Antiarrhythmic Effect of Sacubitril-Valsartan: Cause or Consequence of Clinical Improvement?


 , ,
, ,
Abstract
1. Introduction
2. Experimental Section
2.1. Patient Population
2.2. Definition of Chronic HF with Optimized Standard of Care Therapy
2.3. Study Protocol
2.4. ECG
2.5. Transthoracic Echocardiogram
2.6. Statistical Analysis
3. Results
3.1. Overview of the Study Population
3.2. LCZ696 dose
3.3. ECG Analysis
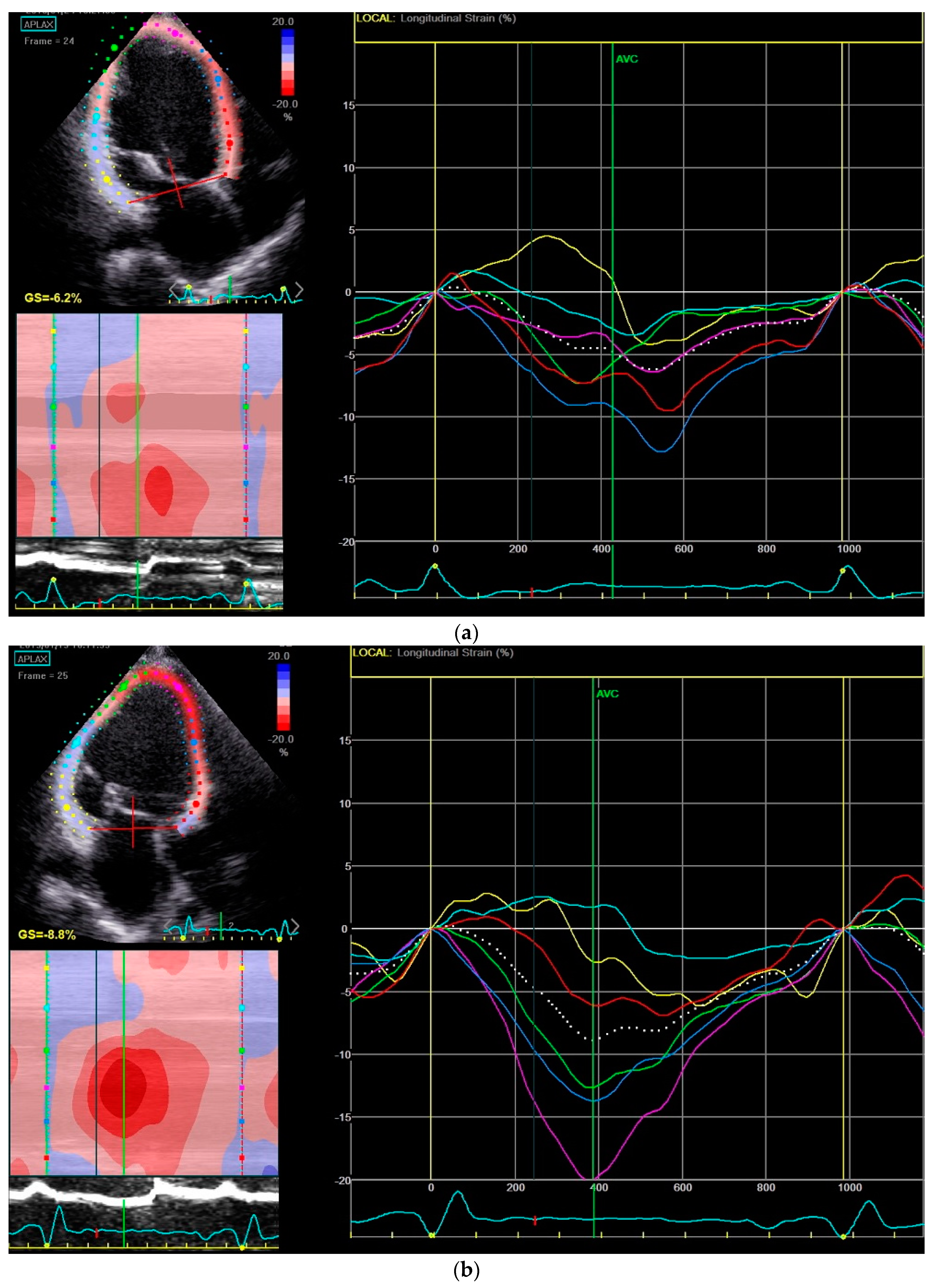
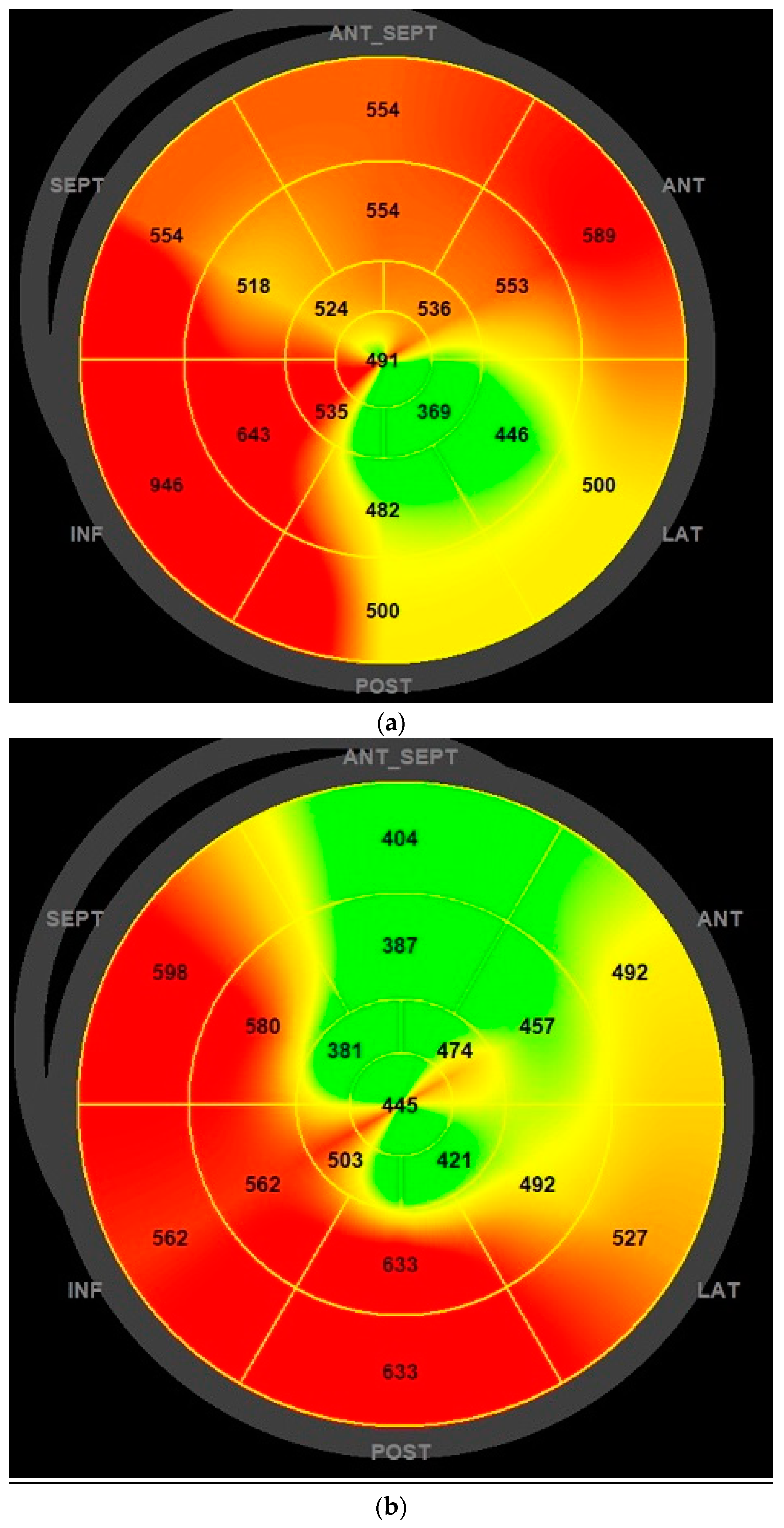
3.4. Transthoracic Echocardiogram Analysis
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar]
- Desai, A.S.; McMurray, J.J.; Packer, M.; Swedberg, K.; Rouleau, J.L.; Chen, F.; Gong, J.; Rizkala, A.R.; Brahimi, A.; Claggett, B.; et al. Effect of the angiotensin-receptor-neprilysin inhibitor LCZ696 compared with enalapril on mode of death in heart failure patients. Eur. Heart J. 2015, 36, 1990–1997. [Google Scholar] [CrossRef] [PubMed]
- Martens, P.; Nuyens, D.; Rivero-Ayerza, M.; Van Herendael, H.; Vercammen, J.; Ceyssens, W.; Luwel, E.; Dupont, M.; Mullens, W. Sacubitril/valsartan reduces ventricular arrhythmias in parallel with left ventricular reverse remodeling in heart failure with reduced ejection fraction. Clin. Res. Cardiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- De Diego, C.; Gonzalez-Torres, L.; Núñez, J.M.; Inda, R.C.; Martin-Langerwerf, D.A.; Sangio, A.D.; Chochowski, P.; Casasnovas, P.; Blazquez, J.C.; Almendral, J. Effects of angiotensin-neprilysin inhibition compared to angiotensin inhibition on ventricular arrhythmias in reduced ejection fraction patients under continuous remote monitoring of implantable defibrillator devices. Heart Rhythm. 2018, 15, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Flather, M.D.; Yusuf, S.; Køber, L.; Pfeffer, M.; Hall, A.; Murray, G.; Torp-Pedersen, C.; Ball, S.; Pogue, J.; Moyé, L.; et al. Long-term ACE-inhibitor therapy in patients with heart failure or left-ventricular dysfunction: A systematic overview of data from individual patients. ACE-Inhibitor Myocardial Infarction Collaborative Group. Lancet 2000, 355, 1575–1581. [Google Scholar] [CrossRef]
- Garg, R.; Yusuf, S. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. Collaborative Group on ACE Inhibitor Trials. JAMA 1995, 273, 1450–1456. [Google Scholar] [CrossRef]
- Al-Gobari, M.; Al-Aqeel, S.; Gueyffier, F.; Burnand, B. Effectiveness of drug interventions to prevent sudden cardiac death in patients with heart failure and reduced ejection fraction: An overview of systematic reviews. BMJ Open 2018, 8, e021108. [Google Scholar] [CrossRef]
- Iborra-Egea, O.; Gálvez-Montón, C.; Roura, S.; Perea-Gil, I.; Prat-Vidal, C.; Soler-Botija, C.; Bayes-Genis, A. Mechanisms of action of sacubitril/valsartan on cardiac remodeling: A systems biology approach. NPJ Syst. Biol. Appl. 2017, 3, 12. [Google Scholar] [CrossRef]
- Sarrias, A.; Bayes-Genis, A. Is Sacubitril/Valsartan (Also) an Antiarrhythmic Drug? Circulation 2018, 138, 551–553. [Google Scholar] [CrossRef]
- Okutucu, S.; Sabanoglu, C.; Yetis Sayin, B.; Aksoy, H.; Bursa, N.; Oto, A. Switching from ramipril to sacubitril/valsartan favorably alters electrocardiographic indices of ventricular repolarization in heart failure with reduced ejection fraction. Acta Cardiol. 2018, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Banasik, G.; Segiet, O.; Elwart, M.; Szulik, M.; Lenarczyk, R.; Kalarus, Z.; Kukulski, T. LV mechanical dispersion as a predictor of ventricular arrhythmia in patients with advanced systolic heart failure: A pilot study. Herz 2016, 41, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Haugaa, K.H.; Grenne, B.L.; Eek, C.H.; Ersbøll, M.; Valeur, N.; Svendsen, J.H.; Florian, A.; Sjøli, B.; Brunvand, H.; Køber, L.; et al. Strain echocardiography improves risk prediction of ventricular arrhythmias after myocardial infarction. JACC Cardiovasc. Imaging 2013, 6, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Kligfield, P.; Gettes, L.S.; Bailey, J.J.; Childers, R.; Deal, B.J.; Hancock, E.W.; Van Herpen, G.; Kors, J.A.; Macfarlane, P.; Mirvis, D.M.; et al. Recommendations for the standardization and interpretation of the electrocardiogram: Part I: The electrocardiogram and its technology. A scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Heart Rhythm 2007, 4, 394–412. [Google Scholar] [PubMed]
- Surawicz, B.; Childers, R.; Deal, B.J.; Gettes, L.S.; Bailey, J.J.; Gorgels, A. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part III: Intraventricular conduction disturbances: A scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J. Am. Coll. Cardiol. 2009, 53, 976–981. [Google Scholar] [PubMed]
- Rautaharju, P.M.; Surawicz, B.; Gettes, L.S.; Bailey, J.J.; Childers, R.; Deal, B.J. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part IV: The ST segment, T and U waves, and the QT interval: A scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J. Am. Coll. Cardiol. 2009, 53, 982–991. [Google Scholar] [PubMed]
- Bazett, H.C. The time relations of the blood-pressure changes after excision of the adrenal glands, with some observations on blood volume changes. J. Physiol. 1920, 53, 320–339. [Google Scholar] [CrossRef] [PubMed]
- Sokolow, M.; Lyon, T.P. The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am. Heart J. 1949, 37, 161–186. [Google Scholar] [CrossRef]
- Al-Gobari, M.; El Khatib, C.; Pillon, F.; Gueyffier, F. β-Blockers for the prevention of sudden cardiac death in heart failure patients: A meta-analysis of randomized controlled trials. BMC Cardiovasc. Disord. 2013, 13, 52. [Google Scholar] [CrossRef]
- Chatterjee, S.; Biondi-Zoccai, G.; Abbate, A.; D’Ascenzo, F.; Castagno, D.; Van Tassell, B.; Mukherjee, D.; Lichstein, E. Benefits of beta blockers in patients with heart failure and reduced ejection fraction: Network meta-analysis. BMJ 2013, 346, f55. [Google Scholar] [CrossRef]
- Le, H.H.; El-Khatib, C.; Mombled, M.; Guitarian, F.; Al-Gobari, M.; Fall, M.; Janiaud, P.; Marchant, I.; Cucherat, M.; Bejan-Angoulvant, T.; et al. Impact of Aldosterone Antagonists on Sudden Cardiac Death Prevention in Heart Failure and Post-Myocardial Infarction Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2016, 11, e0145958. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Ni, J.; Huang, D.; Chen, M.; Yan, S.; Peng, Y. The effect of aldosterone antagonists for ventricular arrhythmia: A meta-analysis. Clin. Cardiol. 2010, 33, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Martens, P.; Belien, H.; Dupont, M.; Mullens, W. Insights into implementation of sacubitril/valsartan into clinical practice. ESC Heart Fail. 2018, 5, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Sundstrom, J.; Lind, L.; Andren, B.; Lithell, H. Left ventricular geometry and function are related to electrocardiographic characteristics and diagnoses. Clin. Physiol. 1998, 18, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Antman, E.M.; Green, L.H.; Grossman, W. Physiologic determinants of the electrocardiographic diagnosis of left ventricular hypertrophy. Circulation 1979, 60, 386–396. [Google Scholar] [CrossRef]
- Køber, L.; Thune, J.J.; Nielsen, J.C.; Haarbo, J.; Videbæk, L.; Korup, E.; Jensen, G.; Hildebrandt, P.; Steffensen, F.H.; Bruun, N.E.; et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N. Engl. J. Med. 2016, 375, 1221–1230. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Mean age (years) | 58.6 ± 11.1 |
| Ischemic etiology | 15 (42.9%) |
| Male gender | 29 (82.9%) |
| New York Heart Association (NYHA) ≥ III | 18 (51.4%) |
| Mean body mass index (kg/m2) | 28.09 ± 3.77 |
| Heart failure hospitalization in the previous year | 15 (42.9%) |
| Median brain natriuretic peptide (BNP) (pg/mL) and interquartile range | 314 (132 to 401) |
| Current smokers | 7 (20.0%) |
| Previous hypertension | 25 (71.4%) |
| Dyslipidemia | 25 (71.4%) |
| Diabetes mellitus | 11 (31.4%) |
| Peripheral artery disease | 4 (11.4%) |
| Familiar history of heart failure | 1 (2.9%) |
| Atrial fibrillation | 14 (40%) |
| Chronic kidney disease | 2 (5.7%) |
| Chronic liver disease | 0 (0.0%) |
| Angiotensin-converting enzyme inhibitors | 29 (82.9%) |
| Angiotensin II receptor blocker | 6 (17.1%) |
| Beta-blockers | 35 (100.0%) |
| Mineralocorticoid receptor antagonist | 33 (94.3%) |
| Ivabradine | 13 (37.1%) |
| Digoxin | 9 (25.7%) |
| Amiodarone | 9 (25.7%) |
| Implantable cardioverter defibrillator | 30 (85.6%) |
| Cardiac resynchronization therapy (CRT-D) | 7 (20%) |
| Percutaneous mitral-valve repair | 3 (8.6%) |
| Electrocardiographic Data | Time 0 | 6 Months | p |
|---|---|---|---|
| Heart rate (bpm) | 72.3 ± 13.0 | 67.1 ± 11.6 | 0.067 |
| PQ interval (ms) | 176.6 ± 21.4 | 174.6 ± 24.8 | 0.724 |
| QRS duration (ms) | 125.1 ± 33.5 | 120.8 ± 31.1 | 0.033 |
| QTc interval (ms) | 451.9 ± 48.1 | 426.0 ± 46.1 | <0.001 |
| SV1 + RV5/6 (mm) | 21.2 ± 11.9 | 16.9 ± 9.8 | 0.001 |
| Biventricular pacing (% n = 8) | 97.4 ± 3.4 | 99.0 ± 0.8 | 0.183 |
| Echocardiographic Data | Time 0 | 6 Months | p |
|---|---|---|---|
| Left ventricular end-diastolic diameter (mm) | 71.3 ± 8.4 | 66.9 ± 7.6 | 0.001 |
| Left ventricular end-systolic diameter (mm) | 57.8 ± 9.4 | 53.1 ± 9.3 | 0.002 |
| Interventricular septum thickness (mm) | 9.6 ± 1.7 | 9.9 ± 1.9 | 0.280 |
| Left ventricular ejection fraction (%) | 29.3 ± 6.4 | 35.2 ± 8.6 | 0.001 |
| Global longitudinal strain (%) | −7.0 ± 2.6 | −8.9 ± 2.8 | 0.001 |
| Mechanical dispersion (ms) | 88.4 ± 28.1 | 78.1 ± 26.1 | 0.036 |
| Left atrium volume (ml/m2) | 51.5 ± 22.6 | 43.7 ± 15.8 | 0.004 |
| Right atrium volume (ml/m2) | 33.1 ± 4.4 | 28.5 ± 13.5 | 0.036 |
| Tricuspid annular systolic excursion (mm) | 19.2 ± 4.4 | 20.0 ± 4.8 | 0.404 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valentim Gonçalves, A.; Pereira-da-Silva, T.; Galrinho, A.; Rio, P.; Moura Branco, L.; Soares, R.; Feliciano, J.; Ilhão Moreira, R.; Cruz Ferreira, R. Antiarrhythmic Effect of Sacubitril-Valsartan: Cause or Consequence of Clinical Improvement? J. Clin. Med. 2019, 8, 869. https://doi.org/10.3390/jcm8060869
Valentim Gonçalves A, Pereira-da-Silva T, Galrinho A, Rio P, Moura Branco L, Soares R, Feliciano J, Ilhão Moreira R, Cruz Ferreira R. Antiarrhythmic Effect of Sacubitril-Valsartan: Cause or Consequence of Clinical Improvement? Journal of Clinical Medicine. 2019; 8(6):869. https://doi.org/10.3390/jcm8060869
Chicago/Turabian StyleValentim Gonçalves, António, Tiago Pereira-da-Silva, Ana Galrinho, Pedro Rio, Luísa Moura Branco, Rui Soares, Joana Feliciano, Rita Ilhão Moreira, and Rui Cruz Ferreira. 2019. "Antiarrhythmic Effect of Sacubitril-Valsartan: Cause or Consequence of Clinical Improvement?" Journal of Clinical Medicine 8, no. 6: 869. https://doi.org/10.3390/jcm8060869
APA StyleValentim Gonçalves, A., Pereira-da-Silva, T., Galrinho, A., Rio, P., Moura Branco, L., Soares, R., Feliciano, J., Ilhão Moreira, R., & Cruz Ferreira, R. (2019). Antiarrhythmic Effect of Sacubitril-Valsartan: Cause or Consequence of Clinical Improvement? Journal of Clinical Medicine, 8(6), 869. https://doi.org/10.3390/jcm8060869