1. Introduction
The diagnosis of congenital heart disease (CHD) encompasses various anatomical abnormalities of the heart and the great arteries [
1]. Modern treatment methods are primarily directed towards the surgical repair of these structural defects. These treatment approaches are considerably life prolonging but mostly not curative, resulting in life-long persisting cardiovascular residua and sequels, e.g., residual shunts, valvular lesions, or implantation of prosthetic materials causing an inherent risk for infective endocarditis in these patients [
2,
3].
It is commonly accepted that the development of infective endocarditis requires bacteremia with microorganisms that can successfully adhere to the endocardial surfaces [
4]. The oral cavity is colonized by a complex microflora and is frequently affected by two of the most prevalent human diseases, i.e., caries and periodontitis. Both are substantially caused by the manifestation of dysbiotic bacterial infections of tooth related structures [
5]. Accordingly, the oral cavity is considered a highly relevant source for bacteremia leading to infective endocarditis. Bacteremia derived from the oral cavity is detectable after minor mucosal trauma, including not only various standard dental diagnostic and therapeutic procedures [
6], but also frequent daily activities, i.e., teeth brushing or mastication [
7]. Consistently, the risk for bacteremia with oral microorganisms is correlated with the presence and severity of oral diseases [
8]. According to recent clinical observations, oral streptococci account for >20% of infective endocarditis [
9].
Apart from the use of systemic antibiotics, the prophylaxis of transient bacteremia due to professional dental care and routine daily activities is directed towards the prevention and treatment of the oral disease itself. Despite the elevated risk of manifestation of infective endocarditis, there exists some evidence that young patients with CHD show increasing amounts of dental deposits, i.e., plaque, more plaque induced gingival inflammation, lower compliance with dental maintenance care, and poorer routine oral hygiene measures during childhood and adolescence [
10,
11]. In a study from Janssens, a high proportion of young patients with CHD aged 14–18 years did not have a dental visit during the past year and even more than 40% never flossed their teeth, indicating insufficient control of potentially infective bacterial deposits [
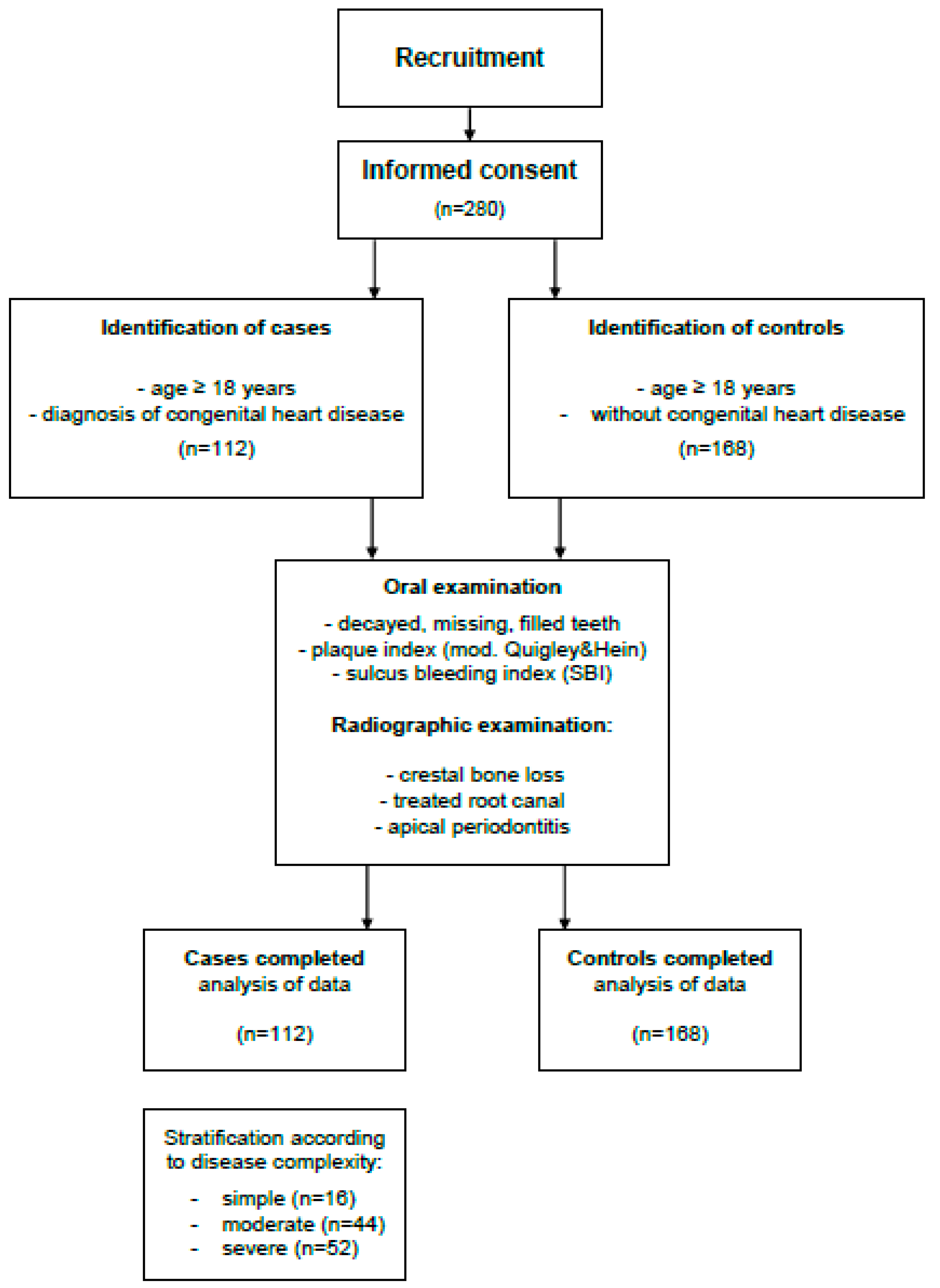
12]. Yet, it remains to be elucidated if adults with CHD also show a lacking adherence to oral preventive measures ultimately resulting in a higher risk for caries, gingivitis or periodontitis. The present case-control study aimed to delineate (1) the level of oral care (2) the prevalence and severity of odontogenic diseases in adults with CHD in comparison to the general population.
4. Discussion
The individual susceptibility for the manifestation of infective endocarditis is strongly influenced by the presence and severity of oral diseases [
7,
18]. The manipulation and perforation of infected tissue, particularly the gingival margin and the periapical tissue, during dental care and routine daily activities, i.e., teeth brushing or mastication, causes an inherent risk for bacteremia [
19]. Antibiotic prophylaxis has been recommended to address the elevated risk for infective endocarditis during occasional diagnostic and therapeutic dental procedures in patients with cardiovascular anomalies, including individuals with CHD [
20,
21]. Considering daily activities, the avoidance of oral diseases seems the most appropriate prevention strategy against infective endocarditis in individuals with predisposing cardiovascular defects [
22]. Comparing the experience with caries and periodontitis between individuals with and without CHD, patients with heart disease presented a considerably better oral health. Focusing on caries, the DMFT reflects the number of already missing, previously restored, and actually decayed teeth. This score was significantly lower among patients with CHD than without. As already reported, these patients with CHD had an average DMFT index of 7.91 [
14]. In the control group examined in the present study, the DMFT reached even 13.59, indicating a considerably higher caries experience for heart-healthy individuals. This might be explained by a stricter adherence to oral maintenance care by individuals with CHD. Thereby, the current observations confirm the results of a recent Swedish study, which found a considerably lower rate of new approximal caries lesions in adolescents with CHD than in healthy controls [
23]. The lower incidence of caries in individuals with heart defects was specifically referred to their enrollment into a systematic preventive program already at the age of one year. However, considering the differences in caries experience between CHD patients and healthy controls one has to bear in mind the higher mean age within the latter group. The DMFT shows an age depending continuous increase. The increase of the DMFT was 3.7, comparing individuals at an age of 30 and 40 years according to a previous survey [
24]. The differences as observed herein might, therefore, at least partially attributable to the higher mean age of healthy controls.
Despite the overall lower caries experience among individuals with CHD, the subgroup of patients needing antibiotic prophylaxis prior to invasive dental procedures, however, showed significantly elevated DMFT scores as previously reported [
14], compared to the remaining cohort. Although not reaching significance this result is in line with the observation of a higher DMFT among patients with TGA as compared to subjects with tetralogy of Fallot representing moderate and severe forms of CHD respectively. Since the recommendation for antibiotic prophylaxis is particularly related to patients with severe forms of CHD due to their extraordinary high risk for infective endocarditis [
19], this observation seems alarming. It might be explained by stronger concerns about the risk to induce bacteremia during regular oral hygiene measures among patients with more severe forms of CHD.
Progressing caries finally reaches the pulp chamber and causes necrosis of the pulp tissue, ultimately resulting in bacterial infection and inflammation of the periapical tissue. Root canal treatment is the commonly accepted therapeutic approach to address both entities. Despite no clear evidence, teeth showing periapical disease have been suggested to cause transient bacteremia in remote sites of the organism [
20,
24]. Herein, heart healthy subjects presented a higher average number of teeth with periapical disease than patients with CHD. However, this difference between the groups was significant in female subjects only. One might speculate that female patients with CHD adhere better to oral supportive care and are more rigorous in maintaining oral health than male patients. Since periapical periodontitis is a consequence of progressing caries, again, these data seem to further support the conclusion that patients with CHD have a lower caries experience than healthy controls.
The total soft tissue surface area of periodontal pockets amounts to almost 44 cm
2 [
25] and has thus been proposed as a highly significant source of entry for bacteria invading the systemic bloodstream [
26]. The surface area seems to correlate with the progression of periodontitis due to the deepening of the periodontal pockets [
25]. Based on radiographic data, periodontal bone loss at both single rooted and multi rooted teeth was three times as high in heart healthy individuals compared to subjects with CHD. Although the difference did not reach significance, there was, again, a trend for a more pronounced bone loss among patients with CHD, for whom antibiotic prophylaxis is recommended prior to invasive dental procedures. The current observations are partially contradictory to two previous studies in children revealing a higher rate of gingivitis, which is commonly considered as precursor disease to periodontitis, among patients with CHD [
10,
11].
It is commonly accepted that the manifestation and progression of periodontitis and caries is essentially bound to the presence of plaque [
5]. Intriguingly, despite their considerably lower experience regarding caries and periodontitis, patients with CHD presented with significantly higher amounts of plaque compared to heart-healthy controls herein. This might lead to the assumption of poorer compliance with oral hygiene measures. As previously reported, an attitude of neglecting the clinical relevance of regular oral hygiene among the CHD cohort of this study was found [
14]. The higher amount of plaque found in patients with CHD might also be explained by differences in the clinical conditions under which it has been determined in both study groups. Healthy control patients attended a university dental school and were thus aware about the examination and/or treatment of their teeth. This might have motivated them to tooth cleaning measures immediately prior to their visit. On the contrary, patients with CHD were examined during routine cardiological follow-up visits at the cardiological clinic, being unaware of the dental examination in this context. This conclusion is supported by the lower rate of sulcus bleeding among CHD patients than in healthy controls. It is commonly accepted that gingival bleeding correlates with the amount of plaque during the past days prior to the examination. Gingival bleeding in the absence of actual plaque confirms plaque that has just been removed immediately prior to the clinical determination of the bleeding score. On the contrary, the absence of bleeding together with the manifestation of current plaque is compatible with effective plaque control within the past days.
The current data reveal distinct differences of oral health between individuals with CHD and heart healthy controls. When drawing conclusions, at least two specific aspects of the study design have to be taken into account. Most important, healthy control subjects were recruited in a tertiary dental hospital center, probably leading to selection bias. This problem was addressed by the random selection of controls among patients attending the hospital for dental treatment by undergraduate students. These patients typically present with common dental problems and appear as a representative sample of the general population. Moreover, since the oral examination was performed at two different hospital centers, clinical data were not collected by the same person in each patient, potentially resulting in a certain degree of interexaminer variability.

 ,
, 

{kind=link}