Early Vitamin C and Thiamine Administration to Patients with Septic Shock in Emergency Departments: Propensity Score-Based Analysis of a Before-and-After Cohort Study

 , , ,
, , ,
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Statistical Analyses
3. Results
3.1. Baseline Characteristics
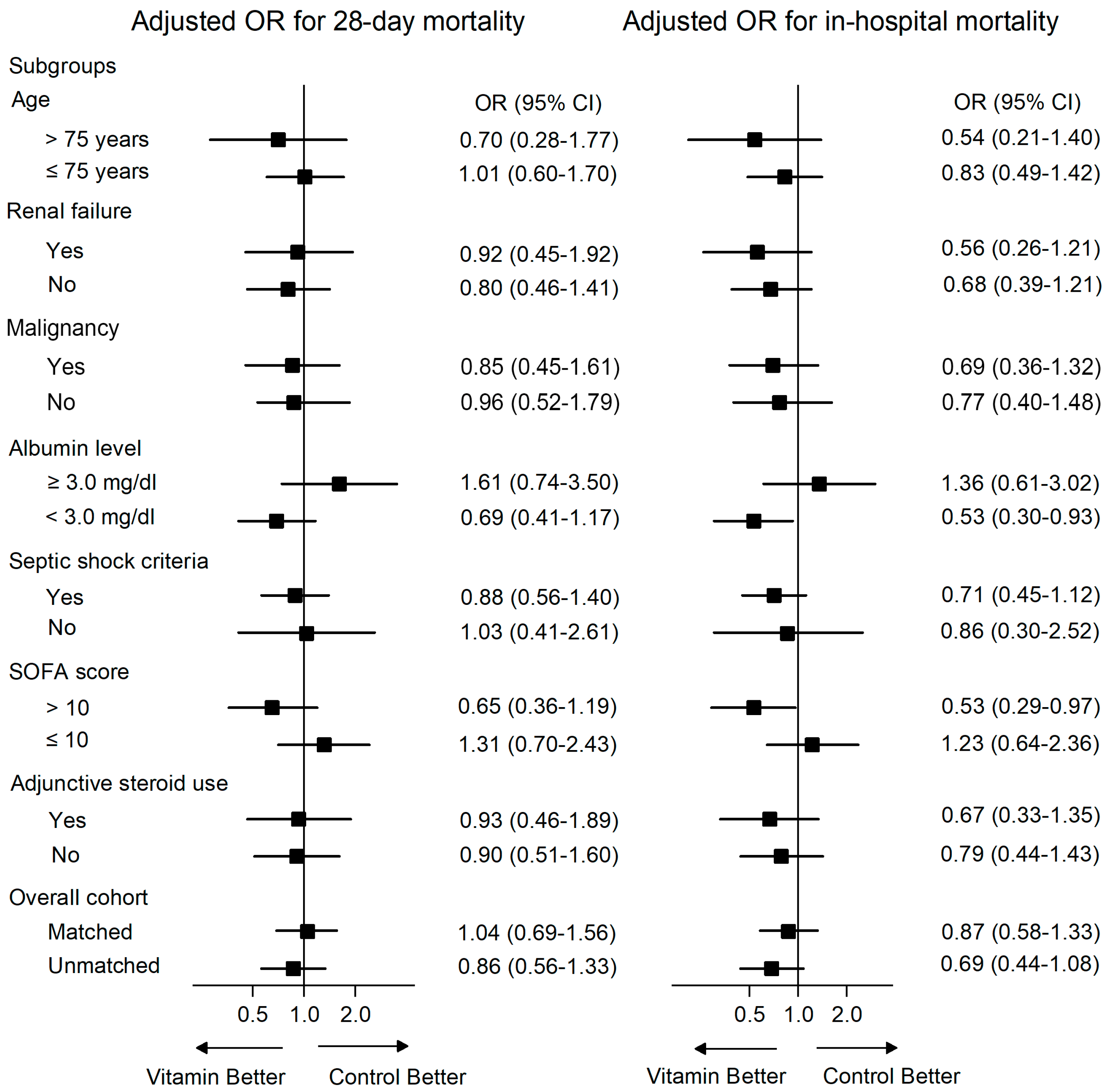
3.2. Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for sepsis and septic shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef]
- Seymour, C.W.; Rosengart, M.R. Septic Shock: Advances in Diagnosis and Treatment. JAMA 2015, 314, 708–717. [Google Scholar] [CrossRef] [PubMed]
- Teng, J.; Pourmand, A.; Mazer-Amirshahi, M. Vitamin C: The next step in sepsis management? J. Crit. Care 2018, 43, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Oudemans-van Straaten, H.M.; Spoelstra-de Man, A.M.; de Waard, M.C. Vitamin C revisited. Crit. Care 2014, 18, 460. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Khangoora, V.; Rivera, R.; Hooper, M.H.; Catravas, J. Hydrocortisone, Vitamin C, and Thiamine for the Treatment of Severe Sepsis and Septic Shock: A Retrospective Before-After Study. Chest 2017, 151, 1229–1238. [Google Scholar] [CrossRef] [PubMed]
- Donnino, M.W.; Andersen, L.W.; Chase, M.; Berg, K.M.; Tidswell, M.; Giberson, T.; Wolfe, R.; Moskowitz, A.; Smithline, H.; Ngo, L.; et al. Randomized, Double-Blind, Placebo-Controlled Trial of Thiamine as a Metabolic Resuscitator in Septic Shock. Crit. Care Med. 2016, 44, 360–367. [Google Scholar] [CrossRef]
- Zabet, M.H.; Mohammadi, M.; Ramezani, M.; Khalili, H. Effect of high-dose Ascorbic acid on vasopressor’s requirement in septic shock. J. Res. Pharm. Pract. 2016, 5, 94–100. [Google Scholar]
- Fowler, A.A., 3rd; Syed, A.A.; Knowlson, S.; Sculthorpe, R.; Farthing, D.; DeWilde, C.; Farthing, C.A.; Larus, T.L.; Martin, E.; Brophy, D.F.; et al. Phase I safety trial of intravenous ascorbic acid in patients with severe sepsis. J. Transl. Med. 2014, 12, 32. [Google Scholar] [CrossRef]
- May, J.M.; Harrison, F.E. Role of vitamin C in the function of the vascular endothelium. Antioxid. Redox Signal 2013, 19, 2068–2083. [Google Scholar] [CrossRef]
- Berger, M.M.; Oudemans-van Straaten, H.M. Vitamin C supplementation in the critically ill patient. Current Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Leite, H.P.; de Lima, L.F. Metabolic resuscitation in sepsis: A necessary step beyond the hemodynamic? J. Thorac. Dis. 2016, 8, E552–E557. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Hwang, S.Y.; Jo, I.J.; Kim, W.Y.; Ryoo, S.M.; Kang, G.H.; Kim, K.; Jo, Y.H.; Chung, S.P.; Joo, Y.S.; et al. Prognostic Value of the Lactate/Albumin Ratio for Predicting 28-Day Mortality in Critically Ill Sepsis Patients. Shock 2018. [Google Scholar] [CrossRef]
- Ko, B.S.; Kim, K.; Choi, S.H.; Kang, G.H.; Shin, T.G.; Jo, Y.H.; Ryoo, S.M.; Beom, J.H.; Kwon, W.Y.; Han, K.S.; et al. Prognosis of patients excluded by the definition of septic shock based on their lactate levels after initial fluid resuscitation: A prospective multi-center observational study. Crit. Care 2018, 22, 47. [Google Scholar] [CrossRef] [PubMed]
- Shin, T.G.; Hwang, S.Y.; Kang, G.H.; Kim, W.Y.; Ryoo, S.M.; Kim, K.; Jo, Y.H.; Chung, S.P.; Joo, Y.S.; Beom, J.H.; et al. Korean Shock Society septic shock registry: A preliminary report. Clin. Exp. Emerg. Med. 2017, 4, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit. Care Med. 2013, 41, 580–637. [Google Scholar] [CrossRef] [PubMed]
- Casserly, B.; Phillips, G.S.; Schorr, C.; Dellinger, R.P.; Townsend, S.R.; Osborn, T.M.; Reinhart, K.; Selvakumar, N.; Levy, M.M. Lactate measurements in sepsis-induced tissue hypoperfusion: Results from the Surviving Sepsis Campaign database. Crit. Care Med. 2015, 43, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.-L.; Ramsay, G.J. 2001 SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference. Crit. Care Med. 2003, 29, 530–538. [Google Scholar]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- de Grooth, H.J.; Manubulu-Choo, W.P.; Zandvliet, A.S.; Spoelstra-de Man, A.M.E.; Girbes, A.R.; Swart, E.L.; Oudemans-van Straaten, H.M. Vitamin C Pharmacokinetics in Critically Ill Patients: A Randomized Trial of Four IV Regimens. Chest 2018, 153, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Barabutis, N.; Khangoora, V.; Marik, P.E.; Catravas, J.D. Hydrocortisone and Ascorbic Acid Synergistically Prevent and Repair Lipopolysaccharide-Induced Pulmonary Endothelial Barrier Dysfunction. Chest 2017, 152, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, E.; Roux-Lombard, P.; Grau, G.E.; Girardin, E.; Ricou, B.; Dayer, J.; Suter, P.M. Plasma concentrations of cytokines, their soluble receptors, and antioxidant vitamins can predict the development of multiple organ failure in patients at risk. Crit. Care Med. 1996, 24, 392–397. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Overall (n = 1144) | Treatment Group (n = 229) | Control Group (n = 915) | p |
|---|---|---|---|---|
| Age (years) | 67 (58–75) | 67 (58–76) | 67 (60–75) | 0.91 |
| Sex, male | 713 (62.3) | 136 (59.4) | 577 (63.1) | 0.30 |
| Comorbidities | ||||
| Hypertension | 412 (36.1) | 89 (38.9) | 323 (35.3) | 0.31 |
| Diabetes | 335 (29.3) | 71 (31.0) | 264 (28.9) | 0.52 |
| Cardiac disease | 152 (13.3) | 24 (10.5) | 128 (13.4) | 0.16 |
| Chronic lung disease | 94 (8.2) | 17 (7.4) | 77 (8.4) | 0.62 |
| Chronic renal disease | 78 (6.8) | 15 (6.6) | 63 (6.9) | 0.85 |
| Chronic liver disease | 180 (15.7) | 35 (15.3) | 145 (15.9) | 0.83 |
| Hematologic malignancy | 113 (9.9) | 19 (8.3) | 94 (10.3) | 0.37 |
| Metastatic solid cancer | 364 (31.8) | 72 (31.4) | 292 (31.9) | 0.89 |
| Suspected infection focus | 0.04 | |||
| Respiratory infection | 268 (22.4) | 41 (17.9) | 227 (24.8) | |
| Urinary tract infection | 158 (13.8) | 41 (17.9) | 117 (12.8) | |
| Intra-abdominal infection | 435 (38.0) | 85 (37.1) | 350 (38.3) | |
| Others or unknown | 283 (24.7) | 62 (27.1) | 221 (24.2) | |
| Laboratory tests | ||||
| White blood cell count, ×103/μL | 9.6 (4.5–16.3) | 8.1 (4.1–15.1) | 9.9 (4.6–16.9) | 0.17 |
| Hemoglobin (g/dL) | 10.7 (9.0–12.4) | 10.6 (9.0–12.2) | 10.8 (9.0–12.5) | 0.33 |
| Platelet count (×103/μL) | 137 (66–215) | 132 (72–183) | 138 (65–225) | 0.30 |
| Creatinine (mg/dL) | 1.3 (0.9–2.0) | 1.4 (1.0–2.2) | 1.3 (0.9–2.0) | 0.06 |
| ALT (U/L) | 28 (16–57) | 30 (16–57) | 28 (16–57) | 0.85 |
| Albumin (g/dL) | 2.9 (2.4–3.4) | 2.8 (2.4–3.3) | 3.0 (2.5–3.4) | 0.01 |
| Initial lactate (mmol/L) | 3.6 (2.0–5.5) | 3.4 (2.1–5.7) | 3.7 (1.9–5.5) | 0.72 |
| Blood culture—positive | 484 (42.3) | 367 (40.1) | 117 (51.1) | <0.01 |
| Septic shock criteria, Sepsis-3 consensus definition | 593 (51.8) | 152 (66.4) | 441 (48.2) | <0.01 |
| Adjunctive steroid use within 48 h | 287 (25.1) | 62 (27.1) | 225 (24.6) | 0.43 |
| Vasopressor use | 966 (84.4) | 217 (94.8) | 749 (81.9) | <0.01 |
| Mechanical ventilation | 328 (17.9) | 67 (39.3) | 261 (28.5) | 0.82 |
| Interventions for source control | 332 (29.0) | 58 (25.3) | 274 (30.0) | 0.16 |
| Maximum SOFA score in 24 h | 8 (5–11) | 9 (6–12) | 8 (5–11) | <0.01 |
| APACHE II score | 20 (15–27) | 27 (21–52) | 27 (20–56) | 0.99 |
| Overall Cohort | Propensity-Matched Cohort | |||||
|---|---|---|---|---|---|---|
| Treatment (n = 229) | Control (n = 915) | p | Treatment (n = 227) | Control (n = 527) | p | |
| 28-day mortality | 42 (18.3) | 160 (17.5) | 0.76 | 42 (18.5) | 92 (17.5) | 0.84 |
| In-hospital mortality | 38 (16.6) | 167 (18.3) | 0.55 | 38 (16.7) | 97 (18.4) | 0.54 |
| ICU LOS (days) | 4 (3–8) | 4 (3–8) | 0.70 | 4 (3–8) | 4 (3–7) | 0.84 |
| Hospital LOS (days) | 14 (9–22) | 13 (8–23) | 0.49 | 14 (9–22) | 13 (8–23) | 0.33 |
| Duration of mechanical ventilation | 6.0 (3.0–15.0) | 6.0 (3.0–12.0) | 0.61 | 5.5 (3.0–15.0) | 5.0 (3.0–10.0) | 0.63 |
| New use of renal replacement therapy | 28 (12.3) | 106 (11.9) | 0.87 | 28 (12.4) | 66 (12.9) | 0.51 |
| Variable | 28-Day Mortality | In-Hospital Mortality | ||||
|---|---|---|---|---|---|---|
| Adjusted OR | 95% CI | p | Adjusted OR | 95% CI | p | |
| Vitamin treatment | 0.86 | 0.56–1.33 | 0.51 | 0.69 | 0.44–1.08 | 0.11 |
| Infection focus | ||||||
| Respiratory | Reference | Reference | ||||
| UTI | 0.52 | 0.26–1.04 | 0.06 | 0.36 | 0.18–0.74 | 0.01 |
| Abdomen | 0.73 | 0.45–1.20 | 0.22 | 0.52 | 0.32–0.86 | 0.01 |
| Other | 1.08 | 0.67–1.74 | 0.75 | 0.77 | 0.47–1.25 | 0.29 |
| WBC count (>12,000/μL) | 1.25 | 0.87–1.79 | 0.22 | 1.33 | 0.93–1.92 | 0.12 |
| Creatinine (>2.0 mg/dL) | 0.93 | 0.62–1.40 | 0.73 | 0.84 | 0.55–1.29 | 0.43 |
| Albumin (<3.0 mg/dL) | 3.00 | 2.05–4.39 | <0.01 | 3.29 | 2.13–5.06 | <0.01 |
| Blood culture positive | 0.51 | 0.34–0.76 | <0.01 | 0.67 | 0.45–1.01 | 0.06 |
| Septic shock criteria | 2.16 | 1.36–3.43 | <0.01 | 2.88 | 1.75–4.72 | <0.01 |
| Vasopressor use | 0.25 | 0.14–0.47 | <0.01 | 0.22 | 0.11–0.42 | <0.01 |
| Source control interventions | 0.58 | 0.36–0.93 | 0.02 | 0.55 | 0.34–0.88 | 0.01 |
| Maximum 24-h SOFA score | 1.30 | 1.23–1.37 | <0.01 | 1.31 | 1.23–1.38 | <0.01 |
| Subgroups | 28-Day Mortality | In-Hospital Mortality | ||
|---|---|---|---|---|
| Treatment | Control | Treatment | Control | |
| Age (years) | ||||
| >75 | 20.7 (12/58) | 17.5 (42/240) | 20.0 (11/58) | 17.9 (43/240) |
| ≤75 | 17.5 (30/171) | 17.5 (118/675) | 15.8 (27/171) | 18.4 (124/675) |
| Renal failure | ||||
| Yes | 29.7 (19/64) | 25.8 (59/229) | 25.0 (16/64) | 26.2 (60/229) |
| No | 13.9 (23/165) | 14.7 (101/686) | 13.3 (22/165) | 15.6 (107/686) |
| Malignancy | ||||
| Yes | 24.1 (22/91) | 23.7 (91/384) | 22.0 (20/91) | 24.0 (92/384) |
| No | 14.5 (20/138) | 13.0 (69/531) | 13.0 (13/138) | 14.1 (75/531) |
| Albumin (mg/dL) | ||||
| ≥3.0 | 13.6 (12/88) | 9.0 (42/465) | 12.5 (11/88) | 9.9 (46/465) |
| <3.0 | 21.3 (30/141) | 26.2 (118/450) | 19.2 (27/141) | 26.9 (121/450) |
| Septic shock criteria | ||||
| Yes | 23.0 (35/152) | 24.7 (109/441) | 21.7 (33/152) | 27.2 (120/441) |
| No | 9.1 (7/77) | 10.8 (51/474) | 6.5 (5/77) | 9.9 (47/474) |
| SOFA score | ||||
| >10 | 30.1 (22/73) | 38.7 (89/230) | 28.8 (21/73) | 42.2 (97/230) |
| ≤10 | 12.8 (20/156) | 10.4 (71/685) | 10.9 (17/156) | 10.2 (70/685) |
| Adjunctive steroid use | ||||
| Yes | 32.3 (20/62) | 30.7 (69/225) | 29.0 (18/62) | 33.3 (75/225) |
| No | 13.2 (22/167) | 13.2 (91/690) | 12.0 (20/167) | 13.3 (92/690) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, T.G.; Kim, Y.-J.; Ryoo, S.M.; Hwang, S.Y.; Jo, I.J.; Chung, S.P.; Choi, S.-H.; Suh, G.J.; Kim, W.Y. Early Vitamin C and Thiamine Administration to Patients with Septic Shock in Emergency Departments: Propensity Score-Based Analysis of a Before-and-After Cohort Study. J. Clin. Med. 2019, 8, 102. https://doi.org/10.3390/jcm8010102
Shin TG, Kim Y-J, Ryoo SM, Hwang SY, Jo IJ, Chung SP, Choi S-H, Suh GJ, Kim WY. Early Vitamin C and Thiamine Administration to Patients with Septic Shock in Emergency Departments: Propensity Score-Based Analysis of a Before-and-After Cohort Study. Journal of Clinical Medicine. 2019; 8(1):102. https://doi.org/10.3390/jcm8010102
Chicago/Turabian StyleShin, Tae Gun, Youn-Jung Kim, Seung Mok Ryoo, Sung Yeon Hwang, Ik Joon Jo, Sung Phil Chung, Sung-Hyuk Choi, Gil Joon Suh, and Won Young Kim. 2019. "Early Vitamin C and Thiamine Administration to Patients with Septic Shock in Emergency Departments: Propensity Score-Based Analysis of a Before-and-After Cohort Study" Journal of Clinical Medicine 8, no. 1: 102. https://doi.org/10.3390/jcm8010102
APA StyleShin, T. G., Kim, Y.-J., Ryoo, S. M., Hwang, S. Y., Jo, I. J., Chung, S. P., Choi, S.-H., Suh, G. J., & Kim, W. Y. (2019). Early Vitamin C and Thiamine Administration to Patients with Septic Shock in Emergency Departments: Propensity Score-Based Analysis of a Before-and-After Cohort Study. Journal of Clinical Medicine, 8(1), 102. https://doi.org/10.3390/jcm8010102