Mental Health Effects of Stress over the Life Span of Refugees


Abstract
1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Participants and Sampling
2.3. Measures and Model Indicators
2.3.1. Instrument Translation and Administration
2.3.2. Stress Constructs and Indicator Measures
2.3.3. Non-War Non-Migration Stress (NWS) Construct
2.3.4. War-Related Stress (WRS) Construct
2.3.5. Post-Migration Stress (PMS) Construct
2.3.6. Mental Health Construct and Indicator Measures
2.4. Data Analyses
3. Results
3.1. Descriptive
3.1.1. Participants
3.1.2. Stress Events
3.1.3. Mental Health Status
3.2. Correlations among Stress and Mental Health
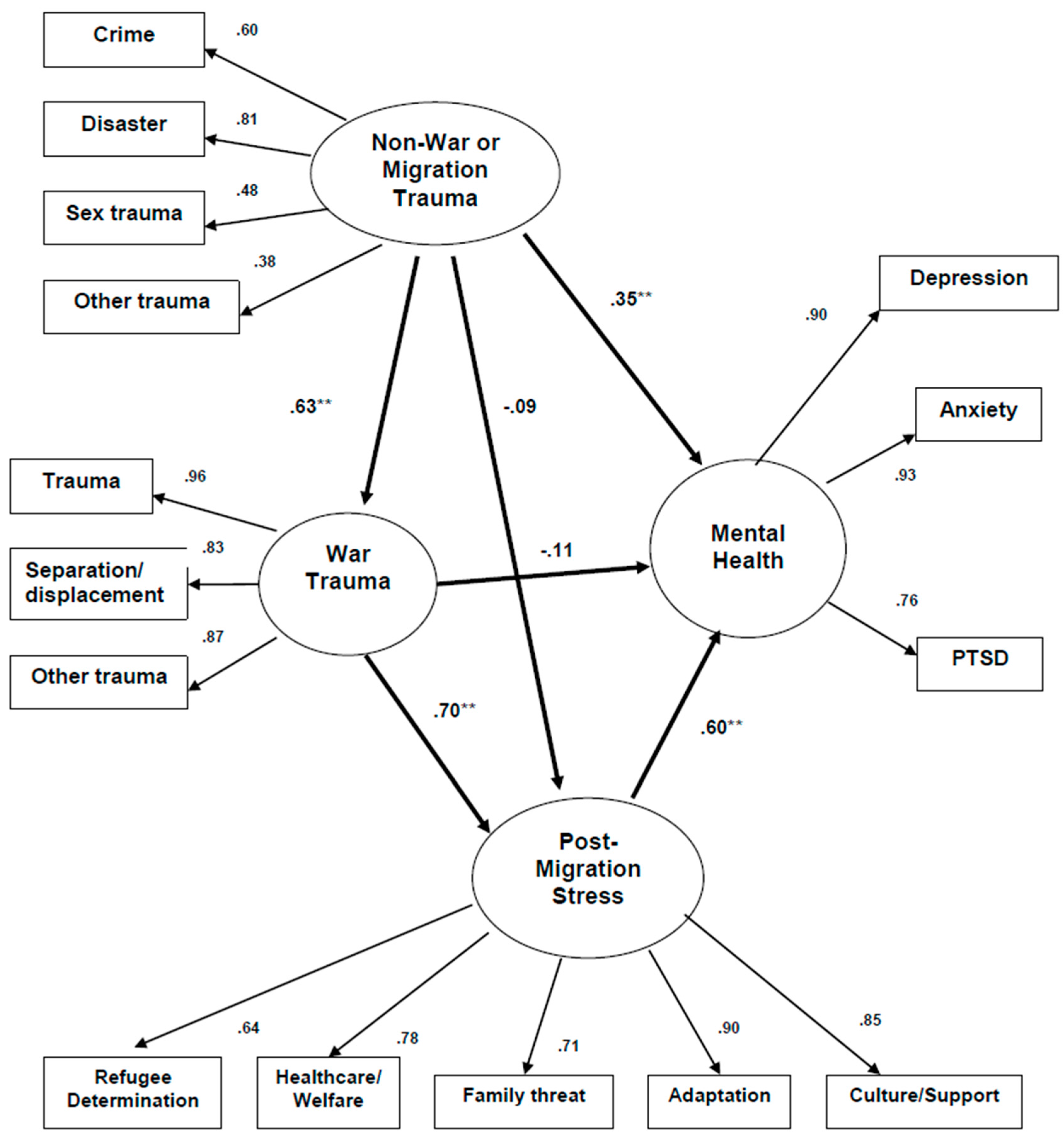
3.3. Predicting Adverse Mental Health from Stress Across the Lifespan
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- United Nations High Commissioner for Reguees (UNHCR). Global Trends: Forced Displacement in 2016. 2017. Available online: http://www.unhcr.org/statistics/unhcrstats/5943e8a34/globaltrends-forced-displacement-2016.html (accessed on 30 December 2017).
- Hollifield, M.; Verbillis-Kolp, S.; Farmer, B.; Toolson, E.C.; Woldehaimanot, T.; Yamazaki, J.; Holland, A.; Clair, J.S.; SooHoo, J. The Refugee Health Screener-15 (RHS-15): Development and validation of an instrument for anxiety, depression, and PTSD in refugees. Gen. Hosp. Psychiatry 2013, 35, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Fazel, M.; Wheeler, J.; Danesh, J. Prevalence of serious mental disorder in 7000 refugees resettled in western countries: A systematic review. Lancet 2005, 365, 1309–1314. [Google Scholar] [CrossRef]
- Fenta, H.; Hyman, I.; Noh, S. Determinants of depression among Ethiopian immigrants and refugees in Toronto. J. Nerv. Ment. Dis. 2004, 192, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Hollifield, M.; Warner, T.D.; Krakow, B.; Jenkins, J.; Westermeyer, J. The range of symptoms in refugees of war: The New Mexico Refugee Symptom Checklist-121. J. Nerv. Ment. Dis. 2009, 197, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Jaranson, J.M.; Butcher, J.; Halcon, L.; Johnson, D.R.; Robertson, C.; Savik, K.; Spring, M.; Westermeyer, J. Somali and Oromo refugees: Correlates of torture and trauma history. Am. J. Public Health 2004, 94, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Laban, C.J.; Gernaat, H.B.; Komproe, I.H.; van der Tweel, I.; De Jong, J.T. Postmigration living problems and common psychiatric disorders in Iraqi asylum seekers in the Netherlands. J. Nerv. Ment. Dis. 2004, 193, 825–832. [Google Scholar] [CrossRef]
- Marshall, G.N.; Schell, T.L.; Elliott, M.N.; Berthold, S.M.; Chun, C.A. Mental health of Cambodian refugees 2 decades after resettlement in the United States. JAMA 2005, 294, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Weine, S.M.; Kulenovic, A.D.; Pavkovic, I.; Gibbons, R. Testimony psychotherapy in Bosnian refugees: A pilot study. Am. J. Psychiatry 1998, 155, 1720–1726. [Google Scholar] [CrossRef] [PubMed]
- Momartin, S.; Steel, Z.; Coello, M.; Aroche, J.; Silove, D.M.; Brooks, R. A comparison of the mental health of refugees with temporary versus permanent protection visas. Med. J. Aust. 2006, 185, 357–361. [Google Scholar] [PubMed]
- Porter, M.; Haslam, N. Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons: A meta-analysis. JAMA 2005, 294, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Beiser, M. Strangers at the Gate. The Boat People’s First Ten Years in Canada; University of Toronto Press: Toronto, ON, Canada, 1999. [Google Scholar]
- Silove, D.; Sinnerbrink, I.; Field, A.; Manicavasagar, V.; Steel, Z. Anxiety, depression and PTSD in asylum-seekers: Associations with pre-migration trauma and post-migration stressors. Br. J. Psychiatry 1997, 170, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Westermeyer, J.; Vang, T.F.; Neider, J. Migration and mental health among Hmong refugees. Association of pre- and postmigration factors with self-rating scales. J. Nerv. Ment. Dis. 1983, 171, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Carswell, K.; Blackburn, P.; Barker, C. The relationship between trauma, post-migration problems and the psychological well-being of refugees and asylum seekers. Int. J. Soc. Psychiatry 2011, 57, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Chu, T.; Keller, A.S.; Rasmussen, A. Effects of post-migration factors on PTSD outcomes among immigrant survivors of political violence. J. Immigr. Minority Health 2013, 15, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Hall, B.J.; Ling, L.; Renzaho, A.M. Pre-migration and post-migration factors associated with mental health in humanitarian migrants in Australia and the moderation effect of post-migration stressors: Findings from the first wave data of the BNLA cohort study. Lancet Psychiatry 2017, 4, 218–229. [Google Scholar] [CrossRef]
- Silove, D. The asylum debacle in Australia: A challenge for psychiatry. Aust. N. Z. J. Psychiatry 2002, 36, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Lindencrona, F.; Ekblad, S.; Hauff, E. Mental health of recently resettled refugees from the Middle East in Sweden: The impact of pre-resettlement trauma, resettlement stress and capacity to handle stress. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, R.D.; Brough, M.; Vromans, L.; Asic-Kobe, M. Mental health of newly arrived Burmese refugees in Australia: Contributions of pre-migration and post-migration experience. Aust. N. Z. J. Psychiatry 2011, 45, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Steel, Z.; Silove, D.; Bird, K.; McGorry, P.; Mohan, P. Pathways from war trauma to posttraumatic stress symptoms among Tamil asylum seekers, refugees, and immigrants. J. Trauma. Stress 1999, 12, 421–435. [Google Scholar] [CrossRef] [PubMed]
- Birman, D.; Tran, N. Psychological distress and adjustment of Vietnamese refugees in the United States: Association with pre- and postmigration factors. Am. J. Orthopsychiatry 2008, 78, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Heptinstall, E.; Sethna, V.; Taylor, E. PTSD and depression in refugee children: Associations with pre-migration trauma and post-migration stress. Eur. Child Adolesc. Psychiatry 2004, 13, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Hollifield, M.; Warner, T.D.; Jenkins, J.; Sinclair-Lian, N.; Krakow, B.; Eckert, V.; Karadaghi, P.; Westermeyer, J. Assessing War Trauma in Refugees: Properties of the Comprehensive Trauma Inventory-104 (CTI-104). J. Trauma. Stress 2006, 19, 527–540. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.; McGorry, P. Psychological sequelae of torture and trauma in Chilean and Salvadorean migrants: A pilot study. Aust. N. Z. J. Psychiatry 1995, 29, 84–95. [Google Scholar] [CrossRef] [PubMed]
- U.N. Declaration against Torture: Article 1; United Nations: New York, NY, USA, 1985. [Google Scholar]
- Westermeyer, J.; Janca, A. Language, culture and psychopathology: Conceptual and methodological issues. Transcult. Psychiatry 1997, 34, 291–311. [Google Scholar] [CrossRef]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross-Cult. Psychol. 1970, 1, 187–216. [Google Scholar] [CrossRef]
- Green, B.L. Psychometric review of Trauma History Questionnaire (Self-Report). In Measurement of Stress, Trauma, and Adaptation; Stamm, B., Ed.; Sidran Press: Luthreville, MD, USA, 1996. [Google Scholar]
- Hollifield, M.; Warner, T.D.; Lian, N.; Krakow, B.; Jenkins, J.H.; Kesler, J.; Stevenson, J.; Westermeyer, J. Measuring trauma and health status in refugees: A critical review. JAMA 2002, 288, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Hollifield, M.; Eckert, V.; Warner, T.D.; Jenkins, J.; Krakow, B.; Ruiz, J.; Westermeyer, J. Development of an inventory for measuring war-related events in refugees. Compr. Psychiatry 2005, 46, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Silove, D.; Steel, Z.; McGorry, P.; Mohan, P. Trauma exposure, postmigration stressors, and symptoms of anxiety, depression and post-traumatic stress in Tamil asylum-seekers: Comparison with refugees and immigrants. Acta Psychiatr. Scand. 1998, 97, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R. The Hopkins Symptom Checklist (HSCL): A measure of primary symptom dimensions. In Modern Problems in Pharmacopsychiatry; Basel, P., Ed.; Karger: Basel, Switzerland, 1974. [Google Scholar]
- Mollica, R.F.; Wyshak, G.; de Marneffe, D.; Khuon, F.; Lavelle, J. Indochinese versions of the Hopkins Symptom Checklist-25: A screening instrument for the psychiatric care of refugees. Am. J. Psychiatry 1987, 144, 497–500. [Google Scholar] [PubMed]
- Winokur, A.; Winokur, D.F.; Rickels, K.; Cox, D.S. Symptoms of emotional distress in a family planning service: Stability over a four-week period. Br. J. Psychiatry 1984, 144, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Foa, E.B.; Riggs, D.S.; Dancu, C.V.; Rothbaum, B.O. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J. Trauma. Stress 1993, 6, 459–473. [Google Scholar] [CrossRef]
- Bollen, K.A. Structural Equations with Latent Variables; Wiley: New York, NY, USA, 1989. [Google Scholar]
- Breslau, N.; Chilcoat, H.D.; Kessler, R.C.; Davis, G.C. Previous exposure to trauma and PTSD effects of subsequent trauma: Results from the Detroit Area Survey of Trauma. Am. J. Psychiatry 1999, 156, 902–907. [Google Scholar] [CrossRef] [PubMed]
- De Jong, J.T.; Komproe, I.H.; Van Ommeren, M.; El Masri, M.; Araya, M.; Khaled, N.; van De Put, W.; Somasundaram, D. Lifetime events and posttraumatic stress disorder in 4 postconflict settings. JAMA 2001, 286, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Mollica, R.F.; McInnes, K.; Pham, T.; Fawzi, M.C.; Murphy, E.; Lin, L. The dose-effect relationships between torture and psychiatric symptoms in Vietnamese ex-political detainees and a comparison group. J. Nerv. Ment. Dis. 1998, 186, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Hollifield, M. Taking measure of war trauma. Lancet 2005, 365, 1283–1284. [Google Scholar] [CrossRef]
- Steel, Z.; Silove, D.; Phan, T.; Bauman, A. Long-term effect of psychological trauma on the mental health of Vietnamese refugees resettled in Australia: A population-based study. Lancet 2002, 360, 1056–1062. [Google Scholar] [CrossRef]
- Gavagan, T.; Brodyaga, L. Medical Care for Immigrants and Refugees. Am. Fam. Phys. 1998, 57, 1061–1068. [Google Scholar]
- Wong, E.C.; Marshall, G.N.; Schell, T.L.; Elliott, M.N.; Babey, S.H.; Hambarsoomians, K. The unusually poor physical health status of Cambodian refugees two decades after resettlement. J. Immigr. Minority Health 2011, 13, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Westermeyer, J.; Tou, F.V.; Neider, J. Symptom change over time among Hmong refugees: Psychiatric patients versus nonpatients. Psychopathology 1984, 17, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Desjarlais, R. World Mental Health Problems, Priorities, and Responses in Low Income Countries; Oxford University Press: New York, NY, USA, 1995. [Google Scholar]
- Fullilove, M. Psychiatric implications of displacement: Contributions for the psychology of place. Am. J. Psychiatry 1996, 153, 1516–1523. [Google Scholar] [PubMed]
- Palinkas, L.A.; Pickwell, S.M. Acculturation as a risk factor for chronic disease among Cambodian refugees in the United States. Soc. Sci. Med. 1995, 40, 1643–1653. [Google Scholar] [CrossRef]
- Vergne, D.E.; Nemeroff, C.B. The interaction of serotonin transporter gene polymorphisms and early adverse life events on vulnerability for major depression. Curr. Psychiatry Rep. 2006, 8, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Başoğlu, M.; Mineka, S.; Paker, M.; Aker, T.; Livanou, M.; Gök, Ş. Psychological preparedness for trauma as a protective factor in survivors of torture. Psychol. Med. 1997, 27, 1421–1433. [Google Scholar] [CrossRef] [PubMed]
- Schumm, J.A.; Briggs-Phillips, M.; Hobfoll, S.E. Cumulative interpersonal traumas and social support as risk and resiliency factors in predicting PTSD and depression among inner-city women. J. Trauma. Stress 2006, 19, 825–836. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Item | Item Response “Serious” or “Very Serious”, Number (%) | Item Score, Mean (SD) ** | ||
|---|---|---|---|---|
| Kurds (n = 117) | VN (n = 135) | Kurds (n = 117) | VN (n = 135) | |
| Interviews by immigration | 17 (15) | 9 (7) | 0.95 (1.27) | 0.47 (0.92) |
| Conflict with immigration officials | 16 (14) | 2 (1) | 0.80 (1.25) | 0.12 (0.52) |
| No permission to work | 14 (12) | 1 (1) | 0.68 (1.24) | 0.07 (0.35) |
| Fears of being sent home | 24 (21) | 6 (4) | 1.03 (1.50) | 0.22 (0.79) |
| Worries about not getting health treatment | 34 (29) | 7 (5) | 1.44 (1.53) | 0.33 (0.82) |
| Poor access to emergency medical care | 37 (32) | 6 (4) | 1.44 (1.56) | 0.35 (0.88) |
| Poor access to long-term medical care | 37 (32) | 6 (4) | 1.44 (1.53) | 0.42 (0.92) |
| Poor access to dentistry care | 45 (38) | 11 (8) | 1.76 (1.56) | 0.60 (1.05) |
| Poor access to counseling services | 31 (26) | 11 (8) | 1.33 (1.47) | 0.56 (1.04) |
| Little government help with welfare | 32 (27) | 10 (7) | 1.48 (1.59) | 0.62 (1.05) |
| Little help with welfare from charities | 29 (25) | 11 (8) | 1.37 (1.53) | 0.54 (1.03) |
| Delays in processing your application | 36 (31) | 9 (7) | 1.58 (1.53) | 0.46 (1.02) |
| Separation from family | 55 (47) | 7 (5) | 2.03 (1.63) | 0.33 (0.86) |
| Worries about family back at home | 78 (67) | 15 (11) | 2.79 (1.42) | 0.84. (1.18) |
| Unable to return home in emergency | 70 (60) | 13 (10) | 2.57 (1.49) | 0.59 (1.12) |
| Communication difficulties | 50 (43) | 9 (7) | 2.05 (1.53) | 0.43 (0.94) |
| Discrimination | 29 (25) | 8 (6) | 1.40 (1.49) | 0.56 (0.95) |
| Not being able to find work | 33 (28) | 9 (7) | 1.57 (1.49) | 0.62 (1.04) |
| Bad job conditions | 35 (30) | 4 (3) | 1.59 (1.45) | 0.36 (0.77) |
| Poverty | 32 (37) | 6 (4) | 1.53 (1.47) | 0.33 (0.87) |
| Loneliness and boredom | 45 (38) | 10 (7) | 1.92 (1.45) | 0.61 (1.07) |
| Isolation | 56 (48) | 6 (4) | 2.15 (1.52) | 0.24 (0.75) |
| Poor access to the foods you like | 16 (14) | 4 (3) | 0.98 (1.29) | 0.35 (0.79) |
| Non-War Non-Migration Trauma 1 | War-Related Trauma 2 | Post-Migration Stress 3 | PTSD 4 | Depression 5 | Anxiety 6 | |
|---|---|---|---|---|---|---|
| War-related Trauma 2 | 0.57 | - | - | - | - | - |
| Post-migration Stress 3 | 0.31 | 0.52 | - | - | - | - |
| PTSD 4 | 0.43 | 0.50 | 0.54 | - | - | - |
| Depression 5 | 0.39 | 0.47 | 0.46 | 0.74 | - | - |
| Anxiety 6 | 0.41 | 0.48 | 0.52 | 0.72 | 0.83 | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hollifield, M.; Warner, T.D.; Krakow, B.; Westermeyer, J. Mental Health Effects of Stress over the Life Span of Refugees. J. Clin. Med. 2018, 7, 25. https://doi.org/10.3390/jcm7020025
Hollifield M, Warner TD, Krakow B, Westermeyer J. Mental Health Effects of Stress over the Life Span of Refugees. Journal of Clinical Medicine. 2018; 7(2):25. https://doi.org/10.3390/jcm7020025
Chicago/Turabian StyleHollifield, Michael, Teddy D. Warner, Barry Krakow, and Joseph Westermeyer. 2018. "Mental Health Effects of Stress over the Life Span of Refugees" Journal of Clinical Medicine 7, no. 2: 25. https://doi.org/10.3390/jcm7020025
APA StyleHollifield, M., Warner, T. D., Krakow, B., & Westermeyer, J. (2018). Mental Health Effects of Stress over the Life Span of Refugees. Journal of Clinical Medicine, 7(2), 25. https://doi.org/10.3390/jcm7020025