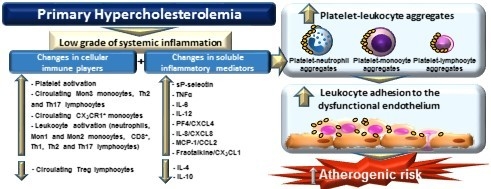
Novel Immune Features of the Systemic Inflammation Associated with Primary Hypercholesterolemia: Changes in Cytokine/Chemokine Profile, Increased Platelet and Leukocyte Activation

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Cell culture
2.2. Human Study Populations
2.3. Flow Cytometry
2.4. Quantification of Soluble Metabolic and Inflammatory Markers
2.5. Leukocyte-Endothelial Cell Interactions under Flow Conditions
2.6. Immunofluorescence Studies
2.7. Statistical Analysis
3. Results
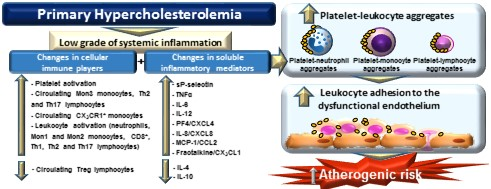
3.1. Platelet Activation Is Enhanced in Patients with PH
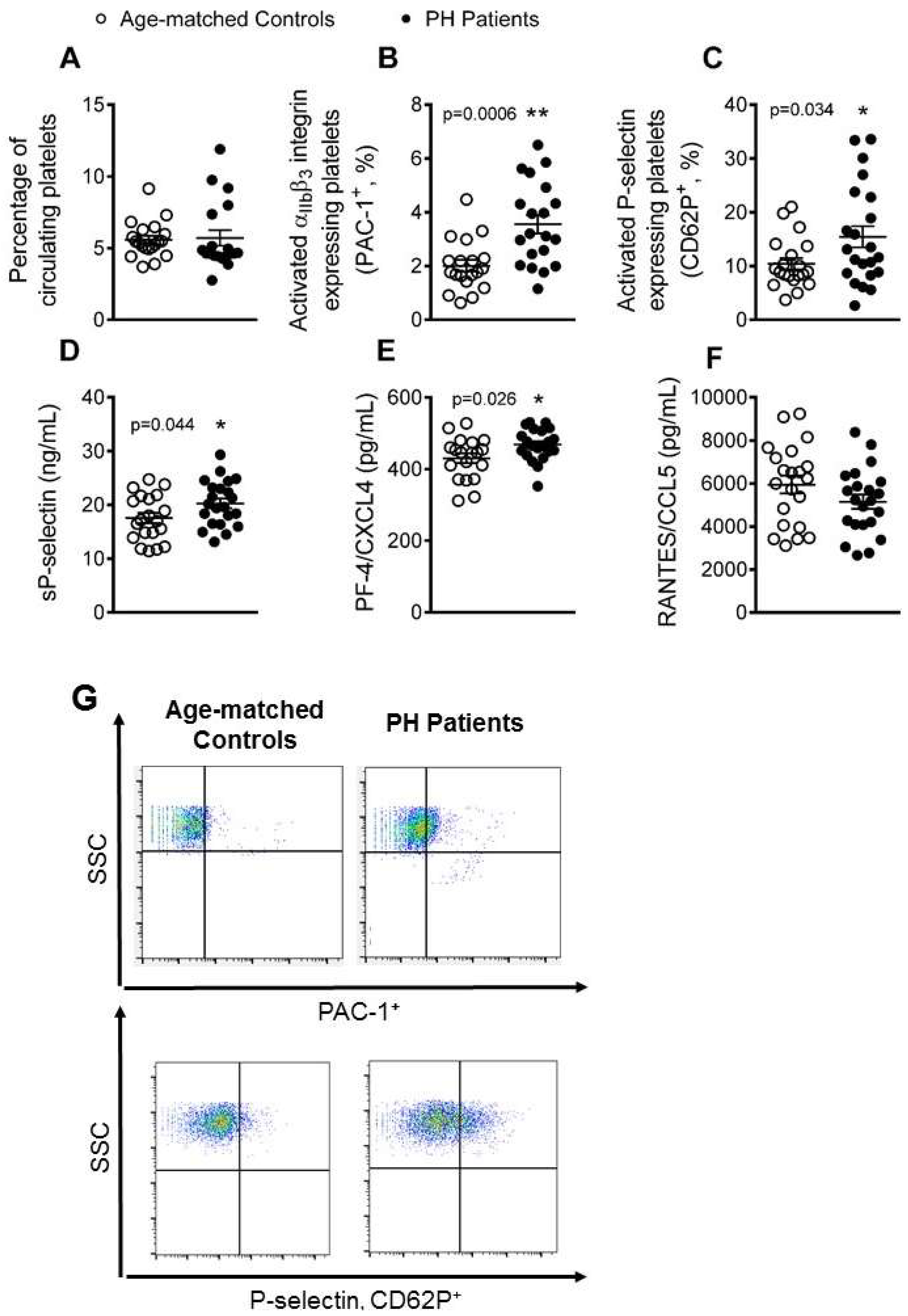
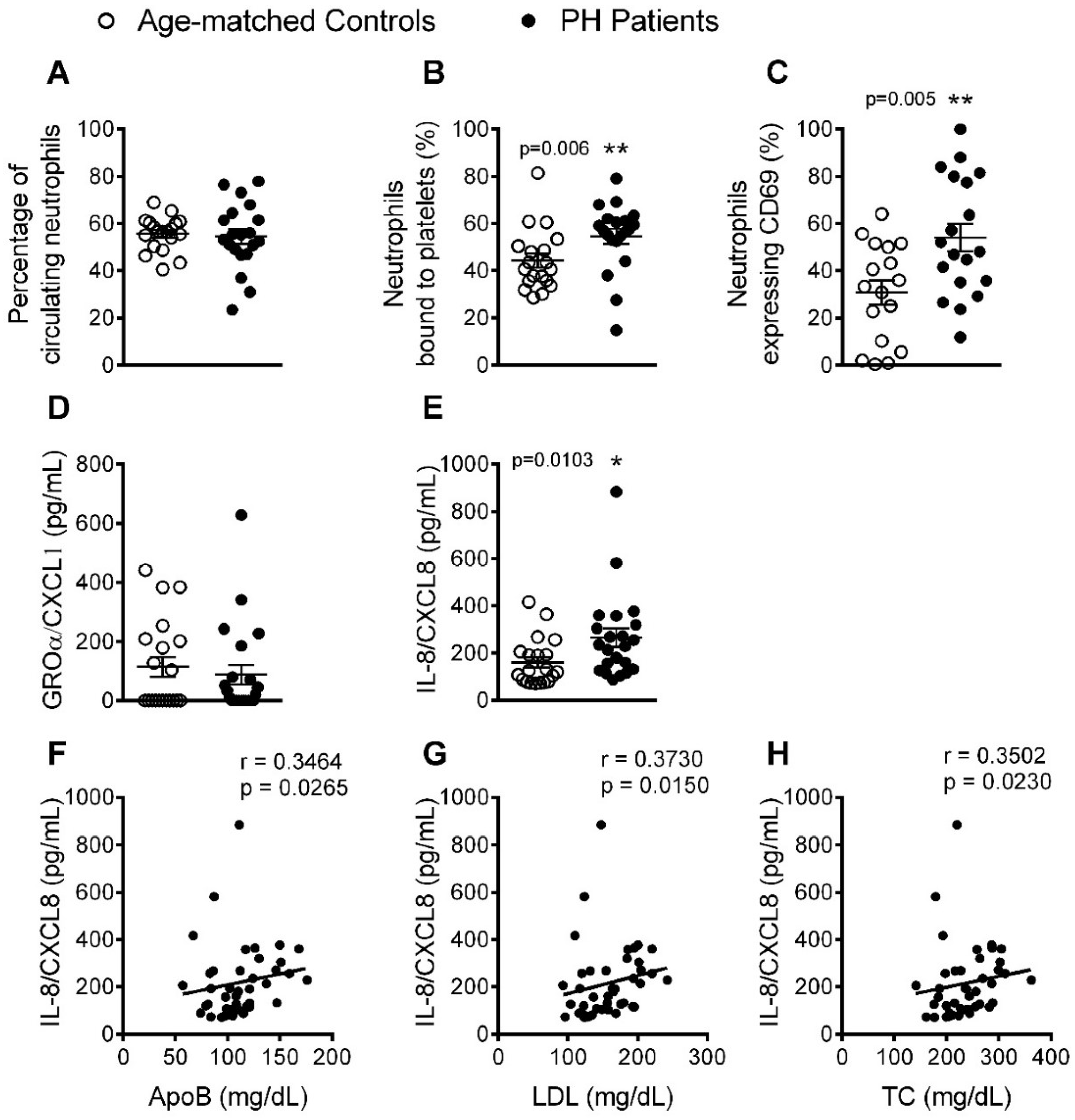
3.2. The Percentage of Platelet-Neutrophil Aggregates, Activated Neutrophils, and Circulating Levels of IL-8, Are Elevated in Patients with PH
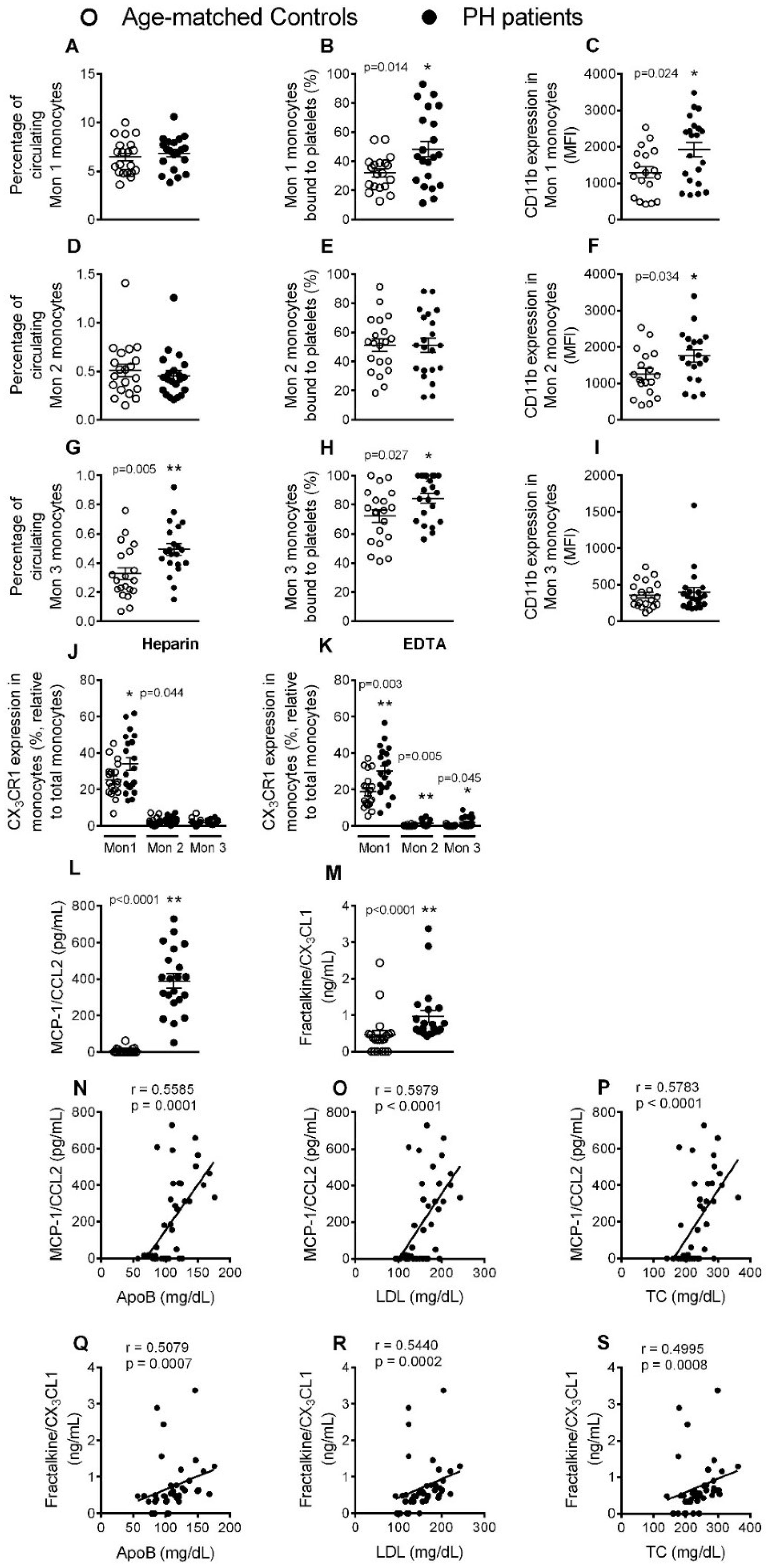
3.3. Circulating Mon 3 Monocytes, Platelet-Mon 1 and 3 Aggregates, Activated Mon 1 and 2 Monocytes, and Plasma Levels of CCL2 and CX3CL1, Are All Elevated in Patients with PH
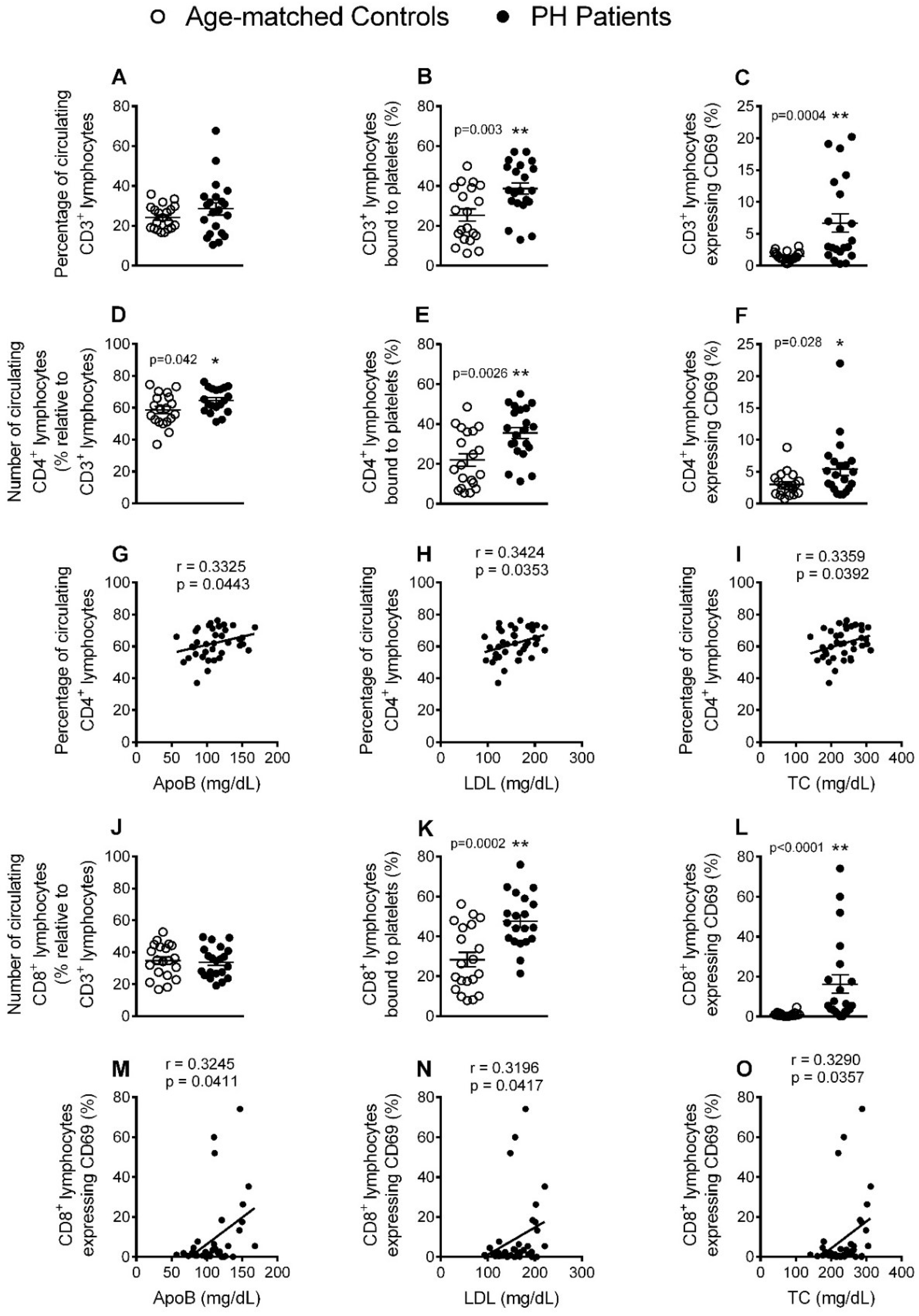
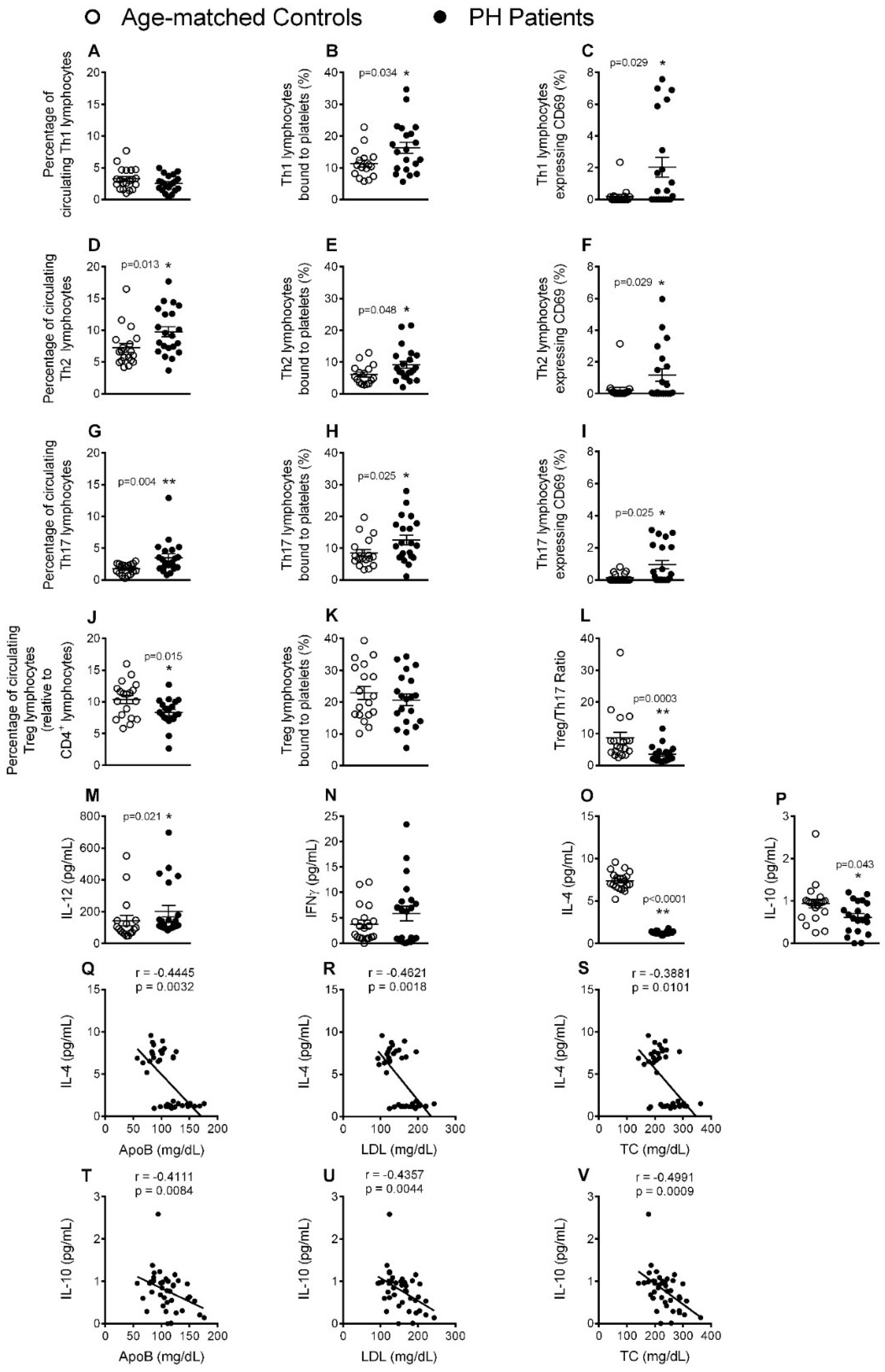
3.4. Circulating CD4+ Lymphocytes, Platelet-Lymphocyte (CD4+ and CD8+) Aggregates and Lymphocyte (CD4+ and CD8+) Activation Are Significantly increased in Patients with PH
3.5. Circulating Levels of Pro-Inflammatory Cytokines but not Adipokines Are Increased in PH Patients
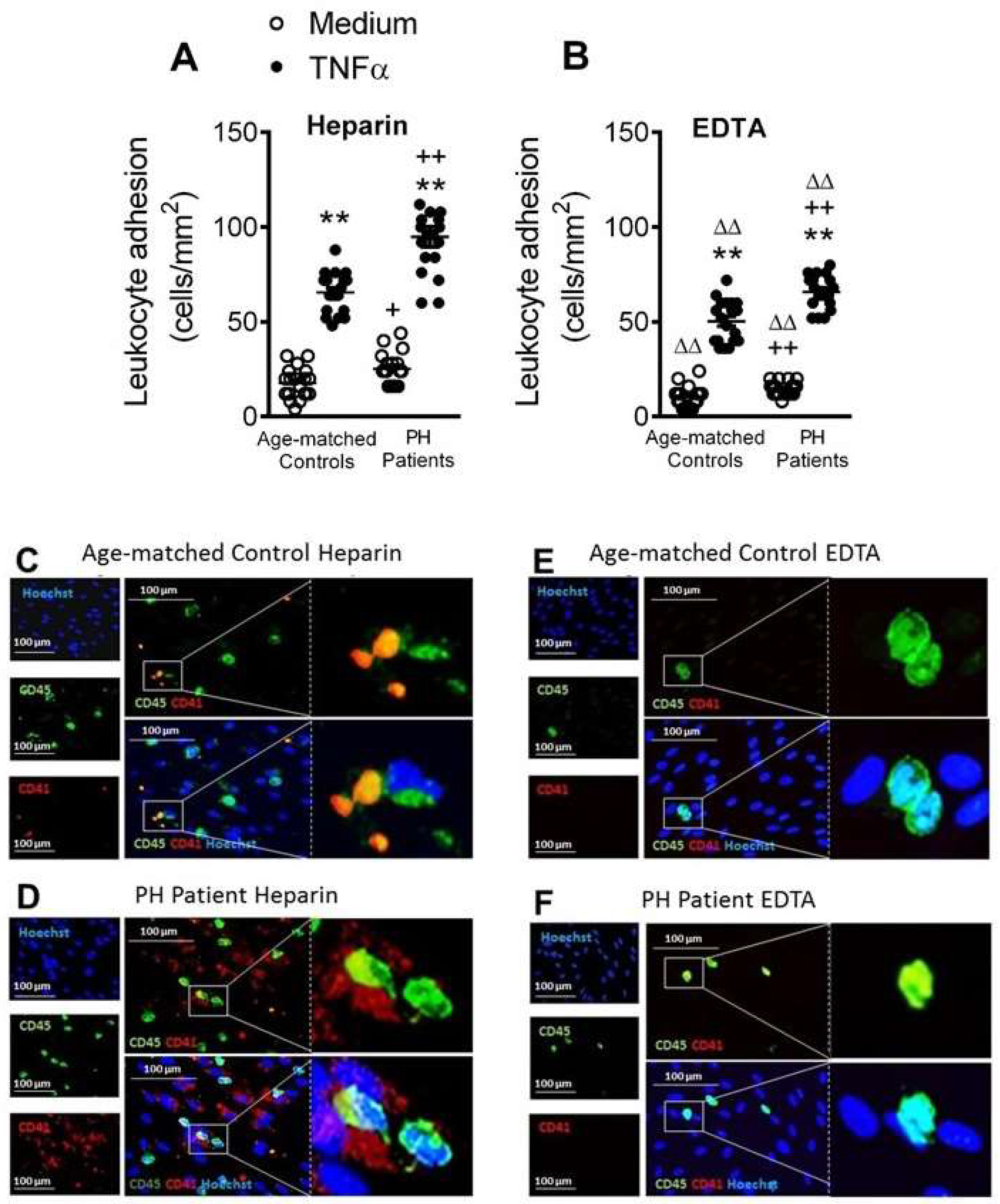
3.6. Circulating Platelet-Leukocytes and Leukocytes from PH Patients Have Increased Adhesiveness to TNFα-Stimulated HUAEC
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Ross, R. The pathogenesis of atherosclerosis: A perspective for the 1990s. Nature 1993, 362, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Catapano, A.L.; Pirillo, A.; Norata, G.D. Vascular inflammation and low-density lipoproteins: Is cholesterol the link? A lesson from the clinical trials. Br. J. Pharmacol. 2017, 174, 3973–3985. [Google Scholar] [CrossRef] [PubMed]
- Langslet, G.; Emery, M.; Wasserman, S.M. Evolocumab (AMG 145) for primary hypercholesterolemia. Expert Rev. Cardiovasc. Ther. 2015, 13, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Barale, C.; Frascaroli, C.; Senkeev, R.; Cavalot, F.; Russo, I. Simvastatin Effects on Inflammation and Platelet Activation Markers in Hypercholesterolemia. Biomed Res. Int. 2018, 2018, 6508709. [Google Scholar] [CrossRef] [PubMed]
- Real, J.T.; Martinez-Hervas, S.; Garcia-Garcia, A.B.; Civera, M.; Pallardo, F.V.; Ascaso, J.F.; Vina, J.R.; Chaves, F.J.; Carmena, R. Circulating mononuclear cells nuclear factor-kappa B activity, plasma xanthine oxidase, and low grade inflammatory markers in adult patients with familial hypercholesterolaemia. Eur. J. Clin. Investig. 2010, 40, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Holven, K.B.; Narverud, I.; Lindvig, H.W.; Halvorsen, B.; Langslet, G.; Nenseter, M.S.; Ulven, S.M.; Ose, L.; Aukrust, P.; Retterstol, K. Subjects with familial hypercholesterolemia are characterized by an inflammatory phenotype despite long-term intensive cholesterol lowering treatment. Atherosclerosis 2014, 233, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.M.; Ye, Z.X.; Chiou, K.R.; Lin, S.J.; Charng, M.J. Vascular stiffness in familial hypercholesterolaemia is associated with C-reactive protein and cholesterol burden. Eur. J. Clin. Investig. 2007, 37, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Sampietro, T.; Tuoni, M.; Ferdeghini, M.; Ciardi, A.; Marraccini, P.; Prontera, C.; Sassi, G.; Taddei, M.; Bionda, A. Plasma cholesterol regulates soluble cell adhesion molecule expression in familial hypercholesterolemia. Circulation 1997, 96, 1381–1385. [Google Scholar] [CrossRef]
- Cortes, R.; Ivorra, C.; Martinez-Hervas, S.; Pedro, T.; Gonzalez-Albert, V.; Artero, A.; Adam, V.; Garcia-Garcia, A.B.; Ascaso, J.F.; Real, J.T.; et al. Postprandial Changes in Chemokines Related to Early Atherosclerotic Processes in Familial Hypercholesterolemic Subjects: A Preliminary Study. Arch. Med. Res. 2016, 47, 33–39. [Google Scholar] [CrossRef]
- Hansen, M.; Kuhlman, A.C.B.; Sahl, R.E.; Kelly, B.; Morville, T.; Dohlmann, T.L.; Chrois, K.M.; Larsen, S.; Helge, J.W.; Dela, F. Inflammatory biomarkers in patients in Simvastatin treatment: No effect of co-enzyme Q10 supplementation. Cytokine 2019, 113, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Charo, I.F.; Ransohoff, R.M. The many roles of chemokines and chemokine receptors in inflammation. N. Engl. J. Med. 2006, 354, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Holven, K.B.; Damas, J.K.; Yndestad, A.; Waehre, T.; Ueland, T.; Halvorsen, B.; Heggelund, L.; Sandberg, W.J.; Semb, A.G.; Froland, S.S.; et al. Chemokines in children with heterozygous familiar hypercholesterolemia: Selective upregulation of RANTES. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Landmesser, U.; Hornig, B.; Drexler, H. Endothelial function: A critical determinant in atherosclerosis? Circulation 2004, 109, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Olson, N.C.; Sallam, R.; Doyle, M.F.; Tracy, R.P.; Huber, S.A. T helper cell polarization in healthy people: Implications for cardiovascular disease. J. Cardiovasc. Transl. Res. 2013, 6, 772–786. [Google Scholar] [CrossRef] [PubMed]
- Chironi, G.; Dosquet, C.; del-Pino, M.; Denarie, N.; Megnien, J.L.; Drouet, L.; Bal dit Sollier, C.; Levenson, J.; Simon, A. Relationship of circulating biomarkers of inflammation and hemostasis with preclinical atherosclerotic burden in nonsmoking hypercholesterolemic men. Am. J. Hypertens. 2006, 19, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Von Hundelshausen, P.; Schmitt, M.M. Platelets and their chemokines in atherosclerosis-clinical applications. Front. Physiol. 2014, 5, 294. [Google Scholar] [CrossRef]
- Mazor, R.; Shurtz-Swirski, R.; Farah, R.; Kristal, B.; Shapiro, G.; Dorlechter, F.; Cohen-Mazor, M.; Meilin, E.; Tamara, S.; Sela, S. Primed polymorphonuclear leukocytes constitute a possible link between inflammation and oxidative stress in hyperlipidemic patients. Atherosclerosis 2008, 197, 937–943. [Google Scholar] [CrossRef]
- Weber, C.; Shantsila, E.; Hristov, M.; Caligiuri, G.; Guzik, T.; Heine, G.H.; Hoefer, I.E.; Monaco, C.; Peter, K.; Rainger, E.; et al. Role and analysis of monocyte subsets in cardiovascular disease. Joint consensus document of the European Society of Cardiology (ESC) Working Groups “Atherosclerosis & Vascular Biology” and “Thrombosis”. Thromb Haemost 2016, 116, 626–637. [Google Scholar] [CrossRef]
- Fadini, G.P.; Simoni, F.; Cappellari, R.; Vitturi, N.; Galasso, S.; Vigili de Kreutzenberg, S.; Previato, L.; Avogaro, A. Pro-inflammatory monocyte-macrophage polarization imbalance in human hypercholesterolemia and atherosclerosis. Atherosclerosis 2014, 237, 805–808. [Google Scholar] [CrossRef]
- Wu, H.; Ballantyne, C.M. Dyslipidaemia: PCSK9 inhibitors and foamy monocytes in familial hypercholesterolaemia. Nat. Rev. Cardiol. 2017, 14, 385–386. [Google Scholar] [CrossRef] [PubMed]
- Kratofil, R.M.; Kubes, P.; Deniset, J.F. Monocyte Conversion During Inflammation and Injury. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Urra, X.; Villamor, N.; Amaro, S.; Gomez-Choco, M.; Obach, V.; Oleaga, L.; Planas, A.M.; Chamorro, A. Monocyte subtypes predict clinical course and prognosis in human stroke. J. Cereb. Blood Flow Metab. 2009, 29, 994–1002. [Google Scholar] [CrossRef] [PubMed]
- Ketelhuth, D.F.; Hansson, G.K. Adaptive Response of T and B Cells in Atherosclerosis. Circ. Res. 2016, 118, 668–678. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.W.; Zheng, X.X.; Zhou, T.; Tong, X.H.; Luo, C.Y.; Wang, X.A. HMGB1Modulates the Treg/Th17 Ratio in Atherosclerotic Patients. J. Atherosc. Thromb. 2016, 23, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Quandt, D.; Rothe, K.; Scholz, R.; Baerwald, C.W.; Wagner, U. Peripheral CD4CD8 double positive T cells with a distinct helper cytokine profile are increased in rheumatoid arthritis. PLoS ONE. 2014, 9, e93293. [Google Scholar] [CrossRef] [PubMed]
- Yoshimoto, T. The Hunt for the Source of Primary Interleukin-4: How We Discovered That Natural Killer T Cells and Basophils Determine T Helper Type 2 Cell Differentiation In Vivo. Front. Immunol. 2018, 9, 716. [Google Scholar] [CrossRef]
- Rius, C.; Company, C.; Piqueras, L.; Cerda-Nicolas, J.M.; Gonzalez, C.; Servera, E.; Ludwig, A.; Morcillo, E.J.; Sanz, M.J. Critical role of fractalkine (CX3CL1) in cigarette smoke-induced mononuclear cell adhesion to the arterial endothelium. Thorax 2013, 68, 177–186. [Google Scholar] [CrossRef]
- Rius, C.; Piqueras, L.; Gonzalez-Navarro, H.; Albertos, F.; Company, C.; Lopez-Gines, C.; Ludwig, A.; Blanes, J.I.; Morcillo, E.J.; Sanz, M.J. Arterial and venous endothelia display differential functional fractalkine (CX3CL1) expression by angiotensin-II. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 96–104. [Google Scholar] [CrossRef]
- Marques, P.; Collado, A.; Escudero, P.; Rius, C.; Gonzalez, C.; Servera, E.; Piqueras, L.; Sanz, M.J. Cigarette Smoke Increases Endothelial CXCL16-Leukocyte CXCR6 Adhesion In Vitro and In Vivo. Potential Consequences in Chronic Obstructive Pulmonary Disease. Front. Immunol. 2017, 8, 1766. [Google Scholar] [CrossRef]
- Furio, E.; Garcia-Fuster, M.J.; Redon, J.; Marques, P.; Ortega, R.; Sanz, M.J.; Piqueras, L. CX3CR1/CX3CL1 Axis Mediates Platelet-Leukocyte Adhesion to Arterial Endothelium in Younger Patients with a History of Idiopathic Deep Vein Thrombosis. Thromb Haemost 2018, 118, 562–571. [Google Scholar] [CrossRef] [PubMed]
- Michelson, A.D.; Barnard, M.R.; Krueger, L.A.; Valeri, C.R.; Furman, M.I. Circulating monocyte-platelet aggregates are a more sensitive marker of in vivo platelet activation than platelet surface P-selectin: Studies in baboons, human coronary intervention, and human acute myocardial infarction. Circulation 2001, 104, 1533–1537. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Volunteers (n = 21) | PH Subjects (n = 22) | p Value | |
|---|---|---|---|
| Age (years) | 48.8 ± 2.7 | 49 ± 3.1 | 0.95 |
| Gender M/F (%) | 5/16 (23.8/76.2) | 4/18 (18.2/81.8) | 0.72 |
| BMI (kg/m2) | 25.4 ± 0.7 | 25.7 ± 0.9 | 0.83 |
| Waist circumference (cm) | 85.3 ± 1.9 | 85.7 ± 2.2 | 0.90 |
| SBP (mmHg) | 115.9 ± 2.0 | 124.7 ± 3.6 * | <0.05 |
| DBP (mmHg) | 71.6 ± 1.8 | 78.5 ± 2.6 * | <0.05 |
| Glucose (mg/dL) | 86.7 ± 1.5 | 88.1 ± 1.9 | 0.57 |
| TC levels (mg/dL) | 206.1 ± 6.8 | 264.6 ± 8.9 ** | <0.01 |
| LDL levels (mg/dL) | 130.6 ± 5.4 | 182.8 ± 6.2 ** | <0.01 |
| TG (mg/dL) | 80.9 ± 7.3 | 109.7 ± 8.5 ** | <0.01 |
| HDL levels (mg/dL) | 65.9 ± 2.5 | 63.4 ± 2.9 | 0.51 |
| ApoB (mg/dL) | 92.5 ± 4.1 | 127.4 ± 5.0 ** | <0.01 |
| GOT (U/L) | 21.7 ± 0.9 | 22.8 ± 1.1 | 0.42 |
| GPT (U/L) | 18.3 ± 1.8 | 18.5 ± 1.1 | 0.90 |
| Creatinine (mg/dL) | 0.7 ± 0.0 | 0.7 ± 0.0 | 0.48 |
| IgG (mg/dL) | 966.7 ± 41.1 | 968.5 ± 34.4 | 0.97 |
| Igm (mg/dL) | 100.4 ± 7.6 | 125.8 ± 14.1 | 0.14 |
| IgE total (IU/L) | 42.6 ± 12.0 | 50.4 ± 16.9 | 0.71 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collado, A.; Marques, P.; Domingo, E.; Perello, E.; González-Navarro, H.; Martinez-Hervás, S.; Real, J.T.; Piqueras, L.; Ascaso, J.F.; Sanz, M.-J. Novel Immune Features of the Systemic Inflammation Associated with Primary Hypercholesterolemia: Changes in Cytokine/Chemokine Profile, Increased Platelet and Leukocyte Activation. J. Clin. Med. 2019, 8, 18. https://doi.org/10.3390/jcm8010018
Collado A, Marques P, Domingo E, Perello E, González-Navarro H, Martinez-Hervás S, Real JT, Piqueras L, Ascaso JF, Sanz M-J. Novel Immune Features of the Systemic Inflammation Associated with Primary Hypercholesterolemia: Changes in Cytokine/Chemokine Profile, Increased Platelet and Leukocyte Activation. Journal of Clinical Medicine. 2019; 8(1):18. https://doi.org/10.3390/jcm8010018
Chicago/Turabian StyleCollado, Aida, Patrice Marques, Elena Domingo, Eva Perello, Herminia González-Navarro, Sergio Martinez-Hervás, José T. Real, Laura Piqueras, Juan F. Ascaso, and Maria-Jesus Sanz. 2019. "Novel Immune Features of the Systemic Inflammation Associated with Primary Hypercholesterolemia: Changes in Cytokine/Chemokine Profile, Increased Platelet and Leukocyte Activation" Journal of Clinical Medicine 8, no. 1: 18. https://doi.org/10.3390/jcm8010018
APA StyleCollado, A., Marques, P., Domingo, E., Perello, E., González-Navarro, H., Martinez-Hervás, S., Real, J. T., Piqueras, L., Ascaso, J. F., & Sanz, M.-J. (2019). Novel Immune Features of the Systemic Inflammation Associated with Primary Hypercholesterolemia: Changes in Cytokine/Chemokine Profile, Increased Platelet and Leukocyte Activation. Journal of Clinical Medicine, 8(1), 18. https://doi.org/10.3390/jcm8010018