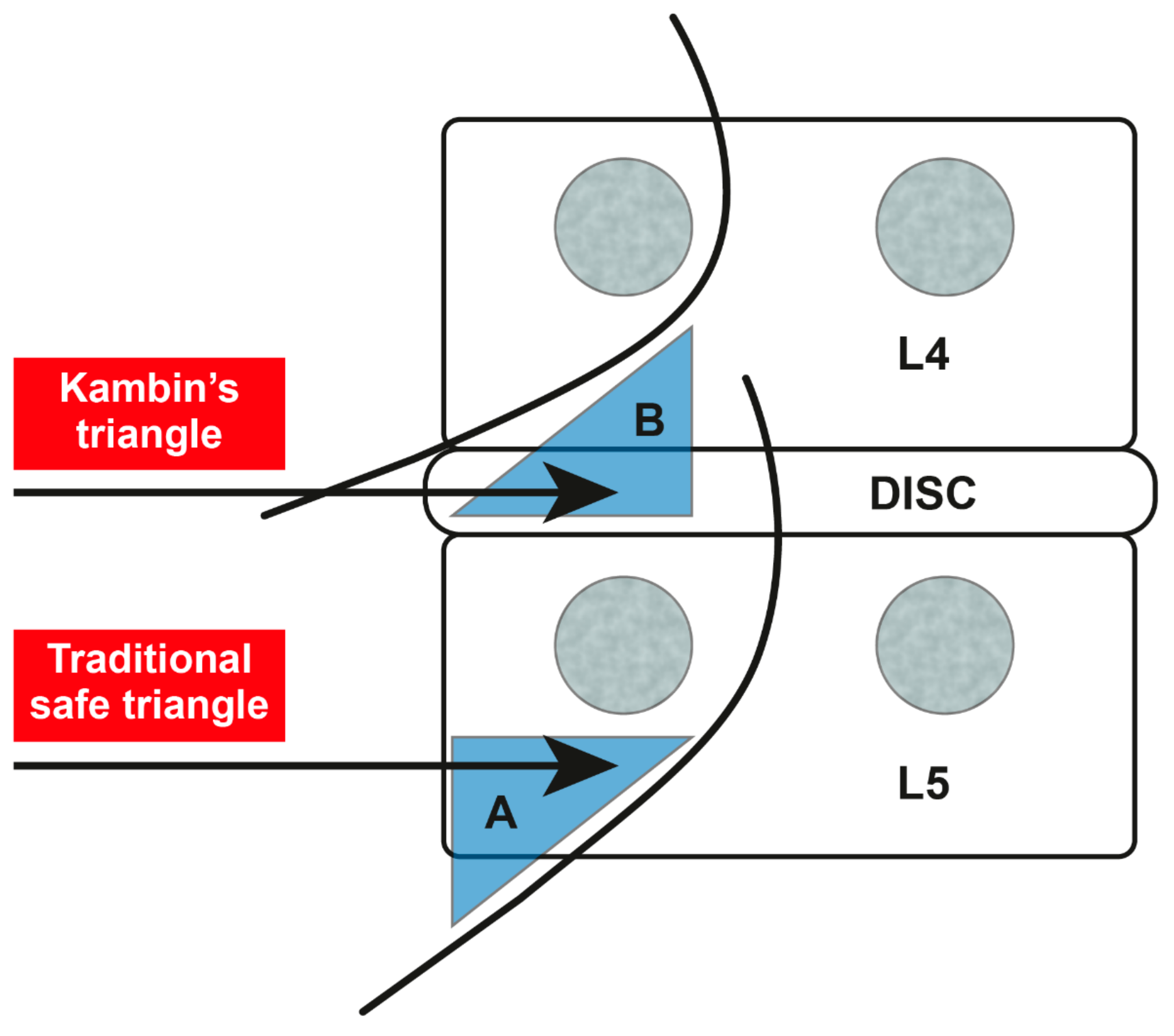
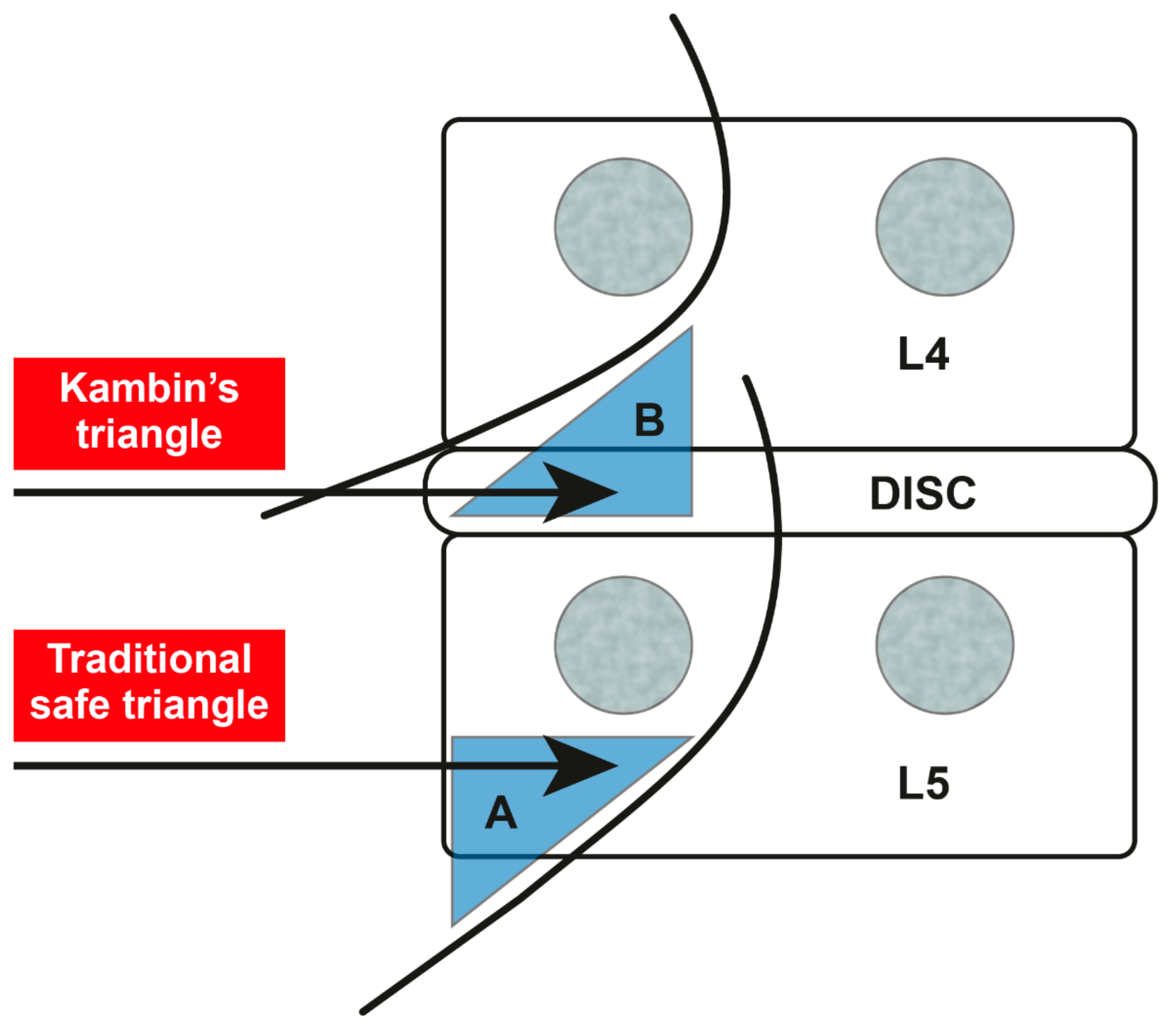
Kambin’s Triangle Approach versus Traditional Safe Triangle Approach for Percutaneous Transforaminal Epidural Adhesiolysis Using an Inflatable Balloon Catheter: A Pilot Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Design and Randomization
2.3. Percutaneous Transforaminal Epidural Adhesiolysis Using an Inflatable Balloon Catheter
2.4. Evaluation of Outcome Variables
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Manchikanti, L.; Abdi, S.; Atluri, S.; Benyamin, R.M.; Boswell, M.V.; Buenaventura, R.M.; Bryce, D.A.; Burks, P.A.; Caraway, D.L.; Calodney, A.K.; et al. An update of comprehensive evidence-based guidelines for interventional techniques in chronic spinal pain. Part II: Guidance and recommendations. Pain Physician 2013, 16, S49–S283. [Google Scholar] [PubMed]
- Tran, D.Q.; Duong, S.; Finlayson, R.J. Lumbar spinal stenosis: A brief review of the nonsurgical management. Can. J. Anaesth. 2010, 57, 694–703. [Google Scholar] [CrossRef] [PubMed]
- Yousef, A.A.; AS, E.L.-D.; Al-Deeb, A.E. The role of adding hyaluronidase to fluoroscopically guided caudal steroid and hypertonic saline injection in patients with failed back surgery syndrome: A prospective, double-blinded, randomized study. Pain Pract. 2010, 10, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Iversen, T.; Solberg, T.K.; Romner, B.; Wilsgaard, T.; Twisk, J.; Anke, A.; Nygaard, O.; Hasvold, T.; Ingebrigtsen, T. Effect of caudal epidural steroid or saline injection in chronic lumbar radiculopathy: Multicentre, blinded, randomised controlled trial. BMJ 2011, 343, d5278. [Google Scholar] [CrossRef]
- Manchikanti, L.; Bakhit, C.E. Percutaneous lysis of epidural adhesions. Pain Physician 2000, 3, 46–64. [Google Scholar]
- Lee, J.H.; Lee, S.H. Clinical effectiveness of percutaneous adhesiolysis using Navicath for the management of chronic pain due to lumbosacral disc herniation. Pain Physician 2012, 15, 213–221. [Google Scholar]
- Manchikanti, L.; Singh, V.; Bakhit, C.E.; Fellows, B. Interventional techniques in the management of chronic pain: Part 1.0. Pain Physician 2000, 3, 7–42. [Google Scholar]
- Karm, M.H.; Choi, S.S.; Kim, D.H.; Park, J.Y.; Lee, S.; Park, J.K.; Suh, Y.J.; Leem, J.G.; Shin, J.W. Percutaneous epidural adhesiolysis using inflatable balloon catheter and balloon-less catheter in central lumbar spinal stenosis with neurogenic claudication: A randomized controlled trial. Pain Physician 2018, 21, 593–606. [Google Scholar]
- Park, C.H.; Lee, S.H. Effectiveness of percutaneous transforaminal adhesiolysis in patients with lumbar neuroforaminal spinal stenosis. Pain Physician 2013, 16, E37–E43. [Google Scholar]
- Slipman, C.W.; Chow, D.W. Therapeutic spinal corticosteroid injections for the management of radiculopathies. Phys. Med. Rehabil. Clin. N. Am. 2002, 13, 697–711. [Google Scholar] [CrossRef]
- Koh, W.U.; Choi, S.S.; Park, S.Y.; Joo, E.Y.; Kim, S.H.; Lee, J.D.; Shin, J.Y.; Suh, J.H.; Leem, J.G.; Shin, J.W. Transforaminal hypertonic saline for the treatment of lumbar lateral canal stenosis: A double-blinded, randomized, active-control trial. Pain Physician 2013, 16, 197–211. [Google Scholar]
- Kim, S.H.; Choi, W.J.; Suh, J.H.; Jeon, S.R.; Hwang, C.J.; Koh, W.U.; Lee, C.; Leem, J.G.; Lee, S.C.; Shin, J.W. Effects of transforaminal balloon treatment in patients with lumbar foraminal stenosis: A randomized, controlled, double-blind trial. Pain Physician 2013, 16, 213–224. [Google Scholar] [PubMed]
- Shin, J.W. A new approach to neuroplasty. Korean J. Pain 2013, 26, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Nam, H.S.; Cho, S.K.; Jung, H.J.; Lee, B.J.; Park, Y. Kambin’s triangle approach of lumbar transforaminal epidural injection with spinal stenosis. Ann. Rehabil. Med. 2011, 35, 833–843. [Google Scholar] [CrossRef]
- Fairbank, J.C.; Pynsent, P.B. The oswestry disability index. Spine (Phila Pa 1976) 2000, 25, 2940–2953. [Google Scholar] [CrossRef]
- Kim, D.Y.; Lee, S.H.; Lee, H.Y.; Lee, H.J.; Chang, S.B.; Chung, S.K.; Kim, H.J. Validation of the Korean version of the oswestry disability index. Spine (Phila Pa 1976) 2005, 30, E123–E127. [Google Scholar] [CrossRef]
- Seo, D.-K.; Lee, S.; Lee, G.; Lee, M.-S.; Yoon, S.-H.; Choi, S.-S.; Shin, J.-W. Retrodiscal epidural balloon adhesiolysis through Kambin’s triangle in chronic lumbar spinal stenosis: A retrospective analysis and technical considerations. Medicine (Baltimore) 2018, 97, e12791. [Google Scholar] [CrossRef]
- Manchikanti, L.; Pampati, V.; Fellows, B.; Rivera, J.J.; Damron, K.S.; Beyer, C.; Cash, K.A. Effectiveness of percutaneous adhesiolysis with hypertonic saline neurolysis in refractory spinal stenosis. Pain Physician 2001, 4, 366–373. [Google Scholar]
- Anderson, S.R.; Racz, G.B.; Heavner, J. Evolution of epidural lysis of adhesions. Pain Physician 2000, 3, 262–270. [Google Scholar]
- Trescot, A.M.; Chopra, P.; Abdi, S.; Datta, S.; Schultz, D.M. Systematic review of effectiveness and complications of adhesiolysis in the management of chronic spinal pain: An update. Pain Physician 2007, 10, 129–146. [Google Scholar]
- Manchikanti, L.; Cash, K.A.; Pampati, V.; Damron, K.S.; McManus, C.D. Evaluation of lumbar transforaminal epidural injections with needle placement and contrast flow patterns: A prospective, descriptive report. Pain Physician 2004, 7, 217–223. [Google Scholar] [PubMed]
- Alleyne, C.H., Jr.; Cawley, C.M.; Shengelaia, G.G.; Barrow, D.L. Microsurgical anatomy of the artery of Adamkiewicz and its segmental artery. J. Neurosurg. 1998, 89, 791–795. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.J.; Dreyfuss, P.; Aprill, C.N.; Bogduk, N. Paraplegia following image-guided transforaminal lumbar spine epidural steroid injection: Two case reports. Pain Med. 2009, 10, 1389–1394. [Google Scholar] [CrossRef] [PubMed]
- Lyders, E.M.; Morris, P.P. A case of spinal cord infarction following lumbar transforaminal epidural steroid injection: MR imaging and angiographic findings. AJNR Am. J. Neuroradiol. 2009, 30, 1691–1693. [Google Scholar] [CrossRef]
- Murthy, N.S.; Maus, T.P.; Behrns, C.L. Intraforaminal location of the great anterior radiculomedullary artery (artery of Adamkiewicz): A retrospective review. Pain Med. 2010, 11, 1756–1764. [Google Scholar] [CrossRef]
- Kambin, P.; Sampson, S. Posterolateral percutaneous suction-excision of herniated lumbar intervertebral discs. Report of interim results. Clin. Orthop. Relat. Res. 1986, 37–43. [Google Scholar]
- Atluri, S.; Glaser, S.E.; Shah, R.V.; Sudarshan, G. Needle position analysis in cases of paralysis from transforaminal epidurals: consider alternative approaches to traditional technique. Pain Physician 2013, 16, 321–334. [Google Scholar]
- Park, C.H.; Lee, S.H.; Park, H.S. Lumbar retrodiscal versus post-ganglionic transforaminal epidural steroid injection for the treatment of lumbar intervertebral disc herniations. Pain Physician 2011, 14, 353–360. [Google Scholar]
- Park, K.D.; Lee, J.; Jee, H.; Park, Y. Kambin triangle versus the supraneural approach for the treatment of lumbar radicular pain. Am. J. Phys. Med. Rehabil. 2012, 91, 1039–1050. [Google Scholar] [CrossRef]
- Min, J.H.; Kang, S.H.; Lee, J.B.; Cho, T.H.; Suh, J.G. Anatomic analysis of the transforaminal ligament in the lumbar intervertebral foramen. Neurosurgery 2005, 57, 37–41. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Safe-Triangle-Approach Group (n = 12) | Kambin’s-Triangle-Approach Group (n = 12) |
|---|---|---|
| Age (years) | 65.3 ± 21.7 | 68.0 ± 15.6 |
| Sex | ||
| Male | 6 (46.1%) | 5 (38.5%) |
| Female | 7 (53.9%) | 8 (61.5%) |
| Height (cm) | 158.6 ± 14.4 | 160.6 ± 8.1 |
| Weight (kg) | 64.3 ± 16.5 | 62.6 ± 12.5 |
| Body mass index (kg/m2) | 25.2 ± 3.1 | 24.1 ± 3.6 |
| Pain duration (years) | 4.7 ± 4.6 | 10.1 ± 8.3 |
| Target root | ||
| Right L5 | 5 (38.5%) | 9 (69.2%) |
| Left L5 | 8 (61.5%) | 4 (30.8%) |
| Approach | Success | Failure | Total | Success Rate | p-Value | |
|---|---|---|---|---|---|---|
| B1 | D2 | F3 | B/(B + D + F) × 100 | |||
| Safe triangle | 10 | 1 | 2 | 13 | 76.92% | |
| Kambin’s triangle | 12 | 1 | 0 | 13 | 92.31% | |
| Total | 22 | 2 | 2 | 26 | 0.593 * | |
| Variables | Approach | Before Procedure | One Month After | Three Months After |
|---|---|---|---|---|
| Numerical Rating Scale | Safe triangle | 6.0 ± 2.05 | 4.9 ± 2.02 | 4.0 ± 2.11 * |
| Kambin’s triangle | 5.3 ± 1.89 | 4.5 ± 2.12 | 4.0 ± 2.58 * | |
| Oswestry Disability Index | Safe triangle | 17.3 ± 6.48 | 12.6 ± 5.50 | 11.2 ± 4.92 * |
| Kambin’s triangle | 18.7 ± 8.38 | 18.1 ± 9.83 | 13.6 ± 7.37 * |
| Variables | Coefficient | Standard Error | p-Value | |
|---|---|---|---|---|
| NRS | Time | |||
| Before | Reference | |||
| One Month After (a) | −1.1 | 0.56 | 0.051 | |
| Three Months After (b) | −2 | 0.56 | <0.001* | |
| Group | ||||
| Safe Triangle (1) | Reference | |||
| Kambin’s Triangle (2) | −0.7 | 0.91 | 0.441 | |
| Time × Group | ||||
| a 2 | 0.3 | 0.80 | 0.706 | |
| b 2 | 0.7 | 0.80 | 0.379 | |
| ODI | Time | |||
| Before | Reference | |||
| One Month After (a) | −4.7 | 1.10 | <0.001* | |
| Three Months After (b) | −6.1 | 1.10 | <0.001* | |
| Group | ||||
| Safe Triangle (1) | Reference | |||
| Kambin’s Triangle (2) | 1.4 | 3.09 | 0.650 | |
| Time × Group | ||||
| a 2 | 4.1 | 1.56 | 0.009* | |
| b 2 | 1 | 1.56 | 0.521 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil, H.Y.; Jeong, S.; Cho, H.; Choi, E.; Nahm, F.S.; Lee, P.-B. Kambin’s Triangle Approach versus Traditional Safe Triangle Approach for Percutaneous Transforaminal Epidural Adhesiolysis Using an Inflatable Balloon Catheter: A Pilot Study. J. Clin. Med. 2019, 8, 1996. https://doi.org/10.3390/jcm8111996
Gil HY, Jeong S, Cho H, Choi E, Nahm FS, Lee P-B. Kambin’s Triangle Approach versus Traditional Safe Triangle Approach for Percutaneous Transforaminal Epidural Adhesiolysis Using an Inflatable Balloon Catheter: A Pilot Study. Journal of Clinical Medicine. 2019; 8(11):1996. https://doi.org/10.3390/jcm8111996
Chicago/Turabian StyleGil, Ho Young, Sangmin Jeong, Hyunwook Cho, Eunjoo Choi, Francis Sahngun Nahm, and Pyung-Bok Lee. 2019. "Kambin’s Triangle Approach versus Traditional Safe Triangle Approach for Percutaneous Transforaminal Epidural Adhesiolysis Using an Inflatable Balloon Catheter: A Pilot Study" Journal of Clinical Medicine 8, no. 11: 1996. https://doi.org/10.3390/jcm8111996
APA StyleGil, H. Y., Jeong, S., Cho, H., Choi, E., Nahm, F. S., & Lee, P.-B. (2019). Kambin’s Triangle Approach versus Traditional Safe Triangle Approach for Percutaneous Transforaminal Epidural Adhesiolysis Using an Inflatable Balloon Catheter: A Pilot Study. Journal of Clinical Medicine, 8(11), 1996. https://doi.org/10.3390/jcm8111996