Treatment with Tumor Necrosis Factor-α Inhibitors, History of Allergy, and Hypercalcemia Are Risk Factors of Immune Reconstitution Inflammatory Syndrome in HIV-Negative Pulmonary Tuberculosis Patients


 , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Methods
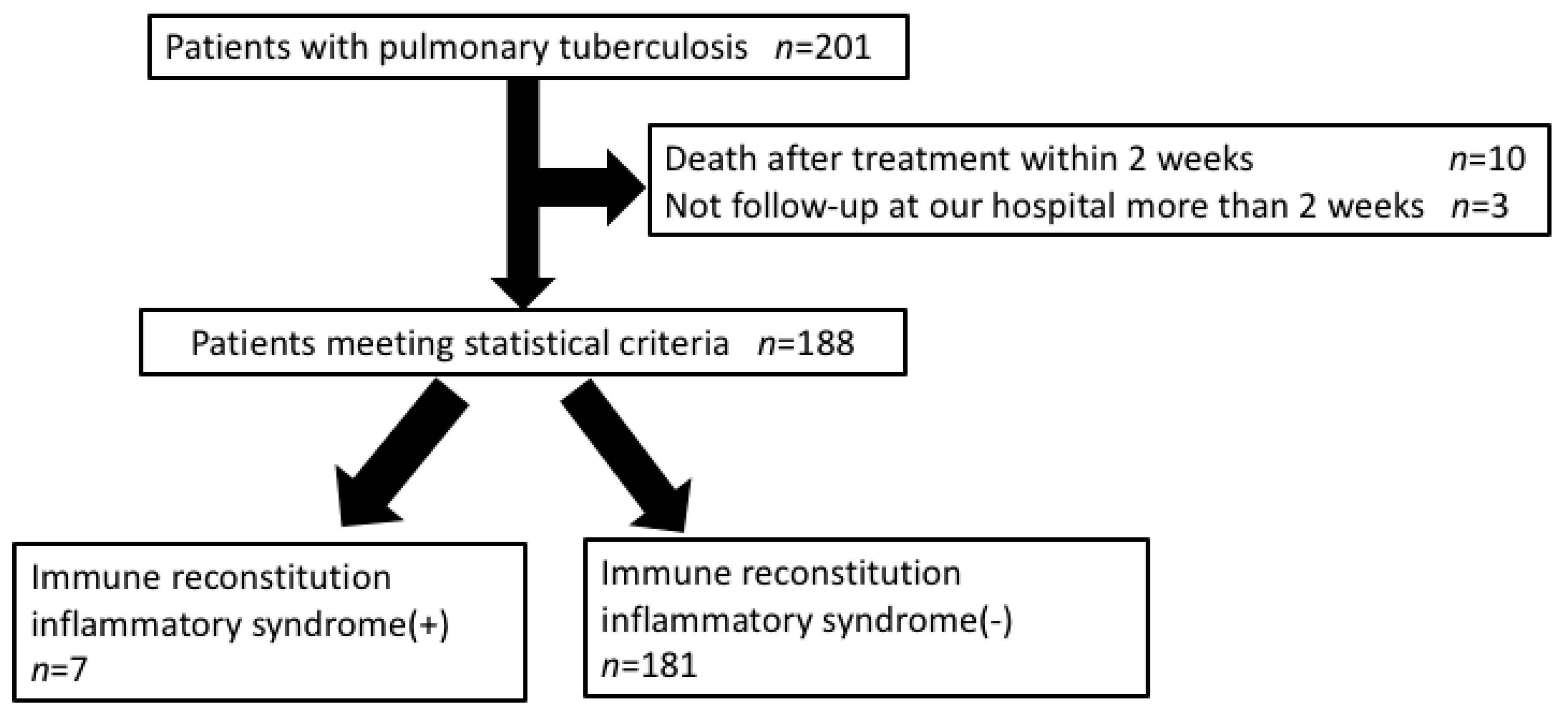
2.1. Study Population
2.2. Diagnosis of IRIS
2.3. Statistical Analysis
3. Results
3.1. Association of Patient Background with IRIS Development
3.2. Association of Clinical Parameters with IRIS Development
3.3. Assessment by Multivariate Analysis of IRIS Development
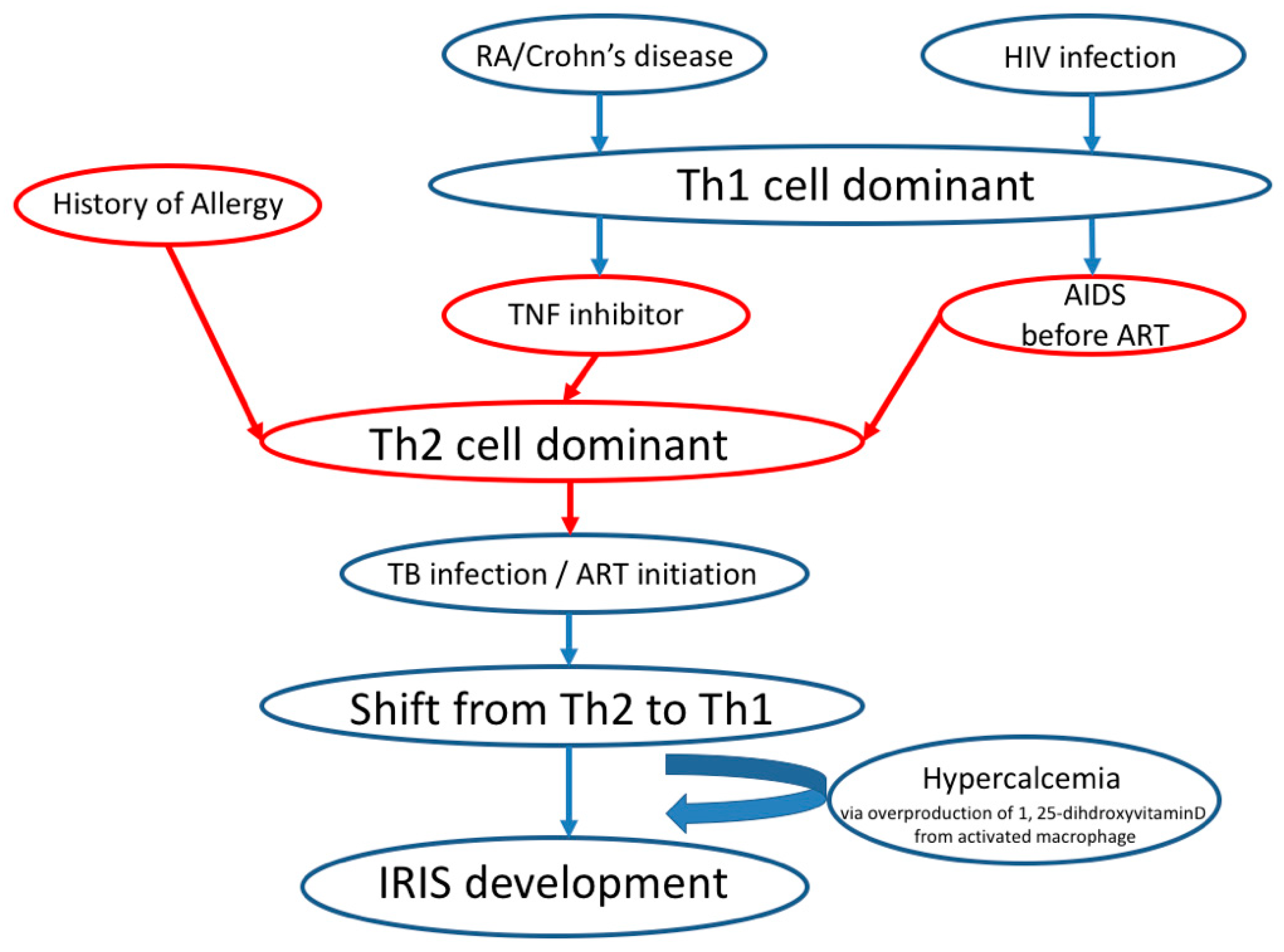
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cheng, V.C.; Yam, W.C.; Woo, P.C.; Lau, S.K.; Hung, I.F.; Wong, S.P.; Cheung, W.C.; Yuen, K.Y. Risk factors for development of paradoxical response during antituberculosis therapy in HIV-negative patients. Eur. J. Clin. Microbiol. Infect. Dis. 2003, 22, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.Y.; Singh, N. Immune reconstitution inflammatory syndrome in non-HIV immunocompromised patients. Curr. Opin. Infect. Dis. 2009, 22, 394–402. [Google Scholar] [CrossRef]
- Cheng, S.L.; Wang, H.C.; Yang, P.C. Paradoxical response during anti-tuberculosis treatment in HIV-negative patients with pulmonary tuberculosis. Int. J. Tuberc. Lung Dis. 2007, 11, 1290–1295. [Google Scholar] [PubMed]
- Breen, R.A.; Smith, C.J.; Bettinson, H.; Dart, S.; Bannister, B.; Johnson, M.A.; Lipman, M.C. Paradoxical reactions during tuberculosis treatment in patients with and without HIV co-infection. Thorax 2004, 59, 704–707. [Google Scholar] [CrossRef]
- Jung, J.W.; Shin, J.W.; Kim, J.Y.; Park, I.W.; Choi, B.W.; Seo, J.S.; Choi, J.C. Risk factors for development of paradoxical response during anti-tuberculosis treatment in HIV-negative patients with pleural tuberculosis. Tohoku J. Exp. Med. 2011, 223, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Narita, M.; Ashkin, D.; Hollender, E.S.; Pitchenik, A.E. Paradoxical worsening of tuberculosis following antiretroviral therapy in patients with AIDS. Am. J. Respir. Crit. Care Med. 1998, 158, 157–161. [Google Scholar] [CrossRef]
- Lipman, M.; Breen, R. Immune reconstitution inflammatory syndrome in HIV. Curr. Opin. Infect. Dis. 2006, 19, 20–25. [Google Scholar] [CrossRef]
- Bonnet, M.; Baudin, E.; Jani, I.V.; Nunes, E.; Verhoustraten, F.; Calmy, A.; Bastos, R.; Bhatt, N.B.; Michon, C. Incidence of paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome and impact on patient outcome. PLoS ONE 2013, 8, e84585. [Google Scholar] [CrossRef]
- Rivoisy, C.; Tubach, F.; Roy, C.; Nicolas, N.; Mariette, X.; Salmon, D.; Lortholary, O.; Bourgarit, A. Paradoxical anti-TNF-associated TB worsening: Frequency and factors associated with IRIS. Jt. BoneSpine 2016, 83, 173–178. [Google Scholar] [CrossRef]
- Tanaka, T.; Sekine, A.; Tsunoda, Y.; Takoi, H.; Lin, S.Y.; Yatagai, Y.; Hayasihara, K.; Saito, T. Central nervous system manifestations of tuberculosis-associated immune reconstitution inflammatory syndrome during adalimumab therapy: A case report and review of the literature. Intern. Med. 2015, 54, 847–851. [Google Scholar] [CrossRef][Green Version]
- Geri, G.; Passeron, A.; Heym, B.; Arlet, J.B.; Pouchot, J.; Capron, L.; Ranque, B. Paradoxical reactions during treatment of tuberculosis with extrapulmonary manifestations in HIV-negative patients. Infection 2013, 41, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.S.; Smith, C.J.; Breen, R.A.; Ormerod, L.P.; Mittal, R.; Fisk, M.; Milburn, H.J.; Price, N.M.; Bothamley, G.H.; Lipman, M.C. Determinants of treatment-related paradoxical reactions during anti-tuberculosis therapy: A case control study. BMC Infect. Dis. 2016, 16, 479. [Google Scholar] [CrossRef] [PubMed]
- Kasama, S.; Toyama, T.; Sumino, H.; Nakazawa, M.; Matsumoto, N.; Sato, Y.; Kumakura, H.; Takayama, Y.; Ichikawa, S.; Suzuki, T.; et al. Prognostic value of serial cardiac 123I-MIBG imaging in patients with stabilized chronic heart failure and reduced left ventricular ejection fraction. J. Nucl. Med. 2008, 49, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Kasama, S.; Toyama, T.; Kurabayashi, M. Serial (1)(2)(3)I-metaiodobenzylguanidine imaging predicts the risk of sudden cardiac death in patients with chronic heart failure. Int. J. Cardiol. 2015, 179, 82–83. [Google Scholar] [CrossRef]
- Musselwhite, L.W.; Andrade, B.B.; Ellenberg, S.S.; Tierney, A.; Belaunzaran-Zamudio, P.F.; Rupert, A.; Lederman, M.M.; Sanne, I.; Sierra Madero, J.G.; Sereti, I. Vitamin D, D-dimer, Interferon gamma, and sCD14 Levels are Independently Associated with Immune Reconstitution Inflammatory Syndrome: A Prospective, International Study. EBioMedicine 2016, 4, 115–123. [Google Scholar] [CrossRef]
- Jeon, K.; Choi, W.I.; An, J.S.; Lim, S.Y.; Kim, W.J.; Park, G.M.; Park, S.S.; Choi, H.S.; Lee, B.H.; Choi, J.C.; et al. Paradoxical response in HIV-negative patients with pleural tuberculosis: A retrospective multicentre study. Int. J. Tuberc. Lung Dis. 2012, 16, 846–851. [Google Scholar] [CrossRef]
- Watanabe, S.; Kaneko, Y.; Kawamoto, H.; Maehara, T.; Baba, Y.; Fujisaki, I.; Saito, N.; Ryu, K.; Seki, A.; Horikiri, T.; et al. Paradoxical response with increased tumor necrosis factor-alpha levels to anti-tuberculosis treatment in a patient with disseminated tuberculosis. Respir. Med. Case Rep. 2017, 20, 201–204. [Google Scholar]
- Unlu, M.; Cimen, P.; Ayranci, A.; Akarca, T.; Karaman, O.; Dereli, M.S. Disseminated tuberculosis infection and paradoxical reaction during antimycobacterial treatment related to TNF-alpha blocker agent Infliximab. Respir. Med. Case Rep. 2014, 13, 43–47. [Google Scholar] [CrossRef]
- Melboucy-Belkhir, S.; Flexor, G.; Stirnemann, J.; Morin, A.S.; Boukari, L.; Polliand, C.; Cruaud, P.; Fain, O. Prolonged paradoxical response to anti-tuberculous treatment after infliximab. Int. J. Infect. Dis. 2010, 14, e333–e334. [Google Scholar] [CrossRef]
- Yamada, H. Current perspectives on the role of IL-17 in autoimmune disease. J. Inflamm. Res. 2010, 3, 33–44. [Google Scholar] [CrossRef]
- Ruschen, S.; Stellberg, W.; Warnatz, H. Kinetics of cytokine secretion by mononuclear cells of the blood from rheumatoid arthritis patients are different from those of healthy controls. Clin. Exp. Immunol. 1992, 89, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Van Roon, J.A.; Verhoef, C.M.; van Roy, J.L.; Gmelig-Meyling, F.H.; Huber-Bruning, O.; Lafeber, F.P.; Bijlsma, J.W. Decrease in peripheral type 1 over type 2 T cell cytokine production in patients with rheumatoid arthritis correlates with an increase in severity of disease. Ann. Rheum. Dis. 1997, 56, 656–660. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Okamoto, S.; Hisamatsu, T.; Kamada, N.; Chinen, H.; Saito, R.; Kitazume, M.T.; Nakazawa, A.; Sugita, A.; Koganei, K.; et al. IL23 differentially regulates the Th1/Th17 balance in ulcerative colitis and Crohn’s disease. Gut 2008, 57, 1682–1689. [Google Scholar] [CrossRef] [PubMed]
- Imami, N.; Antonopoulos, C.; Hardy, G.A.; Gazzard, B.; Gotch, F.M. Assessment of type 1 and type 2 cytokines in HIV type 1-infected individuals: Impact of highly active antiretroviral therapy. AIDS Res. Hum. Retrovir. 1999, 15, 1499–1508. [Google Scholar] [CrossRef]
- Lanzafame, M.; Vento, S. Tuberculosis-immune reconstitution inflammatory syndrome. J. Clin. Tuberc. Other Mycobact. Dis. 2016, 3, 6–9. [Google Scholar] [CrossRef]
- Douglas, S.D.; Durako, S.; Sullivan, K.E.; Camarca, M.; Moscicki, A.B.; Wilson, C.M. TH1 and TH2 cytokine mRNA and protein levels in human immunodeficiency virus (HIV)-seropositive and HIV-seronegative youths. Clin. Diagn. Lab. Immunol. 2003, 10, 399–404. [Google Scholar] [CrossRef]
- Yamada, H.; Hida, N.; Kurashima, Y.; Satoh, H.; Saito, T.; Hizawa, N. A case of severe eosinophilic asthma and refractory rheumatoid arthritis well controlled by combination of IL-5Ralpha antibody and TNFalpha inhibitor. Allergol. Int. 2019, 68, 536–538. [Google Scholar] [CrossRef]
- Singh, N. Hypercalcemia related to immune reconstitution in organ transplant recipients with granulomatous opportunistic infections. Transplantation 2006, 82, 986. [Google Scholar] [CrossRef]
- Pornsuriyasak, P.; Suwatanapongched, T. Thoracic manifestations of paradoxical immune reconstitution inflammatory syndrome during or after antituberculous therapy in HIV-negative patients. Diagn. Interv. Radiol. 2015, 21, 134–139. [Google Scholar] [CrossRef]
- Lin, C.H.; Lin, C.J.; Kuo, Y.W.; Wang, J.Y.; Hsu, C.L.; Chen, J.M.; Cheng, W.C.; Lee, L.N. Tuberculosis mortality: Patient characteristics and causes. BMC Infect. Dis. 2014, 14, 5. [Google Scholar] [CrossRef]
- Alavi-Naini, R.; Moghtaderi, A.; Metanat, M.; Mohammadi, M.; Zabetian, M. Factors associated with mortality in tuberculosis patients. J. Res. Med. Sci. 2013, 18, 52–55. [Google Scholar] [PubMed]
- Erbes, R.; Oettel, K.; Raffenberg, M.; Mauch, H.; Schmidt-Ioanas, M.; Lode, H. Characteristics and outcome of patients with active pulmonary tuberculosis requiring intensive care. Eur. Respir. J. 2006, 27, 1223–1228. [Google Scholar] [CrossRef] [PubMed]
- Meintjes, G.; Boulle, A. Immune reconstitution inflammatory syndrome in a large multicenter cohort study: Case definition and comparability. Expert. Rev. Anti. Infect. 2012, 10, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Sainz-de-la-Maza, S.; Casado, J.L.; Perez-Elias, M.J.; Moreno, A.; Quereda, C.; Moreno, S.; Corral, I. Incidence and prognosis of immune reconstitution inflammatory syndrome in HIV-associated progressive multifocal leucoencephalopathy. Eur. J. Neurol. 2016, 23, 919–925. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| (1) Initial improvement after anti-TB treatment initiation |
| (2) Worsening of the initial symptoms or onset of new TB-like symptoms after the initiation of anti-TB treatment |
| (3) Absence of persistently active TB |
| (4) Absence of any other explanation of clinical deterioration |
| Background Factors | All Patients (n = 188) | IRIS(+) (n = 7) | IRIS(−) (n = 181) | p Value |
|---|---|---|---|---|
| Age | 62.11 ± 21.54 | 62.71 ± 23.73 | 62.08 ± 21.52 | 0.939 |
| Male | 62.8% (118) | 57.1% (4) | 63.0% (114) | 0.754 |
| BMI | 19.77 ± 3.58 | 19.95 ± 5.98 | 19.76 ± 3.49 | 0.898 |
| Allergy | 9.0% (17) | 42.9% (3) | 7.7% (14) | 0.007 * |
| Smoking | 42.6% (80) | 42.9% (3) | 42.5% (77) | 0.987 |
| Alcohol | 33.5% (63) | 42.9% (3) | 33.1% (60) | 0.596 |
| Past infection | 14.9% (28) | 28.6% (2) | 14.4% (26) | 0.314 |
| Foreign nationality | 13.3% (25) | 0.0% (0) | 13.8% (25) | 0.994 |
| Smear positive | 77.1% (145) | 85.7% (6) | 76.8% (139) | 0.602 |
| HIV Infection | 0.0% (0) | 0.0% (0) | 0.0% (0) | - |
| Immunosuppressiye drugs | 11.2% (21) | 57.1% (4) | 9.4% (17) | 0.002 * |
| Biological drug | 2.1% (4) | 28.6% (2) | 1.1% (2) | 0.001 * |
| Non-biological drug | 9.6% (18) | 28.6% (2) | 8.8% (16) | 0.106 |
| Diabetes mellitus | 20.7% (39) | 28.6% (2) | 20.4% (37) | 0.605 |
| Dialysis | 6.4% (12) | 14.3% (1) | 6.1% (11) | 0.400 |
| Past tumor | 19.7% (37) | 0.0% (0) | 20.4% (37) | 0.993 |
| Over 70 years | 45.7% (86) | 57.1% (4) | 45.3% (82) | 0.541 |
| Complication of miliary TB | 10.1% (19) | 28.6% (2) | 9.4% (17) | 0.123 |
| Serological Markers | All Patients (n = 188) | IRIS(+) (n = 7) | IRIS(−) (n = 181) | p Value |
|---|---|---|---|---|
| WBC (/μL) | 7075 ± 3232 | 6700 ± 4125 | 7090 ± 3206 | 0.752 |
| Lym (/μL) | 988 ± 502 | 614 ± 359 | 1003 ± 502 | 0.053 |
| Hb (g/dL) | 11.6 ± 2.0 | 11.2 ± 2.7 | 11.7 ± 1.9 | 0.503 |
| Alb (g/dL) | 3.25 ± 0.82 | 2.44 ± 0.72 | 3.28 ± 0.80 | 0.016 * |
| LDH (U/L) | 220 ± 80 | 203 ± 54 | 221 ± 81 | 0.556 |
| ALP (U/L) | 293 ± 140 | 372 ± 316 | 290 ± 129 | 0.146 |
| ESR (mm/H) | 61.7 ± 33.4 | 79.1 ± 47.7 | 61.0 ± 32.6 | 0.167 |
| CRP (mg/dL) | 3.96 ± 4.61 | 5.83 ± 4.06 | 3.89 ± 4.62 | 0.281 |
| Ca (mg/dL) | 9.74 ± 0.69 | 10.38 ± 0.86 | 9.72 ± 0.68 | 0.039 * |
| D-dimer (μg/mL) | 6.35 ± 9.51 | 9.58 ± 14.06 | 6.19 ± 9.29 | 0.445 |
| HbA1c (NGSP) (%) | 6.22 ± 1.45 | 5.70 ± 0.50 | 6.26 ± 1.49 | 0.292 |
| Treatment course | ||||
| Weeks until 3 consecutive smears negative | 8.00 ± 6.24 | 7.00 ± 4.24 | 8.03 ± 6.31 | 0.746 |
| Death | 9.0% (17) | 42.9% (3) | 7.7% (14) | 0.007 ** |
| Univariate | Multivariate | Wald | p Value | |
|---|---|---|---|---|
| Background factors | ||||
| Age | 1.00 (0.97–1.04) | |||
| Male | 0.78 (0.17–3.61) | |||
| Body mass index | 1.01 (0.81–1.27) | |||
| Allergy | 8.95 (1.82–44.00) | 10.39 (1.17–91.88) | 4.43 | 0.035 * |
| Smoking | 1.01 (0.22–4.66) | |||
| Alcohol | 1.51 (0.33–6.98) | |||
| Past infection | 2.38 (0.44–12.90) | |||
| Immunosuppressive drug | 12.90 (2.65–62.30) | |||
| Biological drug | 35.80 (4.16–308.00) | 142.65 (6.87–2962.35) | 10.27 | 0.001 ** |
| Non-biological immunosuppressive drug | 4.12 (0.74–23.00) | |||
| Diabetes mellitus | 1.56 (0.29–8.35) | |||
| Dialysis | 2.58 (0.29–23.30) | |||
| Complication of miliary TB | 3.86 (0.70–21.40) | |||
| Serological markers | ||||
| White blood cell count (/μL) | 1.00 (1.00–1.00) | |||
| Lymphocyte count (/μL) | 1.00 (1.00–1.00) | |||
| Albumin (g/dL) | 0.26 (0.09–0.78) | |||
| ESR (mm/H) | 1.02 (0.99–1.04) | |||
| C-reactive protein (mg/dL) | 1.07 (0.94–1.22) | |||
| Calcium (mg/dL) | 2.38 (1.04–5.44) | 5.82 (1.26–26.92) | 5.07 | 0.024 * |
| HbA1c (%) | 0.54 (0.17–1.70) | |||
| Treatment course | ||||
| Death | 8.95 (1.82–44.00) |
| Multivariate1 | p Value | Multivariate2 | p Value | Multivariate3 | p Value | |
|---|---|---|---|---|---|---|
| Background factors | ||||||
| Allergy | 9.01 (1.54–52.80) | 0.015 * | 9.96 (1.72–57.90) | 0.010 * | ||
| Biological drug | 36.10 (3.39–385.0) | 0.003 ** | 98.2 (6.79–1420) | <0.001 ** | ||
| Serological markers | ||||||
| Calcium (mg/dL) | 2.36 (1.01–5.53) | 0.049 * | 2.85 (1.15–7.10) | 0.024 * |
| Patient No | Age | sex | Extrapulmonary Tuberculosis | Underlying Disease | Anti-TNFa Regimen | Using Time (months) | IRIS | Discontinuation of Biological Drugs |
|---|---|---|---|---|---|---|---|---|
| 1 | 68 | F | Miliary TB | RA | Adalimumab | 48 | No | Discontinuation |
| 2 | 58 | M | None | Crohn’s disease | Adalimumab | 14 | Yes | Discontinuation |
| 3 | 75 | M | None | Psoriasis vulgaris | Adalimumab | 24 | No | Continuation |
| 4 | 36 | M | None | Crohn’s disease | Infliximab | 64 | yes | Continuation |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hachisu, Y.; Koga, Y.; Kasama, S.; Kaira, K.; Yatomi, M.; Aoki-Saito, H.; Tsurumaki, H.; Kamide, Y.; Sunaga, N.; Maeno, T.; et al. Treatment with Tumor Necrosis Factor-α Inhibitors, History of Allergy, and Hypercalcemia Are Risk Factors of Immune Reconstitution Inflammatory Syndrome in HIV-Negative Pulmonary Tuberculosis Patients. J. Clin. Med. 2020, 9, 96. https://doi.org/10.3390/jcm9010096
Hachisu Y, Koga Y, Kasama S, Kaira K, Yatomi M, Aoki-Saito H, Tsurumaki H, Kamide Y, Sunaga N, Maeno T, et al. Treatment with Tumor Necrosis Factor-α Inhibitors, History of Allergy, and Hypercalcemia Are Risk Factors of Immune Reconstitution Inflammatory Syndrome in HIV-Negative Pulmonary Tuberculosis Patients. Journal of Clinical Medicine. 2020; 9(1):96. https://doi.org/10.3390/jcm9010096
Chicago/Turabian StyleHachisu, Yoshimasa, Yasuhiko Koga, Shu Kasama, Kyoichi Kaira, Masakiyo Yatomi, Haruka Aoki-Saito, Hiroaki Tsurumaki, Yosuke Kamide, Noriaki Sunaga, Toshitaka Maeno, and et al. 2020. "Treatment with Tumor Necrosis Factor-α Inhibitors, History of Allergy, and Hypercalcemia Are Risk Factors of Immune Reconstitution Inflammatory Syndrome in HIV-Negative Pulmonary Tuberculosis Patients" Journal of Clinical Medicine 9, no. 1: 96. https://doi.org/10.3390/jcm9010096
APA StyleHachisu, Y., Koga, Y., Kasama, S., Kaira, K., Yatomi, M., Aoki-Saito, H., Tsurumaki, H., Kamide, Y., Sunaga, N., Maeno, T., Ishizuka, T., & Hisada, T. (2020). Treatment with Tumor Necrosis Factor-α Inhibitors, History of Allergy, and Hypercalcemia Are Risk Factors of Immune Reconstitution Inflammatory Syndrome in HIV-Negative Pulmonary Tuberculosis Patients. Journal of Clinical Medicine, 9(1), 96. https://doi.org/10.3390/jcm9010096