Urinary Excretion of N1-Methylnicotinamide, as a Biomarker of Niacin Status, and Mortality in Renal Transplant Recipients

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Assessment of N1-MN Excretion
2.4. Clinical Endpoints
2.5. Statistical Analysis
3. Results
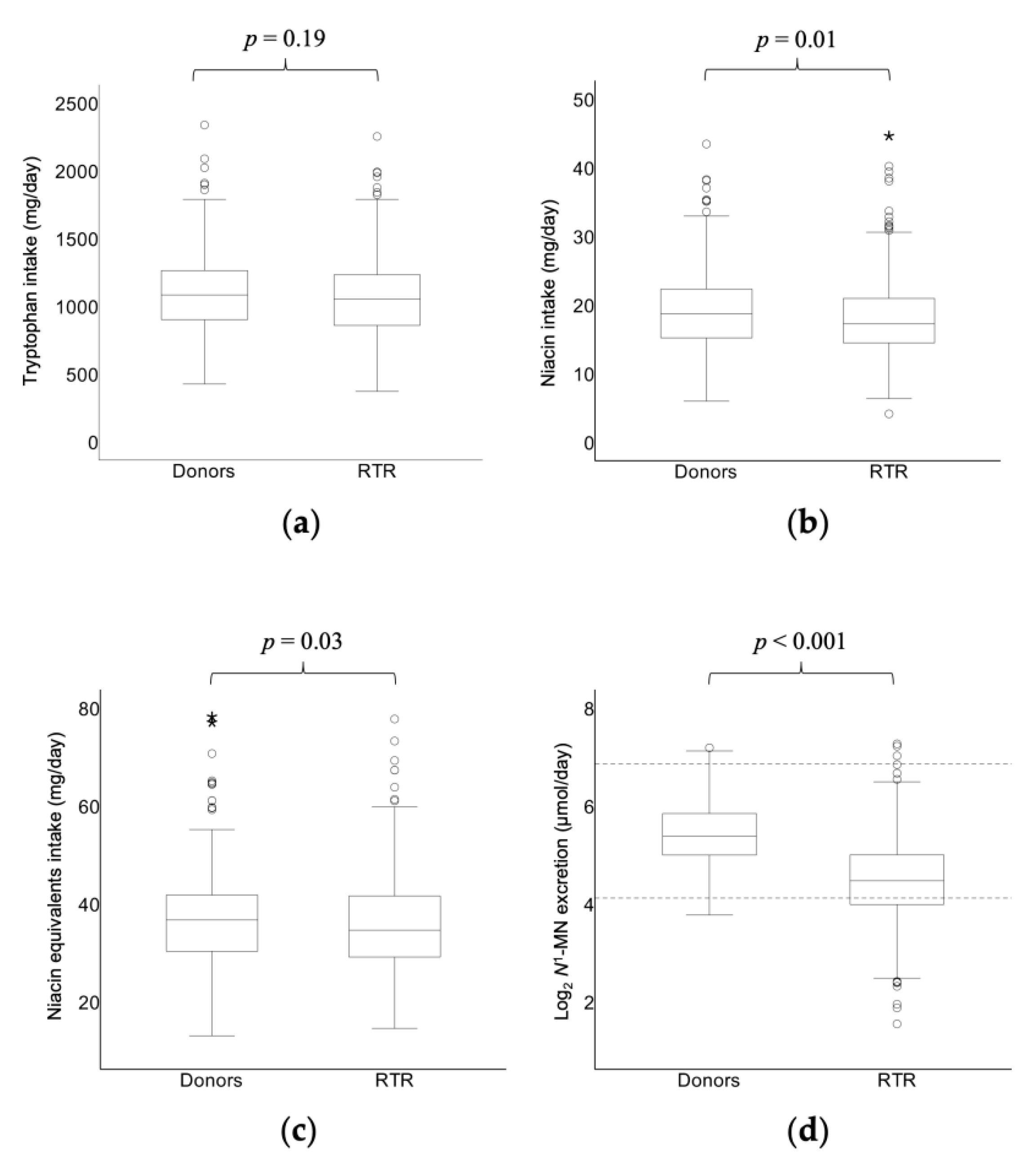
3.1. Baseline Characteristics and Comparison of N1-MN Excretion
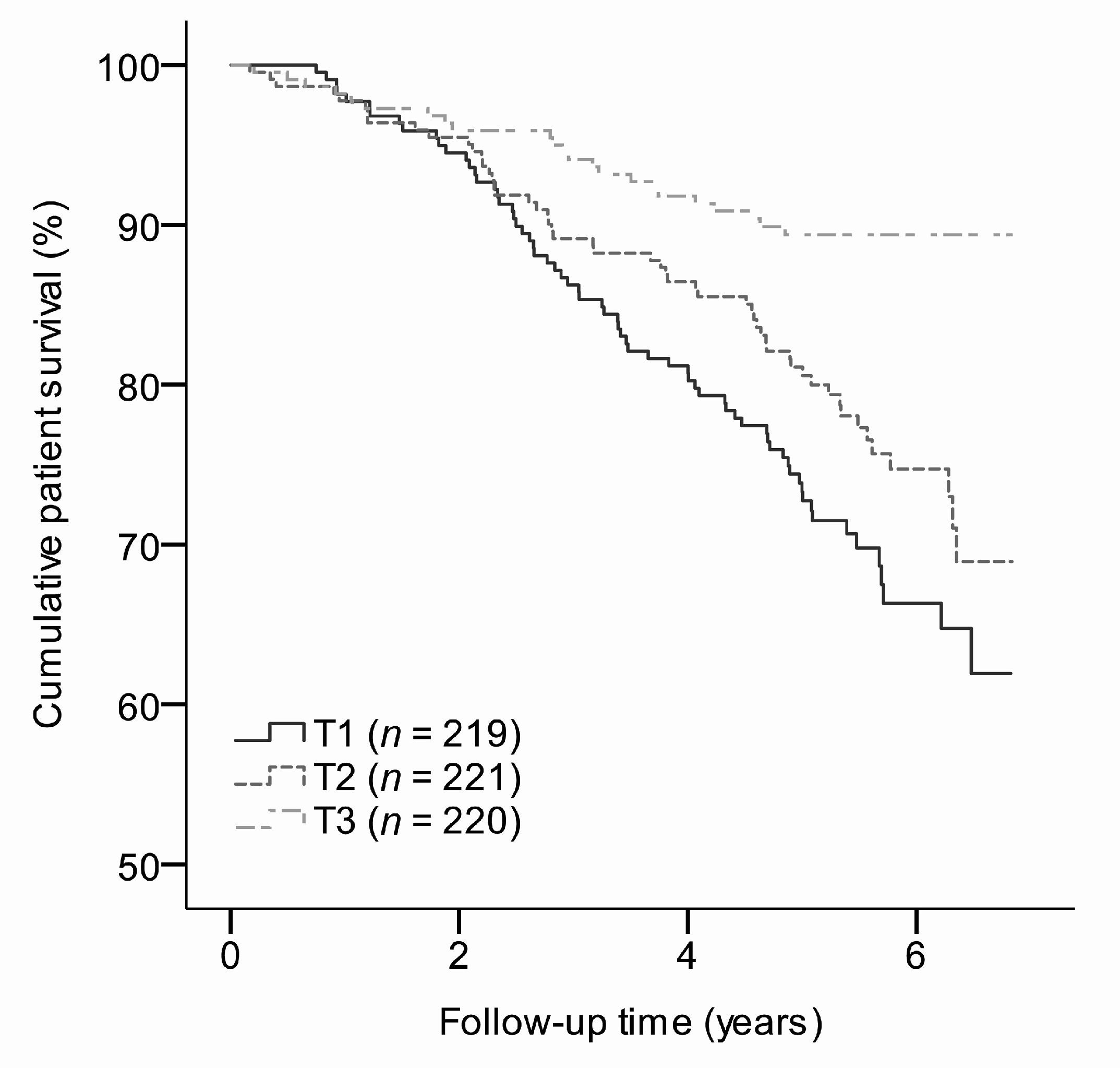
3.2. N1-MN Excretion and Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Garcia, G.G.; Harden, P.; Chapman, J.; World Kidney Day Steering Committee 2012. The Global Role of Kidney Transplantation. Nephrol. Dial. Transplant. 2013, 28, e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Nerini, E.; Bruno, F.; Citterio, F.; Schena, F.P. Nonadherence to Immunosuppressive Therapy in Kidney Transplant Recipients: Can Technology Help? J. Nephrol. 2016, 29, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Nankivell, B.J.; Kuypers, D.R. Diagnosis and Prevention of Chronic Kidney Allograft Loss. Lancet 2011, 378, 1428–1437. [Google Scholar] [CrossRef]
- Tong, A.; Budde, K.; Gill, J.; Josephson, M.A.; Marson, L.; Pruett, T.L.; Reese, P.P.; Rosenbloom, D.; Rostaing, L.; Warrens, A.N.; et al. Standardized Outcomes in Nephrology-Transplantation: A Global Initiative to Develop a Core Outcome Set for Trials in Kidney Transplantation. Transplant. Direct 2016, 2, e79. [Google Scholar] [CrossRef] [PubMed]
- Neuberger, J.M.; Bechstein, W.O.; Kuypers, D.R.; Burra, P.; Citterio, F.; De Geest, S.; Duvoux, C.; Jardine, A.G.; Kamar, N.; Kramer, B.K.; et al. Practical Recommendations for Long-Term Management of Modifiable Risks in Kidney and Liver Transplant Recipients: A Guidance Report and Clinical Checklist by the Consensus on Managing Modifiable Risk in Transplantation (COMMIT) Group. Transplantation 2017, 101, S1–S56. [Google Scholar] [CrossRef] [PubMed]
- Eisenga, M.F.; Kieneker, L.M.; Soedamah-Muthu, S.S.; van den Berg, E.; Deetman, P.E.; Navis, G.J.; Gans, R.O.; Gaillard, C.A.; Bakker, S.J.; Joosten, M.M. Urinary Potassium Excretion, Renal Ammoniagenesis, and Risk of Graft Failure and Mortality in Renal Transplant Recipients. Am. J. Clin. Nutr. 2016, 104, 1703–1711. [Google Scholar] [CrossRef] [PubMed]
- Sotomayor, C.G.; Gomes-Neto, A.W.; Eisenga, M.F.; Nolte, I.M.; Anderson, J.L.C.; de Borst, M.H.; Oste, M.C.J.; Rodrigo, R.; Gans, R.O.B.; Berger, S.P.; et al. Consumption of Fruits and Vegetables and Cardiovascular Mortality in Renal Transplant Recipients: A Prospective Cohort Study. Nephrol. Dial. Transplant. 2018, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Minovic, I.; van der Veen, A.; van Faassen, M.; Riphagen, I.J.; van den Berg, E.; van der Ley, C.; Gomes-Neto, A.W.; Geleijnse, J.M.; Eggersdorfer, M.; Navis, G.J.; et al. Functional Vitamin B-6 Status and Long-Term Mortality in Renal Transplant Recipients. Am. J. Clin. Nutr. 2017, 106, 1366–1374. [Google Scholar] [CrossRef] [PubMed]
- Combs, G.F.; McClungh, J.P. Vitamin B6. In The Vitamins, 5th ed.; Academic Press: Cambridge, MA, USA, 2017; pp. 350–371. [Google Scholar]
- Fukuwatari, T.; Shibata, K. Nutritional Aspect of Tryptophan Metabolism. Int. J. Tryptophan Res. 2013, 6, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Bogan, K.L.; Brenner, C. Nicotinic Acid, Nicotinamide, and Nicotinamide Riboside: A Molecular Evaluation of NAD+ Precursor Vitamins in Human Nutrition. Annu. Rev. Nutr. 2008, 28, 115–130. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization and United Nations High Commissions for Refugees. Pellagra and Its Prevention and Control in Major Emergencies; WHO/NHD/00.10.2000; Available online: https://www.who.int/nutrition/publications/emergencies/WHO_NHD_00.10/en/ (accessed on 26 March 2018).
- Menon, R.M.; Gonzalez, M.A.; Adams, M.H.; Tolbert, D.S.; Leu, J.H.; Cefali, E.A. Effect of the Rate of Niacin Administration on the Plasma and Urine Pharmacokinetics of Niacin and its Metabolites. J. Clin. Pharmacol. 2007, 47, 681–688. [Google Scholar] [CrossRef] [PubMed]
- EFSA NDA Panel. Scientific Opinion on Dietary Reference Values for Niacin. EFSA J. 2014, 12, 3759. [Google Scholar] [CrossRef]
- Van den Berg, E.; Engberink, M.F.; Brink, E.J.; van Baak, M.A.; Joosten, M.M.; Gans, R.O.; Navis, G.; Bakker, S.J. Dietary Acid Load and Metabolic Acidosis in Renal Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 1811–1818. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, E.; Engberink, M.F.; Brink, E.J.; van Baak, M.A.; Gans, R.O.; Navis, G.; Bakker, S.J. Dietary Protein, Blood Pressure and Renal Function in Renal Transplant Recipients. Br. J. Nutr. 2013, 109, 1463–1470. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, E.; Pasch, A.; Westendorp, W.H.; Navis, G.; Brink, E.J.; Gans, R.O.; van Goor, H.; Bakker, S.J. Urinary Sulfur Metabolites Associate with a Favorable Cardiovascular Risk Profile and Survival Benefit in Renal Transplant Recipients. J. Am. Soc. Nephrol. 2014, 25, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating Glomerular Filtration Rate from Serum Creatinine and Cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Salvador, C.L.; Hartmann, A.; Asberg, A.; Bergan, S.; Rowe, A.D.; Morkrid, L. Estimating Glomerular Filtration Rate in Kidney Transplant Recipients: Comparing a Novel Equation with Commonly used Equations in this Population. Transplant. Direct 2017, 3, e332. [Google Scholar] [CrossRef] [PubMed]
- Feunekes, G.I.; Van Staveren, W.A.; De Vries, J.H.; Burema, J.; Hautvast, J.G. Relative and Biomarker-Based Validity of a Food-Frequency Questionnaire Estimating Intake of Fats and Cholesterol. Am. J. Clin. Nutr. 1993, 58, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Feunekes, I.J.; Van Staveren, W.A.; Graveland, F.; De Vos, J.; Burema, J. Reproducibility of a Semiquantitative Food Frequency Questionnaire to Assess the Intake of Fats and Cholesterol in the Netherlands. Int. J. Food Sci. Nutr. 1995, 46, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Verkleij-Hagoort, A.C.; de Vries, J.H.; Ursem, N.T.; de Jonge, R.; Hop, W.C.; Steegers-Theunissen, R.P. Dietary Intake of B-Vitamins in Mothers Born a Child with a Congenital Heart Defect. Eur. J. Nutr. 2006, 45, 478–486. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dutch Nutrient Databank. NEVO Table 2006; Voorlichtingsbureau Voor de Voeding: The Hague, The Netherlands, 2006. [Google Scholar]
- Bouma, G.; van Faassen, M.; Kats-Ugurlu, G.; de Vries, E.G.; Kema, I.P.; Walenkamp, A.M. Niacin (Vitamin B3) Supplementation in Patients with Serotonin-Producing Neuroendocrine Tumor. Neuroendocrinology 2016, 103, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Tamulevicius, P.; Streffer, C. N-Methylnicotinamide as a Possible Prognostic Indicator of Recovery from Leukaemia in Patients Treated with Total-Body Irradiation and Bone Marrow Transplants. Strahlentherapie 1984, 160, 249–254. [Google Scholar] [PubMed]
- Canner, P.L.; Berge, K.G.; Wenger, N.K.; Stamler, J.; Friedman, L.; Prineas, R.J.; Friedewald, W. Fifteen Year Mortality in Coronary Drug Project Patients: Long-Term Benefit with Niacin. J. Am. Coll. Cardiol. 1986, 8, 1245–1255. [Google Scholar] [CrossRef]
- Qiao, Y.L.; Dawsey, S.M.; Kamangar, F.; Fan, J.H.; Abnet, C.C.; Sun, X.D.; Johnson, L.L.; Gail, M.H.; Dong, Z.W.; Yu, B.; et al. Total and Cancer Mortality After Supplementation with Vitamins and Minerals: Follow-Up of the Linxian General Population Nutrition Intervention Trial. J. Natl. Cancer Inst. 2009, 101, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Duggal, J.K.; Singh, M.; Attri, N.; Singh, P.P.; Ahmed, N.; Pahwa, S.; Molnar, J.; Singh, S.; Khosla, S.; Arora, R. Effect of Niacin Therapy on Cardiovascular Outcomes in Patients with Coronary Artery Disease. J. Cardiovasc. Pharmacol. Ther. 2010, 15, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Schandelmaier, S.; Briel, M.; Saccilotto, R.; Olu, K.K.; Arpagaus, A.; Hemkens, L.G.; Nordmann, A.J. Niacin for Primary and Secondary Prevention of Cardiovascular Events. Cochrane Database Syst. Rev. 2017, 6, CD009744. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Lee, M.S.; Wahlqvist, M.L. Prediction of all-Cause Mortality by B Group Vitamin Status in the Elderly. Clin. Nutr. 2012, 31, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Troesch, B.; Hoeft, B.; McBurney, M.; Eggersdorfer, M.; Weber, P. Dietary Surveys Indicate Vitamin Intakes below Recommendations are Common in Representative Western Countries. Br. J. Nutr. 2012, 108, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Hegyi, J.; Schwartz, R.A.; Hegyi, V. Pellagra: Dermatitis, Dementia, and Diarrhea. Int. J. Dermatol. 2004, 43, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Yu, K.; Wang, Q.; Wang, L.; Mao, J.; Qian, J. Pellagra Secondary to Medication and Alcoholism: A Case Report and Review of the Literature. Nutr. Clin. Pract. 2016, 31, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Muller, F.; Sharma, A.; Konig, J.; Fromm, M.F. Biomarkers for in Vivo Assessment of Transporter Function. Pharmacol. Rev. 2018, 70, 246–277. [Google Scholar] [CrossRef] [PubMed]
- Badawy, A.A. Kynurenine Pathway of Tryptophan Metabolism: Regulatory and Functional Aspects. Int. J. Tryptophan Res. 2017, 10, 1178646917691938. [Google Scholar] [CrossRef] [PubMed]
- Bender, D.A.; Magboul, B.I.; Wynick, D. Probable Mechanisms of Regulation of the Utilization of Dietary Tryptophan, Nicotinamide and Nicotinic Acid as Precursors of Nicotinamide Nucleotides in the Rat. Br. J. Nutr. 1982, 48, 119–127. [Google Scholar] [CrossRef] [PubMed]
- McCreanor, G.M.; Bender, D.A. The Metabolism of High Intakes of Tryptophan, Nicotinamide and Nicotinic Acid in the Rat. Br. J. Nutr. 1986, 56, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.N., Jr.; Feigelson, P.; Elvehjem, C.A. Relation of Tryptophan and Niacin to Pyridine Nucleotides of Tissue. J. Biol. Chem. 1950, 187, 597–604. [Google Scholar] [PubMed]
- Kirkland, J.B. Niacin Status, NAD Distribution and ADP-Ribose Metabolism. Curr. Pharm. Des. 2009, 15, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Shibata, K.; Matsuo, H. Effect of Dietary Tryptophan Levels on the Urinary Excretion of Nicotinamide and its Metabolites in Rats Fed a Niacin-Free Diet Or a Constant Total Protein Level. J. Nutr. 1990, 120, 1191–1197. [Google Scholar] [CrossRef] [PubMed]
- Teplan, V.; Valkovsky, I.; Teplan, V., Jr.; Stollova, M.; Vyhnanek, F.; Andel, M. Nutritional Consequences of Renal Transplantation. J. Ren. Nutr. 2009, 19, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Ter Wee, P.M. Protein Energy Wasting and Transplantation. J. Ren. Nutr. 2013, 23, 246–249. [Google Scholar] [CrossRef] [PubMed]
- Nasseri, K.; Daley-Yates, P.T. A Comparison of N-1-Methylnicotinamide Clearance with 5 Other Markers of Renal Function in Models of Acute and Chronic Renal Failure. Toxicol. Lett. 1990, 53, 243–245. [Google Scholar] [CrossRef]
- Maiza, A.; Daley-Yates, P.T. Estimation of the Renal Clearance of Drugs using Endogenous N-1-Methylnicotinamide. Toxicol. Lett. 1990, 53, 231–235. [Google Scholar] [CrossRef]
- Maiza, A.; Waldek, S.; Ballardie, F.W.; Daley-Yates, P.T. Estimation of Renal Tubular Secretion in Man, in Health and Disease, using Endogenous N-1-Methylnicotinamide. Nephron 1992, 60, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Sauve, A.A. NAD (+) Metabolism: Bioenergetics, Signaling and Manipulation for Therapy. Biochim. Biophys. Acta 2016, 1864, 1787–1800. [Google Scholar] [CrossRef] [PubMed]
- Stein, L.R.; Imai, S. The Dynamic Regulation of NAD Metabolism in Mitochondria. Trends Endocrinol. Metab. 2012, 23, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Chini, C.C.S.; Tarrago, M.G.; Chini, E.N. NAD and the Aging Process: Role in Life, Death and Everything in Between. Mol. Cell. Endocrinol. 2017, 455, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Canto, C.; Menzies, K.J.; Auwerx, J. NAD (+) Metabolism and the Control of Energy Homeostasis: A Balancing Act between Mitochondria and the Nucleus. Cell. Metab. 2015, 22, 31–53. [Google Scholar] [CrossRef] [PubMed]
- Hao, C.M.; Haase, V.H. Sirtuins and their Relevance to the Kidney. J. Am. Soc. Nephrol. 2010, 21, 1620–1627. [Google Scholar] [CrossRef] [PubMed]
- Kitada, M.; Kume, S.; Takeda-Watanabe, A.; Kanasaki, K.; Koya, D. Sirtuins and Renal Diseases: Relationship with Aging and Diabetic Nephropathy. Clin. Sci. 2013, 124, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Wakino, S.; Hasegawa, K.; Itoh, H. Sirtuin and Metabolic Kidney Disease. Kidney Int. 2015, 88, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.J.; Liu, N.; Xiao, Z.; Sun, T.; Wu, S.H.; Sun, W.X.; Xu, Z.G.; Yuan, H. Renal Protective Effect of Sirtuin 1. J. Diabetes Res. 2014, 2014, 843786. [Google Scholar] [CrossRef] [PubMed]
- Naska, A.; Lagiou, A.; Lagiou, P. Dietary Assessment Methods in Epidemiological Research: Current State of the Art and Future Prospects. F1000Research 2017, 6, 926. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Donors n = 275 | RTR n = 660 | p-Value 2 |
|---|---|---|---|
| Age, years | 53.3 ± 10.7 | 53.0 ± 12.7 | 0.68 |
| Male, n (%) | 112 (41) | 379 (57) | 0.001 |
| Body surface area, m2 | 1.9 ± 0.2 | 1.9 ± 0.2 | 0.90 |
| Current smoker, n (%) | 39 (14) | 78 (12) | <0.001 |
| Alcohol intake, g/day | 6.7 (1.1–16.4) | 3.1 (0.1–11.9) | <0.001 |
| Energy intake, kcal/day | 2295 ± 746 | 2182 ± 642 | 0.04 |
| Niacin equivalents intake, mg/day 3 | 37.4 ± 10.8 | 35.6 ± 9.2 | 0.03 |
| Tryptophan intake, mg/day | 1089 ± 308 | 1059 ± 271 | 0.19 |
| Niacin intake, mg/day | 19.2 ± 6.2 | 17.9 ± 5.2 | 0.01 |
| N1-MN excretion, μmol/day | 41.4 (31.6–57.2) | 22.0 (15.8–31.8) | <0.001 |
| <17.3 μmol/day, n (%) | 4 (2) | 202 (31) | 0.03 |
| Plasma vitamin B6 (nmol/L) | 42.0 (29.8–60.3) | 29.0 (17.5–49.5) | <0.001 |
| Systolic blood pressure, mmHg | 125.1 ± 13.9 | 135.8 ± 17.3 | <0.001 |
| Diastolic blood pressure, mmHg | 75.6 ± 9.1 | 82.5 ± 11.0 | <0.001 |
| Triglycerides, mmol/L | 1.2 (0.9–1.7) | 1.7 (1.2–2.3) | <0.001 |
| HbA1c, (%) | 5.6 (5.4–5.8) | 5.8 (5.5–6.2) | <0.001 |
| eGFR, ml/min/1.73 m2 | 91.0 ± 14.2 | 53.0 ± 20.0 | <0.001 |
| Acetylsalicylic acid, n (%) | 4 (2) | 127 (19) | <0.001 |
| Proton pump inhibitor, n (%) | 5 (2) | 326 (49) | <0.001 |
| Diuretic, n (%) | 9 (3) | 261 (40) | <0.001 |
| Variable | Model 1 2 | Model 2 3 | Model 3 4 | Model 4 5 | ||||
|---|---|---|---|---|---|---|---|---|
| Std.β | p-Value | Std.β | p-Value | Std.β | p-Value | Std.β | p-Value | |
| Grouping | −0.42 | <0.001 | −0.44 | <0.001 | −0.25 | <0.001 | −0.21 | <0.001 |
| Sex | - | - | −0.15 | <0.001 | −0.14 | <0.001 | −0.10 | 0.002 |
| Age, years | - | - | −0.16 | <0.001 | −0.11 | <0.001 | −0.07 | 0.02 |
| eGFR, ml/min/1.73 m2 | - | - | - | - | 0.31 | <0.001 | 0.29 | <0.001 |
| Energy intake, kcal/day | - | - | - | - | - | - | −0.10 | 0.08 |
| Tryptophan intake, mg/day | - | - | - | - | - | - | 0.007 | 0.91 |
| Niacin intake, mg/day | - | - | - | - | - | - | 0.25 | <0.001 |
| Plasma vitamin B6, nmol/L | - | - | - | - | - | - | 0.23 | <0.001 |
| R2 | 0.18 | 0.23 | 0.28 | 0.37 | ||||
| Variable | Tertiles of Sex-Stratified N1-MN Excretion | p-Value 2 | ||
|---|---|---|---|---|
| T1 n = 219 | T2 n = 221 | T3 n = 220 | ||
| Males, μmol/day | <19.2 | 19.2–28.8 | >28.8 | |
| Females, μmol/day | <16.1 | 16.1–25.6 | >25.6 | |
| Male, n (%) | 126 (58) | 127 (58) | 126 (57) | - |
| Age, years | 54.6 ± 12.7 | 53.7 ± 13.1 | 50.7 ± 12.1 | 0.004 |
| BMI, kg/m2 | 25.8 (22.7–29.4) | 26.1 (23.3–29.0) | 26.0 (23.6–29.6) | 0.41 |
| Body surface area, m2 | 1.9 ± 0.2 | 1.9 ± 0.2 | 2.0 ± 0.2 | 0.13 |
| Lifestyle | ||||
| Current smoker, n (%) | 21 (10) | 25 (11) | 32 (15) | 0.26 |
| Alcohol consumption, g/day | 0.5 (0.0–7.0) | 3.2 (0.1–11.3) | 6.7 (0.8–20.9) | <0.001 |
| Vegetarian, n (%) | 7 (3) | 2 (1) | 3 (1) | 0.16 |
| Dietary intake | ||||
| Energy, kcal/day | 2065 ± 586 | 2197 ± 675 | 2285 ± 647 | 0.002 |
| Tryptophan, mg/day | 1001 ± 253 | 1063 ± 273 | 1112 ± 274 | <0.001 |
| Niacin, mg/day | 16.6 ± 4.9 | 17.6 ± 4.8 | 19.5 ± 5.5 | <0.001 |
| Plasma vitamin B6, nmol/L | 20.3 (14.0–39.0) | 29.5 (19.0–47.0) | 39.0 (22.0–65.0) | <0.001 |
| Hemodynamic | ||||
| Systolic blood pressure, mmHg | 139 ± 18 | 134 ± 18 | 135 ± 16 | 0.01 |
| Diastolic blood pressure, mmHg | 83 ± 11 | 82 ± 12 | 83 ± 11 | 0.20 |
| Mean arterial pressure, mmHg | 109 ± 15 | 106 ± 15 | 106 ± 14 | 0.07 |
| Heart rate, beats per minute | 69 ± 11 | 68 ± 12 | 68 ± 12 | 0.52 |
| Antihypertensive use, n (%) | 199 (91) | 193 (87) | 189 (86) | 0.26 |
| Lipids | ||||
| Total cholesterol, mmol/L | 5.1 ± 1.2 | 5.2 ± 1.1 | 5.0 ± 1.1 | 0.36 |
| HDL, mmol/L | 1.3 (1.0–1.6) | 1.3 (1.1–1.6) | 1.3 (1.1–1.7) | 0.06 |
| LDL, mmol/L | 3.0 ± 0.9 | 3.1 ± 0.9 | 2.9 ± 0.9 | 0.31 |
| Triglycerides, mmol/L | 1.7 (1.3–2.3) | 1.7 (1.3–2.3) | 1.6 (1.1–2.2) | 0.03 |
| Statin, n (%) | 122 (56) | 115 (52) | 112 (51) | 0.55 |
| Glucose homeostasis | ||||
| Glucose, mmol/L | 5.3 (4.8–6.0) | 5.3 (4.8–5.9) | 5.2 (4.7–6.2) | 0.58 |
| HbA1c, (%) | 5.8 (5.5–6.3) | 5.9 (5.6–6.1) | 5.7 (5.4–6.1) | 0.05 |
| Diabetes, n (%) | 58 (27) | 44 (20) | 50 (23) | 0.26 |
| Antidiabetic, n (%) | 41 (19) | 28 (13) | 27 (12) | 0.10 |
| Other serum parameters | ||||
| Hs-CRP, mg/L | 1.7 (0.8–5.3) | 1.6 (0.6–3.8) | 1.4 (0.7–4.6) | 0.42 |
| Phosphate, mmol/L | 1.0 ± 0.2 | 1.0 ± 0.2 | 0.9 ± 0.2 | 0.01 |
| Immunosuppressant medication | ||||
| Prednisolon dose, mg/day | 10 (7.5–10) | 10 (7.5–10) | 10 (7.5–10) | 0.18 |
| Calcineurin inhibitor, n (%) | 136 (62) | 125 (57) | 112 (51) | 0.06 |
| Cyclosporine, n (%) | 87 (40) | 82 (37) | 84 (38) | 0.85 |
| Azathioprine, n (%) | 35 (16) | 36 (16) | 41 (19) | 0.72 |
| Proliferation inhibitor, n (%) | 171 (78) | 186 (84) | 191 (87) | 0.04 |
| Other medication | ||||
| Acetylsalicylic acid, n (%) | 55 (25) | 47 (21) | 25 (11) | 0.001 |
| Anticonvulsant, n (%) | 7 (3) | 5 (2) | 7 (3) | 0.80 |
| Proton pump inhibitor, n (%) | 127 (58) | 107 (48) | 92 (42) | 0.003 |
| Diuretic, n (%) | 104 (48) | 79 (36) | 78 (36) | 0.01 |
| Kidney function | ||||
| Serum creatinine, μmol/L | 138 (104–189) | 122 (101–153) | 114 (94–140) | <0.001 |
| Cystatin C, mg/L | 2.0 (1.4–2.8) | 1.6 (1.3–2.1) | 1.4 (1.2–1.9) | <0.001 |
| eGFR, ml/min/1.73 m2 | 39.0 ± 18.7 | 45.8 ± 16.9 | 52.7 ± 18.0 | <0.001 |
| Proteinuria ≥ 0.5 g/day, n (%) | 55 (25) | 39 (18) | 38 (17) | 0.07 |
| Kidney transplantation | ||||
| Time since transplantation, years | 5.6 (1.7–12.9) | 5.0 (1.5–11.0) | 6.5 (2.9–12.3) | 0.16 |
| Donor | ||||
| Age, years | 46 (33–54) | 47 (29–57) | 43 (29–53) | 0.22 |
| Male, n (%) | 104 (48) | 110 (50) | 112 (51) | 0.60 |
| Post mortem status, n (%) | 161 (74) | 143 (65) | 121 (55) | <0.001 |
| Primary kidney disease | ||||
| Primary glomerular disease, n (%) | 48 (22) | 67 (30) | 71 (32) | 0.04 |
| Glomerulonephritis, n (%) | 12 (6) | 17 (8) | 21 (10) | 0.27 |
| Tubulointerstitial disease, n (%) | 27 (12) | 30 (14) | 20 (9) | 0.32 |
| Polycystic renal disease, n (%) | 52 (24) | 45 (20) | 40 (18) | 0.35 |
| Dysplasia and hypoplasia, n (%) | 9 (4) | 10 (5) | 9 (4) | 0.97 |
| Renovascular disease, n (%) | 17 (8) | 8 (4) | 11 (5) | 0.15 |
| Diabetic nephropathy, n (%) | 15 (7) | 7 (3) | 13 (6) | 0.20 |
| Other or unknown cause, n (%) | 39 (18) | 36 (16) | 35 (16) | 0.85 |
| Model | N1-MN Excretion (log2) As Continuous Variable n = 660 | Tertiles of Sex-Stratified N1-MN Excretion 2 | |||||
|---|---|---|---|---|---|---|---|
| T1 n = 219 | T2 n = 221 | T3 n = 220 | |||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | Reference HR | |
| 1 3 | 0.53 (0.43–0.65) | <0.001 | 3.28 (2.04–5.26) | <0.001 | 2.41 (1.48–3.93) | <0.001 | 1.00 |
| 2 4 | 0.57 (0.45–0.71) | <0.001 | 2.68 (1.67–4.33) | <0.001 | 2.04 (1.25–3.34) | 0.004 | 1.00 |
| 3 5 | 0.59 (0.47–0.74) | <0.001 | 2.65 (1.60–4.39) | <0.001 | 2.10 (1.25–3.52) | 0.005 | 1.00 |
| 4 6 | 0.69 (0.53–0.90) | 0.005 | 2.10 (1.17–3.78) | 0.01 | 2.04 (1.15–3.63 | 0.02 | 1.00 |
| 5 7 | 0.75 (0.58–0.96) | 0.02 | 1.86 (1.07–3.25) | 0.02 | 1.80 (1.04–3.13) | 0.04 | 1.00 |
| 6 8 | 0.65 (0.51–0.82) | <0.001 | 2.25 (1.35–3.75) | 0.002 | 2.06 (1.23–3.46) | 0.006 | 1.00 |
| 7 9 | 0.60 (0.48–0.76) | <0.001 | 2.59 (1.54–4.35) | <0.001 | 2.13 (1.26–3.61) | 0.005 | 1.00 |
| Events (n) | 143 | 67 | 53 | 23 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deen, C.P.J.; van der Veen, A.; van Faassen, M.; Minović, I.; Gomes-Neto, A.W.; Geleijnse, J.M.; Borgonjen-van den Berg, K.J.; Kema, I.P.; Bakker, S.J.L. Urinary Excretion of N1-Methylnicotinamide, as a Biomarker of Niacin Status, and Mortality in Renal Transplant Recipients. J. Clin. Med. 2019, 8, 1948. https://doi.org/10.3390/jcm8111948
Deen CPJ, van der Veen A, van Faassen M, Minović I, Gomes-Neto AW, Geleijnse JM, Borgonjen-van den Berg KJ, Kema IP, Bakker SJL. Urinary Excretion of N1-Methylnicotinamide, as a Biomarker of Niacin Status, and Mortality in Renal Transplant Recipients. Journal of Clinical Medicine. 2019; 8(11):1948. https://doi.org/10.3390/jcm8111948
Chicago/Turabian StyleDeen, Carolien P.J., Anna van der Veen, Martijn van Faassen, Isidor Minović, António W. Gomes-Neto, Johanna M. Geleijnse, Karin J. Borgonjen-van den Berg, Ido P. Kema, and Stephan J.L. Bakker. 2019. "Urinary Excretion of N1-Methylnicotinamide, as a Biomarker of Niacin Status, and Mortality in Renal Transplant Recipients" Journal of Clinical Medicine 8, no. 11: 1948. https://doi.org/10.3390/jcm8111948
APA StyleDeen, C. P. J., van der Veen, A., van Faassen, M., Minović, I., Gomes-Neto, A. W., Geleijnse, J. M., Borgonjen-van den Berg, K. J., Kema, I. P., & Bakker, S. J. L. (2019). Urinary Excretion of N1-Methylnicotinamide, as a Biomarker of Niacin Status, and Mortality in Renal Transplant Recipients. Journal of Clinical Medicine, 8(11), 1948. https://doi.org/10.3390/jcm8111948