Association of Glucose Fluctuations with Sarcopenia in Older Adults with Type 2 Diabetes Mellitus

Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Assessment of Clinical Parameters and Comorbidities Associated with Diabetes
2.3. Measurement of Daily Glucose Levels
2.4. Evaluation of Sarcopenia
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Study Participants
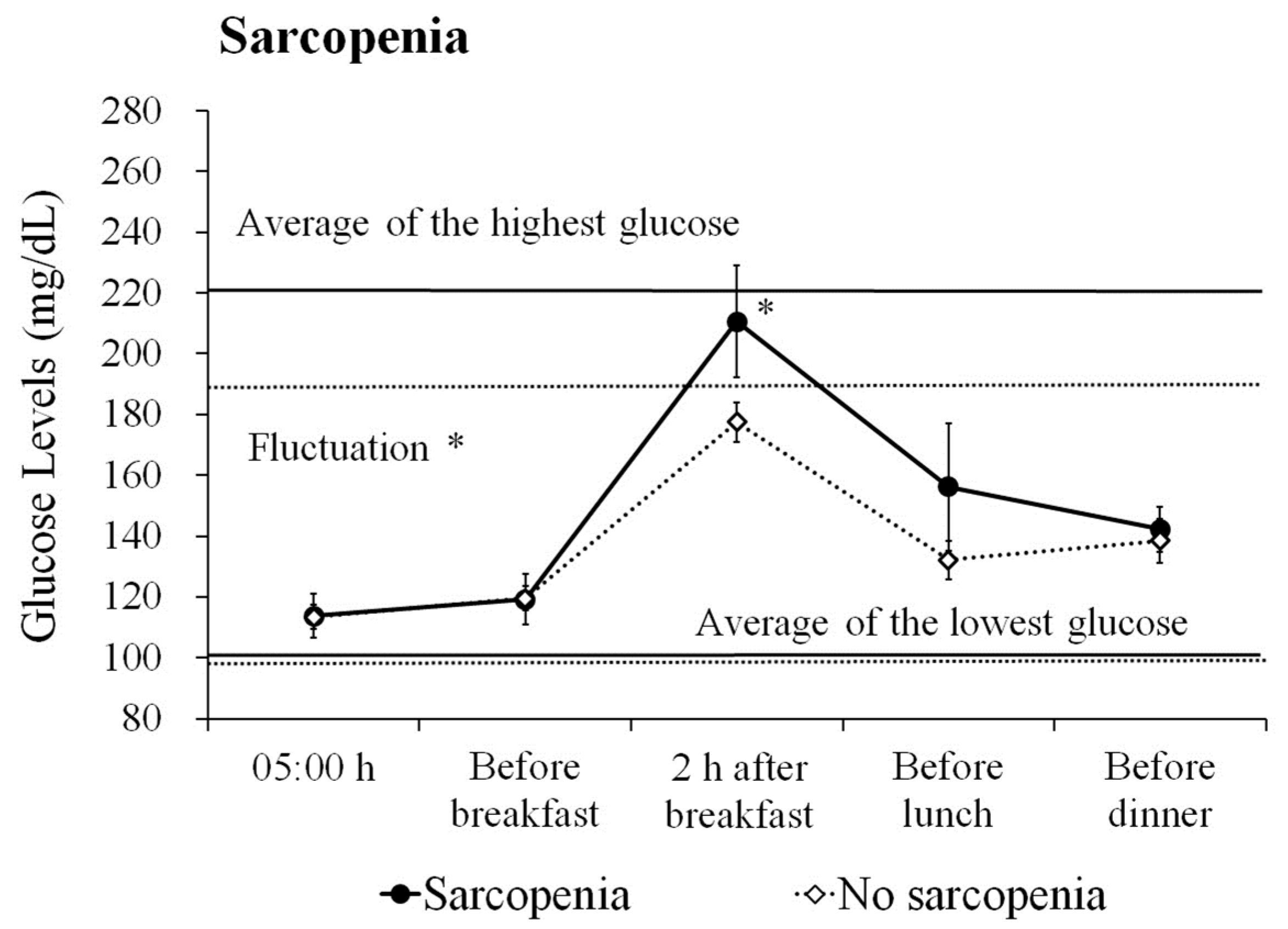
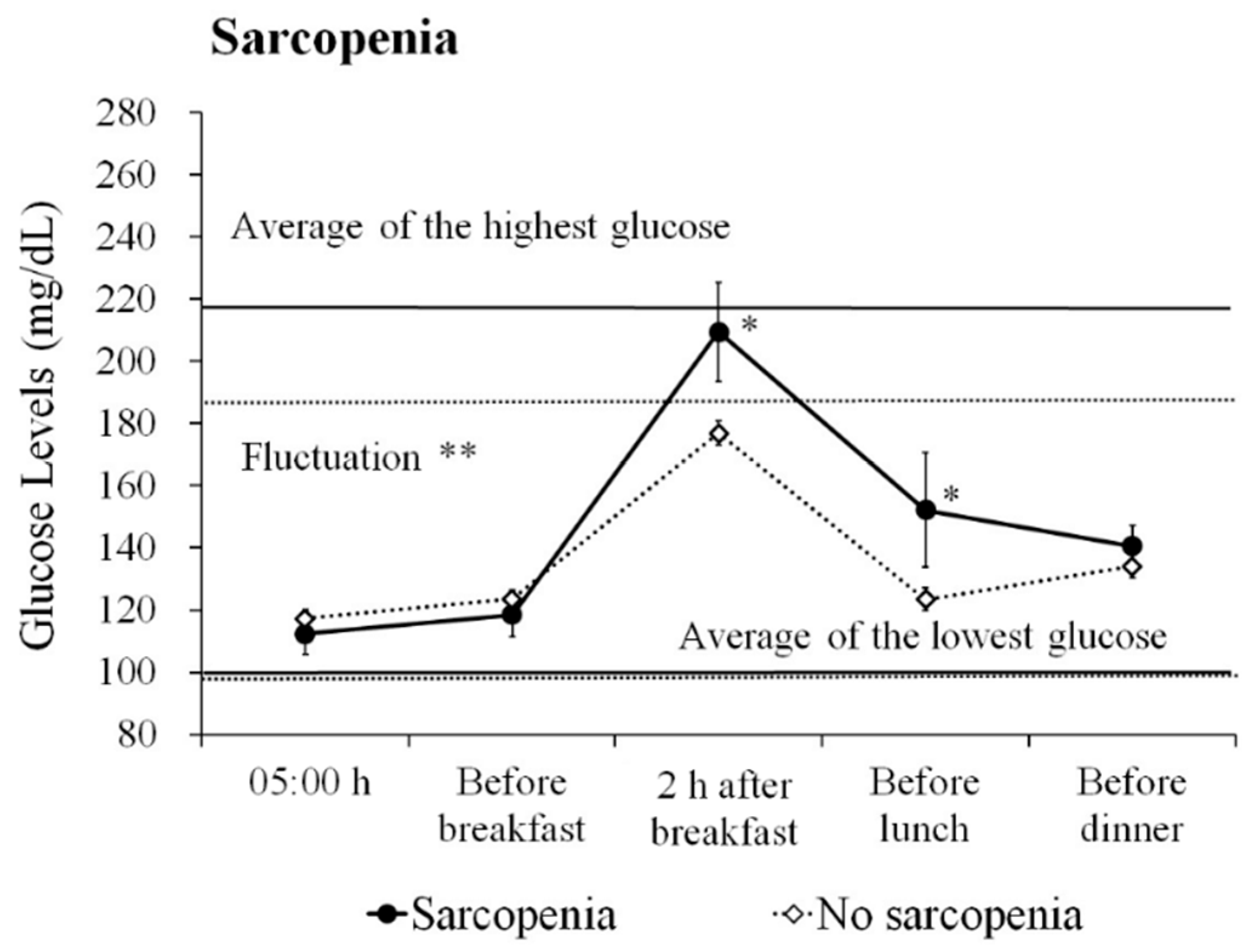
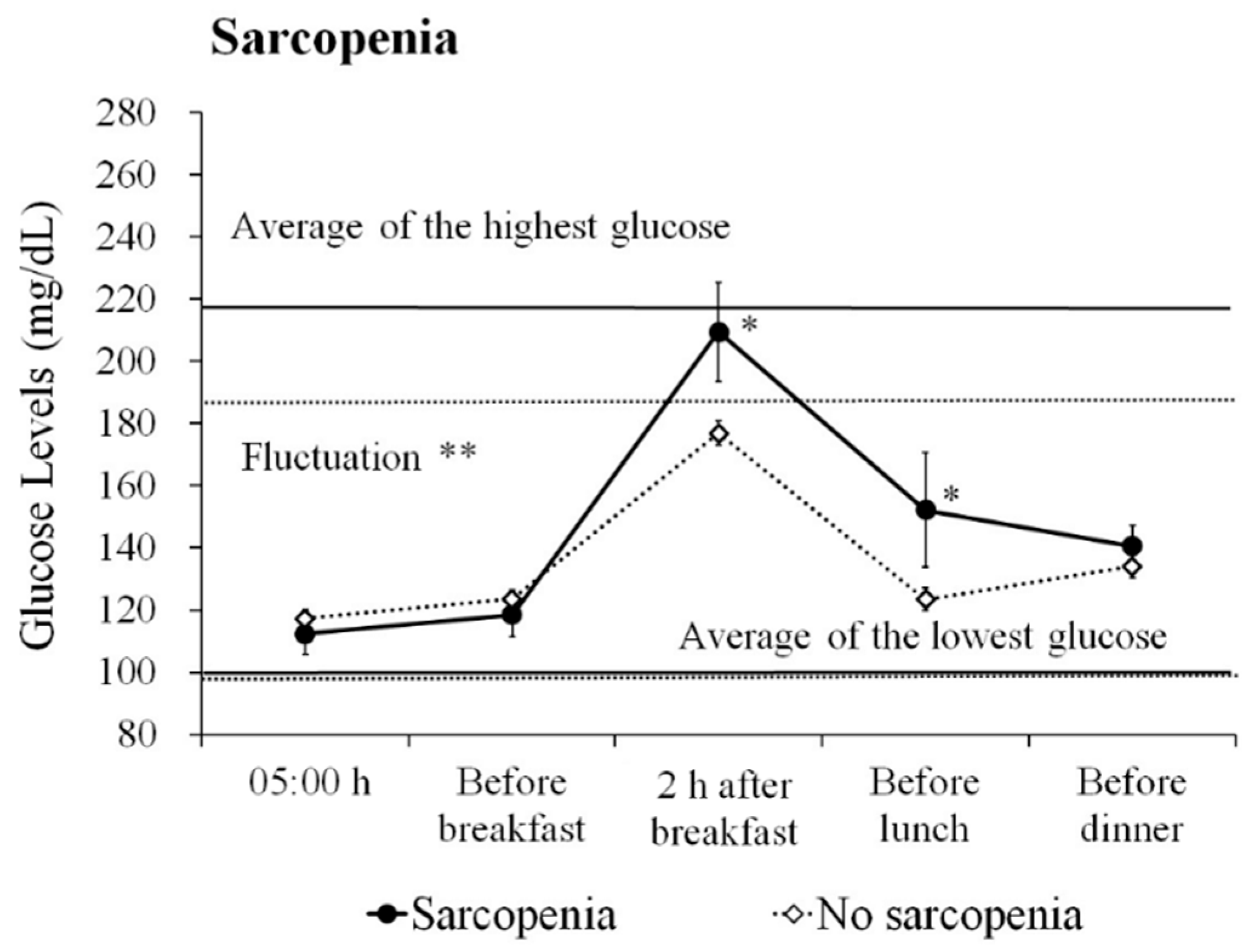
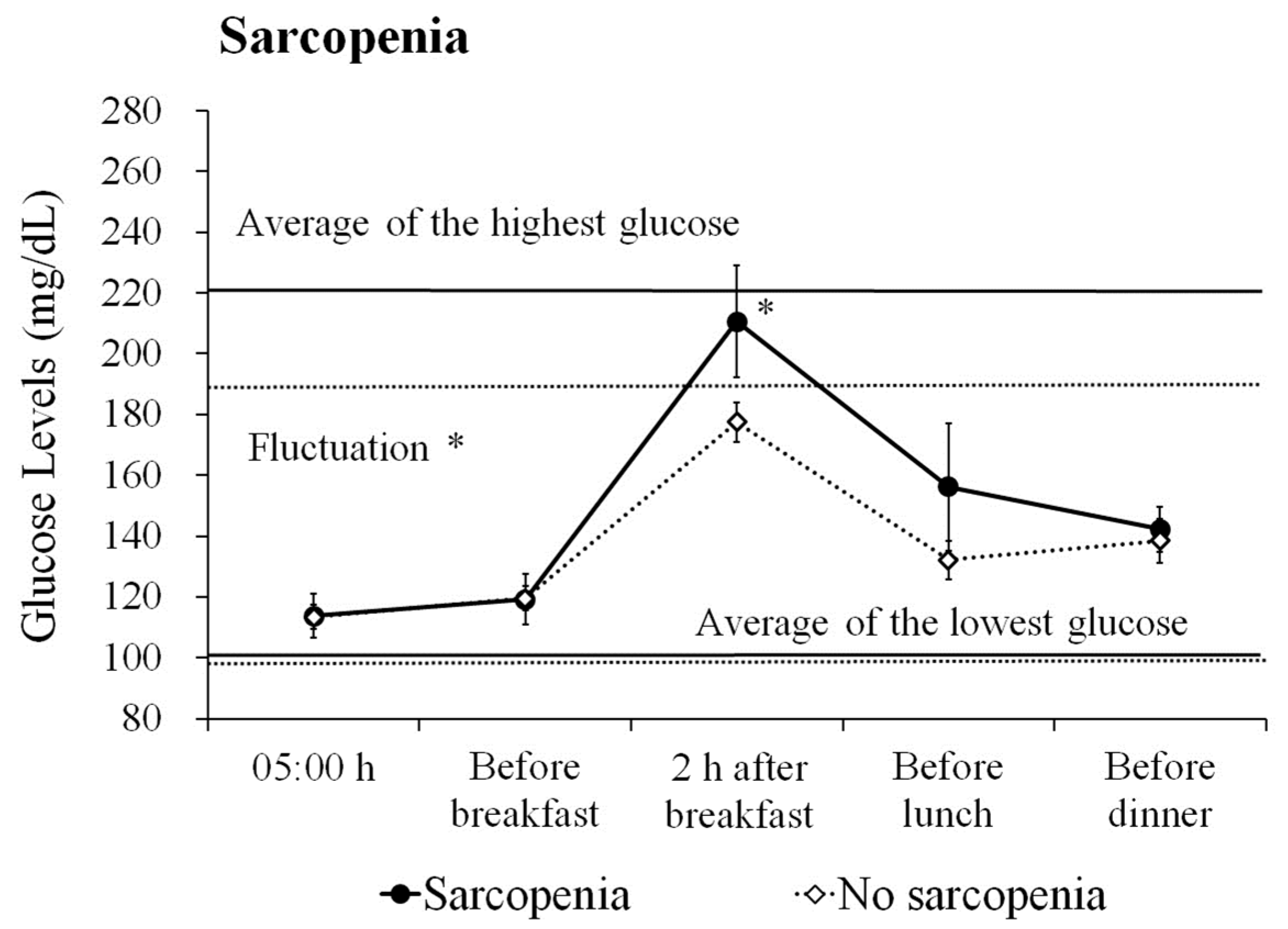
3.2. Differences in Glucose Profiles According to Sarcopenia
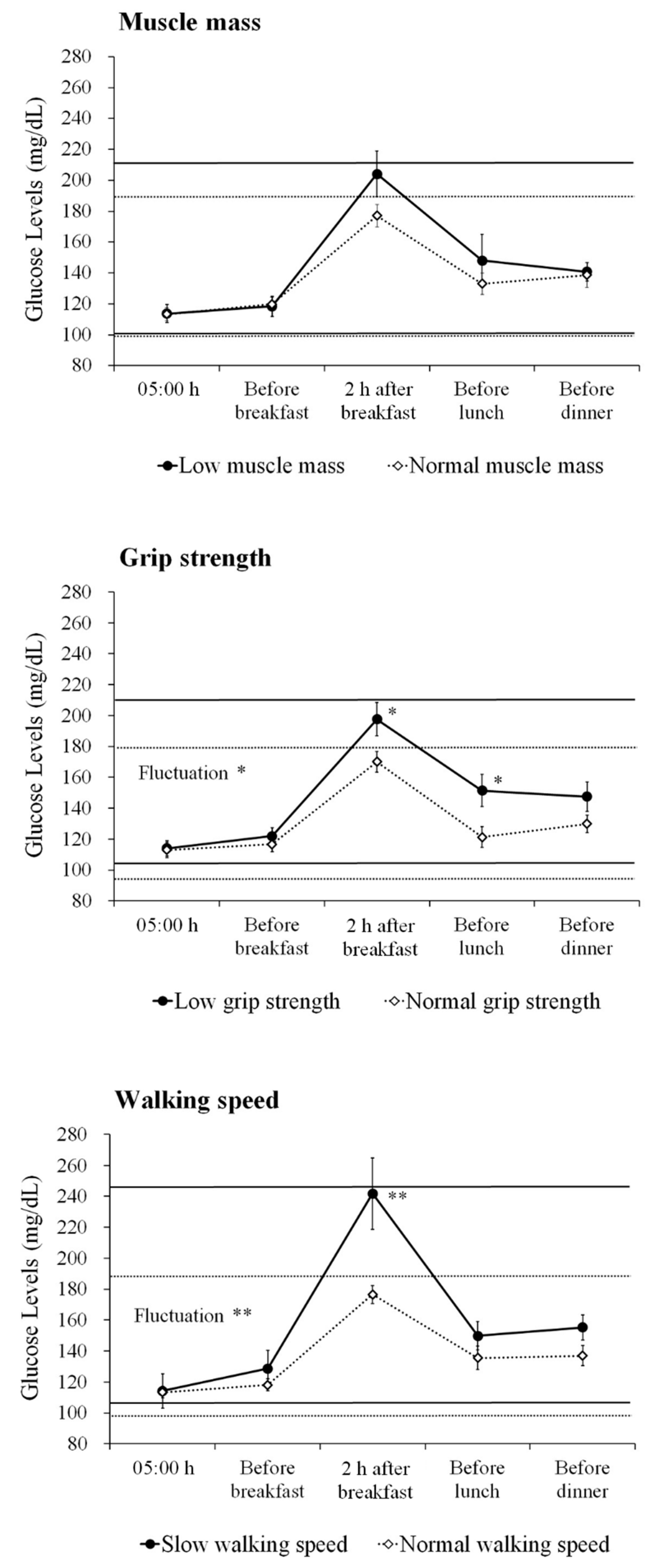
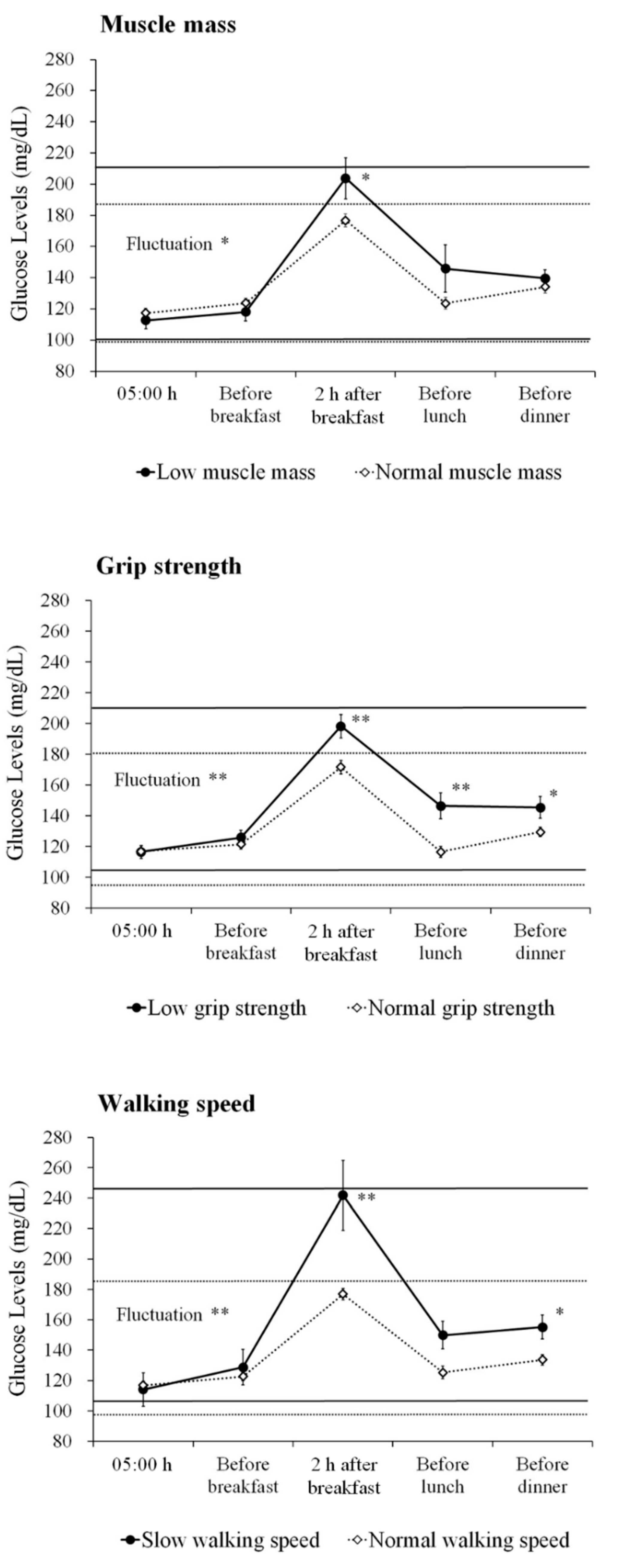
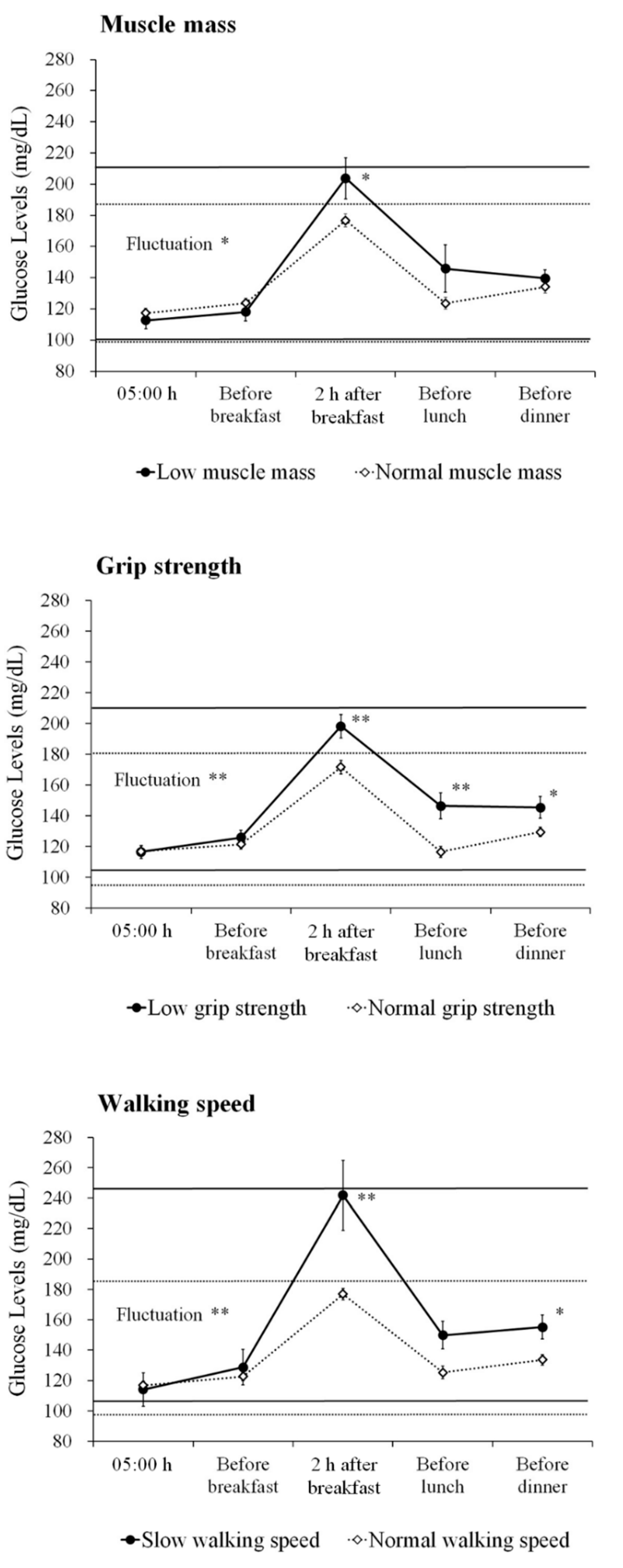
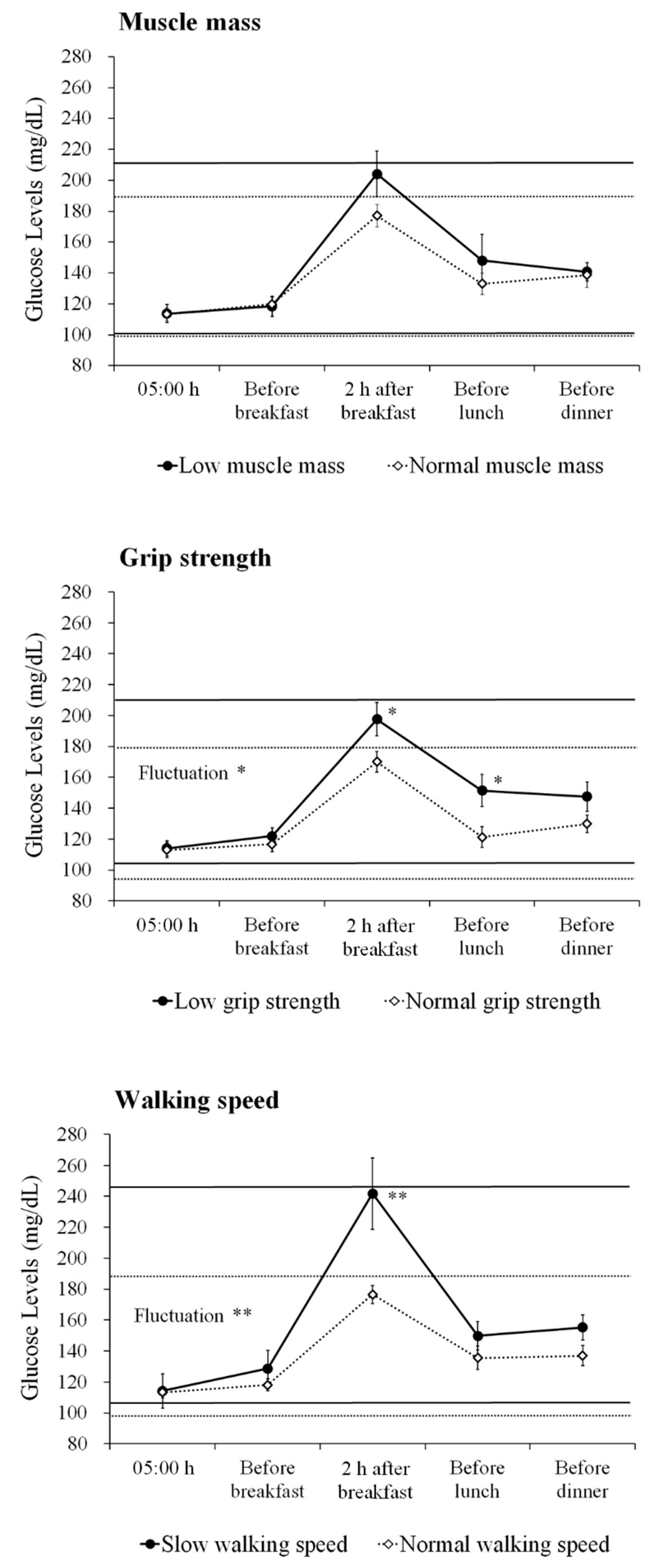
3.3. Differences in Glucose Profiles Based on Sarcopenia Components
3.4. Prevalence of Hypoglycemia and its Association with Sarcopenia
3.5. Association of Glucose Indices with Sarcopenia
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 2018, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Han, A.; Bokshan, S.L.; Marcaccio, S.E.; DePasse, J.M.; Daniels, A.H. Diagnostic Criteria and Clinical Outcomes in Sarcopenia Research: A Literature Review. J. Clin. Med. 2018, 7, E70. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Malmstrom, T.K.; Rodriguez-Manas, L.; Sinclair, A.J. Frailty, sarcopenia and diabetes. J. Am. Med. Dir. Assoc. 2014, 15, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, A.J.; Abdelhafiz, A.H.; Rodriguez-Manas, L. Frailty and sarcopenia-newly emerging and high impact complications of diabetes. J. Diabetes Complicat. 2017, 31, 1465–1473. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.W.; Ha, Y.C.; Kim, K.M.; Moon, J.H.; Choi, S.H.; Lim, S.; Park, Y.J.; Lim, J.Y.; Kim, K.W.; Park, K.S.; et al. Hyperglycemia Is Associated with Impaired Muscle Quality in Older Men with Diabetes: The Korean Longitudinal Study on Health and Aging. Diabetes Metab. J. 2016, 40, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Leenders, M.; Verdijk, L.B.; van der Hoeven, L.; Adam, J.J.; van Kranenburg, J.; Nilwik, R.; van Loon, L.J. Patients with type 2 diabetes show a greater decline in muscle mass, muscle strength, and functional capacity with aging. J. Am. Med. Dir. Assoc. 2013, 14, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Kalyani, R.R.; Metter, E.J.; Egan, J.; Golden, S.H.; Ferrucci, L. Hyperglycemia predicts persistently lower muscle strength with aging. Diabetes Care 2015, 38, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Munshi, M.N.; Segal, A.R.; Slyne, C.; Samur, A.A.; Brooks, K.M.; Horton, E.S. Shortfalls of the use of HbA1C-derived eAG in older adults with diabetes. Diabetes Res. Clin. Pract. 2015, 110, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Munshi, M.N.; Slyne, C.; Segal, A.R.; Saul, N.; Lyons, C.; Weinger, K. Liberating A1C goals in older adults may not protect against the risk of hypoglycemia. J. Diabetes Complicat. 2017, 31, 1197–1199. [Google Scholar] [CrossRef] [PubMed]
- Abdelhafiz, A.H.; McNicholas, E.; Sinclair, A.J. Hypoglycemia, frailty and dementia in older people with diabetes: Reciprocal relations and clinical implications. J. Diabetes Complicat. 2016, 30, 1548–1554. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.M.; Johnson, D.K.; Watts, A.; Swerdlow, R.H.; Brooks, W.M. Reduced lean mass in early Alzheimer disease and its association with brain atrophy. Arch. Neurol. 2010, 67, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, C.; Umegaki, H.; Okamoto, K.; Nakashima, H.; Kuzuya, M.; Toba, K.; Sakurai, T. Physical Function Differences Between the Stages From Normal Cognition to Moderate Alzheimer Disease. J. Am. Med. Dir. Assoc. 2017, 18, e9–e368. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, T.; Nakamura, A.; Kato, T.; Iwata, K.; Saji, N.; Arahata, Y.; Hattori, H.; Bundo, M.; Ito, K.; Niida, S.; et al. Decreased Glucose Metabolism in Medial Prefrontal Areas is Associated with Nutritional Status in Patients with Prodromal and Early Alzheimer’s Disease. J. Alzheimers Dis. 2017, 60, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, T.; Ono, R.; Murata, S.; Saji, N.; Matsui, Y.; Niida, S.; Toba, K.; Sakurai, T. Prevalence and associated factors of sarcopenia in elderly subjects with amnestic mild cognitive impairment or Alzheimer disease. Curr. Alzheimer Res. 2016, 13, 718–726. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef] [PubMed]
- Gnjidic, D.; Hilmer, S.N.; Blyth, F.M.; Naganathan, V.; Waite, L.; Seibel, M.J.; McLachlan, A.J.; Cumming, R.G.; Handelsman, D.J.; Le Couteur, D.G. Polypharmacy cutoff and outcomes: five or more medicines were used to identify community-dwelling older men at risk of different adverse outcomes. J. Clin. Epidemiol. 2012, 65, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Sakurai, T.; Iimuro, S.; Sakamaki, K.; Umegaki, H.; Araki, A.; Ohashi, Y.; Ito, H.; Japanese Elderly Diabetes Intervention Trial Study Group. Risk factors for a 6-year decline in physical disability and functional limitations among elderly people with type 2 diabetes in the Japanese Elderly Diabetes Intervention Trial. Geriatr. Gerontol. Int. 2012, 12, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Monnier, L.; Colette, C.; Dunseath, G.J.; Owens, D.R. The loss of postprandial glycemic control precedes stepwise deterioration of fasting with worsening diabetes. Diabetes Care 2007, 30, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Workgroup on Hypoglycemia, American Diabetes Association. Defining and reporting hypoglycemia in diabetes: a report from the American Diabetes Association Workgroup on Hypoglycemia. Diabetes Care 2005, 28, 1245–1249. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Pagotto, V.; Silveira, E.A. Methods, diagnostic criteria, cutoff points, and prevalence of sarcopenia among older people. ScientificWorldJournal 2014, 2014, 231312. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, R.; Murakami, H.; Sanada, K.; Tanaka, N.; Sawada, S.S.; Tabata, I.; Higuchi, M.; Miyachi, M. Calf circumference as a surrogate marker of muscle mass for diagnosing sarcopenia in Japanese men and women. Geriatr. Gerontol. Int. 2015, 15, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Okochi, J.; Toba, K.; Takahashi, T.; Matsubayashi, K.; Nishinaga, M.; Takahashi, R.; Ohrui, T. Simple screening test for risk of falls in the elderly. Geriatr. Gerontol. Int. 2006, 6, 223–227. [Google Scholar] [CrossRef]
- Abbatecola, A.M.; Paolisso, G.; Fattoretti, P.; Evans, W.J.; Fiore, V.; Dicioccio, L.; Lattanzio, F. Discovering pathways of sarcopenia in older adults: a role for insulin resistance on mitochondria dysfunction. J. Nutr. Health Aging 2011, 15, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, S.T.; Clarke, J.R.; Bomfim, T.R.; De Felice, F.G. Inflammation, defective insulin signaling, and neuronal dysfunction in Alzheimer’s disease. Alzheimers Dement 2014, 10, S76–S83. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, S.; Yakabe, M.; Akishita, M. Age-related sarcopenia and its pathophysiological bases. Inflamm. Regen. 2016, 36, 17. [Google Scholar] [CrossRef] [PubMed]
- Asih, P.R.; Tegg, M.L.; Sohrabi, H.; Carruthers, M.; Gandy, S.E.; Saad, F.; Verdile, G.; Ittner, L.M.; Martins, R.N. Multiple Mechanisms Linking Type 2 Diabetes and Alzheimer’s Disease: Testosterone as a Modifier. J. Alzheimers Dis. 2017, 59, 445–466. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.S.; Yu, L.; Wilson, R.S.; Boyle, P.A.; Schneider, J.A.; Bennett, D.A. Brain pathology contributes to simultaneous change in physical frailty and cognition in old age. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1536–1544. [Google Scholar] [CrossRef] [PubMed]
- Del Campo, N.; Payoux, P.; Djilali, A.; Delrieu, J.; Hoogendijk, E.O.; Rolland, Y.; Cesari, M.; Weiner, M.W.; Andrieu, S.; Vellas, B.; et al. Relationship of regional brain β-amyloid to gait speed. Neurology 2016, 86, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Sato, N.; Morishita, R. The roles of lipid and glucose metabolism in modulation of β-amyloid, tau, and neurodegeneration in the pathogenesis of Alzheimer disease. Front. Aging Neurosci. 2015, 7, 199. [Google Scholar] [CrossRef] [PubMed]
- Vekrellis, K.; Ye, Z.; Qiu, W.Q.; Walsh, D.; Hartley, D.; Chesneau, V.; Rosner, M.R.; Selkoe, D.J. Neurons regulate extracellular levels of amyloid beta-protein via proteolysis by insulin-degrading enzyme. J. Neurosci. 2000, 20, 1657–1665. [Google Scholar] [CrossRef] [PubMed]
- Macauley, S.L.; Stanley, M.; Caesar, E.E.; Yamada, S.A.; Raichle, M.E.; Perez, R.; Mahan, T.E.; Sutphen, C.L.; Holtzman, D.M. Hyperglycemia modulates extracellular amyloid-β concentrations and neuronal activity in vivo. J. Clin. Investig. 2015, 125, 2463–2467. [Google Scholar] [CrossRef] [PubMed]
- Roher, A.E.; Esh, C.L.; Kokjohn, T.A.; Castano, E.M.; Van Vickle, G.D.; Kalback, W.M.; Patton, R.L.; Luehrs, D.C.; Daugs, I.D.; Kuo, Y.M.; et al. Amyloid beta peptides in human plasma and tissues and their significance for Alzheimer’s disease. Alzheimers Dement 2009, 5, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, M.; Sato, N. Bidirectional interactions between diabetes and Alzheimer’s disease. Neurochem. Int. 2017, 108, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Monnier, L.; Mas, E.; Ginet, C.; Michel, F.; Villon, L.; Cristol, J.P.; Colette, C. Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. JAMA 2006, 295, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Smith-Palmer, J.; Brandle, M.; Trevisan, R.; Orsini Federici, M.; Liabat, S.; Valentine, W. Assessment of the association between glycemic variability and diabetes-related complications in type 1 and type 2 diabetes. Diabetes Res. Clin. Pract. 2014, 105, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Gella, A.; Durany, N. Oxidative stress in Alzheimer disease. Cell Adh. Migr. 2009, 3, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Ogama, N.; Sakurai, T.; Kawashima, S.; Tanikawa, T.; Tokuda, H.; Satake, S.; Miura, H.; Shimizu, A.; Kokubo, M.; Niida, S.; et al. Postprandial Hyperglycemia is Associated with White Matter Hyperintensity and Brain Atrophy in Older Patients with Type 2 Diabetes Mellitus. Front. Aging Neurosci.. 2018, 10, 273. [Google Scholar] [CrossRef] [PubMed]
- Ogama, N.; Sakurai, T.; Shimizu, A.; Toba, K. Regional white matter lesions predict falls in patients with amnestic mild cognitive impairment and Alzheimer’s disease. J. Am. Med. Dir. Assoc. 2014, 15, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Ogama, N.; Sakurai, T.; Nakai, T.; Niida, S.; Saji, N.; Toba, K.; Umegaki, H.; Kuzuya, M. Impact of frontal white matter hyperintensity on instrumental activities of daily living in elderly women with Alzheimer disease and amnestic mild cognitive impairment. PLoS ONE 2017, 12, e0172484. [Google Scholar] [CrossRef] [PubMed]
- Hirabayashi, N.; Hata, J.; Ohara, T.; Mukai, N.; Nagata, M.; Shibata, M.; Gotoh, S.; Furuta, Y.; Yamashita, F.; Yoshihara, K.; et al. Association Between Diabetes and Hippocampal Atrophy in Elderly Japanese: The Hisayama Study. Diabetes Care 2016, 39, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.S.; Janssen, I.; Sui, X.; Church, T.S.; Blair, S.N. Longitudinal changes in body composition associated with healthy ageing: men, aged 20-96 years. Br. J. Nutr. 2012, 107, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Park, K.S.; Kim, M.J.; Kim, S.K.; Cho, Y.W.; Park, S.W. Type 2 diabetes is associated with low muscle mass in older adults. Geriatr. Gerontol. Int. 2014, 14, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Park, S.M. Association of muscle mass and fat mass with insulin resistance and the prevalence of metabolic syndrome in Korean adults: a cross-sectional study. Sci. Rep. 2018, 8, 2703. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.; de Courten, B.; Ebeling, P.R. Sarcopenia: a potential cause and consequence of type 2 diabetes in Australia’s ageing population? Med. J. Aust. 2016, 205, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Koch, G.; Belli, L.; Giudice, T.L.; Lorenzo, F.D.; Sancesario, G.M.; Sorge, R.; Bernardini, S.; Martorana, A. Frailty among Alzheimer’s disease patients. CNS Neurol. Disord. Drug Targets 2013, 12, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Robertson, D.A.; Savva, G.M.; Kenny, R.A. Frailty and cognitive impairment--a review of the evidence and causal mechanisms. Ageing Res. Rev. 2013, 12, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Wallace, L.; Theou, O.; Rockwood, K.; Andrew, M.K. Relationship between frailty and Alzheimer’s disease biomarkers: A scoping review. Alzheimers Dement. 2018, 10, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Walston, J.; Buta, B.; Xue, Q.L. Frailty Screening and Interventions: Considerations for Clinical Practice. Clin. Geriatr. Med. 2018, 34, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Langlois, F.; Vu, T.T.; Chassé, K.; Dupuis, G.; Kergoat, M.J.; Bherer, L. Benefits of physical exercise training on cognition and quality of life in frail older adults. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2013, 68, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Bucci, M.; Huovinen, V.; Guzzardi, M.A.; Koskinen, S.; Raiko, J.R.; Lipponen, H.; Ahsan, S.; Badeau, R.M.; Honka, M.J.; Koffert, J.; et al. Resistance training improves skeletal muscle insulin sensitivity in elderly offspring of overweight and obese mothers. Diabetologia 2016, 59, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, D.; Kim, C. Resistance Training for Glycemic Control, Muscular Strength, and Lean Body Mass in Old Type 2 Diabetic Patients: A Meta-Analysis. Diabetes Ther. 2017, 8, 459–473. [Google Scholar] [CrossRef] [PubMed]
- Kalyani, R.R.; Varadhan, R.; Weiss, C.O.; Fried, L.P.; Cappola, A.R. Frailty status and altered glucose-insulin dynamics. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 1300–1306. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Hampel, H.; Molinuevo, J.L.; Blennow, K.; DeKosky, S.T.; Gauthier, S.; Selkoe, D.; Bateman, R.; et al. Advancing research diagnostic criteria for Alzheimer’s disease: the IWG-2 criteria. Lancet Neurol. 2014, 13, 614–629. [Google Scholar] [CrossRef]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef] [PubMed]
- Bergenstal, R.M. Glycemic Variability and Diabetes Complications: Does It Matter? Simply Put, There Are Better Glycemic Markers! Diabetes Care 2015, 38, 1615–1621. [Google Scholar] [CrossRef] [PubMed]
- Donoghue, O.A.; Dooley, C.; Kenny, R.A. Usual and Dual-Task Walking Speed: Implications for Pedestrians Crossing the Road. J. Aging Health 2016, 28, 850–862. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 69) | Cognitive Impairment (n = 32) | Normal Cognition (n = 37) | p-Value † | ||||
|---|---|---|---|---|---|---|---|
| Mean (SD) or n (%) | Min–Max | Mean (SD) or n (%) | Min–Max | Mean (SD) or n (%) | Min–Max | ||
| Age, years | 75.0 (5.3) | 65–87 | 76.0 (5.8) | 65–87 | 74.2 (4.7) | 65–83 | 0.146 |
| Male, n (%) | 36 (52.2) | 15 (46.9) | 21 (56.8) | 0.413 | |||
| Body mass index, kg/m2 | 23.8 (2.7) | 17.8–31.0 | 23.6 (2.6) | 17.8–29.4 | 24.0 (2.7) | 19.9–31.0 | 0.597 |
| Mini-Mental State Examination | 24.4 (5.0) | 13–30 | 21.0 (5.2) | 13–29 | 27.4 (2.0) | 22–30 | <0.001 |
| Diabetes and comorbidities | |||||||
| Duration of diabetes, years | 15.3 (10.8) | 2–48 | 15.3 (10.6) | 2–40 | 15.4 (11.0) | 2–48 | 0.899 |
| Diabetic neuropathy, n (%) | 45 (65.2) | 22 (68.8) | 23 (62.2) | 0.567 | |||
| Diabetic retinopathy, n (%) | 16 (23.2) | 5 (15.6) | 11 (29.7) | 0.166 | |||
| Diabetic nephropathy, n (%) | 21 (30.4) | 12 (37.5) | 9 (24.3) | 0.236 | |||
| Coronary artery disease, n (%) | 15 (21.7) | 6 (18.8) | 9 (24.3) | 0.576 | |||
| Hypertension, n (%) | 53 (76.8) | 24 (75.0) | 29 (78.4) | 0.740 | |||
| Medications and antidiabetic agents, n (%) | |||||||
| Polypharmacy | 56 (81.2) | 29 (90.6) | 27 (73.0) | 0.061 | |||
| Biguanide | 20 (29.0) | 10 (31.3) | 10 (27.0) | 0.700 | |||
| Thiazolidine | 8 (11.6) | 6 (18.8) | 2 (5.4) | 0.132 | |||
| DPP4 inhibitor | 49 (71.0) | 23 (71.9) | 26 (70.3) | 0.884 | |||
| Sulfonylurea | 40 (58.0) | 19 (59.4) | 21 (56.8) | 0.826 | |||
| Insulin secretion promoter | 2 (2.9) | 2 (6.3) | 0 (0.0) | 0.211 | |||
| α-Glucosidase inhibitor | 16 (23.2) | 7 (21.9) | 9 (24.3) | 0.810 | |||
| Insulin | 13 (18.8) | 7 (21.9) | 6 (16.2) | 0.549 | |||
| GLP-1 receptor agonists | 2 (2.9) | 1 (3.1) | 1 (2.7) | 1.000 | |||
| Biochemical parameters | |||||||
| HbA1c, % | 7.1 (0.6) | 6.2–9.3 | 7.3 (0.7) | 6.2–9.3 | 7.0 (0.5) | 6.3–8.6 | 0.107 |
| Triglyceride, mg/dL | 139.8 (69.4) | 44–330 | 165.5 (72.1) | 65–330 | 117.6 (57.2) | 44–279 | 0.004 |
| Total cholesterol, mg/dL | 190.3 (41.1) | 108–316 | 192.0 (41.1) | 108–316 | 188.9 (41.6) | 137–309 | 0.524 |
| HDL cholesterol, mg/dL | 53.6 (13.7) | 27–92 | 50.8 (13.6) | 27–83 | 56.0 (13.5) | 37–92 | 0.112 |
| LDL cholesterol, mg/dL | 109.2 (36.0) | 46–238 | 109.5 (37.2) | 46–211 | 108.9 (35.4) | 67–238 | 0.928 |
| eGFR, mL/min/1.73 m2 | 63.7 (17.6) | 28.3–115.9 | 64.8 (16.9) | 28.3–110.3 | 62.7 (18.3) | 30.6–115.9 | 0.621 |
| Albumin, g/dL | 4.3 (0.4) | 3.5–5.2 | 4.2 (0.3) | 3.5–5.2 | 4.4 (0.3) | 3.8–5.2 | 0.014 |
| UACR, mg/gCr | 156.7 (339.4) | 1.5–1808.3 | 167.1 (349.2) | 1.5–1705.4 | 147.8 (335.3) | 2.7–1808.3 | 0.516 |
| Daily blood glucose level | |||||||
| 05:00 h, mg/dL | 116.6 (22.2) | 57–254 | 113.5 (19.6) | 57–205 | 119.4 (24.2) | 58–254 | 0.485 |
| Before breakfast, mg/dL | 123.0 (21.7) | 51–215 | 119.5 (20.4) | 63–201 | 126.0 (22.6) | 51–215 | 0.216 |
| 2 h after breakfast, mg/dL | 180.7 (34.3) | 68–383 | 184.7 (38.8) | 68–349 | 177.3 (29.9) | 72–383 | 0.880 |
| Before lunch, mg/dL | 126.7 (33.6) | 43–313 | 137.3 (38.5) | 43–313 | 117.6 (25.9) | 45–243 | 0.011 |
| Before dinner, mg/dL | 134.9 (27.5) | 55–331 | 139.2 (33.0) | 60–331 | 131.2 (21.3) | 55–267 | 0.339 |
| Fluctuation, mg/dL | 91.4 (28.5) | 32–155 | 97.0 (29.7) | 49–155 | 86.5 (26.8) | 32–137 | 0.127 |
| Frequency of hypoglycemia* | 0.71 (1.3) | 0–7 | 0.72 (1.5) | 0–7 | 0.70 (1.2) | 0–4 | 0.719 |
| Mobility function | |||||||
| Sarcopenia, n (%) | 8 (11.6) | 7 (21.9) | 1 (2.7) | 0.021 | |||
| Low muscle mass, n (%) | 10 (14.5) | 9 (28.1) | 1 (2.7) | 0.004 | |||
| Low grip strength, n (%) | 24 (34.8) | 17 (53.1) | 7 (18.9) | 0.003 | |||
| Slow walking speed, n (%) | 4 (5.8) | 4 (12.5) | 0 (0.0) | 0.042 | |||
| Glucose Fluctuations | ||||
|---|---|---|---|---|
| Differences * | OR | 95% CI | p-Value | |
| No sarcopenia | Reference | |||
| Sarcopenia | 29.3 mg/dL | 1.045 | (1.007; 1.083) | 0.018 |
| Normal muscle mass | Reference | |||
| Low muscle mass | 22.7 mg/dL | 1.031 | (1.000; 1.064) | 0.0499 |
| Normal grip strength | Reference | |||
| Low grip strength | 20.0 mg/dL | 1.029 | (1.006; 1.053) | 0.014 |
| Normal walking speed | Reference | |||
| Slow walking speed | 48.0 mg/dL | 1.092 | (1.018; 1.172) | 0.014 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogama, N.; Sakurai, T.; Kawashima, S.; Tanikawa, T.; Tokuda, H.; Satake, S.; Miura, H.; Shimizu, A.; Kokubo, M.; Niida, S.; et al. Association of Glucose Fluctuations with Sarcopenia in Older Adults with Type 2 Diabetes Mellitus. J. Clin. Med. 2019, 8, 319. https://doi.org/10.3390/jcm8030319
Ogama N, Sakurai T, Kawashima S, Tanikawa T, Tokuda H, Satake S, Miura H, Shimizu A, Kokubo M, Niida S, et al. Association of Glucose Fluctuations with Sarcopenia in Older Adults with Type 2 Diabetes Mellitus. Journal of Clinical Medicine. 2019; 8(3):319. https://doi.org/10.3390/jcm8030319
Chicago/Turabian StyleOgama, Noriko, Takashi Sakurai, Shuji Kawashima, Takahisa Tanikawa, Haruhiko Tokuda, Shosuke Satake, Hisayuki Miura, Atsuya Shimizu, Manabu Kokubo, Shumpei Niida, and et al. 2019. "Association of Glucose Fluctuations with Sarcopenia in Older Adults with Type 2 Diabetes Mellitus" Journal of Clinical Medicine 8, no. 3: 319. https://doi.org/10.3390/jcm8030319
APA StyleOgama, N., Sakurai, T., Kawashima, S., Tanikawa, T., Tokuda, H., Satake, S., Miura, H., Shimizu, A., Kokubo, M., Niida, S., Toba, K., Umegaki, H., & Kuzuya, M. (2019). Association of Glucose Fluctuations with Sarcopenia in Older Adults with Type 2 Diabetes Mellitus. Journal of Clinical Medicine, 8(3), 319. https://doi.org/10.3390/jcm8030319