16128. [Google Scholar] [CrossRef] [Green Version]
- Preston, C.; Ehrsson, H.H. Illusory changes in body size modulate body satisfaction in a way that is related to non-clinical eating disorder psychopathology. PLoS ONE 2014, 9, e85773. [Google Scholar] [CrossRef] [Green Version]
- Eshkevari, E.; Rieger, E.; Longo, M.R.; Haggard, P.; Treasure, J. Increased plasticity of the bodily self in eating disorders. Psychol. Med. 2012, 42, 819–828. [Google Scholar] [CrossRef] [Green Version]
- Keizer, A.; Smeets, M.A.M.; Postma, A.; van Elburg, A.; Dijkerman, H.C. Does the experience of ownership over a rubber hand change body size perception in anorexia nervosa patients? Neuropsychologia 2014, 62, 26–37. [Google Scholar] [CrossRef]
- Keizer, A.; Van Elburg, A.; Helms, R.; Dijkerman, H.C. A virtual reality full body illusion improves body image disturbance in anorexia nervosa. PLoS ONE 2016, 11, e0163921. [Google Scholar] [CrossRef] [PubMed]
- Sepúlveda, A.R.; Botella, J.; León, J.A. Body-image disturbance in eating disorders: A meta-analysis. Psychol. Spain 2002, 6, 83–95. [Google Scholar]
- Tieri, G.; Tidoni, E.; Pavone, E.F.; Aglioti, S.M. Body visual discontinuity affects feeling of ownership and skin conductance responses. Sci. Rep. 2015, 5, 17139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tieri, G.; Gioia, A.; Scandola, M.; Pavone, E.F.; Aglioti, S.M. Visual appearance of a virtual upper limb modulates the temperature of the real hand: A thermal imaging study in Immersive Virtual Reality. Eur. J. Neurosci. 2017, 45, 1141–1151. [Google Scholar] [CrossRef] [PubMed]
- De Haan, A.M.; Van Stralen, H.E.; Smit, M.; Keizer, A.; Van der Stigchel, S.; Dijkerman, H.C. No consistent cooling of the real hand in the rubber hand illusion. Acta Psychol. (Amst.) 2017, 179, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Mohr, H.M.; Röder, C.; Zimmermann, J.; Hummel, D.; Negele, A.; Grabhorn, R. Body image distortions in bulimia nervosa: Investigating body size overestimation and body size satisfaction by fMRI. Neuroimage 2011, 56, 1822–1831. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorder, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Garner, D. Eating Disorder Inventory-2: Professional Manual; Psychological Assessment Resources Inc: Odessa, Finland, 1991. [Google Scholar]
- Cooper, P.; Taylor, M.; Sc, B.; Cooper, Z.; Fairburn, C.G. The Development and Validation of the Body Shape Questionnaire. Int. J. Eat. Disord. 1987, 6, 485–494. [Google Scholar] [CrossRef]
- Cuzzolaro, M.; Vetrone, G.; Marano, G.; Garfinkel, P.E. The Body Uneasiness Test (BUT): Development and validation of a new body image assessment scale. Eat. Weight Disord. 2006, 11, 1–13. [Google Scholar] [CrossRef]
- Henderson, M.; Freeman, C.P.L. A Self-rating Scale for Bulimia the “BITE”. Br. J. Psychiatry 1987, 150, 18–24. [Google Scholar] [CrossRef] [Green Version]
- Derogatis, L.R. Symptom Checklist-90-R: Administration, Scoring & Procedure Manual for the Revised Version of the SCL-90; National Computer Systems: Minneapolis, MN, USA, 1994. [Google Scholar]
- Slater, M.; Spanlang, B.; Sanchez-Vives, M.V.; Blanke, O. First person experience of body transfer in virtual reality. PLoS ONE 2010, 5, e10564. [Google Scholar] [CrossRef] [Green Version]
- Apps, M.A.J.; Tsakiris, M. The free-energy self: A predictive coding account of self-recognition. Neurosci. Biobehav. Rev. 2014, 44, 85–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bufalari, I.; Lenggenhager, B.; Porciello, G.; Holmes, B.S.; Aglioti, S.M. Enfacing others but only if they are nice to you. Front. Behav. Neurosci. 2014, 8, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Love, J.; Selker, R.; Marsman, M.; Jamil, T.; Dropmann, D.; Verhagen, J.; Ly, A.; Gronau, Q.F.; Šmíra, M.; Epskamp, S.; et al. JASP: Graphical statistical software for common statistical designs. J. Stat. Softw. 2019, 88, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Dienes, Z. Using Bayes to get the most out of non-significant results. Front. Psychol. 2014, 5, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dienes, Z. How Bayes factors change scientific practice. J. Math. Psychol. 2016, 72, 78–89. [Google Scholar] [CrossRef]
- Mölbert, S.C.; Thaler, A.; Mohler, B.J.; Streuber, S.; Romero, J.; Black, M.J.; Zipfel, S.; Karnath, H.O.; Giel, K.E. Assessing body image in anorexia nervosa using biometric self-avatars in virtual reality: Attitudinal components rather than visual body size estimation are distorted. Psychol. Med. 2017, 48, 1–12. [Google Scholar] [CrossRef]
- Longo, M.R. Perceptual and Emotional Embodiment: Foundations of Embodied Cognition Volume 1; Routledge: London, UK, 2015. [Google Scholar]
- Pollatos, O.; Kurz, A.L.; Albrecht, J.; Schreder, T.; Kleemann, A.M.; Schöpf, V.; Kopietz, R.; Wiesmann, M.; Schandry, R. Reduced perception of bodily signals in anorexia nervosa. Eat. Behav. 2008, 9, 381–388. [Google Scholar] [CrossRef]
- Preston, C.; Ehrsson, H.H. Illusory obesity triggers body dissatisfaction responses in the insula and anterior cingulate cortex. Cereb. Cortex 2016, 26, 4450–4460. [Google Scholar] [CrossRef]
- Jabbi, M.; Bastiaansen, J.; Keysers, C. A Common Anterior Insula Representation of Disgust Observation, Experience and Imagination Shows Divergent Functional Connectivity Pathways. PLoS ONE 2008, 3, e2939. [Google Scholar] [CrossRef] [Green Version]
- Wiech, K.; Lin, C.; Brodersen, K.H.; Bingel, U.; Ploner, M.; Tracey, I. Anterior Insula Integrates Information about Salience into Perceptual Decisions about Pain. J. Neurosci. 2010, 30, 16324–16331. [Google Scholar] [CrossRef]
- Galati, G.; Lobel, E.; Vallar, G.; Berthoz, A.; Pizzamiglio, L.; Le Bihan, D. The neural basis of egocentric and allocentric coding of space in humans: A functional magnetic resonance study. Exp. Brain Res. 2000, 133, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Haggard, P.; Longo, M.R.; Aza, E. More than skin deep: Body representation beyond primary somatosensory cortex. Neuropsychologia 2010, 48, 655–668. [Google Scholar]
- Riva, G. Neuroscience and eating disorders: The allocentric lock hypothesis. Med. Hypotheses 2012, 78, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Koskina, A.; Campbell, I.C.; Schmidt, U. Reviews Exposure therapy in eating disorders revisited. Neurosci. Biobehav. Rev. 2013, 37, 193–208. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic and Eating Disorder Variables | |||||||
|---|---|---|---|---|---|---|---|
| HC (N = 20) | AN (N = 20) | ||||||
| M | SD | M | SD | t | df | p | |
| Age | 23.85 | 3.23 | 23.30 | 7.60 | 0.29 | 38 | 0.767 |
| BMI | 18.94 | 0.98 | 15.86 | 1.12 | 9.22 | 38 | 0.001 |
| EDI—drive for thinness | 2.00 | 3.54 | 13.05 | 7.42 | −6.01 | 38 | 0.001 |
| EDI—bulimia | 0.40 | 0.99 | 0.95 | 2.19 | −1.02 | 38 | 0.313 |
| EDI—body dissatisfaction | 4.00 | 3.66 | 13.10 | 7.15 | −5.07 | 38 | 0.001 |
| BSQ | 64.55 | 17.13 | 118.75 | 32.89 | −6.54 | 38 | 0.001 |
| BUT GSI | 0.93 | 0.28 | 2.58 | 1.01 | −7.07 | 37 | 0.001 |
| BITE Symptoms | 6.10 | 3.97 | 11.80 | 6.41 | −3.38 | 38 | 0.002 |
| BITE Severity | 1.15 | 1.18 | 2.80 | 3.96 | −1.79 | 38 | 0.082 |
| Perceived, Ideal and Body Dissatisfaction Measures | ||||||||
|---|---|---|---|---|---|---|---|---|
| HC | AN | |||||||
| Task | M | SD | M | SD | t | df | p | BF |
| Perceived Body | 101.65 | 8.02 | 102.85 | 14.06 | −0.33 | 38 | 0.742 | 0.32 |
| Ideal Body | 94.65 | 1.38 | 87.10 | 1.59 | 2.28 | 38 | 0.028 | 2.26 |
| Body Dissatisfaction | 8.45 | 7.85 | 19.95 | 12.97 | −3.39 | 38 | 0.002 | 20.90 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Provenzano, L.; Porciello, G.; Ciccarone, S.; Lenggenhager, B.; Tieri, G.; Marucci, M.; Dazzi, F.; Loriedo, C.; Bufalari, I. Characterizing Body Image Distortion and Bodily Self-Plasticity in Anorexia Nervosa via Visuo-Tactile Stimulation in Virtual Reality. J. Clin. Med. 2020, 9, 98. https://doi.org/10.3390/jcm9010098
Provenzano L, Porciello G, Ciccarone S, Lenggenhager B, Tieri G, Marucci M, Dazzi F, Loriedo C, Bufalari I. Characterizing Body Image Distortion and Bodily Self-Plasticity in Anorexia Nervosa via Visuo-Tactile Stimulation in Virtual Reality. Journal of Clinical Medicine. 2020; 9(1):98. https://doi.org/10.3390/jcm9010098
Chicago/Turabian StyleProvenzano, Luca, Giuseppina Porciello, Sofia Ciccarone, Bigna Lenggenhager, Gaetano Tieri, Matteo Marucci, Federico Dazzi, Camillo Loriedo, and Ilaria Bufalari. 2020. "Characterizing Body Image Distortion and Bodily Self-Plasticity in Anorexia Nervosa via Visuo-Tactile Stimulation in Virtual Reality" Journal of Clinical Medicine 9, no. 1: 98. https://doi.org/10.3390/jcm9010098
APA StyleProvenzano, L., Porciello, G., Ciccarone, S., Lenggenhager, B., Tieri, G., Marucci, M., Dazzi, F., Loriedo, C., & Bufalari, I. (2020). Characterizing Body Image Distortion and Bodily Self-Plasticity in Anorexia Nervosa via Visuo-Tactile Stimulation in Virtual Reality. Journal of Clinical Medicine, 9(1), 98. https://doi.org/10.3390/jcm9010098