
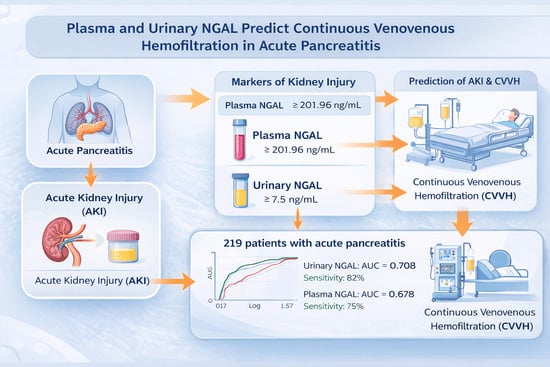
Predicting the Initiation of Continuous Venovenous Hemofiltration in Acute Pancreatitis Patients: The Role of Plasma and Urinary Neutrophil Gelatinase-Associated Lipocalin
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.1.1. Inclusion and Exclusion Criteria
- Age ≥18 years;
- Diagnosis of acute pancreatitis according to the Atlanta 2012 criteria;
- Provided informed consent to participate in the study.
2.1.2. Sample Size
2.1.3. Clinical and Laboratory Data Collection
2.1.4. Imaging Assessment
Measurement of Plasma and Urinary NGAL
2.1.5. Statistical Analysis
2.1.6. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chan, K.S.; Shelat, V.G. Diagnosis, severity stratification and management of adult acute pancreatitis-current evidence and controversies. World J. Gastrointest. Surg. 2022, 14, 1179–1197. [Google Scholar] [CrossRef]
- Trikudanathan, G.; Yazici, C.; Evans Phillips, A.; Forsmark, C.E. Diagnosis and Management of Acute Pancreatitis. Gastroenterology 2024, 167, 673–688. [Google Scholar] [CrossRef] [PubMed]
- Boxhoorn, L.; Voermans, R.P.; Bouwense, S.A.; Bruno, M.J.; Verdonk, R.C.; Boermeester, M.A.; van Santvoort, H.C.; Besselink, M.G. Acute pancreatitis. Lancet 2020, 396, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Selvanathan, D.K.; Johnson, P.G.; Thanikachalam, D.K.; Rajendran, P.; Gopalakrishnan, N. Acute Kidney Injury Complicating Severe Acute Pancreatitis: Clinical Profile and Factors Predicting Mortality. Indian J. Nephrol. 2022, 32, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Nassar, T.I.; Qunibi, W.Y. AKI Associated with Acute Pancreatitis. Clin. J. Am. Soc. Nephrol. 2019, 14, 1106–1115. [Google Scholar] [CrossRef]
- Weng, Y.; Dong, Z.; Ye, G.; Shi, L.; Liu, P.; Zhou, T.; Ye, H. Application of continuous renal replacement therapy (CRRT) in patients with severe acute pancreatitis: An analytical study. BMC Gastroenterol. 2025, 25, 592. [Google Scholar] [CrossRef]
- Chen, F.; Xie, R.; Han, X.; Ning, F.; Chen, Y.; Liu, H.; Liu, L.; Li, X. Study on the clinical effect of initiating continuous blood purification at different times for severe acute pancreatitis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2024, 36, 937–942. [Google Scholar]
- Pandey, R.; Pathak, R.; Jha, A.; Gnawali, A.; Koirala, D. Comparison of Acute Physiology and Chronic Health Evaluation II, Bedside Index for Severity in Acute Pancreatitis and Modified Computed Tomography Severity Index Scores in Predicting the Outcome in Acute Pancreatitis in a Tertiary Care Centre in Nepal. J. Nepal Health Res. Counc. 2023, 21, 203–206. [Google Scholar] [CrossRef]
- Harshit Kumar, A.; Singh Griwan, M. A comparison of APACHE II, BISAP, Ranson’s score and modified CTSI in predicting the severity of acute pancreatitis based on the 2012 revised Atlanta Classification. Gastroenterol. Rep. 2017, 6, 127–131. [Google Scholar] [CrossRef]
- Romejko, K.; Markowska, M.; Niemczyk, S. The Review of Current Knowledge on Neutrophil Gelatinase-Associated Lipocalin (NGAL). Int. J. Mol. Sci. 2023, 24, 10470. [Google Scholar] [CrossRef]
- Marakala, V. Neutrophil gelatinase-associated lipocalin (NGAL) in kidney injury—A systematic review. Clin. Chim. Acta 2022, 536, 135–141. [Google Scholar] [CrossRef]
- Yeung, A.C.Y.; Morozov, A.; Robertson, F.P.; Fuller, B.J.; Davidson, B.R. Neutrophil Gelatinase-Associated Lipocalin (NGAL) in predicting acute kidney injury following orthotopic liver transplantation: A systematic review. Int. J. Surg. 2018, 59, 48–54. [Google Scholar] [CrossRef]
- Shang, W.; Wang, Z. The Update of NGAL in Acute Kidney Injury. Curr. Protein Pept. Sci. 2017, 18, 1211–1217. [Google Scholar] [CrossRef] [PubMed]
- Buonafine, M.; Martinez-Martinez, E.; Jaisser, F. More than a simple biomarker: The role of NGAL in cardiovascular and renal diseases. Clin. Sci. 2018, 132, 909–923. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Jin, X. Predictive Value of Serum NGAL and β2 Microglobulin in Blood and Urine amongst Patients with Acute Pancreatitis and Acute Kidney Injury. Arch. Esp. Urol. 2023, 76, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Nhuong, L.H.; Thang, L.V.; Kien, N.T.; Dung, P.T.; Khanh, N.Q.; Thuy, H.; Tam, N.V.; Thuan, P.D. Urinary NGAL outperforms plasma NGAL in predicting continuous venovenous hemofiltration requirement in acute pancreatitis. Pancreatology, 2026; in press. [Google Scholar] [CrossRef]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S. Classification of acute pancreatitis-2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Devani, K.; Charilaou, P.; Radadiya, D.; Brahmbhatt, B.; Young, M.; Reddy, C. Acute pancreatitis: Trends in outcomes and the role of acute kidney injury in mortality—A propensity-matched analysis. Pancreatology 2018, 18, 870–877. [Google Scholar] [CrossRef]
- Schneider, F.; Maurer, C.; Friedberg, R.C. International Organization for Standardization (ISO) 15189. Ann. Lab. Med. 2017, 37, 365–370. [Google Scholar] [CrossRef]
- Yadav, S.C.; Zhang, B. Effect of Early Continuous Veno-Venous Haemofiltration in Severe Acute Pancreatitis for the Prevention of Local Pancreatic Complications. Gastroenterol. Res. Pract. 2022, 2022, 7575231. [Google Scholar] [CrossRef]
- Hu, Q.; Hu, Y.; Tan, C.; Yang, Y.; Su, H.; Huang, Z.; Tang, W.; Wang, R.; Liu, J.; Wan, M. Acute pancreatitis: Mechanisms and therapeutic approaches. Signal Transduct. Target. Ther. 2026, 11, 15. [Google Scholar] [CrossRef]
- Petrescu, G.S.; Georgescu, I.; Petrescu, A.M.; Radulescu, D.; Petrescu, M.O.; Patrascu, S. Balthazar Score and Neutrophil-Lymphocytes Ratio in Acute Pancreatitis. Curr. Health Sci. J. 2019, 45, 316–320. [Google Scholar] [PubMed]
- Hosokawa, T.; Tanami, Y.; Sato, Y.; Oguma, E. Comparison of the Balthazar score of acute pancreatitis between computed tomography and ultrasound in children: Pitfalls of ultrasound in diagnosing and evaluating pancreatitis. J. Med. Ultrason. 2021, 48, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Tee, Y.S.; Fang, H.Y.; Kuo, I.M.; Lin, Y.S.; Huang, S.F.; Yu, M.C. Serial evaluation of the SOFA score is reliable for predicting mortality in acute severe pancreatitis. Medicine 2018, 97, e9654. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Zhao, L.; Kang, J.; Wen, C.; Li, Y.; Ren, Y.; Wang, H.; Zhang, S.; Yang, S.; Song, J.; et al. Development and validation of a predictive model for acute kidney injury in patients with moderately severe and severe acute pancreatitis. Clin. Exp. Nephrol. 2022, 26, 770–787. [Google Scholar] [CrossRef]
- Chi, C.; Song, X.; Ma, Y.; Wang, C.; Zhu, J. Establishment and Diagnostic Value of an Early Prediction Model for Acute Pancreatitis Complicated With Acute Kidney Injury. Pancreas 2024, 53, e547–e552. [Google Scholar] [CrossRef]
- Pickkers, P.; Darmon, M.; Hoste, E.; Joannidis, M.; Legrand, M.; Ostermann, M.; Prowle, J.R.; Schneider, A.; Schetz, M. Acute kidney injury in the critically ill: An updated review on pathophysiology and management. Intensive Care Med. 2021, 47, 835–850. [Google Scholar] [CrossRef]
- Peng, T.; Peng, X.; Huang, M.; Cui, J.; Zhang, Y.; Wu, H.; Wang, C. Serum calcium as an indicator of persistent organ failure in acute pancreatitis. Am. J. Emerg. Med. 2017, 35, 978–982. [Google Scholar] [CrossRef]
- Hunter, R.W.; Bailey, M.A. Hyperkalemia: Pathophysiology, risk factors and consequences. Nephrol. Dial. Transplant. 2019, 34, iii2–iii11. [Google Scholar] [CrossRef]
- Mochizuki, K.; Fujii, T.; Paul, E.; Anstey, M.; Pilcher, D.V.; Bellomo, R. Early metabolic acidosis in critically ill patients: A binational multicentre study. Crit. Care Resusc. 2021, 23, 67–75. [Google Scholar] [CrossRef]
- Albert, C.; Zapf, A.; Haase, M.; Rover, C.; Pickering, J.W.; Albert, A.; Bellomo, R.; Breidthardt, T.; Camou, F.; Chen, Z.; et al. Neutrophil Gelatinase-Associated Lipocalin Measured on Clinical Laboratory Platforms for the Prediction of Acute Kidney Injury and the Associated Need for Dialysis Therapy: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2020, 76, 826–841 e821. [Google Scholar] [CrossRef]
- Xu, C.; Lin, S.; Mao, L.; Li, Z. Neutrophil gelatinase-associated lipocalin as predictor of acute kidney injury requiring renal replacement therapy: A systematic review and meta-analysis. Front. Med. 2022, 9, 859318. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristics | All (n = 219) | CVVHF (+), (n = 28) | CVVHF (−), (n = 191) | p |
|---|---|---|---|---|
| Age, years | 45.84 ± 13.14 | 46.64 ± 13.97 | 45.72 ± 13.05 | 0.73 |
| Gender, n (%) | ||||
| 180 (82.2) | 27 (96.4) | 153 (80.1) | 0.034 |
| 39 (17.8) | 1 (3.6) | 38 (19.9) | |
| BMI (kg/m2) | ||||
| 17 (7.8) | 2 (7.1) | 15 (7.8) | 0.263 |
| 87 (39.7) | 7 (25.0) | 80 (41.9) | |
| 58 (26.5) | 8 (28.6) | 50 (26.2) | |
| 57 (26.0) | 11 (39.3) | 46 (24.1) | |
| 23.29 ± 4.37 | 23.61 ± 3.63 | 23.25 ± 4.47 | 0.689 |
| Blood pressure, mmHg | ||||
| 130.11 ± 20.98 | 122.00 ± 25.16 | 131.29 ± 20.11 | 0.028 |
| 79.03 ± 13.85 | 75.21 ± 16.74 | 79.59 ± 13.34 | 0.119 |
| 96.07 ± 14.95 | 90.83 ± 18.47 | 96.84 ± 14.26 | 0.047 |
| Comorbidities, n(%) | ||||
| 34 (15.5) | 5 (17.9) | 29 (15.2) | 0.78 |
| 30 (13.7) | 8 (28.6) | 22 (11.5) | 0.033 |
| Etiology, n(%) | ||||
| 48 (21.9) | 6 (21.4) | 42 (22.0) | 0.58 |
| 10 (4.6) | 0 (0) | 10 (5.2) | 0.247 |
| 95 (43.4) | 17 (60.7) | 78 (40.8) | 0.038 |
| Acute pancreatitis | ||||
| 125 (57.1) | 20 (71.4) | 105 (55.0) | 0.36 |
| 56 (25.6) | 4 (14.3) | 52 (27.2) | |
| 14 (6.4) | 2 (7.1) | 12 (6.3) | |
| 24 (11.0) | 2 (7.1) | 22 (11.5) | |
| Hematology | ||||
| 12.83 ± 3.90 | 10.34 ± 3.59 | 13.11 ± 3.03 | 0.82 |
| 137.45 ± 27.97 | 166.00 ± 24.04 | 134.28 ± 27.09 | 0.61 |
| 217 ± 45 | 154.50 ± 48.79 | 224.44 ± 67.37 | 0.73 |
| Blood metabolism | ||||
| 10.13 ± 5.61 | 10.76 ± 10.84 | 10.06 ± 5.31 | 0.003 |
| 64.28 ± 8.19 | 62.75 ± 3.04 | 64.45 ± 8.61 | <0.001 |
| 34.45 ± 5.82 | 36.75 ± 4.87 | 34.20 ± 5.98 | 0.001 |
| 441.00 ± 435.29 | 671.50 ± 369.81 | 415.39 ± 443.60 | <0.001 |
| 46.32 ± 54.15 | 49.00 ± 4.10 | 46.03 ± 57.23 | 0.131 |
| 44.54 ± 56.52 | 22.80 ± 3.39 | 46.95 ± 59.23 | 0.465 |
| 29.11 ± 34.81 | 27.05 ± 3.04 | 29.34 ± 39.79 | 0.240 |
| 635.91 ± 850.26 | 736.65 ± 485.57 | 624.71 ± 890.39 | 0.637 |
| 968.93 ± 1754.8 | 2334.50 ± 1723.22 | 817.20 ± 1738.73 | 0.975 |
| 15.52 ± 26.05 | 8.82 ± 1.66 | 16.26 ± 27.43 | 0.452 |
| 20.68 ± 26.34 | 25.71 ± 10.53 | 20.12 ± 27.67 | 0.438 |
| Arterial blood gas | ||||
| 7.42 ± 0.06 | 7.34 ± 0.07 | 7.43 ± 0.05 | <0.001 |
| 33.90 ± 4.79 | 37.50 ± 10.61 | 33.51 ± 4.17 | 0.092 |
| 85.75 ± 25.04 | 71.50 ± 71.42 | 87.34 ± 19.35 | 0.278 |
| 22.34 ± 3.71 | 19.45 ± 6.72 | 22.66 ±3.42 | <0.001 |
| 395.83 ± 136.11 | 341.95 ± 342.17 | 401.82 ± 115.93 | 0.033 |
| 2.5 ± 2.31 | 6.78 ± 5.53 | 2.03 ± 1.32 | <0.001 |
| 13.42 ± 1.75 | 10.85 ± 1.20 | 13.7 ± 1.57 | <0.001 |
| 1.12 ± 0.14 | 0.99 ± 0.12 | 1.14 ± 0.13 | <0.001 |
| AKI | ||||
| 5.01 ±2.89 | 7.8 ± 3.96 | 4.71 ± 2.72 | <0.001 |
| 77.70 ± 45.75 | 169.50 ± 30.41 | 67.50 ± 34.40 | <0.001 |
| 51 (23.3) | 21 (75.0) | 30 (15.7) | <0.001 |
| 128.86 ± 30.41 | 136.50 ± 3.53 | 128.01 ± 32.02 | 0.975 |
| 3.66 ± 0.53 | 3.80 ± 1.11 | 3.64 ± 0.48 | 0.003 |
| 2.04 ± 0.36 | 1.76 ± 0.67 | 2.06 ± 0.33 | <0.001 |
| 98.44 ± 6.35 | 95.70 ± 1.84 | 98.75 ± 6.63 | 0.477 |
| Acute pancreatitis | ||||
| 160 (73.1) | 5 (17.9) | 155 (81.2) | <0.001 |
| 59 (26.9) | 23 (82.1) | 36 (18.8) | |
| 159 (73.3) | 16 (57.1) | 143 (75.7) | 0.064 |
| 58 (26.7) | 12 (42.9) | 46 (24.3) | |
| 89 (40.6) | 4 (14.3) | 85 (44.5) | 0.002 |
| 130 (59.4) | 24 (85.7) | 106 (55.5) | |
| 4.21 ± 1.79 | 5.22 ± 2.24 | 4.06 ± 1.68 | 0.002 |
| APACHE II | 6.15 ± 4.36 | 13.00 ± 1.41 | 5.39 ± 3.86 | <0.001 |
| SOFA | 1.9 ± 1.94 | 5.00 ± 2.83 | 1.56 ± 1.58 | <0.001 |
| IMRIE | 2.05 ± 1.64 | 2.50 ± 2.12 | 2.00 ± 1.64 | <0.001 |
| BISAP | 1.10 ± 1.07 | 2.00 ± 1.41 | 1.00 ± 1.03 | <0.001 |
| MARSHALL | 1.00 ± 1.34 | 3.50 ± 2.12 | 0.72 ± 0.96 | <0.001 |
| Plasma NGAL | 661.63 ± 732.11 | 2627.39 ± 839.29 | 443.21 ±229.09 | <0.001 |
| Urine NGAL | 264.83 | 1127.98 ± 1300.82 | 168.92 ± 130.91 | <0.001 |
| Mortality | 3 (1.4) | 2 (7.1) | 1 (0.5) | 0.044 |
| Adjusted OR | 95% CI | p | |
|---|---|---|---|
| uNGAL | 0.997 | 0.995–1.000 | 0.016 |
| pNGAL | 0.999 | 0.998–1.001 | 0.371 |
| APACHE II | 0.748 | 0.593–0.944 | 0.014 |
| BISAP | 1.395 | 0.634–3.067 | 0.408 |
| Total Calcium | 11.475 | 1.559–84.454 | 0.017 |
| CRP | 0.999 | 0.996–1.003 | 0.677 |
| Lactat | 0.901 | 0.571–1.424 | 0.656 |
| Variable(s) | AUC (95% CI) | Cut-Off (ng/mL) | p | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|
| Plasma NGAL | 0.678 (0.609–0.835) | 201.96 | 0.002 | 75.00 | 75.24 |
| Urinary NGAL | 0.708 (0.631–0.834) | 7.5 | 0.000 | 82.1 | 71.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Share and Cite
Huu Nhuong, L.; Viet Thang, L.; Trung Kien, N.; Thai Dung, P.; Quoc Khanh, N.; Thuy, H.; Van Tam, N.; Dang Thuan, P. Predicting the Initiation of Continuous Venovenous Hemofiltration in Acute Pancreatitis Patients: The Role of Plasma and Urinary Neutrophil Gelatinase-Associated Lipocalin. J. Clin. Med. 2026, 15, 2509. https://doi.org/10.3390/jcm15072509
Huu Nhuong L, Viet Thang L, Trung Kien N, Thai Dung P, Quoc Khanh N, Thuy H, Van Tam N, Dang Thuan P. Predicting the Initiation of Continuous Venovenous Hemofiltration in Acute Pancreatitis Patients: The Role of Plasma and Urinary Neutrophil Gelatinase-Associated Lipocalin. Journal of Clinical Medicine. 2026; 15(7):2509. https://doi.org/10.3390/jcm15072509
Chicago/Turabian StyleHuu Nhuong, Le, Le Viet Thang, Nguyen Trung Kien, Pham Thai Dung, Nguyen Quoc Khanh, Hoang Thuy, Nguyen Van Tam, and Pham Dang Thuan. 2026. "Predicting the Initiation of Continuous Venovenous Hemofiltration in Acute Pancreatitis Patients: The Role of Plasma and Urinary Neutrophil Gelatinase-Associated Lipocalin" Journal of Clinical Medicine 15, no. 7: 2509. https://doi.org/10.3390/jcm15072509
APA StyleHuu Nhuong, L., Viet Thang, L., Trung Kien, N., Thai Dung, P., Quoc Khanh, N., Thuy, H., Van Tam, N., & Dang Thuan, P. (2026). Predicting the Initiation of Continuous Venovenous Hemofiltration in Acute Pancreatitis Patients: The Role of Plasma and Urinary Neutrophil Gelatinase-Associated Lipocalin. Journal of Clinical Medicine, 15(7), 2509. https://doi.org/10.3390/jcm15072509