Type 1 or Type 2 Myocardial Infarction in Patients with a History of Coronary Artery Disease: Data from the Emergency Department

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Methods
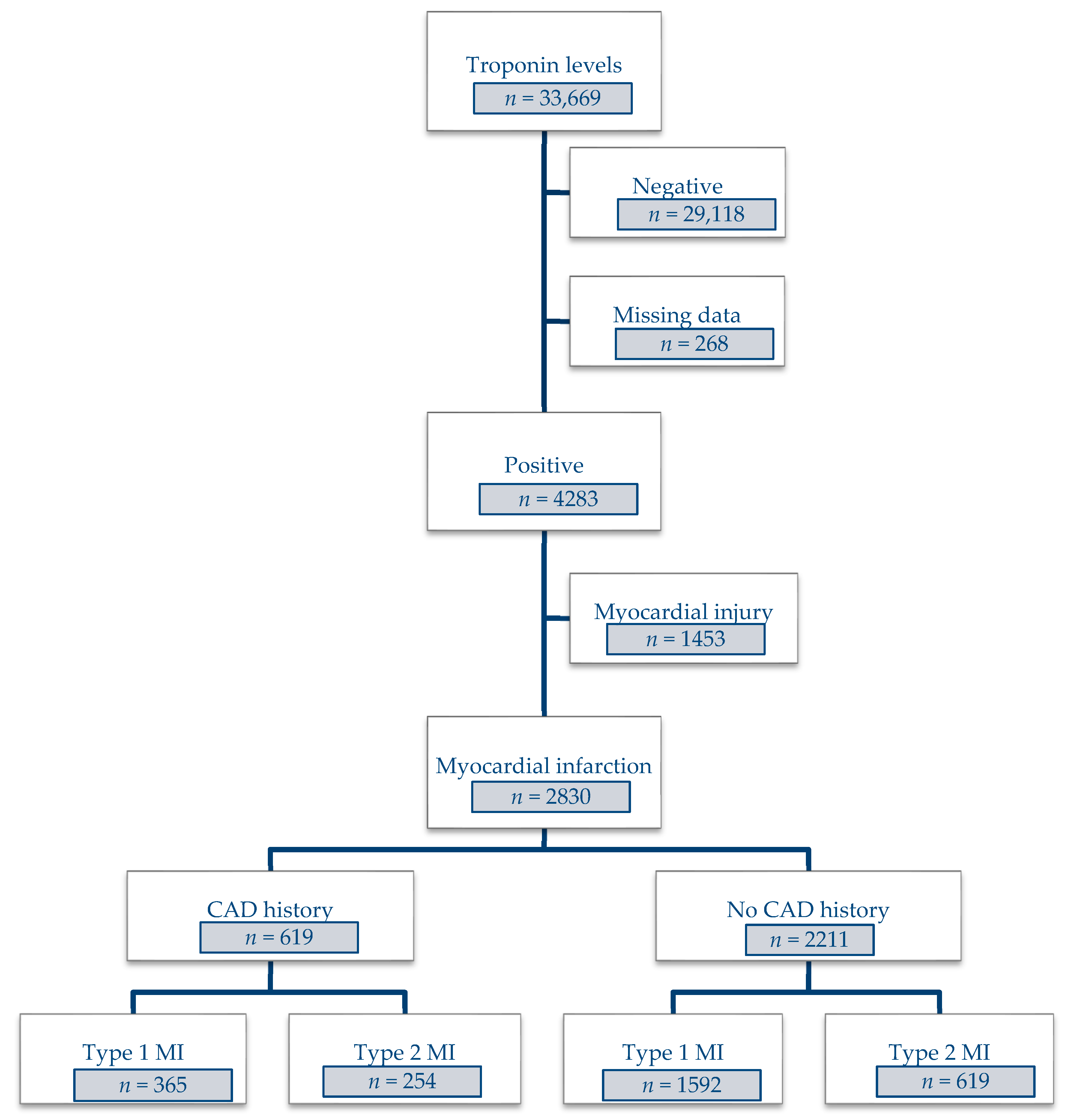
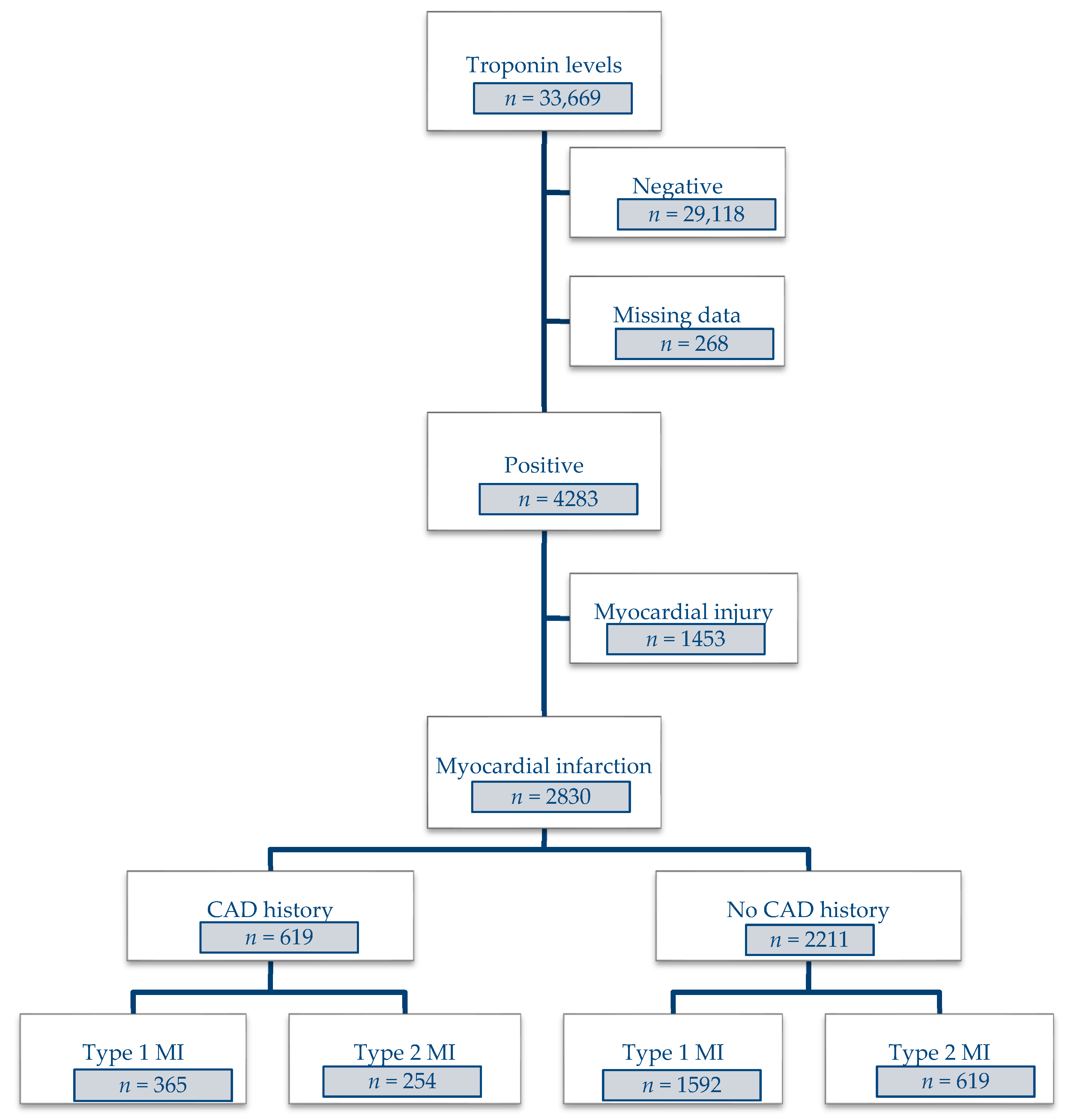
2.1. Study Population
2.2. Diagnostic Classification
2.3. Data Collection
2.4. Statistical Analyses
3. Results
3.1. All MI Patients
3.2. Patients with CAD Disease
3.2.1. Risk Factors and History
3.2.2. Presentation at Admission
3.2.3. Coronary Angiography Data
3.2.4. Overall In-Hospital and Cardiovascular Mortality
3.2.5. Factors Associated with the Occurrence of T2MI
4. Discussion
- T2MI was common in an unselected population (31% of MI in our cohort), especially among patients with a known history of CAD (41%).
- The existence of known underlying CAD increased the probability of having T2MI versus T1MI by 40%.
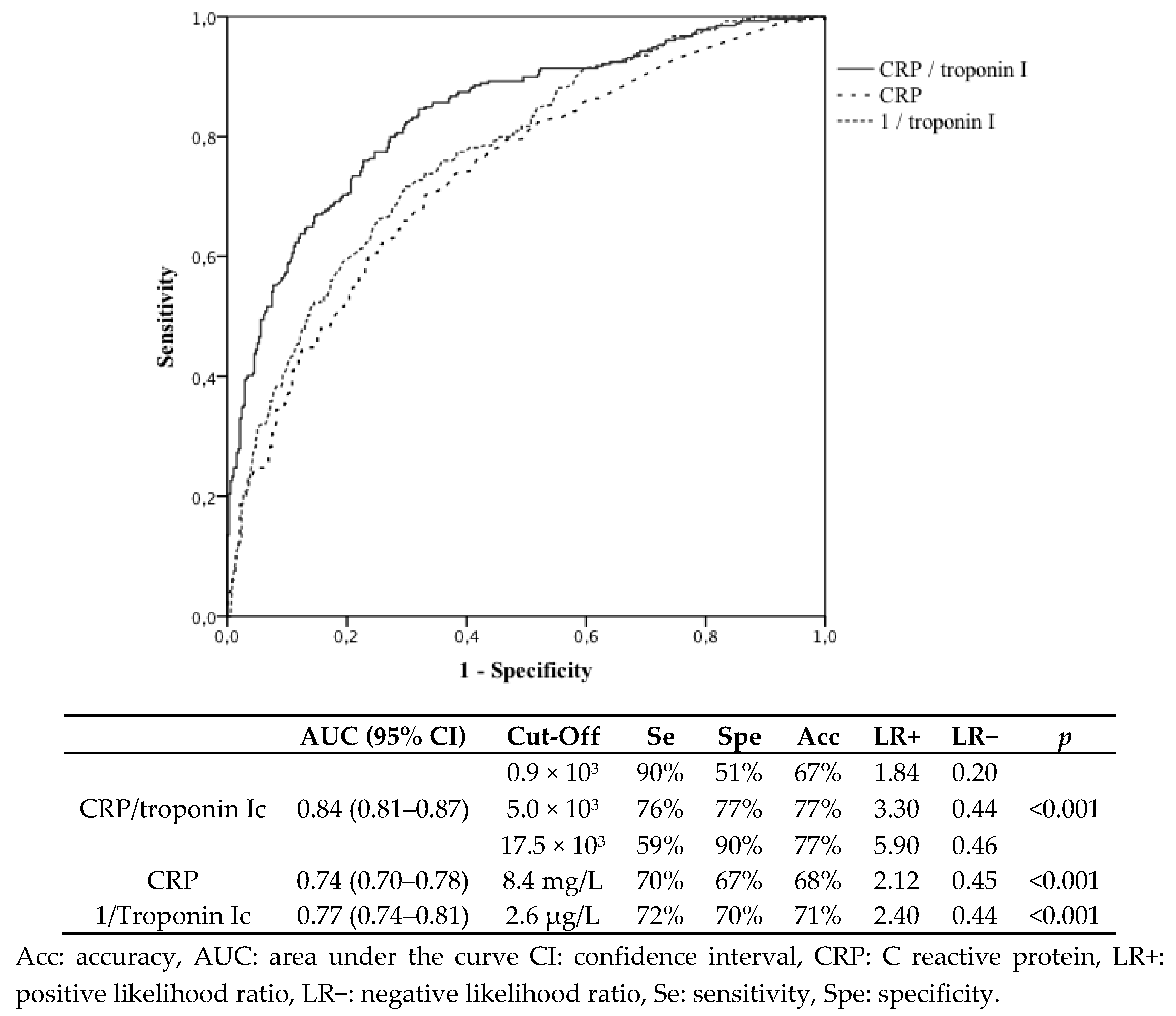
- In MI patients with a history of CAD, a high CRP/troponin ratio predicted T2MI remarkably well.
4.1. CAD Predisposes a Patient to T2MI More Than T1MI
4.2. Differentiation between T1MI and T2MI in CAD Patients
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018). J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef] [PubMed]
- Putot, A.; Derrida, S.B.; Zeller, M.; Avondo, A.; Ray, P.; Manckoundia, P.; Cottin, Y. Short-Term Prognosis of Myocardial Injury, Type 1, and Type 2 Myocardial Infarction in the Emergency Unit. Am. J. Med. 2018, 131, 1209–1219. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.S.V.; McAllister, D.A.; Mills, R.; Lee, K.K.; Churchhouse, A.M.D.; Fleming, K.M.; Layden, E.; Anand, A.; Fersia, O.; Joshi, N.V.; et al. Sensitive troponin assay and the classification of myocardial infarction. Am. J. Med. 2015, 128, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Gluckman, T.J.; Tcheng, J.E. What’s in a Name? The New ICD-10 (10th Revision of the International Statistical Classification of Diseases and Related Health Problems) Codes and Type 2 Myocardial Infarction. Circulation 2017, 136, 1180–1182. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Garzón, J.; Sandoval, Y.; Smith, S.W.; Love, S.; Schulz, K.; Thordsen, S.E.; Johnson, B.K.; Driver, B.; Jacoby, K.; Carlson, M.D.; et al. Discordance between ICD-Coded Myocardial Infarction and Diagnosis according to the Universal Definition of Myocardial Infarction. Clin. Chem. 2017, 63, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Nestelberger, T.; Boeddinghaus, J.; Badertscher, P.; Twerenbold, R.; Wildi, K.; Breitenbücher, D.; Sabti, Z.; Puelacher, C.; Rubini Giménez, M.; Kozhuharov, N.; et al. Effect of Definition on Incidence and Prognosis of Type 2 Myocardial Infarction. J. Am. Coll. Cardiol. 2017, 70, 1558–1568. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D.; Writing Group on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Third universal definition of myocardial infarction. Glob. Heart 2012, 7, 275–295. [Google Scholar] [CrossRef]
- Saaby, L.; Poulsen, T.S.; Hosbond, S.; Larsen, T.B.; Pyndt Diederichsen, A.C.; Hallas, J.; Thygesen, K.; Mickley, H. Classification of myocardial infarction: Frequency and features of type 2 myocardial infarction. Am. J. Med. 2013, 126, 789–797. [Google Scholar] [CrossRef]
- Stein, G.Y.; Herscovici, G.; Korenfeld, R.; Matetzky, S.; Gottlieb, S.; Alon, D.; Gevrielov-Yusim, N.; Iakobishvili, Z.; Fuchs, S. Type-II myocardial infarction--patient characteristics, management and outcomes. PLoS ONE 2014, 9, e84285. [Google Scholar] [CrossRef]
- Ong, A.T.L.; Serruys, P.W.; Mohr, F.W.; Morice, M.-C.; Kappetein, A.P.; Holmes, D.R.; Mack, M.J.; van den Brand, M.; Morel, M.-A.; van Es, G.-A.; et al. The SYNergy between percutaneous coronary intervention with TAXus and cardiac surgery (SYNTAX) study: Design, rationale, and run-in phase. Am. Heart J. 2006, 151, 1194–1204. [Google Scholar] [CrossRef]
- Gupta, S.; Vaidya, S.R.; Arora, S.; Bahekar, A.; Devarapally, S.R. Type 2 versus type 1 myocardial infarction: A comparison of clinical characteristics and outcomes with a meta-analysis of observational studies. Cardiovasc. Diagn. Ther. 2017, 7, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Baron, T.; Hambraeus, K.; Sundström, J.; Erlinge, D.; Jernberg, T.; Lindahl, B.; TOTAL-AMI study group. Type 2 myocardial infarction in clinical practice. Heart 2015, 101, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Javed, U.; Aftab, W.; Ambrose, J.A.; Wessel, R.J.; Mouanoutoua, M.; Huang, G.; Barua, R.S.; Weilert, M.; Sy, F.; Thatai, D. Frequency of elevated troponin I and diagnosis of acute myocardial infarction. Am. J. Cardiol. 2009, 104, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Strassle, P.D.; Qamar, A.; Wheeler, E.N.; Levine, A.L.; Misenheimer, J.A.; Cavender, M.A.; Stouffer, G.A.; Kaul, P. Impact of Type 2 Myocardial Infarction (MI) on Hospital-Level MI Outcomes: Implications for Quality and Public Reporting. J. Am. Heart Assoc. 2018, 7, e008661. [Google Scholar] [CrossRef]
- Gaggin, H.K.; Liu, Y.; Lyass, A.; van Kimmenade, R.R.J.; Motiwala, S.R.; Kelly, N.P.; Mallick, A.; Gandhi, P.U.; Ibrahim, N.E.; Simon, M.L.; et al. Incident Type 2 Myocardial Infarction in a Cohort of Patients Undergoing Coronary or Peripheral Arterial AngiographyClinical Perspective. Circulation 2017, 135, 116–127. [Google Scholar] [CrossRef]
- Chapman, A.R.; Shah, A.S.V.; Lee, K.K.; Anand, A.; Francis, O.; Adamson, P.; McAllister, D.A.; Strachan, F.; Newby, D.E.; Mills, N.L. Long Term Outcomes in Patients with Type 2 Myocardial Infarction and Myocardial Injury. Circulation 2017, 137, 1236–1245. [Google Scholar] [CrossRef]
- Sandoval, Y.; Jaffe, A.S. Type 2 Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 73, 1846–1860. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Chest pain, dyspnea and other symptoms in patients with type 1 and 2 myocardial infarction. A literature review. Int. J. Cardiol. 2016, 215, 20–22. [Google Scholar] [CrossRef]
- Putot, A.; Jeanmichel, M.; Chagué, F.; Manckoundia, P.; Cottin, Y.; Zeller, M. Type 2 Myocardial Infarction: A Geriatric Population-based Model of Pathogenesis. Aging Dis. 2019. [Google Scholar] [CrossRef]
- Putot, A.; Chague, F.; Manckoundia, P.; Cottin, Y.; Zeller, M. Post-Infectious Myocardial Infarction: New Insights for Improved Screening. J. Clin. Med. 2019, 8, 827. [Google Scholar] [CrossRef]
- Gerber, Y.; Weston, S.A.; Jiang, R.; Roger, V.L. The changing epidemiology of myocardial infarction in Olmsted County, Minnesota, 1995–2012. Am. J. Med. 2015, 128, 144–151. [Google Scholar] [CrossRef] [PubMed]
- French, J.K.; Burgess, S.; Chew, D.P. Re-infarction after primary percutaneous coronary intervention. Curr. Opin. Cardiol. 2015, 30, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Seto, T.B.; Taira, D.A.; Berezin, R.; Chauhan, M.S.; Cutlip, D.E.; Ho, K.K.; Kuntz, R.E.; Cohen, D.J. Percutaneous coronary revascularization in elderly patients: Impact on functional status and quality of life. Ann. Intern. Med. 2000, 132, 955–958. [Google Scholar] [CrossRef] [PubMed]
- Consuegra-Sánchez, L.; Martínez-Díaz, J.J.; de Guadiana-Romualdo, L.G.; Wasniewski, S.; Esteban-Torrella, P.; Clavel-Ruipérez, F.G.; Bardají, A.; Castillo-Moreno, J.A.; Kaski, J.C. No additional value of conventional and high-sensitivity cardiac troponin over clinical scoring systems in the differential diagnosis of type 1 vs. type 2 myocardial infarction. Clin. Chem. Lab. Med. 2018, 56, 702–709. [Google Scholar] [CrossRef]
- Greenslade, J.H.; Adikari, T.; Mueller, C.; Sandoval, Y.; Nestelberger, T.; Parsonage, W.; Hawkins, T.; Cullen, L. Characteristics and occurrence of type 2 myocardial infarction in emergency department patients: A prospective study. Emerg. Med. J. 2018, 35, 169–175. [Google Scholar] [CrossRef]
- Neumann, J.T.; Sörensen, N.A.; Rübsamen, N.; Ojeda, F.; Renné, T.; Qaderi, V.; Teltrop, E.; Kramer, S.; Quantius, L.; Zeller, T.; et al. Discrimination of patients with type 2 myocardial infarction. Eur. Heart J. 2017, 38, 3514–3520. [Google Scholar] [CrossRef]
- Nowak, R.M.; Jacobsen, G.; Christenson, R.H.; Moyer, M.; Hudson, M.; McCord, J. Differentiating type 1 and 2 acute myocardial infarctions using the N-terminal pro B-type natriuretic peptide/cardiac troponin T ratio. Am. J. Emerg. Med. 2018, 36, 1849–1854. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Univariate | Multivariate | |||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Age | 1.06 (1.05–1.07) | <0.001 | 1.02 (1.01–1.03) | <0.001 |
| Female | 2.78 (2.36–3.28) | <0.001 | 1.64 (1.30–2.06) | <0.001 |
| Obesity | 0.39 (0.30–0.50) | <0.001 | 0.42 (0.31–0.57) | <0.001 |
| Current smoking | 0.26 (0.22–0.31) | <0.001 | 0.48 (0.38–0.61) | <0.001 |
| Family history of CAD | 0.33 (0.26–0.42) | <0.001 | 0.47 (0.35–0.63) | <0.001 |
| Hypertension | 1.95 (1.65–2.32) | <0.001 | 1.05 (0.83–1.32) | 0.7 |
| History of CAD | 1.79 (11.49–2.15) | <0.001 | 1.38 (1.08–1.77) | 0.010 |
| Chronic kidney disease | 2.71 (2.03–3.60) | <0.001 | 1.45 (0.99–2.12) | 0.06 |
| Troponin Ic | 0.97 (0.97–0.98) | <0.001 | 0.99 (0.99–0.99) | <0.001 |
| CRP > 3 mg/L | 3.44 (2.79–4.24) | <0.001 | 2.76 (2.16–3.53) | <0.001 |
| Renal failure at admission | 2.60 (2.20–3.08) | <0.001 | 1.34 (1.05–1.70) | 0.02 |
| STEMI | 0.11 (0.09–0.13) | <0.001 | 0.20 (0.15–0.26) | <0.001 |
| T1MI (n = 365) | T2MI (n = 254) | p | |
|---|---|---|---|
| Risk factors | |||
| Age, years | 72 (62–81) | 82 (71–87) | <0.001 |
| Female | 84 (23%) | 98 (39%) | <0.001 |
| Obesity | 97 (27%) | 27 (11%) | <0.001 |
| Hypercholesterolemia | 259 (71%) | 169 (67%) | 0.2 |
| Hypertension | 276 (76%) | 211 (83%) | 0.03 |
| Diabetes | 138 (38%) | 99 (39%) | 0.8 |
| Current smoking | 243 (67%) | 101 (40%) | <0.001 |
| Family history of CAD | 108 (30%) | 37 (15%) | <0.001 |
| Heart failure | 36 (10%) | 78 (31%) | <0.001 |
| Stroke | 40 (11%) | 50 (20%) | 0.002 |
| Peripheral arteriopathy | 54 (15%) | 55 (22%) | 0.03 |
| Chronic kidney disease | 45 (12%) | 55 (22%) | 0.002 |
| Usual treatments | |||
| Anti-platelet | 301 (83%) | 189 (74%) | 0.01 |
| Anticoagulant | 55 (15%) | 69 (27%) | <0.001 |
| Clinical data | |||
| HR, bpm | 76 (66–92) | 84 (72–102) | <0.001 |
| SBP, mmHg | 135 (120–158) | 131 (114–160) | 0.2 |
| DBP, mmHg | 77 (66–88) | 70 (60–84) | <0.001 |
| STEMI | 136 (37%) | 28 (11%) | <0.001 |
| Admission to ICU | 362 (100%) | 141 (55%) | <0.001 |
| Biological data | |||
| Troponin Ic (peak), µg/L | 8.2 (1.8–36.0) | 0.80 (0.2–5.3) | <0.001 |
| CRP > 3 mg/L | 215 (62%) | 218 (88%) | <0.001 |
| Hemoglobin, g/dL | 13.8 (12.3–15.2) | 12.1 (10.3–13.5) | <0.001 |
| Creatinine, µmol/L | 89 (72–114) | 99 (77–146) | <0.001 |
| Angiographic data | |||
| Coronary angiography | 351 (96%) | 105 (41%) | <0.001 |
| Non obstructive/normal | 19 (5%) | 16 (15%) | <0.001 |
| Three-vessel disease | 150 (43%) | 59 (56%) | 0.01 |
| SYNTAX score | 12 (5–21) | 12 (2–23) | 0.9 |
| Acute management | |||
| PCI | 235 (64%) | 29 (11%) | <0.001 |
| CABG | 29 (8%) | 4 (4%) | 0.1 |
| Thrombolysis | 13 (4%) | 0 (0%) | 0.05 |
| In-hospital mortality | |||
| Death | 24 (7%) | 38 (15%) | 0.001 |
| Death, CV causes | 23 (6%) | 24 (9%) | 0.1 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Obesity | 0.33 (0.21–0.52) | <0.001 | 0.39 (0.23–0.66) | <0.001 |
| Current smoking | 0.33 (0.24–0.46) | <0.001 | 0.41 (0.27–0.62) | <0.001 |
| Family history of CAD | 0.41 (0.27–0.61) | <0.001 | 0.51 (0.32–0.83) | 0.007 |
| Heart failure | 4.05 (2.62–6.26) | <0.001 | 2.98 (1.73–5.14) | <0.001 |
| Troponin Ic | 0.96 (0.95–0.98) | <0.001 | 0.97 (0.96–0.99) | <0.001 |
| CRP > 3 mg/L | 4.38 (2.84–6.76) | <0.001 | 3.53 (2.17–5.75) | <0.001 |
| Acute renal failure | 1.94 (1.40–2.68) | <0.001 | 1.22 (0.80–1.85) | 0.4 |
| STEMI | 0.21 (0.13–0.33) | <0.001 | 0.37 (0.21–0.64) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Putot, A.; Jeanmichel, M.; Chagué, F.; Avondo, A.; Ray, P.; Manckoundia, P.; Zeller, M.; Cottin, Y. Type 1 or Type 2 Myocardial Infarction in Patients with a History of Coronary Artery Disease: Data from the Emergency Department. J. Clin. Med. 2019, 8, 2100. https://doi.org/10.3390/jcm8122100
Putot A, Jeanmichel M, Chagué F, Avondo A, Ray P, Manckoundia P, Zeller M, Cottin Y. Type 1 or Type 2 Myocardial Infarction in Patients with a History of Coronary Artery Disease: Data from the Emergency Department. Journal of Clinical Medicine. 2019; 8(12):2100. https://doi.org/10.3390/jcm8122100
Chicago/Turabian StylePutot, Alain, Mélanie Jeanmichel, Frédéric Chagué, Aurélie Avondo, Patrick Ray, Patrick Manckoundia, Marianne Zeller, and Yves Cottin. 2019. "Type 1 or Type 2 Myocardial Infarction in Patients with a History of Coronary Artery Disease: Data from the Emergency Department" Journal of Clinical Medicine 8, no. 12: 2100. https://doi.org/10.3390/jcm8122100
APA StylePutot, A., Jeanmichel, M., Chagué, F., Avondo, A., Ray, P., Manckoundia, P., Zeller, M., & Cottin, Y. (2019). Type 1 or Type 2 Myocardial Infarction in Patients with a History of Coronary Artery Disease: Data from the Emergency Department. Journal of Clinical Medicine, 8(12), 2100. https://doi.org/10.3390/jcm8122100