
Radiological Evaluation of Retained Primary Molars in Adolescents with Mandibular Second Premolar Agenesis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Panoramic Examination
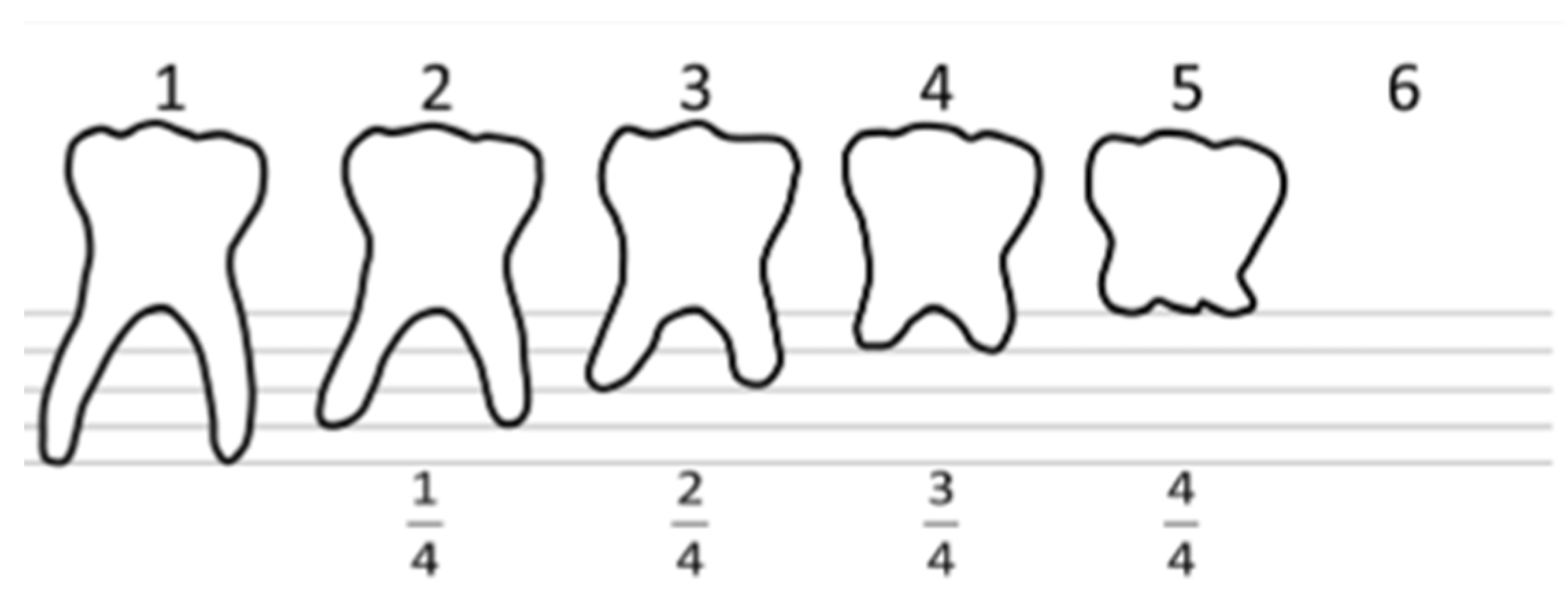
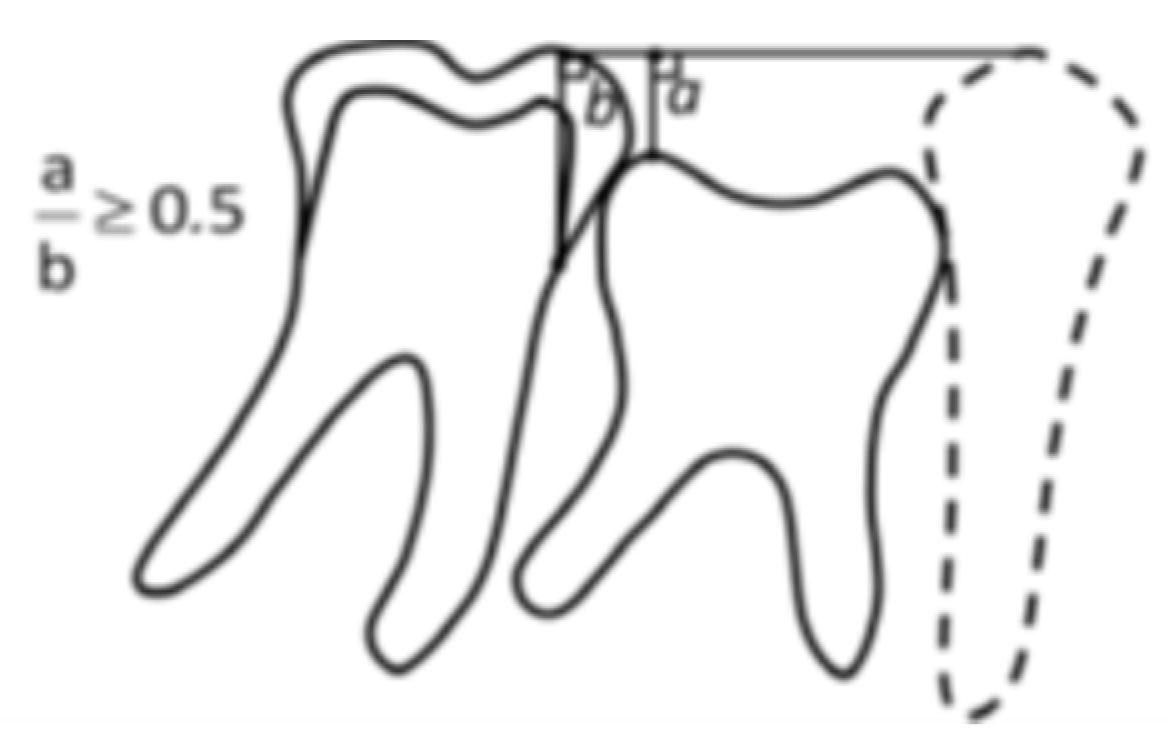
2.3. Radiological Analysis
2.4. Statistical Analysis
2.5. Ethical Committee
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al-Ani, A.H.; Antoun, J.S.; Thomson, W.M.; Merriman, T.R.; Farella, M. Hypodontia: An Update on Its Etiology, Classification, and Clinical Management. BioMed Res. Int. 2017, 2017, 9378325. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, K.; Miskelly, J.; Voge, E.; Macfarlane, T.V. Prevalence of hypodontia and associated factors: A systematic review and meta-analysis. J. Orthod. 2014, 41, 299–316. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, C.C.O.; Melo, D.L.; da Silva, P.P.; Normando, D. What is the survival rate of deciduous molars in cases with agenesis of premolar successors? A systematic review. Angle Orthod. 2022, 92, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Hvaring, C.L.; Øgaard, B.; Stenvik, A.; Birkeland, K. The prognosis of retained primary molars without successors: Infraocclusion, root resorption and restorations in 111 patients. Eur. J. Orthod. 2014, 36, 26–30. [Google Scholar] [CrossRef]
- Arandi, N.Z.; Rabi, T. Mandibular Second Premolar Agenesis: A Retrospective Cross-sectional Study from Palestine. J. Pharm. Bioallied Sci. 2024, 16, S125–S129. [Google Scholar] [CrossRef]
- Bjerklin, K.; Bennett, J. The long-term survival of lower second primary molars in subjects with agenesis of the premolars. Eur. J. Orthod. 2000, 22, 245–255. [Google Scholar] [CrossRef]
- Bjerklin, K.; Al-Najjar, M.; Kårestedt, H.; Andrén, A. Agenesis of mandibular second premolars with retained primary molars. A longitudinal radiographic study of 99 subjects from 12 years of age to adulthood. Eur. J. Orthod. 2008, 30, 254–261. [Google Scholar] [CrossRef]
- Hvaring, C.L.; Birkeland, K. The long-term fate of persisting deciduous molars and canines in 42 patients with severe hypodontia: A 12-year follow-up. Eur. J. Orthod. 2020, 42, 581–586. [Google Scholar] [CrossRef]
- Ith-Hansen, K.; Kjær, I. Persistence of deciduous molars in subjects with agenesis of the second premolars. Eur. J. Orthod. 2000, 22, 239–243. [Google Scholar] [CrossRef]
- Sletten, D.W.; Smith, B.M.; Southard, K.A.; Casko, J.S.; Southard, T.E. Retained deciduous mandibular molars in adults: A radiographic study of long-term changes. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 625–630. [Google Scholar] [CrossRef]
- Kjaer, I.; Nielsen, M.H.; Skovgaard, L.T.; Kjær, I. Can persistence of primary molars be predicted in subjects with multiple tooth agenesis? Eur J Orthod. Eur. J. Orthod. 2008, 30, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Bilinska, M.; Zadurska, M.; Czochrowska, E. Status of retained deciduous second molars in subjects with agenesis of second premolars in relation to age. Eur. J. Paediatr. Dent. 2023, 24, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Haselden, K.; Hobkirk, J.; Goodman, J.; Jones, S.; Hemmings, K. Root resorption in retained deciduous canine and molar teeth without permanent successors in patients with severe hypodontia. Int. J. Paediatr. Dent. 2001, 11, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Laverty, D.P.; Fairbrother, K.; Addison, O. The Current Evidence on Retaining or Prosthodontically Replacing Retained Deciduous Teeth in the Adult Hypodontia Patient: A Systematic Review. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 2–15. [Google Scholar] [CrossRef]
- Akgöl, B.B.; Üstün, N.; Bayram, M. Characterizing infraocclusion in primary molars: Prevalence, accompanying findings, and infraocclusion severity and treatment implications. BMC Oral Health 2024, 24, 661. [Google Scholar] [CrossRef]
- Meistere, D.; Kronina, L.; Karkle, A.; Neimane, L. Non-syndromic tooth agenesis in Latvian adolescent dental patients: A retrospective study with relevant literature review. Eur. Arch. Paediatr. Dent. 2024, 25, 427–432. [Google Scholar] [CrossRef]
- Arhakis, A.; Boutiou, E. Etiology, Diagnosis, Consequences and Treatment of Infraoccluded Primary Molars. Open Dent. J. 2016, 10, 714–719. [Google Scholar] [CrossRef]
- Üstün, N.; Özükoç, C. Prevalence of Mandibular Second Premolar Agenesis in Individuals and Associated Factors: A Meta-Analysis. Selcuk Dent. J. 2022, 9, 182–190. [Google Scholar] [CrossRef]
- Garib, D.G.; Alves, A.C.d.M.; Janson, G.; Salles, R.B.; Ferreira, D.G. Correlation of root resorption and infraocclusion in mandibular deciduous second molars without succedaneous permanent teeth. J. World Fed. Orthod. 2014, 3, 110–113. [Google Scholar] [CrossRef]
- Maldupa, I.; Sopule, A.; Uribe, S.E.; Brinkmane, A.; Senakola, E. Caries Prevalence and Severity for 12-Year-Old Children in Latvia. Int. Dent. J. 2021, 71, 214–223. [Google Scholar] [CrossRef]
- Harokopakis-Hajishengallis, E. Physiologic root resorption in primary teeth: Molecular and histological events. J. Oral Sci. 2007, 49, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Calheiros-Lobo, M.J.; Costa, F.; Pinho, T. Infraocclusion level and root resorption of the primary molar in second premolar agenesis: A retrospective cross-sectional study in the Portuguese population. Dent. Med. Probl. 2022, 59, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Aktan, A.M.; Kara, I.; Şener, I.; Bereket, C.; Çelik, S.; Kırtay, M.; ÇIftçI, M.E.; ArıCı, N. An evaluation of factors associated with persistent primary teeth. Eur. J. Orthod. 2012, 34, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Devlin, H.; Yuan, J. Object position and image magnification in dental panoramic radiography: A theoretical analysis. Dentomaxillofac. Radiol. 2013, 42, 29951683. [Google Scholar] [CrossRef]
- Ekim, S.L.; Hatibovic-Kofman, S. A treatment decision-making model for infraoccluded primary molars. Int. J. Paediatr. Dent. 2001, 11, 340–346. [Google Scholar] [CrossRef]
- Vieira-Andrade, R.G.; Drumond, C.L.; Alves, L.P.A.; Marques, L.S.; Ramos-Jorge, M.L. Inflammatory root resorption in primary molars: Prevalence and associated factors. Braz. Oral Res. 2012, 26, 335–340. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| CONDITION | N | % |
|---|---|---|
| Good condition | 83 | 35.2% |
| Not present in the oral cavity | 98 | 41.5% |
Poor condition
| 55 16 8 5 11 15 | 23.3% 6.8% 3.4% 2.1% 4.7% 6.3% |
| Total | 236 | 100% |
| Root Resorption | |||||||
| 1 | 2 | 3 | 4 | 5 | 6 | Pathological | |
| Number of teeth (Total = 236) | 29 | 35 | 33 | 16 | 8 | 98 | 17 |
| Infraocclusion | |||||||
| NI | <0.20 | 0.21–0.50 | >0.50 | CBE | |||
| Number of teeth (Total = 136) | 100 | 5 | 19 | 8 | 4 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meistere, D.; Karkle, A.; Mengele, S.; Kronina, L.; Neimane, L. Radiological Evaluation of Retained Primary Molars in Adolescents with Mandibular Second Premolar Agenesis. J. Clin. Med. 2025, 14, 3241. https://doi.org/10.3390/jcm14093241
Meistere D, Karkle A, Mengele S, Kronina L, Neimane L. Radiological Evaluation of Retained Primary Molars in Adolescents with Mandibular Second Premolar Agenesis. Journal of Clinical Medicine. 2025; 14(9):3241. https://doi.org/10.3390/jcm14093241
Chicago/Turabian StyleMeistere, Dita, Aleksandra Karkle, Sindija Mengele, Liga Kronina, and Laura Neimane. 2025. "Radiological Evaluation of Retained Primary Molars in Adolescents with Mandibular Second Premolar Agenesis" Journal of Clinical Medicine 14, no. 9: 3241. https://doi.org/10.3390/jcm14093241
APA StyleMeistere, D., Karkle, A., Mengele, S., Kronina, L., & Neimane, L. (2025). Radiological Evaluation of Retained Primary Molars in Adolescents with Mandibular Second Premolar Agenesis. Journal of Clinical Medicine, 14(9), 3241. https://doi.org/10.3390/jcm14093241