A Systematic Review of Survival Rates of Osseointegrated Implants in Fully and Partially Edentulous Patients Following Immediate Loading

 ,
, 
 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Statement of Question (PICOS)
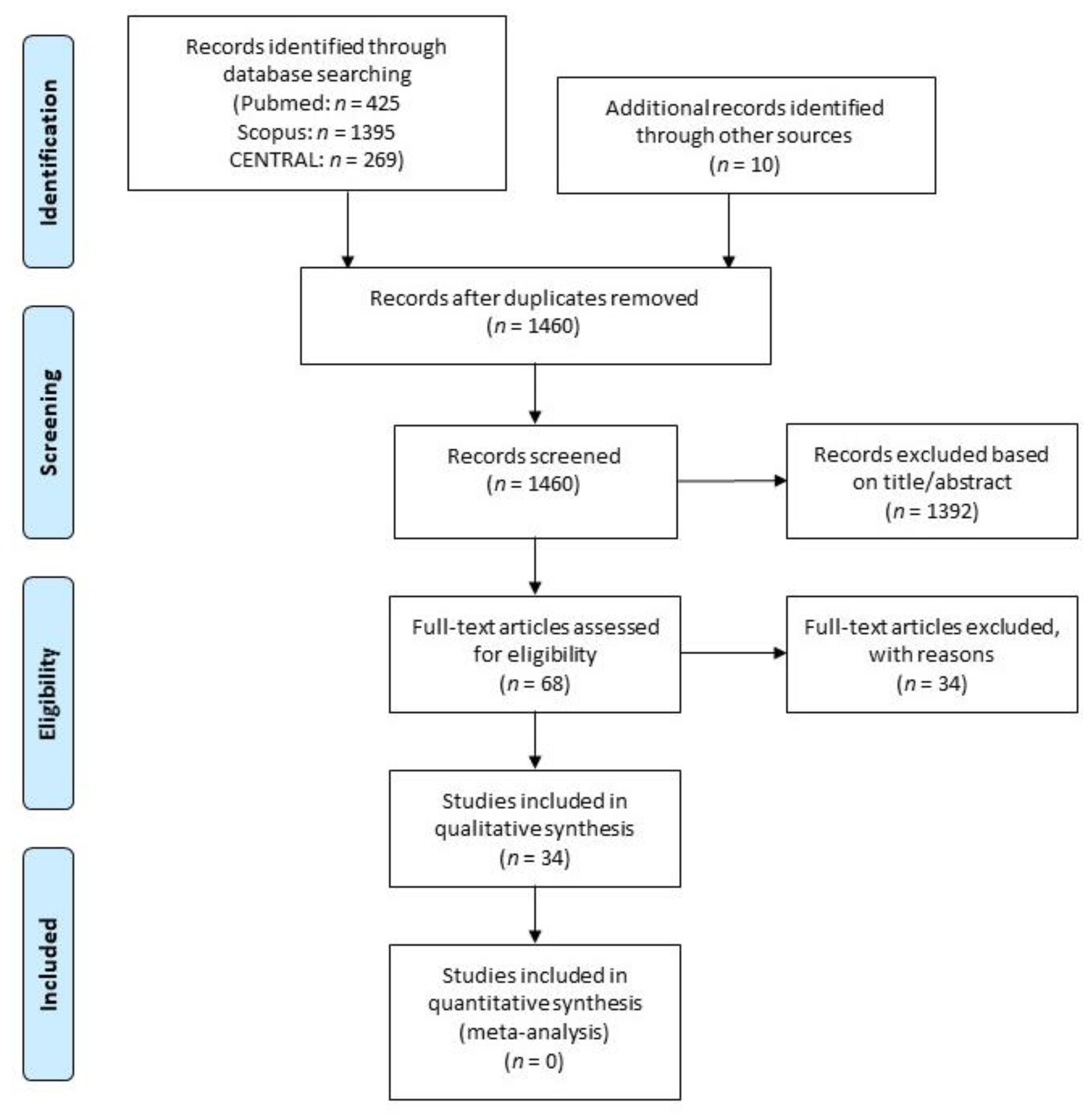
2.2. Search Strategy
2.3. Inclusion Criteria
- Human studies.
- Publication in English language.
- Prospective studies (randomized clinical trials (RCT), controlled clinical trials (CCT) or prospective case series (PCS)).
- Functional fixed prosthesis delivered within 72 h after postimplant placement.
- At least five years follow-up after prosthesis delivery.
- At least 10 patients treated with immediately loaded implants.
- Patients older than 18 years.
- Data regarding success and/or survival of immediately loaded implants, as well as complications, had to be reported.
- No restriction was placed regarding the publication year.
- Case reports, retrospective studies, and reviews of the literature, as well as animal and in vitro studies, were excluded.
- When papers from the same group of authors were identified, with very similar databases of patients, materials, methods, and outcomes, the authors were contacted to clarify whether the pool of patients was indeed the same. In the case of multiple publications relative to different aspects or phases of the same study, only the one reporting results with the longest follow-up was considered.
2.4. Selection Criteria and Data Extraction
2.5. Methodological Quality Assessment
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Albrektsson, T.; Brånemark, P.-I.; Hansson, H.-A.; Lindström, J. Osseointegrated Titanium Implants: Requirements for Ensuring a Long-Lasting, Direct Bone-to-Implant Anchorage in Man. Acta Orthopaed. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Testori, T.; Del Fabbro, M.; Bianchi, F.; Francetti, L.; Weinstein, R.L.; Feldman, S.; Vincenzi, G.; Sullivan, D.; Rossi, R., Jr.; Anitua, E. A multicenter prospective evaluation of 2-months loaded OsseotiteR implants placed in the posterior jaws: 3-year follow-up results. Clin. Oral Implant. Res. 2002, 13, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Chiapasco, M.; Gatti, C.; Rossi, E.; Haeflige, W.; Markwaldel, T.H. Implant-retained mandibular overdentures with immediate loading. Clin. Oral Implant. Res. 1997, 8, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Testori, T.; Francetti, L.; Taschieri, S.; Weinstein, R. Systematic Review of Survival Rates for Immediately Loaded Dental Implants. Int. J. Periodontics Restor. Dent. 2006, 26, 249–263. [Google Scholar]
- Brånemark, P. Osseointegrated implants in the treatment of edentulous jaw, Experience from a 10-year period. Scand. J. Plast. Reconstr. Surg. 1977, 1, 1–132. [Google Scholar]
- Sarmiento, A.; Schaeffer, J. Fracture healing in rat femora as affected by functional weight-bearing. J. Bone Jt. Surg. Am. 1977, 59, 369–375. [Google Scholar] [CrossRef]
- Hulbert, S.F.; Matthews, J.R.; Klawitter, J.J.; Sauer, B.W.; Leonard, R.B. Effect of stress on tissue ingrowth into porous aluminum oxide. J. Biomed. Mat. Res. 1974, 8, 85–97. [Google Scholar] [CrossRef]
- Rubin, C.; McLeod, K. Promotion of bony ingrowth by frequency-specific, low-amplitude mechanical strain. Clin. Orthop. Relat. Res. 1994, 298, 165–174. [Google Scholar] [CrossRef]
- Albrektsson, T.; Buser, D.; Chen, S.T.; Cochran, D.; DeBruyn, H.; Jemt, T.; Koka, S.; Nevins, M.; Sennerby, L.; Simion, M.; et al. Statements from the Estepona Consensus Meeting on Peri-implantitis. Clin. Implant Dent. Relat. Res. 2012, 14, 781–782. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Immediate nonfunctional versus immediate functional loading and dental implant failure rates: A systematic review and meta-analysis. J. Dent. 2014, 42, 1052–1059. [Google Scholar] [CrossRef]
- Testori, T.; Bianchi, F.; Del Fabbro, M.; Francetti, L.; Weinstein, R.L. Immediate non-occlusal loading vs. early loading in partially edentulous patients. Pract. Proced. Esthet. Dent. 2003, 15, 787–794. [Google Scholar]
- Testori, T.; Galli, F.; Del Fabbro, M. Immediate Loading: A New Era in Oral Implantology; Testori, T., Galli, F., Del Fabbro, M., Eds.; Quintessence Publishing Co. Ltd.: Berlin, Germany, 2011. [Google Scholar]
- Degidi, M.; Piattelli, A. Immediate Functional and Non-Functional Loading of Dental Implants: A 2- to 60-Month Follow-Up Study of 646 Titanium Implants. J. Periodontol. 2003, 74, 225–241. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Nardi, D.; Piattelli, A. A comparison between immediate loading and immediate restoration in cases of partial posterior mandibular edentulism: A 3-year randomized clinical trial. Clin. Oral Implant. Res. 2010, 21, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Wood, D.L.; Hoag, P.M.; Donnenfeld, O.W.; Rosenfeld, L.D. Alveolar Crest Reduction Following Full and Partial Thickness Flaps. J. Periodontol. 1972, 43, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzla, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Jaffin, R.; Kolesar, M.; Kumar, A.; Ishikawa, S.; Fiorellini, J. The radiographic bone loss pattern adjacent to immediately placed, immediately loaded implants. Int. J. Oral Maxillofac. Implant. 2007, 22, 187–194. [Google Scholar] [CrossRef]
- Calandriello, R.; Tomatis, M. Immediate Occlusal Loading of Single Lower Molars Using Brånemark System® Wide Platform TiUnite™ Implants: A 5-Year Follow-Up Report of a Prospective Clinical Multicenter Study. Clin. Implant Dent. Relat. Res. 2011, 13, 311–318. [Google Scholar] [CrossRef]
- Degidi, M.; Iezzi, G.; Perrotti, V.; Piattelli, A. Comparative Analysis of Immediate Functional Loading and Immediate Nonfunctional Loading to Traditional Healing Periods: A 5-Year Follow-Up of 550 Dental Implants. Clin. Implant Dent. Relat. Res. 2009, 11, 257–266. [Google Scholar] [CrossRef]
- Payer, M.; Heschl, A.; Wimmer, G.; Wegscheider, W.; Kirmeier, R.; Lorenzoni, M. Immediate provisional restoration of screw-type implants in the posterior mandible: Results after 5 years of clinical function. Clin. Oral Implant. Res. 2010, 21, 815–821. [Google Scholar] [CrossRef]
- Capelli, M.; Esposito, M.; Zuffetti, F.; Galli, F.; Del Fabbro, M.; Testori, T. A 5-year report from a multicentre randomised clinical trial: Immediate non-occlusal versus early loading of dental implants in partially edentulous patients. Eur. J. Oral Implantol. 2010, 3, 209–219. [Google Scholar]
- Prosper, L.; Crespi, R.; Valenti, E.; Capparé, P.; Gherlone, E. 3 Five-Year Follow-up of Wide-Diameter Implants Placed in Fresh Molar Extraction Sockets in the Mandible: Immediate Versus Delayed Loading. Int. J. Oral Maxillofac. Implant. 2010, 25, 607–612. [Google Scholar]
- Malchiodi, L.; Giovanni Corrocher, G.; Cucchi, A.; Ghensi, P.; Bissolotti, G.; Nocini, P.F. Long-Term Results of Immediately Loaded Fast bone Regeneration–Coated Implants Placed in Fresh Extraction Sites in the Upper Jaw. J. Oral Implantol. 2010, 36, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Balshi, T.J.; Wolfinger, G.J.; Wulc, D.; Balshi, S.F. A Prospective Analysis of Immediate Provisionalization of Single Implants. J. Prosthodont. 2011, 20, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Malo, P.; Nobre, M.A.; Lopes, A.; Moss, S.M.; Molina, G.J. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. JADA 2011, 142, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, Y.; Akoglu, B.; Kulak-Ozkan, Y. Maxillary Sinus Floor Augmentation Using Bovine Bone Grafts with Simultaneous Implant Placement: A 5-Year Prospective Follow-Up Study. Implant Dent. 2011, 20, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Mertens, C.; Steveling, H.G. Early and immediate loading of titanium implants with fluoride-modified surfaces: Results of 5-year prospective study. Clin. Oral Impl. Res. 2011, 22, 1354–1360. [Google Scholar] [CrossRef]
- Horwitz, J.; Machtei, E.E. Immediate and Delayed Restoration of Dental Implants in Patients with a History of Periodontitis: A Prospective Evaluation up to 5 Years. Int. J. Oral Maxillofac. Implant. 2012, 27, 1137–1143. [Google Scholar]
- Levine, R.A.; Sendi, P.; Bornstein, M.M. Immediate Restoration of Nonsubmerged Titanium Implants with a Sandblasted and Acid-Etched Surface: Five-Year Results of a Prospective Case Series Study Using Clinical and Radiographic Data. Int. J. Periodontics Restor. Dent. 2012, 32, 39–47. [Google Scholar]
- Davò, R.; Malevez, C.; Pons, O. Immediately loaded zygomatic implants: A 5-year prospective study. Eur. J. Oral Implantol. 2013, 6, 39–47. [Google Scholar]
- Degidi, M.; Nardi, D.; Piattelli, A. A Six-Year Follow-up of Full-Arch Immediate Restorations Fabricated with an Intraoral Welding Technique. Implant Dent. 2013, 22, 224–231. [Google Scholar] [CrossRef]
- Romanos, G.E.; Gaertner, K.; Aydin, E.; Nentwig, G.H. Long-term results after immediate loading of platform-switched implants in smokers versus nonsmokers with full-arch restorations. Int. J. Oral Maxillofac. Implant. 2013, 8, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Glauser, R. Implants with an oxidized surface placed predominately in soft bone quality and subjected to immediate occlusal loading: Results from a 7-year clinical follow-up. Clin. Implant Dent. Relat. Res. 2013, 15, 322–331. [Google Scholar] [CrossRef] [PubMed]
- Rocci, A.; Rocci, M.; Rocci, C.; Scoccia, A.; Gargari, M.; Martignoni, M.; Gottlow, J.; Sennerby, L. Immediate Loading of Brånemark System TiUnite and Machined-Surface Implants in the Posterior Mandible, Part II: A Randomized Open-Ended 9-Year Follow-up Clinical Trial. Int. J. Oral Maxillofac. Implant. 2013, 28, 891–895. [Google Scholar] [CrossRef] [PubMed]
- Tealdo, T.; Menini, M.; Bevilacqua, M.; Pera, F.; Pesce, P.; Signori, A.; Pera, P. Immediate versus delayed loading of dental implants in edentulous patients’ maxillae: A 6-year prospective study. Int. J. Prosthodont. 2014, 27, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Crespi, R.; Capparè, P.; Gastaldi, G.; Gherlone, E.F. Immediate Occlusal Loading of Full-Arch Rehabilitations: Screw-Retained Versus Cement-Retained Prosthesis. An 8-Year Clinical Evaluation. Int. J. Oral Maxillofac. Implant. 2014, 29, 1406–1411. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.F.; Reside, G.; Raes, F.; Garriga, J.S.; Tarrida, L.G.; Wiltfang, J.; Kern, M.D.M.; De Bruyn, H. Immediate Provisionalization of Dental Implants in Grafted Alveolar Ridges in the Esthetic Zone: A 5-Year Evaluation. Int. J. Periodontics Restor. Dent. 2014, 34, 477–486. [Google Scholar] [CrossRef]
- Jokstad, A.; Alkumru, H. Immediate function on the day of surgery compared with a delayed implant loading process in the mandible: A randomized clinical trial over 5 years. Clin. Oral Impl. Res. 2014, 25, 1325–1335. [Google Scholar] [CrossRef][Green Version]
- Donati, M.; La Scala, V.; Di Raimondo, R.; Speroni, S.; Testi, M.; Berglundh, T. Marginal Bone Preservation in Single-Tooth Replacement: A 5-Year Prospective Clinical Multicenter Study. Clin. Implant Dent. Relat. Res. 2015, 17, 425–434. [Google Scholar] [CrossRef]
- Shigehara, S.; Ohba, S.; Nakashima, K.; Takanashi, Y.; Asahina, I. Immediate Loading of Dental Implants Inserted in Edentulous Maxillas and Mandibles: 5-Year Results of a Clinical Study. J. Oral Implantol. 2015, 41, 701–705. [Google Scholar] [CrossRef]
- Romanos, G.E.; Gaertner, K.; Nentwig, G.H. Long-Term Evaluation of Immediately Loaded Implants in the Edentulous Mandible Using Fixed Bridges and Platform Shifting. Clin. Implant Dent. Relat. Res. 2014, 16, 601–608. [Google Scholar] [CrossRef]
- Toljanic, J.A.; Ekstrand, K.; Baer, R.A.; Thor, A. Immediate Loading of Tilted and Axial Posterior Implants in the Edentulous Maxillary Arch: A Retrospective Comparison of 5-Year Outcomes. Int. J. Oral Maxillofac. Implant. 2018, 33, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Cannizzaro, G.; Felice, P.; Boveri, M.; Lazzarini, M.; Ferri, V.; Leone, M.; Trullenque-Eriksson, A.; Esposito, M. Immediate loading of two flapless placed mandibular implants supporting cross-arch fixed prostheses: A 5-year follow-up prospective single cohort study. Eur. J. Oral Implantol. 2016, 9, 165–177. [Google Scholar] [PubMed]
- Canullo, L.; Caneva, M.; Tallarico, M. Ten-year hard and soft tissue results of a pilot double-blinded randomized controlled trial on immediately loaded post extractive implants using platform-switching concept. Clin. Oral Impl. Res. 2017, 28, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Glibert, M.; De Bruyn, H.; Östman, P.O. Six-Year Radiographic, Clinical, and Soft Tissue Outcomes of Immediately Loaded, Straight-Walled, Platform-Switched, Titanium-Alloy Implants with Nanosurface Topography. Int. J. Oral Maxillofac. Implant. 2016, 31, 167–171. [Google Scholar] [CrossRef]
- Tallarico, M.; Meloni, S.M.; Canullo, L.; Caneva, M.; Polizzi, G. Five-Year Results of a Randomized Controlled Trial Comparing Patients Rehabilitated with Immediately Loaded Maxillary Cross-Arch Fixed Dental Prosthesis Supported by Four or Six Implants Placed Using Guided Surgery. Clin. Implant Dent. Relat. Res. 2016, 18, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Agliardi, E.L.; Romeo, D.; Panigatti, S.; de Araújo Nobre, M.; Maló, P. Immediate full-arch rehabilitation of the severely atrophic maxilla supported by zygomatic implants: A prospective clinical study with minimum follow-up of 6 years. Int. J. Oral Maxillofac. Surg. 2017, 46, 1592–1599. [Google Scholar] [CrossRef] [PubMed]
- Garlini, G.; Chierichetti, V.; Redemagni, M.; Calderini, A. Single Post-Extractive Implants with Immediate Loading: Soft Tissue Response After 10 Years. Oral Health Dent. 2017, 1, 72–82. [Google Scholar]
- Meloni, S.M.; Tallarico, M.; Pisano, M.; Xhanari, E.; Canullo, L. Immediate Loading of Fixed Complete Denture Prosthesis Supported by 4–8 Implants Placed Using Guided Surgery: A 5-Year Prospective Study on 66 Patients with 356 Implants. Clin. Implant Dent. Relat. Res. 2017, 19, 195–206. [Google Scholar] [CrossRef]
- Raes, F.; Cooper, L.F.; Tarrida, L.G.; Vandromme, H.; De Bruyn, H. Oral health-related quality of life changes after placement of immediatelyloaded single implants in healed alveolar ridges or extraction sockets: A 5-year prospective follow-up study. Clin. Oral Impl. Res. 2017, 28, 662–667. [Google Scholar] [CrossRef]
- Misch, C.E.; Hahn, J.; Judy, K.W. Workshop guidelines on immediate loading in implant dentistry. J. Oral Implantol. 2004, 30, 283–288. [Google Scholar] [CrossRef]
- Szmukler-Moncler, S.; Salama, H.; Reingewirtz, Y.; Dubruille, J.H. Time of loading and effect of micromotion on bone—Dental implant interface: Review of experimental literature Timing of Loading and Effect of Micromotion on Bone—Dental Implant Interface: Review of Experimental Literature. J. Biomed. Mater. Res. 1998, 43, 192–203. [Google Scholar] [CrossRef]
- Nkenke, E.; Fenner, M. Indications for immediate loading of implants and implant success. Clin. Oral Impl. Res. 2006, 17, 19–34. [Google Scholar] [CrossRef] [PubMed]
- Gallucci, G.O.; Benic, G.I.; Eckert, S.E.; Papaspyridakos, P.; Schimmel, M.; Schrott, A.; Weber, H.-P. Consensus Statements and Clinical Recommendations for Implant Loading Protocols. Int. J. Oral Maxillofac. Implant. 2014, 29, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Weber, H.P.; Morton, D.; Gallucci, G.O.; Roccuzzo, M.; Cordaro, L.; Grutter, L. Consensus statements and recommended clinical procedures regarding loading protocols. Int. J. Oral Maxillofac. Implant. 2009, 24, 180–183. [Google Scholar]
- Chappuis, V.; Araujo, M.G.; Buser, D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000 2017, 73, 73–83. [Google Scholar] [CrossRef]
- De Bruyn, H.; Raes, F.; Cooper, L.F.; Reside, G.; Garriga, J.S.; Tarrida, L.G.; Wiltfang, J.; Kern, M. Three-years clinical outcome of immediate provisionalization of single Osseospeed implants in extraction sockets and healed ridges. Clin. Oral Impl. Res. 2013, 24, 217–223. [Google Scholar] [CrossRef]
- Testori, T.; Del Fabbro, M.; Galli, F.; Francetti, L.; Taschieri, S.; Weinstein, R. Immediate occlusal loading the same day or the after implant placement: Comparison of 2 different time frames in total edentulous lower jaws. J. Oral Implantol. 2004, 30, 307–313. [Google Scholar] [CrossRef]
- Buser, D.; Cho, J.-Y.; Yeo, A. Surgical Manual of Implant Dentistry: Step-by-Step Procedures; Quintessence Publishing: Batavia, IL, USA, 2007; Chapter 4; pp. 39–61. [Google Scholar]
- Clementini, M.; Risi, V.; De Vittorini, G. Dimensional changes after immediate implant placement with or without simultaneous regenerative procedures: A systematic review and. J. Clin. Periodontol. 2015, 1, 666–677. [Google Scholar] [CrossRef]
- Thoma, D.S.; Muhlemann, S.; Jung, R.E. Critical soft-tissue dimensions with dental implants and treatment concepts. Periodontology 2000 2014, 66, 106–118. [Google Scholar] [CrossRef]
- Cooper, L.F.; Reside, G.J.; Raes, F.; Garriga, J.S.; Tarrida, L.G.; Wiltfang, J.; Kern, M.; De Bruyn, H. Immediate provisionalization of dental implants placed in healed alveolar ridges and extraction sockets: A 5-year prospective evaluation. Int. J. Oral Maxillofac. Implant. 2014, 29, 709–717. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reference, Year | Study Design | Prosthesis Type | No. Total IL Patients | Complications/Time | No. IL Implants MAND/MAX | Follow-Up, Mean (Range) | Implant Loss and Time | Implant Survival Rate % | Bone Loss, mm (Mean ± SD) |
|---|---|---|---|---|---|---|---|---|---|
| Jaffin et al. 2007 [17] | PCS | Fixed Full | 17 | None reported | 139 (54 mand/85 max) | 60 months | No failures | 100.0% | NR |
| Calandriello et al. 2009 [18] | PCS | Single tooth | 33 | None reported | 40 mand | 60 months | Two failures in mand; three and ten months | 95.0% | 1.17 ± 0.90 |
| Degidi et al. 2009 [19] | RCT | Fixed Full/Single tooth | 82 | None reported | 262 (167 mand/73 max/22 single) + 286 control | 60 months | Three failures in mand; five years | 98.86% | 0.9 |
| Payer et al. 2010 [20] | PCS | Fixed partial/Single tooth | 24 | 1 comp/8 week | 40 mand | 60 months | Three failures in mand; 12 months | 92.50% | 1.21 ± 1.12 |
| Capelli et al. 2010 [21] | RCT | Fixed partial/Single tooth | 25 | 1 comp/33 month | 52 (38 mand/14 max) | 60 months | One failure; two months | 98.08% | 1.18 ± 0.56 |
| Prosper et al. 2010 [22] | PCS | Single tooth | 35 | None reported | 60 mand | 60 months | Two failures; 60 months | 96.67% | 1.31 ± 0.44 |
| Malchiodi et al. 2010 [23] | PCS | 58 Fixed Full/70 Fixed partial/30 Single tooth | 70 | Not Reported | 158 max | 60 months | Two failures max; 23–26 days | 98.73% | NR |
| Balshi et al. 2011 [24] | PCS | Single tooth | 140 | Not Reported | 164 (28 mand/136 max) | 66 months | Three mand/four max failures (time NR) | 95.73% | NR |
| Malo et al. 2011 [25] | PCS | Fixed Full | 245 | 1 biol. comp/4 mo 12 mech. comp | 980 mand | 10 years | Twenty-one failures (different times) | 97.86% | NR |
| Özkan et al. 2011 [26] | PCS | Twelve single tooth/36 Fixed partial | 28 | Four porcelain fractures | 84 max | 60 months | No failures | 100% | 0.34 |
| Mertens et al. 2011 [27] | PCS | Four fixed full/14 fixed partial/31 single tooth | 17 | None reported | 14 (5 mand/9 max) | 60 months | No failures | 100% | 0.1 ± 0.4 |
| Horwitz et al. 2012 [28] | PCS | Fixed full mouth/fixed partial | 19 | 74 (28 mand/46 max) | 60 months | Twelve failures before six months | 71.43% | 1.41 ± 0.67 | |
| Levine et al. 2012 [29] | PCS | Single tooth | 20 | One crown decementation | 21 mand | 60 months | No failures | 100% | 0.58 |
| Degidi et al. 2013 [31] | PCS | Fixed full | 52 | One peri-implantitis/ 25 mucositis | 256 (144 max/112 mand) | 72 months | Two max (<6, 60–72 months), one mand (<6 months) | 98.8% | 1.39 (Max) 1.29 (Mand) |
| Romanos et al. 2013 [32] | PCS | Fixed full | 20 | 163 | 80.3 months | Three failures; four months (max nonsmoker), eight months (mand. smoker), 78 months (max smoker) | 98% | 0.46 ± 0.98(Sm) 0.43 ± 1.35(NSm) | |
| Davó et al. 2013 [30] | PCS | Fixed full/fixed partial | 42 | Swelling, pain | 221 max (2 zy) | 60 months | Nine failures (eight <6 months, one at 36–48 months) | 95.93% | NR |
| Glauser et al. 2013 [33] | PCS | Twenty single tooth/one fixed full/30 fixed partial | 38 | “Nonserious compl.” | 102 (38 max/64 mand) | 61.3 months | Three max failures; <3 months | 97.10% | 1.54 |
| Rocci et al. 2013 [34] | RCT | Fixed partial | 22 | None reported | 66 mand | 9 years | Three failures; <7 months | 95.5% | 0.9 |
| Tealdo et al. 2014 [35] | CCT | Fixed Full | 34 | None reported | 163 max | 75.2 months | Ten failures; <3 months | 93.9% | 1.62 ± 1.12 |
| Crespi et al. 2014 [36] | RCT | Fixed Full | 28 | “Minor compl.” | 272 (192 max/80 mand) | 84 months | Two failures, no region; two months | 99.27% | 0.32 ± 0.21 (CR) 0.48 ± 0.40 (SR) |
| Cooper et al. 2014 [37] | PCS | Single tooth | 94 | Minor papilla problems | 113 max | 60 months | Four failures; <1 year | 96% | 0.43 ± 0.63 (FES) 0.38 ± 0.62 (HR) |
| Jokstad et al. 2014 [38] | RCT | Fixed full | 16 | None reported | 64 mand | 60 months | No failures | 100% | 1.3 ± 0.7 |
| Donati et al. 2015 [39] | RCT | Single tooth | 104 | “Minor compl.” | 111 anterior | 60 months | Four failures before three months | 97.10% | 0.27 |
| Shigehara et al. 2015 [40] | PCS | Fixed full | 27 | “Minor compl.” | 189 | 77.9 months | No failures | 100.0% | NR |
| Romanos et al. 2014 [41] | RCT | Fixed partial | 13 | None reported | 78 mand | 12.27 years | No failures | 100% | 0.70 ± 1.09 (Mes) 0.43 ± 1.02 (Dis) |
| Toljanic et al. 2016 [42] | PCS | Fixed full | 51 | “Minor compl.” | 306 max | 60 months | Twenty failures; two years | 92% | 0.44 ± 1.25 |
| Cannizzaro et al. 2016 [43] | PCS | Fixed full | 79 | “Minor compl.” | 158 mand | 60 months | Two failures; three weeks | 98.70% | 0.69 |
| Canullo et al. 2016 [44] | RCT | Single tooth | 22 | None reported | 22 max | 10 years | No failures | 100% | 0.49 ± 0.27 |
| Glibert et al. 2016 [45] | PCS | Nineteen single tooth/23 fixed partial/eight fixed full | 40 | Not reported | 112 (40 mand/72 max) | 6.2 years | One failure at three months | 99.10% | 0.35 |
| Tallarico et al. 2016 [46] | RCT | Fixed full | 40 | “Minor compl.” | 200 max | 60 months | Seven failures; five at <6 months, two at 24–36 months | 97.50% | 1.71 ± 0.42 (Ao4) 1.51 ± 36 (Ao6) |
| Agliardi et al. 2017 [47] | PCS | Fixed full | 15 | “Minor compl.” | 60 max (42 zy) | 79 months | No failures | 100% | 1.39 ± 0.10 |
| Garlini et al. 2017 [48] | PCS | Fixed partial | 94 | 1 suppuration | 147 (41 mand/106 max) | 10 years | Two failures; <1 month | 98.56% | NR |
| Meloni et al. 2017 [49] | PCS | Fixed full | 66 | Minor or technical | 356 (92 mand/264 max) | 71.2 months | Five failures in 0–1 years, two failures in 3–5 years | 98% | 1.61 ± 0.41 |
| Raes et al. 2017 [50] | PCS | Fixed partial | 96 | “Minor compl.” | 102 (single ant max) | 60 months | Two failures; 6–12 months | 98% | NR |
| Interval, Months | Implants at Risk | Failed Implants | Dropouts/Lost to Follow-Up | Implant Survival Rate | Cumulative Survival Rate |
|---|---|---|---|---|---|
| 0–6 | 5163 | 78 | 24 | 98.49% | 98.49% |
| 6–12 | 5061 | 18 | 55 | 99.64% | 98.14% |
| 12–24 | 4991 | 5 | 66 | 99.90% | 98.04% |
| 24–36 | 4917 | 4 | 62 | 99.92% | 97.96% |
| 36–48 | 4851 | 7 | 61 | 99.86% | 97.82% |
| 48–60 | 4783 | 8 | 1644 | 99.83% | 97.66% |
| 60–72 | 3131 | 3 | 1598 | 99.90% | 97.56% |
| 72–84 | 1530 | 2 | 491 | 99.87% | 97.43% |
| 84–96 | 1037 | 2 | 715 | 99.81% | 97.25% |
| 96–108 | 320 | 1 | 76 | 99.69% | 96.94% |
| 108–120 | 243 | 0 | 67 | 100.0% | 96.94% |
| >120 | 176 | 0 | 100.0% | 96.94% |
| Reference, Year | Selection 1 | Selection 2 | Selection 3 | Selection 4 | Comparability | Outcome 1 | Outcome 2 | Outcome 3 | Total |
|---|---|---|---|---|---|---|---|---|---|
| Jaffin et al. 2007 [17] | * | * | 2 * | ||||||
| Calandriello et al. 2009 [18] | * | * | 2 * | ||||||
| Degidi et al. 2009 [19] | * | * | * | * | 4 * | ||||
| Payer et al. 2010 [20] | * | * | * | * | 4 * | ||||
| Capelli et al. 2010 [21] | * | * | * | * | * | * | 6 * | ||
| Prosper et al. 2010 [22] | * | * | * | * | 4 * | ||||
| Malchiodi et al. 2010 [23] | * | * | * | * | 4 * | ||||
| Balshi et al. 2011 [24] | * | * | * | 3 * | |||||
| Malo et al. 2011 [25] | * | * | * | 3 * | |||||
| Özkan et al. 2011 [26] | * | * | * | * | * | 5 * | |||
| Mertens et al. 2011 [27] | * | * | * | * | * | 5 * | |||
| Horwitz et al. 2012 [28] | * | * | * | * | 4 * | ||||
| Levine et al. 2012 [29] | * | * | * | * | 4 * | ||||
| Degidi et al. 2013 [31] | * | * | * | 3 * | |||||
| Romanos et al. 2013 [32] | * | * | * | * | 4 * | ||||
| Davó et al. 2013 [30] | * | * | * | 3 * | |||||
| Glauser et al. 2013 [33] | * | * | * | * | 4 * | ||||
| Rocci et al. 2013 [34] | * | * | * | * | * | * | 6 * | ||
| Tealdo et al. 2014 [35] | * | * | * | * | * | 5 * | |||
| Crespi et al. 2014 [36] | * | ** | * | * | * | 6 * | |||
| Cooper et al. 2014 [37] | * | * | * | * | 4 * | ||||
| Jokstad et al. 2014 [38] | * | * | * | ** | * | * | * | 8 * | |
| Donati et al. 2015 [39] | * | * | * | * | 4 * | ||||
| Shigehara et al. 2015 [40] | * | * | * | * | 4 * | ||||
| Romanos et al. 2014 [41] | * | * | * | * | * | 5 * | |||
| Toljanic et al. 2016 [42] | * | * | * | * | * | 5 * | |||
| Cannizzaro et al. 2016 [43] | * | * | * | * | * | 5 * | |||
| Canullo et al. 2016 [44] | * | * | * | * | * | * | * | 7 * | |
| Glibert et al. 2016 [45] | * | * | * | * | 4 * | ||||
| Tallarico et al. 2016 [46] | * | * | * | * | * | 5 * | |||
| Agliardi et al. 2017 [47] | * | * | * | * | 4 * | ||||
| Garlini et al. 2017 [48] | * | * | * | * | 4 * | ||||
| Meloni et al. 2017 [49] | * | * | * | * | 4 * | ||||
| Raes et al. 2017 [50] | * | * | * | * | 4 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Del Fabbro, M.; Testori, T.; Kekovic, V.; Goker, F.; Tumedei, M.; Wang, H.-L. A Systematic Review of Survival Rates of Osseointegrated Implants in Fully and Partially Edentulous Patients Following Immediate Loading. J. Clin. Med. 2019, 8, 2142. https://doi.org/10.3390/jcm8122142
Del Fabbro M, Testori T, Kekovic V, Goker F, Tumedei M, Wang H-L. A Systematic Review of Survival Rates of Osseointegrated Implants in Fully and Partially Edentulous Patients Following Immediate Loading. Journal of Clinical Medicine. 2019; 8(12):2142. https://doi.org/10.3390/jcm8122142
Chicago/Turabian StyleDel Fabbro, Massimo, Tiziano Testori, Vladan Kekovic, Funda Goker, Margherita Tumedei, and Hom-Lay Wang. 2019. "A Systematic Review of Survival Rates of Osseointegrated Implants in Fully and Partially Edentulous Patients Following Immediate Loading" Journal of Clinical Medicine 8, no. 12: 2142. https://doi.org/10.3390/jcm8122142
APA StyleDel Fabbro, M., Testori, T., Kekovic, V., Goker, F., Tumedei, M., & Wang, H.-L. (2019). A Systematic Review of Survival Rates of Osseointegrated Implants in Fully and Partially Edentulous Patients Following Immediate Loading. Journal of Clinical Medicine, 8(12), 2142. https://doi.org/10.3390/jcm8122142