Use of Antiplatelet Agents and Survival of Tuberculosis Patients: A Population-Based Cohort Study

 , ,
, ,  and
and
Abstract
1. Introduction
2. Experimental Section
2.1. Ethics Statement
2.2. Study Participants and Setting
2.3. Definitions and Data Collection
2.4. Outcomes
2.5. Statistical Analysis
3. Results
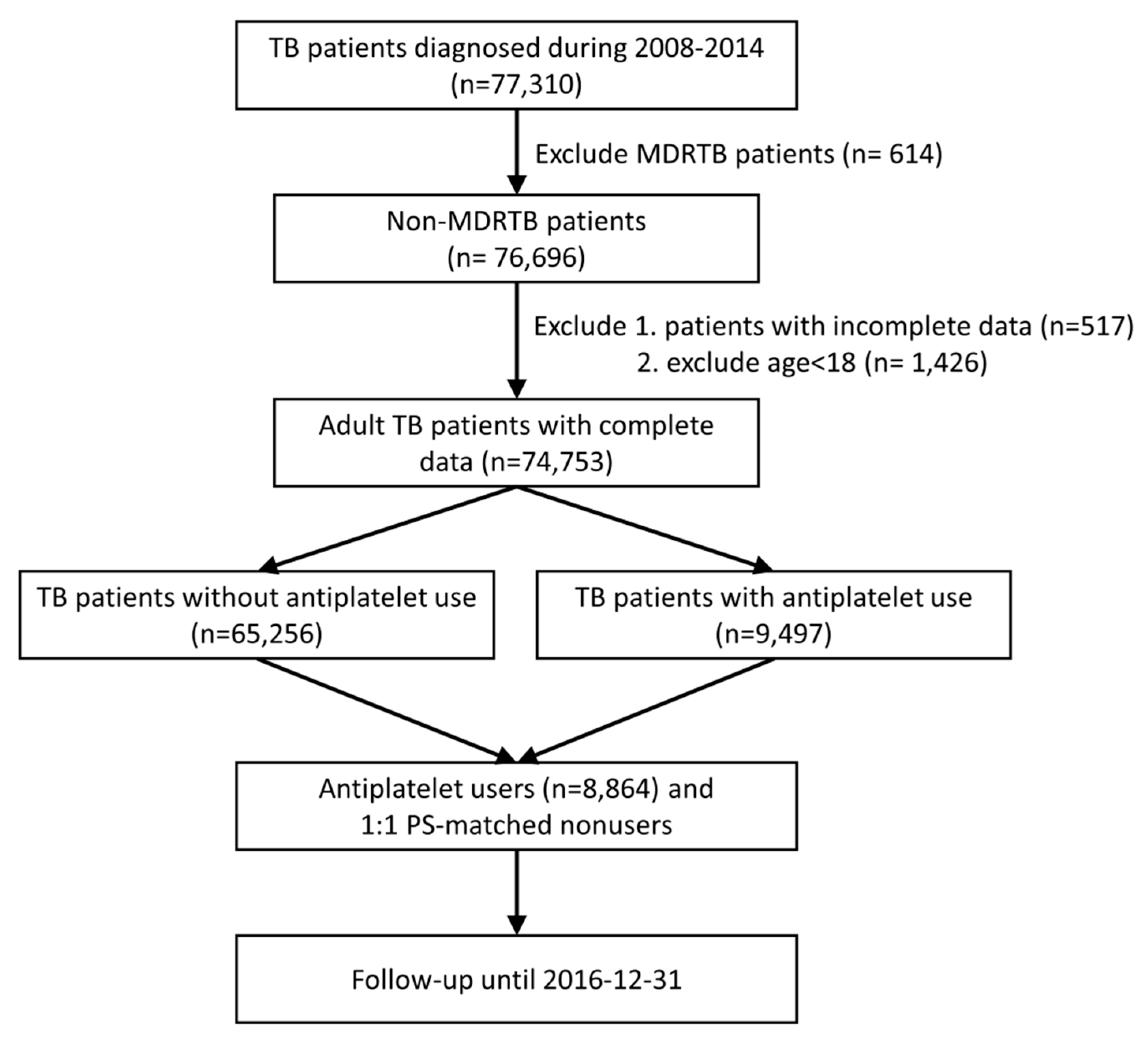
3.1. Patients Identification
3.2. Demographic Data
3.3. Survival Analysis
3.4. One-Year Mortality Analysis
3.5. Major Bleeding Event Analysis
4. Discussion
5. Data Availability
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. Resolution WHA67/11: Global Strategy and Targets for Tuberculosis Prevention, Care and Control after 2015; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Pai, M.; Behr, M.A.; Dowdy, D.; Dheda, K.; Divangahi, M.; Boehme, C.C.; Ginsberg, A.; Swaminathan, S.; Spigelman, M.; Getahun, H.; et al. Tuberculosis. Nat. Rev. Dis. Primers 2016, 2, 16076. [Google Scholar] [CrossRef] [PubMed]
- Belard, S.; Remppis, J.; Bootsma, S.; Janssen, S.; Kombila, D.U.; Beyeme, J.O.; Rossatanga, E.G.; Kokou, C.; Osbak, K.K.; Obiang Mba, R.M.; et al. Tuberculosis Treatment Outcome and Drug Resistance in Lambarene, Gabon: A Prospective Cohort Study. Am. J. Trop. Med. Hyg. 2016, 95, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Wang, J.Y.; Lin, H.C.; Lin, P.Y.; Chang, J.H.; Suk, C.W.; Lee, L.N.; Lan, C.C.; Bai, K.J. Treatment delay and fatal outcomes of pulmonary tuberculosis in advanced age: A retrospective nationwide cohort study. BMC Infect. Dis. 2017, 17, 449. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Dorhoi, A.; Mollenkopf, H.J.; Yin, H.; Dong, Z.; Mao, L.; Zhou, J.; Bi, A.; Weber, S.; Maertzdorf, J.; et al. Platelets direct monocyte differentiation into epithelioid-like multinucleated giant foam cells with suppressive capacity upon mycobacterial stimulation. J. Infect. Dis. 2014, 210, 1700–1710. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.Y.; Kim, Y.J.; Lee, H.J.; Cho, S.Y.; Park, T.S. Mean Platelet Volume in Mycobacterium tuberculosis infection. BioMed Res. Int. 2016, 2016, 7508763. [Google Scholar] [CrossRef] [PubMed]
- Kutiyal, A.S.; Gupta, N.; Garg, S.; Hira, H.S. A Study of Haematological and Haemostasis Parameters and Hypercoagulable State in Tuberculosis Patients in Northern India and the Outcome with Anti-Tubercular Therapy. J. Clin. Diagn. Res. 2017, 11, OC09–OC13. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.A.; Kirwan, D.E.; Whittington, A.M.; Krishnan, N.; Robertson, B.D.; Gilman, R.H.; López, J.W.; Singh, S.; Porter, J.C.; Friedland, J.S. Platelets Regulate Pulmonary Inflammation and Tissue Destruction in Tuberculosis. Am. J. Respir. Crit. Care Med. 2018, 198, 245–255. [Google Scholar] [CrossRef]
- Hortle, E.; Johnson, K.E.; Johansen, M.D.; Nguyen, T.; Shavit, J.A.; Britton, W.J.; Tobin, D.M.; Oehlers, S.H. Thrombocyte Inhibition Restores Protective Immunity to Mycobacterial Infection in Zebrafish. J. Infect. Dis. 2019. [Google Scholar] [CrossRef]
- Hsing, A.W.; Ioannidis, J.P. Nationwide Population Science: Lessons from the Taiwan National Health Insurance Research Database. JAMA Intern. Med. 2015, 175, 1527–1529. [Google Scholar] [CrossRef]
- Lin, H.H.; Wu, C.Y.; Wang, C.H.; Fu, H.; Lönnroth, K.; Chang, Y.C.; Huang, Y.T. Association of Obesity, Diabetes, and Risk of Tuberculosis: Two Population-Based Cohorts. Clin. Infect. Dis. 2018, 66, 699–705. [Google Scholar] [CrossRef]
- Lo, H.Y.; Chou, P.; Yang, S.L.; Lee, C.Y.; Kuo, H.S. Trends in tuberculosis in Taiwan, 2002–2008. J. Formos. Med. Assoc. 2011, 110, 501–510. [Google Scholar] [CrossRef]
- Lin, L.Y.; Warren-Gash, C.; Smeeth, L.; Chen, P.C. Data resource profile: The National Health Insurance Research Database (NHIRD). Epidemiol. Health 2018, 40, e2018062. [Google Scholar] [CrossRef] [PubMed]
- Yeh, J.J.; Lin, C.L.; Hsu, C.Y.; Shae, Z.; Kao, C.H. Statin for Tuberculosis and Pneumonia in Patients with Asthma–Chronic Pulmonary Disease Overlap Syndrome: A Time-Dependent Population-Based Cohort Study. J. Clin. Med. 2018, 7, 381. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.Y.; Hsu, W.H.; Lin, C.C.; Lin, C.L.; Tsai, C.H.; Lin, C.H.; Chen, D.C.; Lin, T.C.; Hsu, C.Y.; Kao, C.H. Association of Arrhythmia in Patients with Cervical Spondylosis: A Nationwide Population-Based Cohort Study. J. Clin. Med. 2018, 7, 236. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Pioglitazone Reduces Dementia Risk in Patients with Type 2 Diabetes Mellitus: A Retrospective Cohort Analysis. J. Clin. Med. 2018, 7, 306. [Google Scholar] [CrossRef]
- Centers for Disease Control, Ministry of Health and Welfare. Taiwan Guidelines for TB Diagnosis & Treatment, 6th ed.; Centers for Disease Control, Ministry of Health and Welfare: Taipei, Taiwan, 2017. [Google Scholar]
- WHOCC. Definition and General Considerations. 2018. Available online: https://www.whocc.no/ddd/definition_and_general_considera/#Definition (accessed on 26 June 2019).
- Schulman, S.; Kearon, C. Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [PubMed]
- Schulman, S.; Angerås, U.; Bergqvist, D.; Eriksson, B.; Lassen, M.R.; Fisher, W. Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in surgical patients. J. Thromb. Haemost. 2010, 8, 202–204. [Google Scholar]
- Bannay, A.; Chaignot, C.; Blotiere, P.O.; Basson, M.; Weill, A.; Ricordeau, P.; Alla, F. The Best Use of the Charlson Comorbidity Index with Electronic Health Care Database to Predict Mortality. Med. Care 2016, 54, 188–194. [Google Scholar] [CrossRef]
- Bhatt, L.K.; Veeranjaneyulu, A. Enhancement of matrix metalloproteinase 2 and 9 inhibitory action of minocycline by aspirin: An approach to attenuate outcome of acute myocardial infarction in diabetes. Arch. Med. Res. 2014, 45, 203–209. [Google Scholar] [CrossRef]
- Kroesen, V.M.; Rodriguez-Martinez, P.; Garcia, E.; Rosales, Y.; Díaz, J.; Martín-Céspedes, M.; Tapia, G.; Sarrias, M.R.; Cardona, P.J.; Vilaplana, C. A Beneficial Effect of Low-Dose Aspirin in a Murine Model of Active Tuberculosis. Front. Immunol. 2018, 9, 798. [Google Scholar] [CrossRef]
- Thachil, J. Antiplatelet therapy—A summary for the general physicians. Clin. Med. 2016, 16, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Patrignani, P.; Patrono, C. Aspirin, platelet inhibition and cancer prevention. Platelets 2018, 29, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.J. The evolution of antiplatelet therapy in the treatment of acute coronary syndromes: From aspirin to the present day. Drugs 2012, 72, 2087–2116. [Google Scholar] [CrossRef] [PubMed]
- Petit-Jentreau, L.; Tailleux, L.; Coombes, J.L. Purinergic Signaling: A Common Path in the Macrophage Response against Mycobacterium tuberculosis and Toxoplasma gondii. Front. Cell Infect. Microbiol. 2017, 7, 347. [Google Scholar] [CrossRef] [PubMed]
- Maiga, M.; Ammerman, N.C.; Maiga, M.C.; Tounkara, A.; Siddiqui, S.; Polis, M.; Murphy, R.; Bishai, W.R. Adjuvant host-directed therapy with types 3 and 5 but not type 4 phosphodiesterase inhibitors shortens the duration of tuberculosis treatment. J. Infect. Dis. 2013, 208, 512–519. [Google Scholar] [CrossRef]
- Byrne, S.T.; Denkin, S.M.; Zhang, Y. Aspirin and ibuprofen enhance pyrazinamide treatment of murine tuberculosis. J. Antimicrob. Chemother. 2007, 59, 313–316. [Google Scholar] [CrossRef]
- Maitra, A.; Bates, S.; Shaik, M.; Evangelopoulos, D.; Abubakar, I.; McHugh, T.D.; Lipman, M.; Bhakta, S. Repurposing drugs for treatment of tuberculosis: A role for non-steroidal anti-inflammatory drugs. Br. Med. Bull. 2016, 118, 138–148. [Google Scholar] [CrossRef]
- Hinz, C.; Aldrovandi, M.; Uhlson, C.; Marnett, L.J.; Longhurst, H.J.; Warner, T.D.; Alam, S.; Slatter, D.A.; Lauder, S.N.; Allen-Redpath, K.; et al. Human Platelets Utilize Cycloxygenase-1 to Generate Dioxolane A3, a Neutrophil-activating Eicosanoid. J. Biol. Chem. 2016, 291, 13448–13464. [Google Scholar] [CrossRef]
- Schrottmaier, W.C.; Kral, J.B.; Badrnya, S.; Assinger, A. Aspirin and P2Y12 Inhibitors in platelet-mediated activation of neutrophils and monocytes. Thromb. Haemost. 2015, 114, 478–489. [Google Scholar] [CrossRef]
- Vilaplana, C.; Marzo, E.; Tapia, G.; Diaz, J.; Garcia, V.; Cardona, P.J. Ibuprofen therapy resulted in significantly decreased tissue bacillary loads and increased survival in a new murine experimental model of active tuberculosis. J. Infect. Dis. 2013, 208, 199–202. [Google Scholar] [CrossRef]
- Dallenga, T.; Linnemann, L.; Paudyal, B.; Repnik, U.; Griffiths, G.; Schaible, U.E. Targeting neutrophils for host-directed therapy to treat tuberculosis. Int. J. Med. Microbiol. 2018, 308, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, P.M.; Price, J.F.; Fowkes, F.G.; Zanchetti, A.; Roncaglioni, M.C.; Tognoni, G.; Lee, R.; Belch, J.F.; Wilson, M.; Mehta, Z.; et al. Short-term effects of daily aspirin on cancer incidence, mortality, and non-vascular death: Analysis of the time course of risks and benefits in 51 randomised controlled trials. Lancet 2012, 379, 1602–1612. [Google Scholar] [CrossRef]
- Ogundeji, A.O.; Pohl, C.H.; Sebolai, O.M. Repurposing of Aspirin and Ibuprofen as Candidate Anti-Cryptococcus Drugs. Antimicrob. Agents Chemother. 2016, 60, 4799–4808. [Google Scholar] [CrossRef] [PubMed]
- Lo, H.Y.; Yang, S.L.; Chou, P.; Chuang, J.H.; Chiang, C.Y. Completeness and timeliness of tuberculosis notification in Taiwan. BMC Public Health 2011, 11, 915. [Google Scholar] [CrossRef] [PubMed]
- Lo, H.Y.; Yang, S.L.; Lin, H.H.; Bai, K.J.; Lee, J.J.; Lee, T.I.; Chiang, C.Y. Does enhanced diabetes management reduce the risk and improve the outcome of tuberculosis? Int. J. Tuberc. Lung Dis. 2016, 20, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Sostres, C.; Lanas, A. Epidemiology of Low Dose Aspirin Damage in the Lower Gastrointestinal Tract. Curr. Pharm. Des. 2015, 21, 5094–5100. [Google Scholar] [CrossRef] [PubMed]
- Byrne, S.T.; Denkin, S.M.; Zhang, Y. Aspirin antagonism in isoniazid treatment of tuberculosis in mice. Antimicrob. Agents Chemother. 2007, 51, 794–795. [Google Scholar] [CrossRef] [PubMed]
- Schaller, A.; Sun, Z.; Yang, Y.; Somoskovi, A.; Zhang, Y. Salicylate reduces susceptibility of Mycobacterium tuberculosis to multiple antituberculosis drugs. Antimicrob. Agents Chemother. 2002, 46, 2636–2639. [Google Scholar] [CrossRef]
- Judge, H.M.; Patil, S.B.; Buckland, R.J.; Jakubowski, J.A.; Storey, R.F. Potentiation of clopidogrel active metabolite formation by rifampicin leads to greater P2Y12 receptor blockade and inhibition of platelet aggregation after clopidogrel. J. Thromb. Haemost. 2010, 8, 1820–1827. [Google Scholar] [CrossRef]
- Park, S.; Kang, H.J.; Jeon, J.H.; Kim, M.J.; Lee, I.K. Recent advances in the pathogenesis of microvascular complications in diabetes. Arch. Pharm. Res. 2019, 42, 252–262. [Google Scholar] [CrossRef]
- Russo, I.; Penna, C.; Musso, T.; Popara, J.; Alloatti, G.; Cavalot, F.; Pagliaro, P. Platelets, diabetes and myocardial ischemia/reperfusion injury. Cardiovasc. Diabetol. 2017, 16, 71. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, D.; Panagiotou, A. Oral antiplatelet agents and chronic kidney disease. Hellenic J. Cardiol. 2011, 52, 509–515. [Google Scholar] [PubMed]
- Vila, L.; Cullare, C.; Sola, J.; Puig, L.; de Castellarnau, C.; de Moragas, J.M. Cyclooxygenase activity is increased in platelets from psoriatic patients. J. Investig. Dermatol. 1991, 97, 922–926. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.R.; Huang, Y.P.; Kuo, Y.T.; Luo, C.H.; Shih, Y.J.; Shu, C.C.; Wang, J.Y.; Ko, J.C.; Yu, C.J.; Lin, H.H. Diabetes Mellitus and Latent Tuberculosis Infection: A Systematic Review and Metaanalysis. Clin. Infect. Dis. 2017, 64, 719–727. [Google Scholar] [PubMed]
- Vallerskog, T.; Martens, G.W.; Kornfeld, H. Diabetic mice display a delayed adaptive immune response to Mycobacterium tuberculosis. J. Immunol. 2010, 184, 6275–6282. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Before PS matching | After PS matching | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall (N = 74,753) | Antiplatelet users (N = 9497) | Non-users (n = 65,256) | p value * | Overall (n = 17,728) | Antiplatelet users (N = 8864) | Non-users (n = 8864) | p value * | |||||
| All (n = 9497) | ASA (n = 7764) | Non-ASA (n = 1855) | All (n = 8864) | ASA (n = 7281) | Non-ASA (n = 1704) | |||||||
| Age (mean ± SD) | 63.6 ± 18.5 | 76.1 ± 10.6 | 75.7 ± 10.7 | 77.5 ± 9.9 | 61.7 ± 19.7 | < 0.001 | 75.9 ± 10.6 | 75.7 ± 10.6 | 75.4 ± 10.7 | 77.2 ± 9.9 | 76.0 ± 10.6 | 0.063 |
| Male sex | 52,155 (69.8%) | 7019 (73.9%) | 5702 (73.4%) | 1409 (76.0%) | 45,136 (69.2%) | < 0.001 | 13,059 (73.7%) | 6568 (74.1%) | 5368 (73.7%) | 1295 (76.0%) | 6,491 (73.2%) | 0.195 |
| Low income | 4,005 (5.4%) | 303 (3.2%) | 250 (3.2%) | 59 (3.2%) | 3702 (5.7%) | < 0.001 | 529 (3.0%) | 286 (3.2%) | 234 (3.2%) | 47 (2.8%) | 243 (2.7%) | 0.064 |
| CCI (mean ± SD) | 3.7 ± 2.1 | 5.1 ± 2.0 | 5.0 ± 2.0 | 5.6 ± 2.1 | 3.5 ± 2.6 | < 0.001 | 5.1 ± 2.0 | 5.1 ± 2.0 | 4.9 ± 2.0 | 5.5 ± 2.1 | 5.1 ± 2.0 | 0.804 |
| CAD | 20,975 (28.1%) | 6,571 (69.2%) | 5263 (67.8%) | 1444 (77.8%) | 14,404 (22.1%) | < 0.001 | 12,303 (69.4%) | 6097 (68.8%) | 4911 (67.5%) | 1,319 (77.4%) | 6206 (70.0%) | 0.078 |
| Stroke | 6313 (8.5%) | 2610 (27.5%) | 1968 (25.4%) | 655 (35.3%) | 3703 (5.7%) | < 0.001 | 4550 (25.7%) | 2381 (26.9%) | 1799 (24.7%) | 599 (35.2%) | 2169 (24.5%) | < 0.001 |
| DM | 14,779 (19.8%) | 3604 (38.0%) | 2950 (38.0%) | 717 (38.7%) | 11,175 (17.1%) | < 0.001 | 6666 (37.6%) | 3365 (38.0%) | 2775 (38.1%) | 654 (38.4%) | 3301 (37.2%) | 0.329 |
| ESRD | 1911 (2.6%) | 500 (5.3%) | 325 (4.2%) | 207 (11.2%) | 1411 (2.2%) | < 0.001 | 885 (5.0%) | 451 (5.1%) | 293 (4.0%) | 185 (10.9%) | 434 (4.9%) | 0.581 |
| Cancer | 7730 (10.3%) | 1086 (11.4%) | 839 (10.8%) | 253 (13.6%) | 6,644 (10.2%) | < 0.001 | 1969 (11.1%) | 993 (11.2%) | 773 (10.6%) | 231 (13.6%) | 976 (11.0%) | 0.702 |
| AIDS | 491 (0.7%) | 7 (0.1%) | 7 (0.1%) | 0 (0%) | 484 (0.7%) | < 0.001 | 10 (0.1%) | 7 (0.1%) | 7 (0.1%) | 0 (0%) | 3 (0.03%) | 0.343 |
| RA | 1004 (1.3%) | 127 (1.3%) | 101 (1.3%) | 33 (1.8%) | 877 (1.3%) | 0.996 | 242 (1.4%) | 118 (1.3%) | 95 (1.3%) | 30 (1.8%) | 124 (1.4%) | 0.746 |
| Psoriasis | 705 (0.9%) | 114 (1.2%) | 78 (1.0%) | 36 (1.9%) | 591 (0.9%) | 0.007 | 211 (1.2%) | 104 (1.2%) | 73 (1.0%) | 30 (1.8%) | 107 (1.2%) | 0.890 |
| AS | 613 (0.8%) | 97 (1.0%) | 75 (1.0%) | 22 (1.2%) | 516 (0.8%) | 0.023 | 173 (1.0%) | 92 (1.0%) | 70 (1.0%) | 22 (1.3%) | 81 (0.9%) | 0.445 |
| COPD | 13,187 (17.6%) | 2660 (28.0%) | 2135 (27.5%) | 568 (30.6%) | 10,527 (16.1%) | < 0.001 | 5045 (28.5%) | 2,503 (28.2%) | 2,014 (27.7%) | 535 (31.4%) | 2,542 (28.7%) | 0.527 |
| Transplant | 135 (0.2%) | 24 (0.3%) | 17 (0.2%) | 8 (0.4%) | 111 (0.2%) | 0.101 | 40 (0.2%) | 24 (0.3%) | 17 (0.2%) | 8 (0.5%) | 16 (0.2%) | 0.268 |
| Pneumoconiosis | 69 (0.1%) | 13 (0.1%) | 11 (0.1%) | ** | 56 (0.1%) | NS | 20 (0.1%) | 11 (0.1%) | 9 (0.1%) | ** | 9 (0.1%) | NS |
| Bronchiectasis | 1474 (2.0%) | 233 (2.5%) | 192 (2.5%) | 46 (2.5%) | 1241 (1.9%) | < 0.001 | 462 (2.6%) | 216 (2.4%) | 177 (2.4%) | 42 (2.5%) | 246 (2.8%) | 0.172 |
| Hypertension | 37867 (50.7%) | 8688 (91.5%) | 7095 (91.4%) | 1717 (92.6%) | 29179 (44.7%) | < 0.001 | 16259 (91.7%) | 8095 (91.3%) | 6646 (91.3%) | 1572 (92.2%) | 8164 (92.1%) | 0.064 |
| TB severity | ||||||||||||
| Smear positive | 30,257 (40.5%) | 3445 (36.3%) | 2873 (37.0%) | 621 (33.5%) | 26,812 (41.1%) | < 0.001 | 6731 (38.0%) | 3348 (37.8%) | 2795 (38.4%) | 604 (35.6%) | 3383 (38.2%) | 0.599 |
| Culture positive | 56,383 (75.4%) | 7343 (77.3%) | 6030 (77.7%) | 1389 (74.9%) | 49,040 (75.2%) | < 0.001 | 13,575 (76.6%) | 6784 (76.5%) | 5598 (76.9%) | 1,263 (74.1%) | 6791 (76.6%) | 0.915 |
| Cavitation | 12,092 (16.2%) | 950 (10.0%) | 832 (10.7%) | 120 (6.5%) | 11,142 (17.1%) | < 0.001 | 1832 (10.3%) | 927 (10.5%) | 816 (11.2%) | 114 (6.7%) | 905 (10.2%) | 0.604 |
| ASA (n = 7281) | Matched non-user (n = 7281) | p value | Non-ASA (n = 1704) | Matched non-user (n = 1704) | p value | |
|---|---|---|---|---|---|---|
| Age (mean ± SD) | 75.4 ± 10.7 | 75.7 ± 10.7 | 0.072 | 77.2 ± 9.9 | 77.6 ± 9.8 | 0.244 |
| Male sex | 5368 (73.7%) | 5317 (73.0%) | 0.349 | 1295 (76.0%) | 1275 (74.8%) | 0.450 |
| Low income | 234 (3.2%) | 198 (2.7%) | 0.087 | 47 (2.8%) | 43(2.5%) | 0.749 |
| CCI | 4.9 ± 2.0 | 5.0 ± 2.0 | 0.474 | 5.5 ± 2.1 | 5.5 ± 2.1 | 0.634 |
| Coronary artery disease | 4911 (67.5%) | 4990 (68.5%) | 0.166 | 1319 (77.4%) | 1339 (78.6%) | 0.432 |
| Stroke | 1799 (24.7%) | 1647 (22.6%) | 0.003 | 599 (35.2%) | 551 (32.3%) | 0.089 |
| Diabetes mellitus | 2775 (38.1%) | 2715 (37.3%) | 0.313 | 654 (38.4%) | 649 (38.1%) | 0.888 |
| End-stage renal disease | 293 (4.0%) | 306 (4.2%) | 0.617 | 185 (10.9%) | 136 (8.0%) | 0.005 |
| Cancer | 773 (10.6%) | 778 (10.7%) | 0.914 | 231 (13.6%) | 210 (12.3%) | 0.307 |
| AIDS | 7 (0.1%) | 3 (0.04%) | 0.343 | 0 (0%) | 0 (0%) | > 0.999 |
| Rheumatoid arthritis | 95 (1.3%) | 96 (1.3%) | > 0.999 | 30 (1.8%) | 27 (1.6%) | 0.789 |
| Psoriasis | 73 (1.0%) | 81 (1.1%) | 0.571 | 30 (1.8%) | 26 (1.5%) | 0.686 |
| Ankylosing spondylitis | 70 (1.0%) | 66 (0.9%) | 0.796 | 22 (1.3%) | 15 (0.9%) | 0.321 |
| COPD | 2014 (27.7%) | 2051 (28.2%) | 0.506 | 535 (31.4%) | 533 (31.3%) | 0.971 |
| Transplant | 17 (0.2%) | 14 (0.2%) | 0.719 | 8 (0.5%) | 5 (0.3%) | 0.578 |
| Pneumoconiosis | 9 (0.1%) | 8 (0.1%) | > 0.999 | ** | ** | NS |
| Bronchiectasis | 177 (2.4%) | 203 (2.8%) | 0.194 | 42 (2.5%) | 47 (2.8%) | 0.668 |
| Tuberculosis severity | ||||||
| Smear positive | 2795 (38.4%) | 2829 (38.9%) | 0.574 | 604 (35.6%) | 609 (35.8%) | 0.886 |
| Culture positive | 5598 (76.9%) | 5602 (76.9%) | 0.953 | 1263 (74.1%) | 1272 (74.7%) | 0.754 |
| Cavitation | 816 (11.2%) | 785 (10.8%) | 0.427 | 114 (6.7%) | 120 (7.0%) | 0.735 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.-R.; Lee, M.-C.; Chang, C.-H.; Liu, C.-J.; Chang, L.-Y.; Zhang, J.-F.; Wang, J.-Y.; Lee, C.-H. Use of Antiplatelet Agents and Survival of Tuberculosis Patients: A Population-Based Cohort Study. J. Clin. Med. 2019, 8, 923. https://doi.org/10.3390/jcm8070923
Lee M-R, Lee M-C, Chang C-H, Liu C-J, Chang L-Y, Zhang J-F, Wang J-Y, Lee C-H. Use of Antiplatelet Agents and Survival of Tuberculosis Patients: A Population-Based Cohort Study. Journal of Clinical Medicine. 2019; 8(7):923. https://doi.org/10.3390/jcm8070923
Chicago/Turabian StyleLee, Meng-Rui, Ming-Chia Lee, Chia-Hao Chang, Chia-Jung Liu, Lih-Yu Chang, Jun-Fu Zhang, Jann-Yuan Wang, and Chih-Hsin Lee. 2019. "Use of Antiplatelet Agents and Survival of Tuberculosis Patients: A Population-Based Cohort Study" Journal of Clinical Medicine 8, no. 7: 923. https://doi.org/10.3390/jcm8070923
APA StyleLee, M.-R., Lee, M.-C., Chang, C.-H., Liu, C.-J., Chang, L.-Y., Zhang, J.-F., Wang, J.-Y., & Lee, C.-H. (2019). Use of Antiplatelet Agents and Survival of Tuberculosis Patients: A Population-Based Cohort Study. Journal of Clinical Medicine, 8(7), 923. https://doi.org/10.3390/jcm8070923