Bidirectional Association between Nonalcoholic Fatty Liver Disease and Gallstone Disease: A Cohort Study

 ,
,
Abstract
1. Introduction
2. Methods
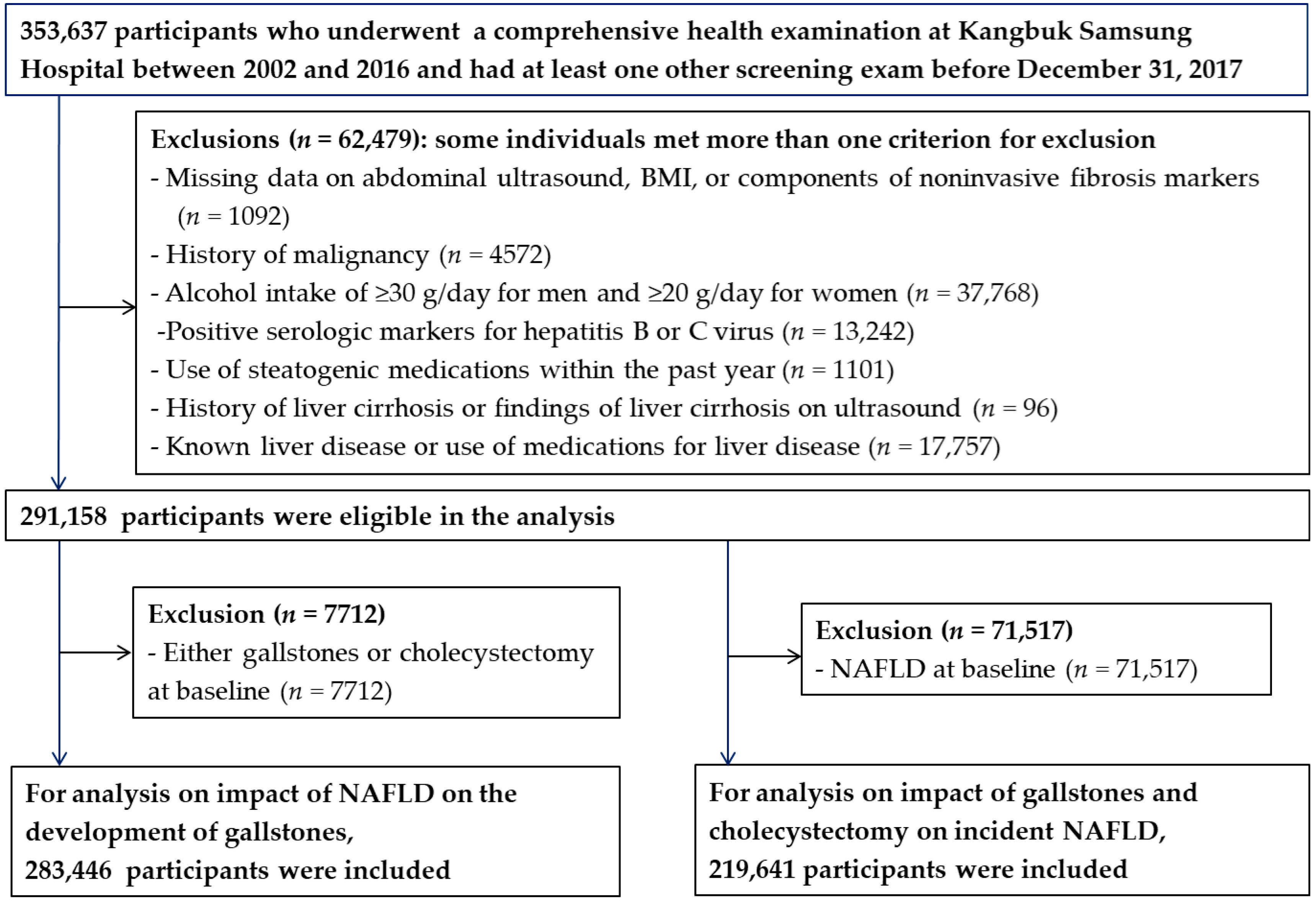
2.1. Study Population
2.2. Measurements
2.3. Statistical Analyses
2.3.1. Baseline NAFLD and Incident GD
2.3.2. Baseline Gallstone, Cholecystectomy and Incident NAFLD.
3. Results
3.1. Baseline NAFLD and Incident GD
3.2. Baseline Gallstone, Cholecystectomy and Incident NAFLD
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Number | Person-Years | Incident Case | Incidence Density (1000 Person-Years) | Age- and Sex-Adjusted HR a (95% CI) | Multivariate HR a (95% CI) | ||
|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | ||||||
| Men | |||||||
| BMI < 25 kg/m2 | |||||||
| No NAFLD | 72,546 | 473,899.9 | 1333 | 2.8 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 20,146 | 122,294.6 | 560 | 4.6 | 1.59 (1.44–1.75) | 1.53 (1.37–1.71) | 1.38 (1.22–1.56) |
| BMI ≥ 25 kg/m2 | |||||||
| No NAFLD | 20,382 | 131,432.8 | 540 | 4.1 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 35,519 | 217,114.3 | 1212 | 5.6 | 1.37 (1.24–1.52) | 1.37 (1.22–1.53) | 1.24 (1.10–1.40) |
| Women | |||||||
| BMI < 25 kg/m2 | |||||||
| No NAFLD | 112,024 | 635,857.6 | 1969 | 3.1 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 6230 | 32,165.6 | 168 | 5.2 | 1.70 (1.45–1.99) | 1.64 (1.37–1.97) | 1.36 (1.12–1.65) |
| BMI ≥ 25 kg/m2 | |||||||
| No NAFLD | 9494 | 54,555.3 | 338 | 6.2 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 7105 | 36,106.9 | 320 | 8.9 | 1.51 (1.30–1.76) | 1.42 (1.19–1.69) | 1.38 (1.14–1.66) |
Appendix B
| Number | Person-Years | Incident Case | Incidence Density (1000 Person-Year) | Age- and Sex-Adjusted HR a (95% CI) | Multivariate HR a (95% CI) | ||
|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | ||||||
| Total | |||||||
| FLI <30 | 142,201 | 686,999.9 | 2197 | 3.2 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| FLI 30–<60 | 34,267 | 173,595.0 | 876 | 5.0 | 1.70 (1.55–1.85) | 1.31 (1.17–1.46) | 1.22 (1.08–1.38) |
| FLI ≥60 | 18,198 | 89,353.3 | 572 | 6.4 | 2.25 (2.03–2.49) | 1.47 (1.27–1.71) | 1.29 (1.08–1.54) |
| p for trend | <0.001 | <0.001 | 0.002 | ||||
| Men | |||||||
| FLI <30 | 52,982 | 272,555.5 | 795 | 2.9 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| FLI 30–<60 | 29,360 | 152,751.1 | 712 | 4.7 | 1.51 (1.36–1.67) | 1.29 (1.13–1.48) | 1.21 (1.05–1.41) |
| FLI ≥60 | 16,556 | 82,794.1 | 491 | 5.9 | 1.98 (1.77–2.21) | 1.52 (1.27–1.82) | 1.30 (1.04–1.63) |
| p for trend | <0.001 | <0.001 | 0.013 | ||||
| Women | |||||||
| FLI <30 | 89,219 | 414,444.4 | 1402 | 3.3 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| FLI 30–<60 | 4907 | 20,843.9 | 164 | 7.8 | 2.36 (2.00–2.79) | 1.38 (1.11–1.71) | 1.24 (0.98–1.56) |
| FLI ≥60 | 1642 | 6559.2 | 81 | 12.3 | 3.83 (3.05–4.81) | 1.46 (1.05–2.04) | 1.31 (0.91–1.89) |
| p for trend | <0.001 | 0.004 | 0.074 | ||||
Appendix C
| Number | Person-Years | Incident Case | Incidence Density (1000 Person-Year) | Age- and Sex-Adjusted HR a (95% CI) | Multivariate HR a (95% CI) | ||
|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | ||||||
| Gallstone or cholecystecomty | |||||||
| Total | |||||||
| No NAFLD | 214,446 | 1,299,654.6 | 4927 | 3.8 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 69,000 | 409,552.0 | 2612 | 6.4 | 1.73 (1.64–1.82) | 1.28 (1.20–1.37) | 1.24 (1.16–1.33) |
| Men | |||||||
| No NAFLD | 92,928 | 607,142.6 | 2207 | 3.6 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 55,665 | 340,888.9 | 2036 | 6.0 | 1.63 (1.53–1.73) | 1.29 (1.20–1.39) | 1.23 (1.14–1.34) |
| Women | |||||||
| No NAFLD | 121,518 | 692,512.0 | 2720 | 3.9 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 13,335 | 68,663.1 | 576 | 8.4 | 2.11 (1.93–2.32) | 1.33 (1.18–1.50) | 1.28 (1.13–1.45) |
| Cholecystectomy | |||||||
| Total | |||||||
| No NAFLD | 214,446 | 1,311,709.6 | 1150 | 0.9 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 69,000 | 415,994.8 | 556 | 1.3 | 1.56 (1.40–1.74) | 1.10 (0.96–1.26) | 1.10 (0.95–1.27) |
| Men | |||||||
| No NAFLD | 92,928 | 613,204.5 | 543 | 0.9 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 55,665 | 346,147.1 | 424 | 1.2 | 1.40 (1.24–1.59) | 1.06 (0.90–1.25) | 1.04 (0.88–1.24) |
| Women | |||||||
| No NAFLD | 121,518 | 698,505.0 | 607 | 0.9 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 13,335 | 69,847.7 | 132 | 1.9 | 2.03 (1.67–2.47) | 1.30 (1.01–1.68) | 1.26 (0.96–1.64) |
Appendix D
| Multivariable-Adjusted Odds Ratios (95% CI) for NAFLD | Multivariable-Adjusted Odds Ratios (95% CI) for GD | |
|---|---|---|
| Age per 10-year increment | 1.16 (1.14–1.19) | 1.71 (1.65–1.76) |
| Male | 2.49 (2.40–2.59) | 0.61 (0.56–0.66) |
| Suwon center | 1.38 (1.34–1.41) | 1.04 (0.98–1.11) |
| year of screening exam per 1-year | 1.06 (1.05–1.06) | 1.04 (1.03–1.05) |
| Education level ≥ college graduate | 1.15 (1.11–1.19) | 1.31 (1.22–1.42) |
| Alcohol intake | ||
| <10 g of ethanol per day | 0.88 (0.85–0.91) | 0.95 (0.89–1.02) |
| ≥10 g of ethanol per day | 0.72 (0.69–0.75) | 0.86 (0.79–0.94) |
| Smoking | ||
| Ever smoker | 1.01 (0.97–1.05) | 1.08 (0.99–1.19) |
| Never smoker | 0.93 (0.89–0.96) | 1.13 (1.04–1.24) |
| Vigorous exercise ≥ 3 times per week | 0.82 (0.79–0.85) | 0.99 (0.91–1.07) |
| History of hypertension | 1.10 (1.05–1.16) | 0.96 (0.86–1.06) |
| History of diabetes | 1.82 (1.65–2.02) | 1.01 (0.85–1.20) |
| Medication for dyslipidemia | 1.62 (1.44–1.83) | 0.89 (0.72–1.10) |
| BMI per 1 SD increment | 2.74 (2.69–2.79) | 1.23 (1.19–1.27) |
| LDL-C per 1 SD increment | 1.33 (1.32–1.35) | 0.96 (0.93–0.99) |
| HDL-C per 1 SD increment | 0.73 (0.72–0.74) | 0.93 (0.90–0.96) |
| TC per 1 SD increment | 1.59 (1.57–1.62) | 0.93 (0.89–0.96) |
| HOMA-IR per 1 SD increment | 1.71 (1.68–1.74) | 1.15 (1.11–1.18) |
| hsCRP per 1 SD increment | 1.30 (1.28–1.31) | 1.14 (1.11–1.18) |
References
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American gastroenterological association, American association for the study of liver diseases, and American college of gastroenterology. Gastroenterology 2012, 142, 1592–1609. [Google Scholar] [CrossRef] [PubMed]
- Neuschwander-Tetri, B.A.; Caldwell, S.H. Nonalcoholic steatohepatitis: Summary of an AASLD single topic conference. Hepatology 2003, 37, 1202–1219. [Google Scholar] [CrossRef] [PubMed]
- Nascimbeni, F.; Ballestri, S.; Machado, M.V.; Mantovani, A.; Cortez-Pinto, H.; Targher, G.; Lonardo, A. Clinical relevance of liver histopathology and different histological classifications of NASH in adults. Expert. Rev. Gastroenterol. Hepatol. 2018, 12, 351–367. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Henry, L. Contribution of alcoholic and nonalcoholic fatty liver disease to the burden of liver-related morbidity and mortality. Gastroenterology 2016, 150, 1778–1785. [Google Scholar] [CrossRef] [PubMed]
- Anstee, Q.M.; Targher, G.; Day, C.P. Progression of NAFLD to diabetes mellitus, cardiovascular disease or cirrhosis. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Nascimbeni, F.; Romagnoli, D.; Lonardo, A. The independent predictors of non-alcoholic steatohepatitis and its individual histological features: Insulin resistance, serum uric acid, metabolic syndrome, alanine aminotransferase and serum total cholesterol are a clue to pathogenesis and candidate targets for treatment. Hepatol. Res. 2016, 46, 1074–1087. [Google Scholar] [PubMed]
- Ballestri, S.; Zona, S.; Targher, G.; Romagnoli, D.; Baldelli, E.; Nascimbeni, F.; Roverato, A.; Guaraldi, G.; Lonardo, A. Nonalcoholic fatty liver disease is associated with an almost twofold increased risk of incident type 2 diabetes and metabolic syndrome. Evidence from a systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2016, 31, 936–944. [Google Scholar] [CrossRef] [PubMed]
- Italian Association for the Study of the Liver. AISF position paper on nonalcoholic fatty liver disease (NAFLD): Updates and future directions. Dig. Liver Dis. 2017, 49, 471–483. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Nascimbeni, F.; Mantovani, A.; Targher, G. Hypertension, diabetes, atherosclerosis and NASH: Cause or consequence? J. Hepatol. 2018, 68, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Vanni, E.; Bugianesi, E.; Kotronen, A.; De Minicis, S.; Yki-Jarvinen, H.; Svegliati-Baroni, G. From the metabolic syndrome to NAFLD or vice versa? Dig. Liver Dis. 2010, 42, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Yki-Jarvinen, H. Non-alcoholic fatty liver disease as a cause and a consequence of metabolic syndrome. Lancet. Diabetes Endocrinol. 2014, 2, 901–910. [Google Scholar] [CrossRef]
- Di Ciaula, A.; Wang, D.Q.; Portincasa, P. An update on the pathogenesis of cholesterol gallstone disease. Curr. Opin. Gastroenterol. 2018, 34, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Loria, P.; Lonardo, A.; Lombardini, S.; Carulli, L.; Verrone, A.; Ganazzi, D.; Rudilosso, A.; D’Amico, R.; Bertolotti, M.; Carulli, N. Gallstone disease in non-alcoholic fatty liver: Prevalence and associated factors. J. Gastroenterol. Hepatol. 2005, 20, 1176–1184. [Google Scholar] [CrossRef] [PubMed]
- Ramos-De la Medina, A.; Remes-Troche, J.M.; Roesch-Dietlen, F.B.; Perez-Morales, A.G.; Martinez, S.; Cid-Juarez, S. Routine liver biopsy to screen for nonalcoholic fatty liver disease (NAFLD) during cholecystectomy for gallstone disease: Is it justified? J. Gastrointest. Surg. 2008, 12, 2097–2102. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.S.; Gong, J.J.; Wang, X.W.; Chen, L.; Qin, S.; Huang, L.F.; Chen, Y.Q.; Ren, H.; Yang, Q.B.; Hu, H.D. Promotional effect of nonalcoholic fatty liver disease on Gallstone disease: A systematic review and meta-analysis. Turk. J. Gastroenterol. 2017, 28, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Jaruvongvanich, V.; Sanguankeo, A.; Upala, S. Significant association between gallstone disease and nonalcoholic fatty liver disease: A systematic review and meta-analysis. Dig. Dis. Sci. 2016, 61, 2389–2396. [Google Scholar] [CrossRef] [PubMed]
- Marchesini, G.; Bugianesi, E.; Forlani, G.; Cerrelli, F.; Lenzi, M.; Manini, R.; Natale, S.; Vanni, E.; Villanova, N.; Melchionda, N.; et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology 2003, 37, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Nervi, F.; Arrese, M. Cholecystectomy and NAFLD: Does gallbladder removal have metabolic consequences? Am. J. Gastroenterol. 2013, 108, 959–961. [Google Scholar] [CrossRef] [PubMed]
- Biddinger, S.B.; Haas, J.T.; Yu, B.B.; Bezy, O.; Jing, E.; Zhang, W.; Unterman, T.G.; Carey, M.C.; Kahn, C.R. Hepatic insulin resistance directly promotes formation of cholesterol gallstones. Nat. Med. 2008, 14, 778–782. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.H.; Ali, A. Nonalcoholic fatty liver disease and cholesterol gallstones: Which comes first? Scand. J. Gastroenterol. 2014, 49, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.C.; Wilson, A.M.; Slavin, J.; Best, J.D.; Jenkins, A.J.; Desmond, P.V. Associations between liver histology and severity of the metabolic syndrome in subjects with nonalcoholic fatty liver disease. Diabetes Care 2005, 28, 1222–1224. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.Y.; Hsu, C.T.; Liu, J.H.; Tung, T.H. Clinical predictors of incident gallstone disease in a Chinese population in Taipei, Taiwan. BMC Gastroenterol. 2014, 14, 83. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Lin, H.; Zhang, C.; Wang, L.; Wu, S.; Zhang, D.; Tang, F.; Xue, F.; Liu, Y. Non-alcoholic fatty liver disease associated with gallstones in females rather than males: A longitudinal cohort study in Chinese urban population. BMC Gastroenterol. 2014, 14, 213. [Google Scholar] [CrossRef] [PubMed]
- Housset, C.; Chretien, Y.; Debray, D.; Chignard, N. Functions of the gallbladder. Compr. Physiol. 2016, 6, 1549–1577. [Google Scholar] [PubMed]
- Chang, Y.; Jung, H.S.; Cho, J.; Zhang, Y.; Yun, K.E.; Lazo, M.; Pastor-Barriuso, R.; Ahn, J.; Kim, C.W.; Rampal, S.; et al. Metabolically Healthy obesity and the development of nonalcoholic fatty liver disease. Am. J. Gastroenterol. 2016, 111, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Cho, Y.K.; Kim, Y.; Sung, E.; Ahn, J.; Jung, H.S.; Yun, K.E.; Shin, H.; Ryu, S. Non-heavy drinking and worsening of non-invasive fibrosis markers in nonalcoholic fatty liver disease: A cohort study. Hepatology 2018. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia Pty Limited: Sydney, Australia, 2000. [Google Scholar]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef] [PubMed]
- McPherson, S.; Stewart, S.F.; Henderson, E.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. Simple non-invasive fibrosis scoring systems can reliably exclude advanced fibrosis in patients with non-alcoholic fatty liver disease. Gut 2010, 59, 1265–1269. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.G.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J. Comparison of noninvasive markers of fibrosis in patients with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Wai, C.T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Mathiesen, U.L.; Franzen, L.E.; Aselius, H.; Resjo, M.; Jacobsson, L.; Foberg, U.; Fryden, A.; Bodemar, G. Increased liver echogenicity at ultrasound examination reflects degree of steatosis but not of fibrosis in asymptomatic patients with mild/moderate abnormalities of liver transaminases. Dig. Liver Dis. 2002, 34, 516–522. [Google Scholar] [CrossRef]
- Everhart, J.E.; Khare, M.; Hill, M.; Maurer, K.R. Prevalence and ethnic differences in gallbladder disease in the United States. Gastroenterology 1999, 117, 632–639. [Google Scholar] [CrossRef]
- Royston, P.; Parmar, M.K. Flexible parametric proportional-hazards and proportional-odds models for censored survival data, with application to prognostic modelling and estimation of treatment effects. Stat. Med. 2002, 21, 2175–2197. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Diggory, R. Acalculous gallbladder disease: The outcomes of treatment by laparoscopic cholecystectomy. Ann. R. Coll. Surg. Engl. 2011, 93, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Schwesinger, W.H.; Diehl, A.K. Changing indications for laparoscopic cholecystectomy. Stones without symptoms and symptoms without stones. Surg. Clin. North Am. 1996, 76, 493–504. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The fatty liver index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [PubMed]
- Arrese, M.; Cortes, V.; Barrera, F.; Nervi, F. Nonalcoholic fatty liver disease, cholesterol gallstones, and cholecystectomy: New insights on a complex relationship. Curr. Opin. Gastroenterol. 2018, 34, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Wu, J.S.; Yang, Y.C.; Chang, C.S.; Lu, F.H.; Chang, C.J. Moderate to severe, but not mild, nonalcoholic fatty liver disease associated with increased risk of gallstone disease. Scand. J. Gastroenterol. 2014, 49, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Q.H.; Zhu, W.H.; Yu, Y.X.; Huang, F.F.; Chen, L.Y. Nonalcoholic fatty liver was associated with asymptomatic gallstones in a Chinese population. Medicine (Baltimore) 2017, 96, e7853. [Google Scholar] [CrossRef] [PubMed]
- Fracanzani, A.L.; Valenti, L.; Russello, M.; Miele, L.; Bertelli, C.; Bellia, A.; Masetti, C.; Cefalo, C.; Grieco, A.; Marchesini, G.; et al. Gallstone disease is associated with more severe liver damage in patients with non-alcoholic fatty liver disease. PLoS ONE 2012, 7, e41183. [Google Scholar] [CrossRef] [PubMed]
- Qin, J.-J.; Ding, W.-J. Nonalcoholic fatty liver disease and its relevant factors increased the risk of gallstone disease: A systematic review and meta-analysis. Int. J. Clin. Exp. Med. 2016, 9, 3009–3016. [Google Scholar]
- Cortes, V.; Quezada, N.; Uribe, S.; Arrese, M.; Nervi, F. Effect of cholecystectomy on hepatic fat accumulation and insulin resistance in non-obese Hispanic patients: A pilot study. Lipids Health Dis. 2017, 16, 129. [Google Scholar] [CrossRef] [PubMed]
- Seppala-Lindroos, A.; Vehkavaara, S.; Hakkinen, A.M.; Goto, T.; Westerbacka, J.; Sovijarvi, A.; Halavaara, J.; Yki-Jarvinen, H. Fat accumulation in the liver is associated with defects in insulin suppression of glucose production and serum free fatty acids independent of obesity in normal men. J. Clin. Endocrinol. Metab. 2002, 87, 3023–3028. [Google Scholar] [CrossRef] [PubMed]
- Feldman, A.; Eder, S.K.; Felder, T.K.; Kedenko, L.; Paulweber, B.; Stadlmayr, A.; Huber-Schonauer, U.; Niederseer, D.; Stickel, F.; Auer, S.; et al. Clinical and metabolic characterization of lean Caucasian subjects with non-alcoholic fatty liver. Am. J. Gastroenterol. 2017, 112, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.Y.; Qiao, Q.H.; Zhang, S.C.; Chen, Y.H.; Chao, G.Q.; Fang, L.Z. Metabolic syndrome and gallstone disease. World J. Gastroenterol. 2012, 18, 4215–4220. [Google Scholar] [CrossRef] [PubMed]
- Simonen, P.; Kotronen, A.; Hallikainen, M.; Sevastianova, K.; Makkonen, J.; Hakkarainen, A.; Lundbom, N.; Miettinen, T.A.; Gylling, H.; Yki-Jarvinen, H. Cholesterol synthesis is increased and absorption decreased in non-alcoholic fatty liver disease independent of obesity. J. Hepatol. 2011, 54, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Min, H.K.; Kapoor, A.; Fuchs, M.; Mirshahi, F.; Zhou, H.; Maher, J.; Kellum, J.; Warnick, R.; Contos, M.J.; Sanyal, A.J. Increased hepatic synthesis and dysregulation of cholesterol metabolism is associated with the severity of nonalcoholic fatty liver disease. Cell Metab. 2012, 15, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Halldestam, I.; Kullman, E.; Borch, K. Incidence of and potential risk factors for gallstone disease in a general population sample. Br. J. Surg. 2009, 96, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, E.A. Epidemiology and risk factors for gallstone disease: Has the paradigm changed in the 21st century? Curr. Gastroenterol. Rep. 2005, 7, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, E.A. Gallstone disease: Epidemiology of gallbladder stone disease. Best Pract. Res. Clin. Gastroenterol. 2006, 20, 981–996. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.H.; Lim, B.C.; Myung, S.J.; Lee, S.K.; Ohrr, H.C.; Kim, Y.T.; Roe, I.H.; Kim, J.H.; Chung, J.B.; Kim, C.D.; et al. Epidemiological study on Korean gallstone disease: A nationwide cooperative study. Dig. Dis. Sci. 1999, 44, 1674–1683. [Google Scholar] [CrossRef] [PubMed]
- Musso, G.; Gambino, R.; Cassader, M. Recent insights into hepatic lipid metabolism in non–alcoholic fatty liver disease (NAFLD). Prog. Lipid Res. 2009, 48, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Almond, H.R.; Vlahcevic, Z.R.; Bell, C.C.Jr.; Gregory, D.H.; Swell, L. Bile acid pools, kinetics and biliary lipid composition before and after cholecystectomy. N. Engl. J. Med. 1973, 289, 1213–1216. [Google Scholar] [CrossRef] [PubMed]
- Trauner, M.; Claudel, T.; Fickert, P.; Moustafa, T.; Wagner, M. Bile acids as regulators of hepatic lipid and glucose metabolism. Dig. Dis. 2010, 28, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.; Zollner, G.; Trauner, M. Nuclear receptors in liver disease. Hepatology 2011, 53, 1023–1034. [Google Scholar] [CrossRef] [PubMed]
- Barrera, F.; Azocar, L.; Molina, H.; Schalper, K.A.; Ocares, M.; Liberona, J.; Villarroel, L.; Pimentel, F.; Perez-Ayuso, R.M.; Nervi, F.; et al. Effect of cholecystectomy on bile acid synthesis and circulating levels of fibroblast growth factor 19. Ann. Hepatol. 2015, 14, 710–721. [Google Scholar] [PubMed]
- Ruhl, C.E.; Everhart, J.E. Relationship of non-alcoholic fatty liver disease with cholecystectomy in the US population. Am. J. Gastroenterol. 2013, 108, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Zweers, S.J.; Booij, K.A.; Komuta, M.; Roskams, T.; Gouma, D.J.; Jansen, P.L.; Schaap, F.G. The human gallbladder secretes fibroblast growth factor 19 into bile: Towards defining the role of fibroblast growth factor 19 in the enterobiliary tract. Hepatology 2012, 55, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, S.; Damron, H.A.; Hillgartner, F.B. Fibroblast growth factor-19, a novel factor that inhibits hepatic fatty acid synthesis. J. Biol. Chem. 2009, 284, 10023–10033. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; John, L.M.; Adams, S.H.; Yu, X.X.; Tomlinson, E.; Renz, M.; Williams, P.M.; Soriano, R.; Corpuz, R.; Moffat, B.; et al. Fibroblast growth factor 19 increases metabolic rate and reverses dietary and leptin-deficient diabetes. Endocrinology 2004, 145, 2594–2603. [Google Scholar] [CrossRef] [PubMed]
- Kullak-Ublick, G.A.; Paumgartner, G.; Berr, F. Long-term effects of cholecystectomy on bile acid metabolism. Hepatology 1995, 21, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Alisi, A.; Ceccarelli, S.; Panera, N.; Prono, F.; Petrini, S.; De Stefanis, C.; Pezzullo, M.; Tozzi, A.; Villani, A.; Bedogni, G.; et al. Association between serum atypical fibroblast growth factors 21 and 19 and pediatric nonalcoholic fatty liver disease. PLoS ONE 2013, 8, e67160. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Lonardo, A. NAFLD as a sexual dimorphic disease: Role of gender and reproductive status in the development and progression of nonalcoholic fatty liver disease and inherent cardiovascular risk. Adv. Ther. 2017, 34, 1291–1326. [Google Scholar] [CrossRef] [PubMed]
- Lammert, F.; Gurusamy, K.; Ko, C.W.; Miquel, J.F.; Mendez-Sanchez, N.; Portincasa, P.; van Erpecum, K.J.; van Laarhoven, C.J.; Wang, D.Q. Gallstones. Nat. Rev. Dis. Primers. 2016, 2, 16024. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Chang, C.H.; Wang, J.L.; Kuo, H.K.; Lin, J.W.; Shau, W.Y.; Lee, P.H. Nationwide epidemiological study of severe gallstone disease in Taiwan. BMC Gastroenterol. 2009, 9, 63. [Google Scholar] [CrossRef] [PubMed]
- Key, T.J.; Appleby, P.N.; Reeves, G.K.; Roddam, A.; Dorgan, J.F.; Longcope, C.; Stanczyk, F.Z.; Stephenson, H.E.Jr.; Falk, R.T.; Miller, R.; et al. Body mass index, serum sex hormones, and breast cancer risk in postmenopausal women. J. Natl. Cancer Inst. 2003, 95, 1218–1226. [Google Scholar] [PubMed]
- Stender, S.; Nordestgaard, B.G.; Tybjaerg-Hansen, A. Elevated body mass index as a causal risk factor for symptomatic gallstone disease: A mendelian randomization study. Hepatology 2013, 58, 2133–2141. [Google Scholar] [CrossRef] [PubMed]
- Cirillo, D.J.; Wallace, R.B.; Rodabough, R.J.; Greenland, P.; LaCroix, A.Z.; Limacher, M.C.; Larson, J.C. Effect of estrogen therapy on gallbladder disease. JAMA 2005, 293, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Mamdani, M.M.; Tu, K.; van Walraven, C.; Austin, P.C.; Naylor, C.D. Postmenopausal estrogen replacement therapy and increased rates of cholecystectomy and appendectomy. CMAJ 2000, 162, 1421–1424. [Google Scholar] [PubMed]
- Clark, J.M.; Diehl, A.M. Defining nonalcoholic fatty liver disease: Implications for epidemiologic studies. Gastroenterology 2003, 124, 248–250. [Google Scholar] [CrossRef] [PubMed]
- Portincasa, P.; Moschetta, A.; Palasciano, G. Cholesterol gallstone disease. Lancet 2006, 368, 230–239. [Google Scholar] [CrossRef]

| Characteristic | Men (n = 148,593) | p Value | Women (n = 134,853) | p Value | ||
|---|---|---|---|---|---|---|
| No Incident Gallstones | Incident Gallstones | No Incident Gallstones | Incident Gallstones | |||
| Number | 144,948 | 3645 | 132,058 | 2795 | ||
| Age (years) a | 37.0 (7.8) | 37.9 (8.3) | <0.001 | 36.9 (8.3) | 36.8 (7.7) | 0.260 |
| Current smoker (%) | 38.0 | 40.4 | 0.004 | 2.2 | 2.5 | 0.303 |
| Alcohol intake (%) b | 45.1 | 40.5 | <0.001 | 7.4 | 6.0 | 0.007 |
| Vigorous exercise (%) c | 15.0 | 12.8 | <0.001 | 12.7 | 11.8 | 0.141 |
| Higher education (%) d | 86.8 | 85.9 | 0.210 | 72.5 | 71.1 | 0.141 |
| Fatty liver (%) | 37.2 | 48.6 | <0.001 | 9.7 | 17.5 | <0.001 |
| Diabetes mellitus (%) | 3.0 | 4.0 | <0.001 | 1.4 | 2.0 | 0.008 |
| Hypertension (%) | 15.2 | 19.0 | <0.001 | 5.6 | 7.5 | <0.001 |
| Medication for dyslipidemia (%) | 1.2 | 1.3 | 0.490 | 0.9 | 0.7 | 0.303 |
| Obesity (%) | 37.4 | 48.1 | <0.001 | 12.1 | 23.5 | <0.001 |
| BMI (kg/m2) | 24.3 (2.9) | 25.1 (3.0) | <0.001 | 21.7 (2.9) | 22.8 (3.6) | <0.001 |
| Systolic BP (mmHg) a | 115.9 (12.2) | 117.3 (12.4) | <0.001 | 105.3 (12.8) | 107.8 (14.0) | <0.001 |
| Diastolic BP (mmHg) a | 74.9 (9.3) | 76.4 (9.4) | <0.001 | 67.1 (9.0) | 68.7 (9.7) | <0.001 |
| Glucose (mg/dL) a | 95.2 (14.7) | 96.4 (16.9) | <0.001 | 90.9 (11.5) | 92.4 (13.7) | <0.001 |
| Total cholesterol (mg/ dL) a | 197.8 (34.2) | 201.7 (36.0) | <0.001 | 185.8 (32.8) | 187.3 (34.2) | 0.022 |
| LDL-C (mg/ dL) a | 121.5 (30.2) | 123.0 (30.8) | 0.002 | 106.1 (28.5) | 108.0 (29.5) | <0.001 |
| HDL-C (mg/ dL) a | 52.2 (11.5) | 49.9 (10.7) | <0.001 | 63.0 (14.1) | 59.4 (13.4) | <0.001 |
| Triglycerides (mg/ dL) e | 116 (82–166) | 129 (93–186) | <0.001 | 73 (56–100) | 82 (60–116) | <0.001 |
| Albumin (g/dL) a | 4.7 (0.2) | 4.6 (0.2) | <0.001 | 4.5 (0.2) | 4.5 (0.2) | 0.342 |
| AST (U/L) e | 23 (19–28) | 24 (20–29) | <0.001 | 18 (16–22) | 19 (16–22) | <0.001 |
| ALT (U/L) e | 24 (18–35) | 28 (20–41) | <0.001 | 14 (11–18) | 15 (12–20) | <0.001 |
| GGT (U/L) e | 26 (18–41) | 31 (20–48) | <0.001 | 12 (9–16) | 13 (10–19) | <0.001 |
| hsCRP (mg/L) e | 0.5 (0.3–1.0) | 0.7 (0.4–1.3) | <0.001 | 0.3 (0.1–0.7) | 0.4 (0.2–1.0) | <0.001 |
| HOMA-IR e | 1.6 (1.1–2.2) | 1.9 (1.3–2.5) | <0.001 | 1.4 (0.9–2.0) | 1.7 (1.2–2.3) | <0.001 |
| Number | Person-Years | Incident Case | Incidence Density (1000 Person-Year) | Age- and Sex-Adjusted HR a (95% CI) | Multivariate HR a (95% CI) | ||
|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | ||||||
| Total (n = 283,446) | |||||||
| No NAFLD | 214,446 | 1,295,745.6 | 4180 | 3.2 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 69,000 | 407,681.4 | 2260 | 5.5 | 1.77 (1.68–1.87) | 1.31 (1.22–1.40) | 1.26 (1.17–1.35) |
| Men (n = 148,593) | |||||||
| No NAFLD | 121,518 | 605,332.7 | 2307 | 3.1 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 13,335 | 339,409.0 | 488 | 5.2 | 1.67 (1.57–1.79) | 1.32 (1.22–1.43) | 1.26 (1.15–1.37) |
| Women (n = 134,853) | |||||||
| No. NAFLD | 92,928 | 690,412.9 | 1873 | 3.3 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD | 55,665 | 68,272.5 | 1772 | 7.1 | 2.17 (1.96–2.41) | 1.35 (1.18–1.53) | 1.28 (1.11–1.46) |
| Number | Person-Years | Incident Case | Incidence Density (1000 Person-Year) | Age- and sex-Adjusted HR a (95% CI) | Multivariate HR a (95% CI) | ||
|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | ||||||
| Based on NFS | |||||||
| No NAFLD | 214,446 | 1,295,745.6 | 4180 | 3.2 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD, Low NFS | 63,985 | 384,074.4 | 2056 | 5.4 | 1.73 (1.64–1.83) | 1.30 (1.21–1.39) | 1.25 (1.16–1.34) |
| NAFLD, Intermediate or high NFS | 5015 | 23,607.0 | 204 | 8.6 | 2.40 (2.07–2.78) | 1.54 (1.30–1.82) | 1.50 (1.26–1.78) |
| p for trend | <0.001 | <0.001 | <0.001 | ||||
| Based on FIB 4 | |||||||
| No NAFLD | 214,446 | 1,295,745.6 | 4180 | 3.2 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD, Low FIB 4 | 65,526 | 392,234.6 | 2157 | 5.5 | 1.77 (1.68–1.88) | 1.31 (1.23–1.41) | 1.26 (1.17–1.36) |
| NAFLD, Intermediate or high FIB 4 | 3474 | 15,446.8 | 103 | 6.7 | 1.68 (1.37–2.06) | 1.20 (0.95–1.51) | 1.21 (0.96–1.53) |
| p for trend | <0.001 | <0.001 | <0.001 | ||||
| Based on APRI | |||||||
| No NAFLD | 214,446 | 1,295,745.6 | 4180 | 3.2 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| NAFLD, Low APRI | 64,537 | 381,044.8 | 2101 | 5.5 | 1.76 (1.67–1.86) | 1.31 (1.22–1.40) | 1.26 (1.17–1.36) |
| NAFLD, Intermediate or high APRI | 4463 | 26,636.6 | 159 | 6.0 | 1.89 (1.61–2.22) | 1.31 (1.10–1.57) | 1.26 (1.05–1.50) |
| p for trend | <0.001 | <0.001 | <0.001 | ||||
| Number | Person-Years | Incident Case | Incidence Density (1000 Person-Year) | Age- And Sex-Adjusted HR a (95% CI) | Multivariate HR a (95% CI) | ||
|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | ||||||
| Total (n = 219,641) | |||||||
| No gallstone disease | 214,446 | 1,141,715.8 | 47,992 | 42.0 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Gallstone | 4073 | 19,015.1 | 1051 | 55.3 | 1.36 (1.28–1.44) | 1.16 (1.09–1.24) | 1.14 (1.07–1.22) |
| Cholecystectomy | 1122 | 4723.8 | 258 | 54.6 | 1.23 (1.09–1.39) | 1.10 (0.97–1.25) | 1.17 (1.03–1.33) |
| Men (n = 94,865) | |||||||
| No gallstone disease | 92,928 | 484,621.6 | 32,782 | 67.6 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Gallstone | 1494 | 6653.3 | 570 | 85.7 | 1.26 (1.16–1.37) | 1.12 (1.03–1.22) | 1.10 (1.01–1.20) |
| Cholecystectomy | 443 | 1763.4 | 154 | 87.3 | 1.29 (1.10–1.51) | 1.21 (1.04–1.42) | 1.29 (1.10–1.52) |
| Women (n = 124,776) | |||||||
| No gallstone disease | 121,518 | 657,094.2 | 15,210 | 23.1 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Gallstone | 2579 | 12,361.8 | 481 | 38.9 | 1.53 (1.40–1.68) | 1.23 (1.13–1.35) | 1.15 (1.05–1.27) |
| Cholecystectomy | 679 | 2960.5 | 104 | 35.1 | 1.17 (0.96–1.42) | 0.98 (0.80–1.19) | 1.05 (0.86–1.28) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.; Noh, Y.-H.; Suh, B.-S.; Kim, Y.; Sung, E.; Jung, H.-S.; Kim, C.-W.; Kwon, M.-J.; Yun, K.E.; Noh, J.-W.; et al. Bidirectional Association between Nonalcoholic Fatty Liver Disease and Gallstone Disease: A Cohort Study. J. Clin. Med. 2018, 7, 458. https://doi.org/10.3390/jcm7110458
Chang Y, Noh Y-H, Suh B-S, Kim Y, Sung E, Jung H-S, Kim C-W, Kwon M-J, Yun KE, Noh J-W, et al. Bidirectional Association between Nonalcoholic Fatty Liver Disease and Gallstone Disease: A Cohort Study. Journal of Clinical Medicine. 2018; 7(11):458. https://doi.org/10.3390/jcm7110458
Chicago/Turabian StyleChang, Yoosoo, Yoo-Hun Noh, Byung-Seong Suh, Yejin Kim, Eunju Sung, Hyun-Suk Jung, Chan-Won Kim, Min-Jung Kwon, Kyung Eun Yun, Jin-Won Noh, and et al. 2018. "Bidirectional Association between Nonalcoholic Fatty Liver Disease and Gallstone Disease: A Cohort Study" Journal of Clinical Medicine 7, no. 11: 458. https://doi.org/10.3390/jcm7110458
APA StyleChang, Y., Noh, Y.-H., Suh, B.-S., Kim, Y., Sung, E., Jung, H.-S., Kim, C.-W., Kwon, M.-J., Yun, K. E., Noh, J.-W., Shin, H., Cho, Y. K., & Ryu, S. (2018). Bidirectional Association between Nonalcoholic Fatty Liver Disease and Gallstone Disease: A Cohort Study. Journal of Clinical Medicine, 7(11), 458. https://doi.org/10.3390/jcm7110458