Remnant Lipoprotein Cholesterol and Cardiovascular and Cerebrovascular Events in Patients with Non-Alcoholic Fatty Liver Disease

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Cardiovascular Endpoints
Statistical Analysis
3. Results
3.1. Factors Associated to Levels of RLP-C above Median
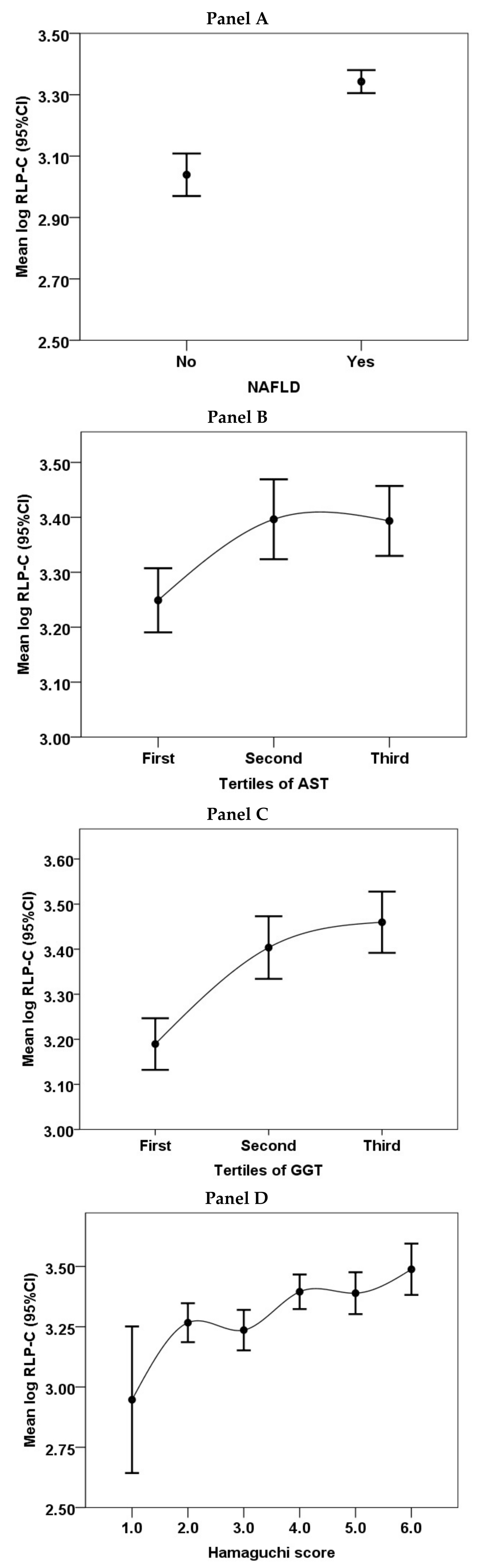
3.2. Subgroup of Patients with NAFLD
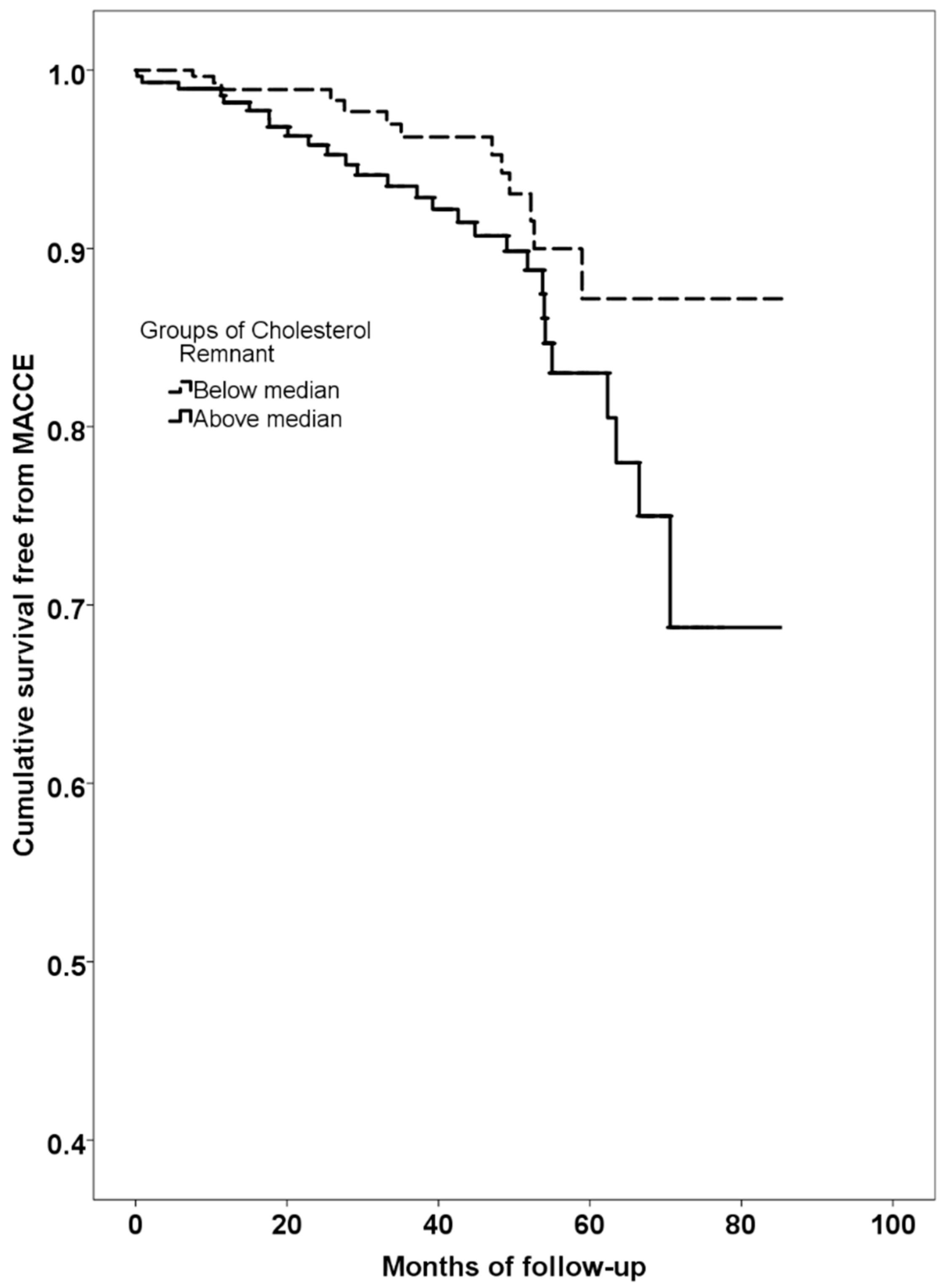
3.3. Predictors of MACCE
4. Discussion
Author Contributions
Conflicts of Interest
References
- Khan, R.S.; Newsome, P.N. Non-alcoholic fatty liver disease and liver transplantation. Metab. Clin. Exp. 2016, 65, 1208–1223. [Google Scholar] [CrossRef] [PubMed]
- Anstee, Q.M.; Mantovani, A.; Tilg, H.; Targher, G. Risk of cardiomyopathy and cardiac arrhythmias in patients with nonalcoholic fatty liver disease. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 425–439. [Google Scholar] [CrossRef] [PubMed]
- Angelico, F.; del Ben, M.; Conti, R.; Francioso, S.; Feole, K.; Fiorello, S.; Cavallo, M.G.; Zalunardo, B.; Lirussi, F.; Alessandri, C.; et al. Insulin resistance, the metabolic syndrome, and nonalcoholic fatty liver disease. J. Clin. Endocrinol. Metab. 2005, 90, 1578–1582. [Google Scholar] [CrossRef] [PubMed]
- Pastori, D.; Baratta, F.; Carnevale, R.; Cangemi, R.; del Ben, M.; Bucci, T.; Polimeni, L.; Labbadia, G.; Nocella, C.; Scardella, L.; et al. Similar reduction of cholesterol-adjusted vitamin e serum levels in simple steatosis and non-alcoholic steatohepatitis. Clin. Transl. Gastroenterol. 2015, 6, e113. [Google Scholar] [CrossRef] [PubMed]
- Pastori, D.; Loffredo, L.; Perri, L.; Baratta, F.; Scardella, L.; Polimeni, L.; Pani, A.; Brancorsini, M.; Albanese, F.; Catasca, E.; et al. Relation of nonalcoholic fatty liver disease and Framingham risk score to flow-mediated dilation in patients with cardiometabolic risk factors. Am. J. Cardiol. 2015, 115, 1402–1406. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Lonardo, A.; Bonapace, S.; Byrne, C.D.; Loria, P.; Targher, G. Risk of cardiovascular, cardiac and arrhythmic complications in patients with non-alcoholic fatty liver disease. World J. Gastroenterol. WJG 2014, 20, 1724–1745. [Google Scholar] [CrossRef] [PubMed]
- Polimeni, L.; del Ben, M.; Baratta, F.; Perri, L.; Albanese, F.; Pastori, D.; Violi, F.; Angelico, F. Oxidative stress: New insights on the association of non-alcoholic fatty liver disease and atherosclerosis. World J. Hepatol. 2015, 7, 1325–1336. [Google Scholar] [CrossRef] [PubMed]
- Chatrath, H.; Vuppalanchi, R.; Chalasani, N. Dyslipidemia in patients with nonalcoholic fatty liver disease. Semin. Liver Dis. 2012, 32, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Alkhouri, N.; Carter-Kent, C.; Elias, M.; Feldstein, A.E. Atherogenic dyslipidemia and cardiovascular risk in children with nonalcoholic fatty liver disease. Clin. Lipidol. 2011, 6, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Corey, K.E.; Chalasani, N. Management of dyslipidemia as a cardiovascular risk factor in individuals with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2014, 12, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- DeFilippis, A.P.; Blaha, M.J.; Martin, S.S.; Reed, R.M.; Jones, S.R.; Nasir, K.; Blumenthal, R.S.; Budoff, M.J. Nonalcoholic fatty liver disease and serum lipoproteins: The multi-ethnic study of atherosclerosis. Atherosclerosis 2013, 227, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Fujioka, Y.; Ishikawa, Y. Remnant lipoproteins as strong key particles to atherogenesis. J. Atheroscler. Thromb. 2009, 16, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Kugiyama, K.; Doi, H.; Takazoe, K.; Kawano, H.; Soejima, H.; Mizuno, Y.; Tsunoda, R.; Sakamoto, T.; Nakano, T.; Nakajima, K.; et al. Remnant lipoprotein levels in fasting serum predict coronary events in patients with coronary artery disease. Circulation 1999, 99, 2858–2860. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, H.; Sugiyama, S.; Honda, O.; Koide, S.; Nakamura, S.; Sakamoto, T.; Yoshimura, M.; Ogawa, H.; Fujioka, D.; Kugiyama, K. Prognostic value of remnant-like lipoprotein particle levels in patients with coronary artery disease and type ii diabetes mellitus. J. Am. Coll. Cardiol. 2004, 43, 2219–2224. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Obata, J.E.; Hirano, M.; Kitta, Y.; Fujioka, D.; Saito, Y.; Kawabata, K.; Watanabe, K.; Watanabe, Y.; Mishina, H.; et al. Predictive value of remnant lipoprotein for cardiovascular events in patients with coronary artery disease after achievement of ldl-cholesterol goals. Atherosclerosis 2011, 218, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.V.; Nakamura, T.; Kugiyama, K. High remnant lipoprotein predicts recurrent cardiovascular events on statin treatment after acute coronary syndrome. Circ. J. Off. J. Jpn. Circ. Soc. 2014, 78, 2492–2500. [Google Scholar] [CrossRef]
- Nguyen, S.V.; Nakamura, T.; Uematsu, M.; Fujioka, D.; Watanabe, K.; Watanabe, Y.; Obata, J.E.; Nakamura, K.; Kugiyama, K. Remnant lipoproteinemia predicts cardiovascular events in patients with type 2 diabetes and chronic kidney disease. J. Cardiol. 2017, 69, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, M.; Kojima, T.; Itoh, Y.; Harano, Y.; Fujii, K.; Nakajima, T.; Kato, T.; Takeda, N.; Okuda, J.; Ida, K.; et al. The severity of ultrasonographic findings in nonalcoholic fatty liver disease reflects the metabolic syndrome and visceral fat accumulation. Am. J. Gastroenterol. 2007, 102, 2708–2715. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D. Third universal definition of myocardial infarction. J. Am. Coll. Cardiol. 2012, 60, 1581–1598. [Google Scholar] [CrossRef] [PubMed]
- Special report from the national institute of neurological disorders and stroke. Special report from the national institute of neurological disorders and stroke. Classification of cerebrovascular diseases iii. Stroke J. Cereb. Circ. 1990, 21, 637–676. [Google Scholar] [CrossRef]
- Wu, S.; Wu, F.; Ding, Y.; Hou, J.; Bi, J.; Zhang, Z. Association of non-alcoholic fatty liver disease with major adverse cardiovascular events: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 33386. [Google Scholar] [CrossRef] [PubMed]
- Veronesi, G.; Ferrario, M.M.; Chambless, L.E.; Sega, R.; Mancia, G.; Corrao, G.; Fornari, C.; Cesana, G. Gender differences in the association between education and the incidence of cardiovascular events in northern italy. Eur. J. Public Health 2011, 21, 762–767. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.R.; Shah, P.K.; Nakajima, K.; Cupples, L.A.; Wilson, P.W.; Ordovas, J.M.; Schaefer, E.J. Remnant-like particle (rlp) cholesterol is an independent cardiovascular disease risk factor in women: Results from the framingham heart study. Atherosclerosis 2001, 154, 229–236. [Google Scholar] [CrossRef]
- Imke, C.; Rodriguez, B.L.; Grove, J.S.; McNamara, J.R.; Waslien, C.; Katz, A.R.; Willcox, B.; Yano, K.; Curb, J.D. Are remnant-like particles independent predictors of coronary heart disease incidence? The honolulu heart study. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1718–1722. [Google Scholar] [CrossRef] [PubMed]
- Nordestgaard, B.G.; Benn, M.; Schnohr, P.; Tybjaerg-Hansen, A. Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA: J. Am. Med. Assoc. 2007, 298, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Joshi, P.H.; Khokhar, A.A.; Massaro, J.M.; Lirette, S.T.; Griswold, M.E.; Martin, S.S.; Blaha, M.J.; Kulkarni, K.R.; Correa, A.; D’Agostino, R.B., Sr.; et al. Remnant lipoprotein cholesterol and incident coronary heart disease: The jackson heart and framingham offspring cohort studies. J. Am. Heart Assoc. 2016, 5, e002765. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Lonardo, A. Nafld as a sexual dimorphic disease: Role of gender and reproductive status in the development and progression of nonalcoholic fatty liver disease and inherent cardiovascular risk. Adv. Ther. 2017, 34, 1291–1326. [Google Scholar] [CrossRef] [PubMed]
- Treeprasertsuk, S.; Leverage, S.; Adams, L.A.; Lindor, K.D.; St Sauver, J.; Angulo, P. The framingham risk score and heart disease in nonalcoholic fatty liver disease. Liver Int. Off. J. Int. Assoc. Study Liver 2012, 32, 945–950. [Google Scholar] [CrossRef] [PubMed]
- McPherson, R. Remnant cholesterol: “Non-(hdl-c + ldl-c)” as a coronary artery disease risk factor. J. Am. Coll. Cardiol. 2013, 61, 437–439. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.T.; Devaraj, S.; Balis, D.; Adams-Huet, B.; Jialal, I. Effect of statin therapy on remnant lipoprotein cholesterol levels in patients with combined hyperlipidemia. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 2026–2031. [Google Scholar] [CrossRef] [PubMed]
- Pastori, D.; Polimeni, L.; Baratta, F.; Pani, A.; del Ben, M.; Angelico, F. The efficacy and safety of statins for the treatment of non-alcoholic fatty liver disease. Dig. Liver Dis. 2015, 47, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Ray, K.K.; Wiklund, O.; Corsini, A.; Catapano, A.L.; Bruckert, E.; de Backer, G.; Hegele, R.A.; Hovingh, G.K.; Jacobson, T.A.; et al. Adverse effects of statin therapy: Perception vs. The evidence—Focus on glucose homeostasis, cognitive, renal and hepatic function, haemorrhagic stroke and cataract. Eur. Heart J. 2018, 39, 2526–2539. [Google Scholar] [CrossRef] [PubMed]
- Imprialos, K.P.; Stavropoulos, K.; Doumas, M.; Skalkou, A.; Zografou, I.; Athyros, V.G. The potential role of statins in treating liver disease. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Del Ben, M.; Baratta, F.; Polimeni, L.; Pastori, D.; Loffredo, L.; Averna, M.; Violi, F.; Angelico, F. Under-prescription of statins in patients with non-alcoholic fatty liver disease. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 161–167. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Whole Population (n = 798) | Patients with RLP-C below Median (<25.5 mg/dL) (n = 399) | Patients with RLP-C above Median (≥25.5 mg/dL) (n = 399) | p | |
|---|---|---|---|---|
| Age (years) | 56.6 ± 12.8 | 58.1 ± 13.1 | 55.2 ± 12.4 | 0.002 |
| Women(%) | 37.3 | 41.4 | 33.3 | 0.023 |
| Body mass index (kg/m2) | 29.6 ± 5.0 | 29.1 ± 5.1 | 30.1 ± 4.9 | 0.004 |
| Waist circumference (cm) | 105.1 ± 12.2 | 103.6 ± 12.7 | 106.5 ± 11.7 | 0.001 |
| Total cholesterol (mg/dL) | 198.1 ± 41.1 | 188.4 ± 37.5 | 207.7 ± 42.4 | <0.001 |
| High density lipoprotein cholesterol (mg/dL) | 49.5 ± 14.0 | 54.6 ± 14.7 | 44.5 ± 11.4 | <0.001 |
| Low density lipoprotein cholesterol (mg/dL) | 118.8 ± 36.2 | 115.2 ± 33.4 | 122.4 ± 38.5 | 0.006 |
| Triglycerides (mg/dL) | 150.8 ± 101.2 | 95.7 ± 29.5 | 206.2 ± 116.4 | <0.001 |
| Alanine aminotransferase (IU/L) | 24.0 (17.0–39.0) | 22.0 (16.0–34.0) | 27.0 (20.0–42.0) | <0.001 |
| Aspartate aminotransferase (IU/L) | 21.0 (17.0–27.0) | 20.0 (16.0–25.0) | 22.0 (18.0–29) | <0.001 |
| Gamma-glutamyl transpeptidase (IU/L) | 25.0 (17.0–40.0) | 21.0 (16.0–33.0) | 28.5 (19.0–46.0) | <0.001 |
| Platelets (109/L) | 236.1 ± 60.4 | 233.8 ± 58.3 | 238.3 ± 62.3 | 0.321 |
| Blood Glucose (mg/dL) | 103.8 ± 27.9 | 100.5 ± 21.1 | 107.0 ± 32.9 | 0.001 |
| Glycated haemoglobin (HbA1c) (%) | 5.8 ± 1.1 | 5.7 ± 1.0 | 5.9 ± 1.1 | 0.007 |
| Type 2 diabetes (%) | 26.6 | 24.1 | 29.1 | 0.109 |
| Arterial hypertension (%) | 61.1 | 62.1 | 60.2 | 0.610 |
| Systolic blood pressure (mmHg) | 130 (120–140) | 130 (120–140) | 130 (120–140) | 0.384 |
| Diastolic blood pressure (mmHg) | 80 (75–85) | 80 (70–85) | 80 (75–85) | 0.226 |
| Previous cardiovascular vascular disease (%) * | 13.0 | 15.2 | 10.8 | 0.072 |
| Metabolic Syndrome (%) | 52.0 | 31.5 | 72.0 | <0.001 |
| Non-alcoholic fatty liver disease (%) | 79.2 | 69.2 | 89.2 | <0.001 |
| Statin therapy (%) | 40.8 | 37.7 | 43.8 | 0.090 |
| Model A. Whole Cohort | Adjusted Odds Ratio (95% Confidence Intervals) | p |
|---|---|---|
| Age above median | 0.494 (0.348–0.701) | <0.001 |
| Female sex | 0.671 (0.482–0.936) | 0.019 |
| Previous cardiovascular events | 0.794 (0.476–1.324) | 0.376 |
| Non-alcoholic fatty liver disease | 2.246 (1.480–3.411) | <0.001 |
| Metabolic Syndrome | 5.933 (4.219–8.344) | <0.001 |
| Model B. NAFLD patients | ||
| Age above median | 0.550 (0.374–0.808) | 0.002 |
| Female sex | 0.684 (0.472–0.990) | 0.044 |
| Previous cardiovascular events | 0.791 (0.443–1.414) | 0.430 |
| Metabolic Syndrome | 6.588 (4.534–9.573) | <0.001 |
| Univariable | p Value | Hazard Ratio | 95% Confidence Interval | |
|---|---|---|---|---|
| Age | 0.001 | 1.050 | 1.019 | 1.081 |
| Female sex | 0.031 | 0.428 | 0.198 | 0.926 |
| Previous cardiovascular events | <0.001 | 3.442 | 1.802 | 6.573 |
| Arterial hypertension | 0.113 | 1.785 | 0.872 | 3.653 |
| Diabetes | 0.586 | 1.192 | 0.634 | 2.239 |
| Body mass index | 0.898 | 0.996 | 0.939 | 1.057 |
| Waist circumference | 0.269 | 1.014 | 0.990 | 1.038 |
| Metabolic syndrome * | 0.042 | 2.233 | 1.030 | 4.840 |
| Cholesterol remnant (above median) | 0.044 | 1.966 | 1.018 | 3.800 |
| Multivariable | p Value | Hazard Ratio | 95% Confidence Interval | |
| Age | 0.024 | 1.039 | 1.005 | 1.074 |
| Female sex | 0.047 | 0.454 | 0.208 | 0.989 |
| Cholesterol remnant (above median) | 0.020 | 2.202 | 1.132 | 4.285 |
| Previous cardiovascular events | 0.036 | 2.210 | 1.052 | 4.643 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pastori, D.; Baratta, F.; Novo, M.; Cocomello, N.; Violi, F.; Angelico, F.; Del Ben, M. Remnant Lipoprotein Cholesterol and Cardiovascular and Cerebrovascular Events in Patients with Non-Alcoholic Fatty Liver Disease. J. Clin. Med. 2018, 7, 378. https://doi.org/10.3390/jcm7110378
Pastori D, Baratta F, Novo M, Cocomello N, Violi F, Angelico F, Del Ben M. Remnant Lipoprotein Cholesterol and Cardiovascular and Cerebrovascular Events in Patients with Non-Alcoholic Fatty Liver Disease. Journal of Clinical Medicine. 2018; 7(11):378. https://doi.org/10.3390/jcm7110378
Chicago/Turabian StylePastori, Daniele, Francesco Baratta, Marta Novo, Nicholas Cocomello, Francesco Violi, Francesco Angelico, and Maria Del Ben. 2018. "Remnant Lipoprotein Cholesterol and Cardiovascular and Cerebrovascular Events in Patients with Non-Alcoholic Fatty Liver Disease" Journal of Clinical Medicine 7, no. 11: 378. https://doi.org/10.3390/jcm7110378
APA StylePastori, D., Baratta, F., Novo, M., Cocomello, N., Violi, F., Angelico, F., & Del Ben, M. (2018). Remnant Lipoprotein Cholesterol and Cardiovascular and Cerebrovascular Events in Patients with Non-Alcoholic Fatty Liver Disease. Journal of Clinical Medicine, 7(11), 378. https://doi.org/10.3390/jcm7110378