Impact of Simultaneous Consideration of Cardiac and Vascular Function on Long-Term All-Cause and Cardiovascular Mortality

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethics Statement
2.3. Echocardiographic Evaluation
2.4. Measurement of baPWV
2.5. Collection of Medical and Demographic Data
2.6. Definition of all-cause and CV mortality
2.7. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. J. Am. Coll. Cardiol. 2013, 128, 1810–1852. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Ferranti, S., de; Despres, J.P.; Fullerton, H.J.; Howard, V.J.; et al. Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, 434–441. [Google Scholar] [CrossRef]
- Levy, W.C.; Mozaffarian, D.; Linker, D.T.; Sutradhar, S.C.; Anker, S.D.; Cropp, A.B.; Anand, I.; Maggioni, A.; Burton, P.; Sullivan, M.D.; et al. The Seattle Heart Failure Model: Prediction of survival in heart failure. Circulation 2006, 113, 1424–1433. [Google Scholar] [CrossRef] [PubMed]
- Pocock, S.J.; Ariti, C.A.; McMurray, J.J.; Maggioni, A.; Kober, L.; Squire, I.B.; Swedberg, K.; Dobson, J.; Poppe, K.K.; Whalley, G.A.; et al. Predicting survival in heart failure: A risk score based on 39,372 patients from 30 studies. Eur. Heart J. 2013, 34, 1404–1413. [Google Scholar] [CrossRef] [PubMed]
- Ouwerkerk, W.; Voors, A.A.; Zwinderman, A.H. Factors influencing the predictive power of models for predicting mortality and/or heart failure hospitalization in patients with heart failure. JACC Heart Fail. 2014, 2, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, K.; Bennett, D.; Conrad, N.; Williams, T.M.; Basu, J.; Dwight, J.; Woodward, M.; Patel, A.; McMurray, J.; MacMahon, S. Risk prediction in patients with heart failure: A systematic review and analysis. JACC Heart Fail. 2014, 2, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Breathett, K.; Allen, L.A.; Udelson, J.; Davis, G.; Bristow, M. Changes in left ventricular ejection fraction predict survival and hospitalization in heart failure with reduced ejection fraction. Circ. Heart Fail. 2016, 9, e002962. [Google Scholar] [CrossRef]
- Solomon, S.D.; Anavekar, N.; Skali, H.; McMurray, J.J.; Swedberg, K.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Wang, D.; Pocock, S.; et al. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation 2005, 112, 3738–3744. [Google Scholar] [CrossRef]
- St John Sutton, M.; Pfeffer, M.A.; Moye, L.; Plappert, T.; Rouleau, J.L.; Lamas, G.; Rouleau, J.; Parker, J.O.; Arnold, M.O.; Sussex, B.; et al. Cardiovascular death and left ventricular remodeling two years after myocardial infarction: Baseline predictors and impact of long-term use of captopril: Information from the Survival and Ventricular Enlargement (SAVE) trial. Circulation 1997, 96, 3294–3299. [Google Scholar] [CrossRef]
- McDermott, M.M.; Feinglass, J.; Lee, P.I.; Mehta, S.; Schmitt, B.; Lefevre, F.; Gheorghiade, M. Systolic function, readmission rates, and survival among consecutively hospitalized patients with congestive heart failure. Am. Heart J. 1997, 134, 728–736. [Google Scholar] [CrossRef]
- Mosterd, A.; Cost, B.; Hoes, A.W.; de Bruijne, M.C.; Deckers, J.W.; Hofman, A.; Grobbee, D.E. The prognosis of heart failure in the general population: The Rotterdam Study. Eur. Heart J. 2001, 22, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Imanishi, R.; Seto, S.; Toda, G.; Yoshida, M.; Ohtsuru, A.; Koide, Y.; Baba, T.; Yano, K. High brachial-ankle pulse wave velocity is an independent predictor of the presence of coronary artery disease in men. Hypertens. Res. 2004, 27, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Mattace-Raso, F.U.; van der Cammen, T.J.; Hofman, A.; van Popele, N.M.; Bos, M.L.; Schalekamp, M.A.; Asmar, R.; Reneman, R.S.; Hoeks, A.P.; Breteler, M.M.; et al. Arterial stiffness and risk of coronary heart disease and stroke: The Rotterdam Study. Circulation 2006, 113, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Willum-Hansen, T.; Staessen, J.A.; Torp-Pedersen, C.; Rasmussen, S.; Thijs, L.; Ibsen, H.; Jeppesen, J. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation 2006, 113, 664–670. [Google Scholar] [CrossRef]
- Asmar, R.; Benetos, A.; Topouchian, J.; Laurent, P.; Pannier, B.; Brisac, A.M.; Target, R.; Levy, B.I. Assessment of arterial distensibility by automatic pulse wave velocity measurement. Validation and clinical application studies. Hypertension 1995, 26, 485–490. [Google Scholar] [CrossRef]
- Miyano, I.; Nishinaga, M.; Takata, J.; Shimizu, Y.; Okumiya, K.; Matsubayashi, K.; Ozawa, T.; Sugiura, T.; Yasuda, N.; Doi, Y. Association between brachial-ankle pulse wave velocity and 3-year mortality in community-dwelling older adults. Hypertens. Res. 2010, 33, 678–682. [Google Scholar] [CrossRef]
- Chen, Y.; Shen, F.; Liu, J.; Yang, G.Y. Arterial stiffness and stroke: De-stiffening strategy, a therapeutic target for stroke. Stroke Vasc. Neurol. 2017, 2, 65–72. [Google Scholar] [CrossRef]
- Hsu, P.C.; Lin, T.H.; Lee, C.S.; Chu, C.Y.; Su, H.M.; Voon, W.C.; Lai, W.T.; Sheu, S.H. Impact of a systolic parameter, defined as the ratio of right brachial pre-ejection period to ejection time, on the relationship between brachial-ankle pulse wave velocity and left ventricular diastolic function. Hypertens. Res. 2011, 34, 462–467. [Google Scholar] [CrossRef][Green Version]
- Tomiyama, H.; Yamashina, A.; Arai, T.; Hirose, K.; Koji, Y.; Chikamori, T.; Hori, S.; Yamamoto, Y.; Doba, N.; Hinohara, S. Influences of age and gender on results of noninvasive brachial-ankle pulse wave velocity measurement--a survey of 12517 subjects. Atherosclerosis 2003, 166, 303–309. [Google Scholar] [CrossRef]
- Yokoyama, H.; Shoji, T.; Kimoto, E.; Shinohara, K.; Tanaka, S.; Koyama, H.; Emoto, M.; Nishizawa, Y. Pulse wave velocity in lower-limb arteries among diabetic patients with peripheral arterial disease. J. Atheroscler. Thromb. 2003, 10, 253–258. [Google Scholar] [CrossRef]
- Lee, D.S.; Gona, P.; Albano, I.; Larson, M.G.; Benjamin, E.J.; Levy, D.; Kannel, W.B.; Vasan, R.S. A systematic assessment of causes of death after heart failure onset in the community: Impact of age at death, time period, and left ventricular systolic dysfunction. Circ. Heart Fail. 2011, 4, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.L.; Masoudi, F.A.; Vaccarino, V.; Radford, M.J.; Krumholz, H.M. Outcomes in heart failure patients with preserved ejection fraction: Mortality, readmission, and functional decline. J. Am. Coll. Cardiol. 2003, 41, 1510–1518. [Google Scholar] [CrossRef]
- Cohn, J.N.; Johnson, G. Heart failure with normal ejection fraction. The V-HeFT Study. Veterans Administration Cooperative Study Group. Circulation 1990, 81, III48–III53. [Google Scholar] [PubMed]
- Sugahara, M.; Kagiyama, N.; Hasselberg, N.E.; Blauwet, L.A.; Briller, J.; Cooper, L.; Fett, J.D.; Hsich, E.; Wells, G.; McNamara, D.; et al. IPAC Investigators. Global Left Ventricular Strain at Presentation Is Associated with Subsequent Recovery in Patients with Peripartum Cardiomyopathy. J. Am. Soc. Echocardiogr. 2019, 32, 1565–1573. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Lu, H.; Li, L. Reduced Left Ventricular Ejection Fraction Is a Risk Factor for In-Hospital Mortality in Patients after Percutaneous Coronary Intervention: A Hospital-Based Survey. Biomed Res. Int. 2018, 2018. [Google Scholar] [CrossRef]
- Tanaka, H.; Munakata, M.; Kawano, Y.; Ohishi, M.; Shoji, T.; Sugawara, J.; Tomiyama, H.; Yamashina, A.; Yasuda, H.; Sawayama, T.; et al. Comparison between carotid-femoral and brachial-ankle pulse wave velocity as measures of arterial stiffness. J. Hypertens. 2009, 27, 2022–2027. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
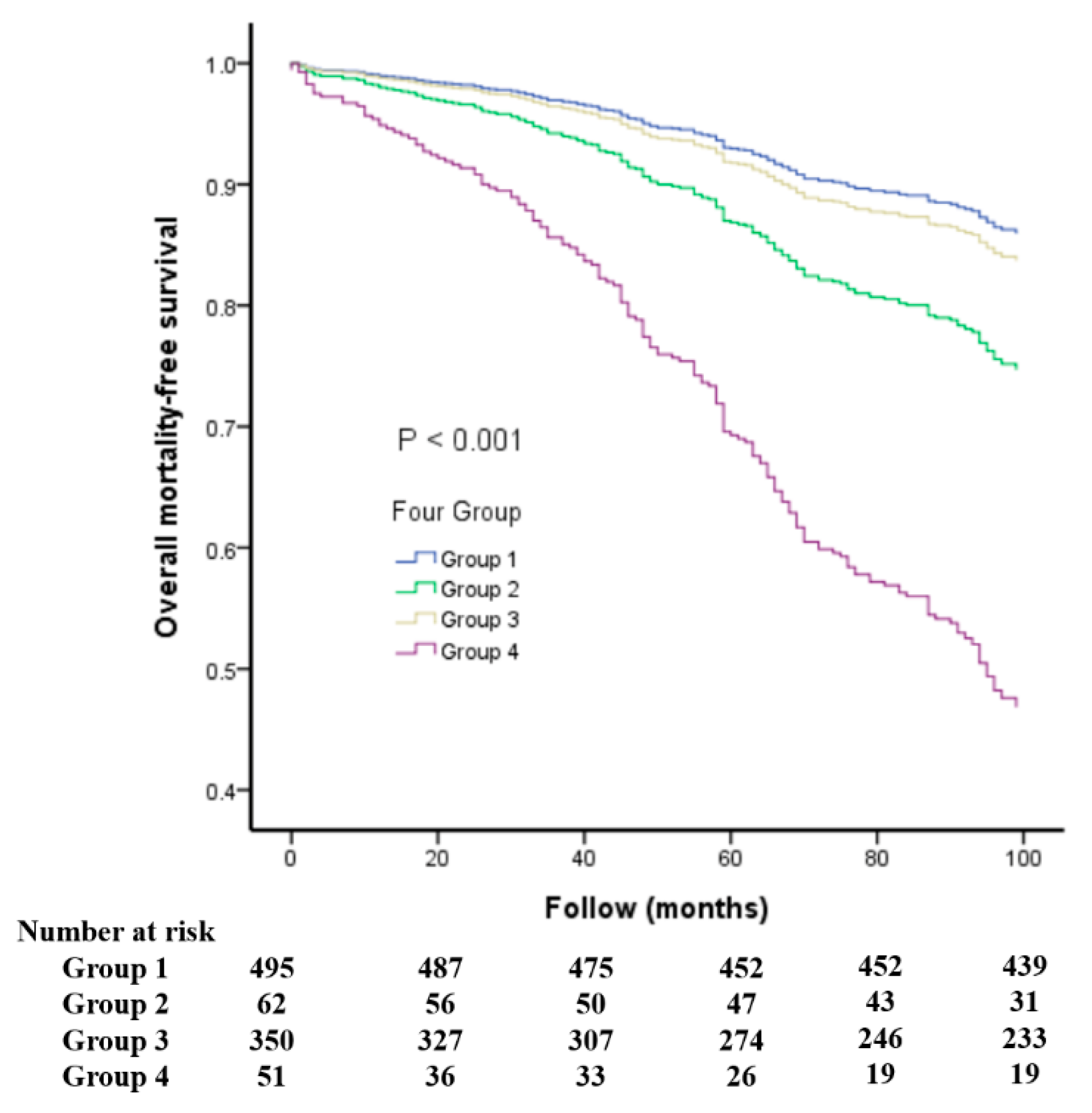
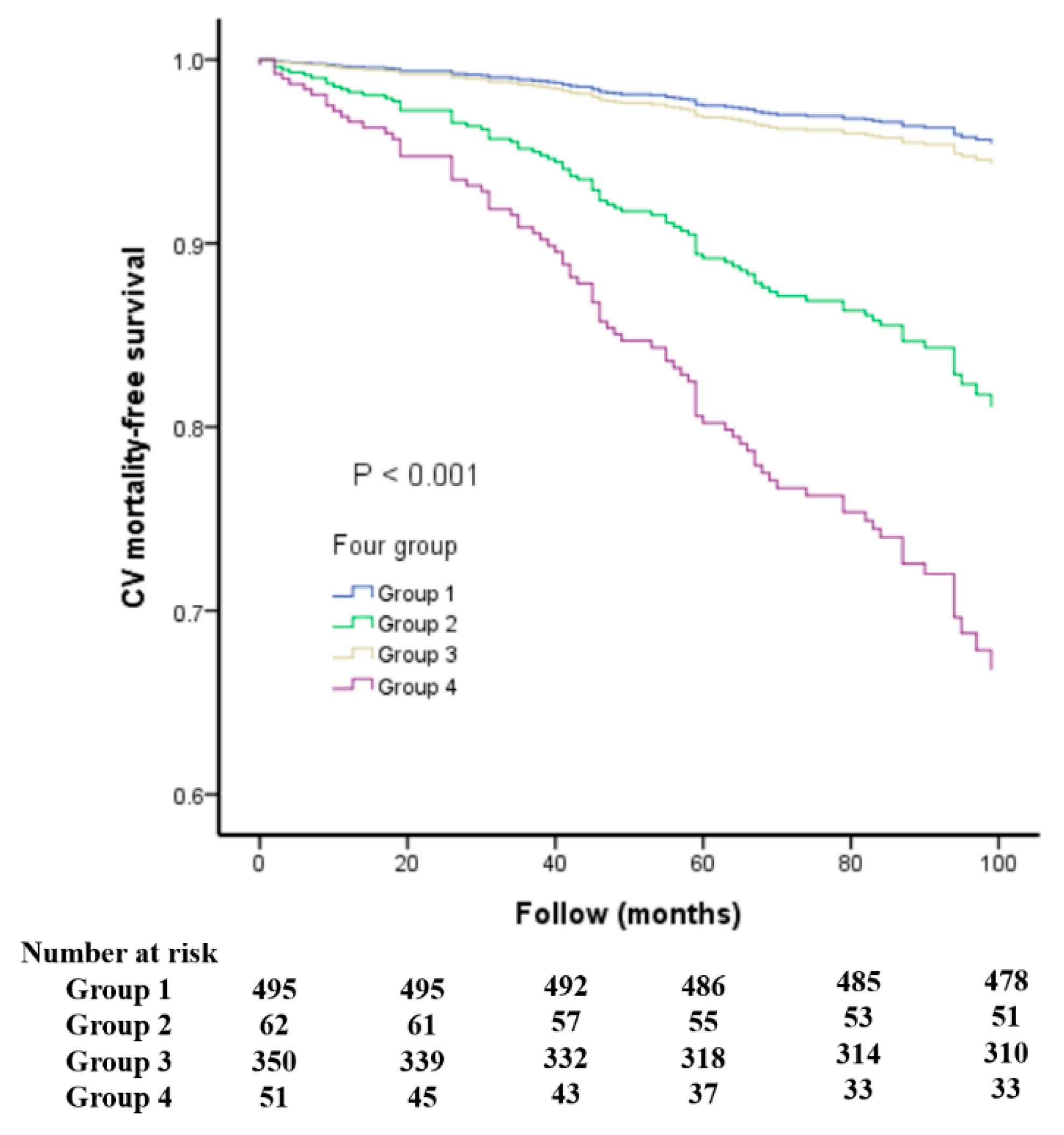
| Group1 (LVEF ≥ 50%, baPWV below the Median) | Group2 (LVEF < 50%, baPWV below the Median) | Group 3 (LVEF ≥ 50%, baPWV above the Median) | Group 4 (LVEF < 50%, baPWV above the Median) | p Value (ANOVA among Groups) | All Patients | |
|---|---|---|---|---|---|---|
| Number | 495 | 62 | 350 | 51 | 958 | |
| Age (years) | 56 ± 13 | 58 ± 16 | 70 ± 11 *,$ | 71 ± 12 *,$ | <0.001 | 62 ± 14 |
| Male Gender (%) | 59.0 | 75.4 * | 47.6 *,$ | 60.8 | <0.001 | 55.8 |
| DM (%) | 21.6 | 35.5 * | 37.7 * | 31.4 | <0.001 | 28.9 |
| CVD (%) | 20.8 | 54.8 * | 26.0 $ | 51.0 *,# | <0.001 | 26.5 |
| Mean blood pressure | 92 ± 12 | 87 ± 12 * | 103 ± 13 *,$ | 100 ± 15 *,$ | <0.001 | 96 ± 14 |
| Total cholesterol | 192 ± 39 | 176 ± 50 | 191 ± 40 | 183 ± 46 | 0.07 | 190 ± 41 |
| BMI (kg/m2) | 26.8 ± 4.0 | 26.5 ± 4.7 | 25.9 ± 3.8 * | 24.4 ± 3.5 *,$ | <0.001 | 26.3 ± 4.0 |
| Heart rate (beats/min) | 67 ± 10 | 75 ± 17 * | 70 ± 12 *,$ | 79 ± 17 *,# | <0.001 | 69 ± 12 |
| LVEF (%) | 67 ± 8 | 38 ± 9 * | 67 ± 8 $ | 38 ± 8 *,# | <0.001 | 64 ± 12 |
| baPWV (cm/s) | 1475 ± 173 | 1456 ± 178 | 2163 ± 387 *,$ | 2278 ± 668 *,$ | <0.001 | 1768 ± 466 |
| Numbers of Mortality | ||||||
| All-cause | 58 | 23 | 120 | 37 | <0.001 | 238 |
| Cardiovascular | 17 | 13 | 41 | 20 | <0.001 | 91 |
| Medications | ||||||
| Aspirin (%) | 30.2 | 47.5 * | 33.9 $ | 41.2 | 0.026 | 33.1 |
| β-blockers (%) | 40.7 | 67.2 * | 38.1 $ | 35.3 $ | <0.001 | 41.0 |
| CCBs (%) | 38.2 | 19.7 * | 46.4 *,$ | 25.5 # | <0.001 | 39.2 |
| ACEIs (%) | 5.9 | 21.3 * | 9.5 $ | 11.8 | <0.001 | 8.5 |
| ARBs (%) | 47.3 | 50.8 | 50.7 | 45.1 | 0.72 | 48.5 |
| Diuretics (%) | 24.9 | 59.0 * | 31.9 *,$ | 47.1 *,# | <0.001 | 30.7 |
| Parameter | Univariate | Multivariate (Forward) | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Age (+ 13.74 year) | 2.949 (2.494–3.486) | <0.001 | 3.159 (2.524–3.952) | <0.001 |
| Male gender (male vs. female) | 1.109 (0.852–1.444) | 0.44 | 1.573 (1.152–2.150) | 0.004 |
| Diabetes mellitus (yes vs. no) | 2.275 (1.750–2.957) | <0.001 | 2.411 (1.773–3.278) | <0.001 |
| Mean blood pressure (+13.80 mmHg) | 1.120 (0.983–1.276) | 0.09 | 1.300 (1.101–1.534) | 0.002 |
| Total cholesterol (−40.68 mg/dL) | 0.741 (0.631–0.872) | <0.001 | – | – |
| Heart rate (+12.20 beat/minute) | 1.242 (1.096–1.407) | 0.001 | – | – |
| Smoking (ever vs. no) | 0.775 (0.518–1.158) | 0.21 | ||
| Medications | ||||
| Aspirin use | 1.252 (0.954–1.642) | 0.11 | ||
| Beta blocker use | 1.037 (0.796–1.351) | 0.79 | ||
| Calcium channel blocker use | 1.127 (0.865–1.468) | 0.38 | ||
| ACEI use | 1.142 (0.736–1.773) | 0.55 | ||
| ARB use | 1.044 (0.804–1.354) | 0.75 | ||
| Diuretic use | 1.886 (1.449–2.454) | <0.001 | – | – |
| Study Group | <0.001 | <0.001 | ||
| Group 2 vs. Group 1 | 3.810 (2.307–6.292) | <0.001 | 1.954 (1.049–3.638) | 0.035 |
| Group 3 vs. Group 1 | 3.459 (2.516–4.756) | <0.001 | 1.150 (0.764–1.730) | 0.50 |
| Group 4 vs. Group 1 | 10.854 (7.014–16.797) | <0.001 | 4.693 (2.745–8.022) | <0.001 |
| Parameter | Univariate | Multivariate (Forward) | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Age (+13.74 year) | 3.035 (2.305–3.997) | <0.001 | 2.860 (2.103–3.889) | <0.001 |
| Male gender (male vs female) | 0.991 (0.647–1.516) | 0.97 | – | – |
| Diabetes mellitus (yes vs. no) | 2.727 (1.789–4.157) | <0.001 | 2.746 (1.772–4.256) | <0.001 |
| Mean blood pressure (+13.80 mmHg) | 1.208 (0.982–1.487) | 0.074 | 1.371 (1.086–1.731) | 0.008 |
| Total cholesterol (−40.68 mg/dL) | 0.774 (0.592–1.012) | 0.061 | ||
| Heart rate (+12.20 beat/minute) | 1.309 (1.073–1.598) | 0.008 | – | – |
| Smoking (ever vs. no) | 0.749 (0.388–1.448) | 0.39 | ||
| Medications | ||||
| Aspirin use | 1.318(0.852–2.039) | 0.22 | ||
| Beta blocker use | 1.271(0.834–1.938) | 0.26 | ||
| Calcium channel blocker use | 1.180(0.772–1.806) | 0.45 | ||
| ACEI use ARB use | 1.235(0.619–2.463) 1.283(0.841–1.956) | 0.55 0.25 | – | – |
| Diuretic use | 1.909(1.248–2.922) | 0.003 | – | – |
| Study Group | <0.001 | <0.001 | ||
| Group 2 vs. Group 1 | 6.612 (3.096–14.120) | <0.001 | 4.518 (2.050–9.955) | <0.001 |
| Group 3 vs. Group 1 | 3.881 (2.199–6.849) | <0.001 | 1.256 (0.661–2.387) | 0.49 |
| Group 4 vs. Group 1 | 20.443 (10.494–39.823) | <0.001 | 8.702 (4.283–17.679) | <0.001 |
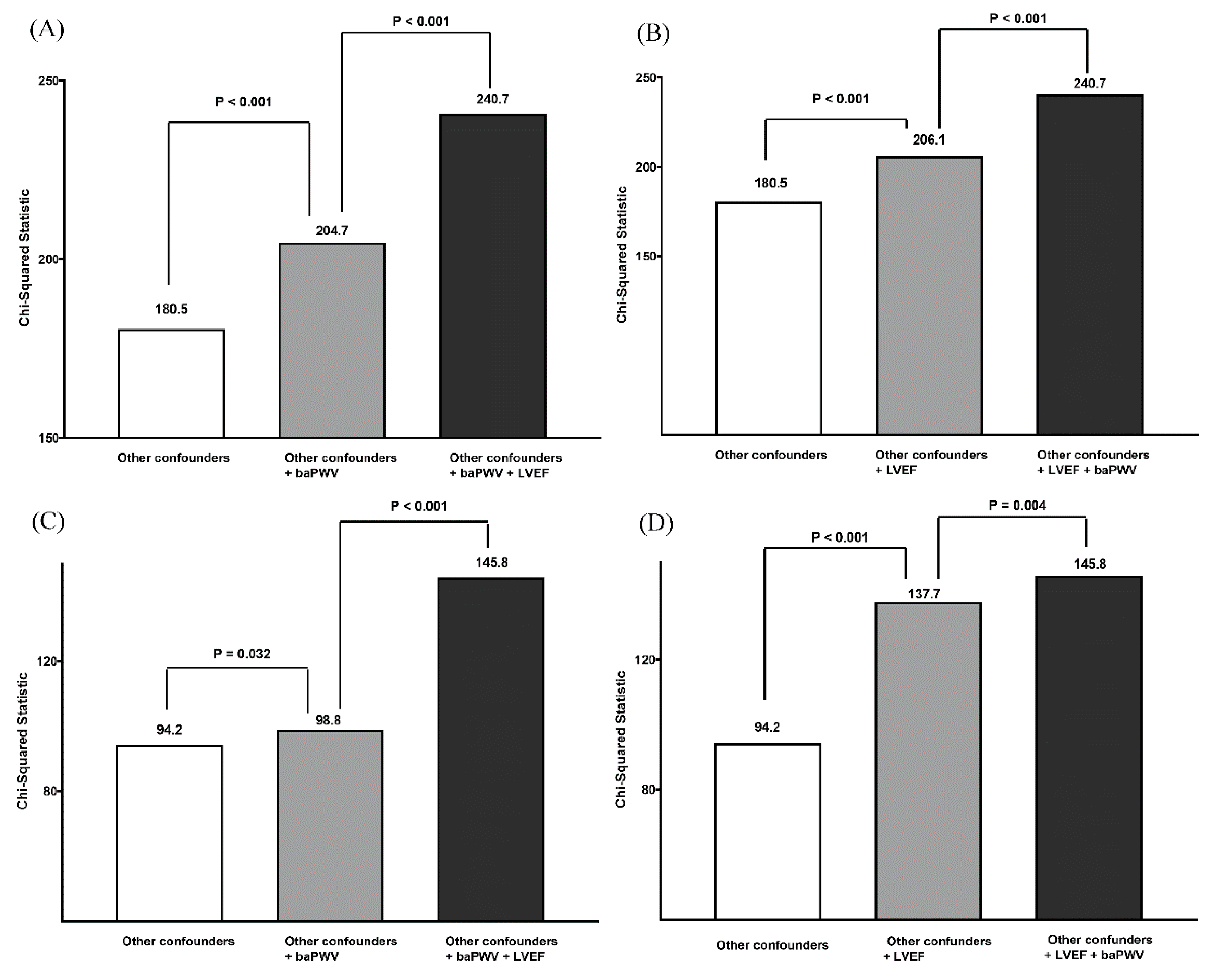
| Model | Variable | All-Cause Mortality Prediction | CV Mortality Prediction | ||
|---|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | ||
| Model 1: LVEF | LVEF | 0.648 (0.579–0.725) | <0.001 | 0.548 (0.464–0.648) | <0.001 |
| Model 2: LVEF + other confounders | LVEF | 0.655 (0.565–0.758) | <0.001 | 0.510 (0.423–0.614) | <0.001 |
| Model 3: baPWV | baPWV | 1.886 (1.713–2.076) | <0.001 | 1.831 (1.556–2.154) | <0.001 |
| Model 4: baPWV + other confounders | baPWV | 1.573 (1.356–1.825) | <0.001 | 1.272 (1.029–1.571) | 0.026 |
| Model 5: Other confounders + LVEF + baPWV | baPWV LVEF | 1.640(1.416–1.899) 0.628(0.541–0.729) | <0.001 <0.001 | 1.462 (1.205–1.774) 0.507 (0.422–0.609) | <0.001 <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, P.-C.; Lee, W.-H.; Tsai, W.-C.; Chu, C.-Y.; Chen, Y.-C.; Lee, M.-K.; Lin, T.-H.; Lee, C.-S.; Voon, W.-C.; Lai, W.-T.; et al. Impact of Simultaneous Consideration of Cardiac and Vascular Function on Long-Term All-Cause and Cardiovascular Mortality. J. Clin. Med. 2019, 8, 2145. https://doi.org/10.3390/jcm8122145
Hsu P-C, Lee W-H, Tsai W-C, Chu C-Y, Chen Y-C, Lee M-K, Lin T-H, Lee C-S, Voon W-C, Lai W-T, et al. Impact of Simultaneous Consideration of Cardiac and Vascular Function on Long-Term All-Cause and Cardiovascular Mortality. Journal of Clinical Medicine. 2019; 8(12):2145. https://doi.org/10.3390/jcm8122145
Chicago/Turabian StyleHsu, Po-Chao, Wen-Hsien Lee, Wei-Chung Tsai, Chun-Yuan Chu, Ying-Chih Chen, Meng-Kuang Lee, Tsung-Hsien Lin, Chee-Siong Lee, Wen-Chol Voon, Wen-Ter Lai, and et al. 2019. "Impact of Simultaneous Consideration of Cardiac and Vascular Function on Long-Term All-Cause and Cardiovascular Mortality" Journal of Clinical Medicine 8, no. 12: 2145. https://doi.org/10.3390/jcm8122145
APA StyleHsu, P.-C., Lee, W.-H., Tsai, W.-C., Chu, C.-Y., Chen, Y.-C., Lee, M.-K., Lin, T.-H., Lee, C.-S., Voon, W.-C., Lai, W.-T., Sheu, S.-H., & Su, H.-M. (2019). Impact of Simultaneous Consideration of Cardiac and Vascular Function on Long-Term All-Cause and Cardiovascular Mortality. Journal of Clinical Medicine, 8(12), 2145. https://doi.org/10.3390/jcm8122145