

A Cross-Sectional Survey Assessing the Factors Influencing Dentists’ Decisions on Post-Endodontic Prosthetic Crown Restoration

 ,
, 
 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Diagnostic Imaging Preferences and Perception
3.2. The Influence of CBCT Diagnostic Precision on Clinical Decision-Making
Impact of CBCT Diagnostic Precision on Treatment Choices
3.3. Effect of CBCT Precision on Decision to Postpone Definitive Restorations
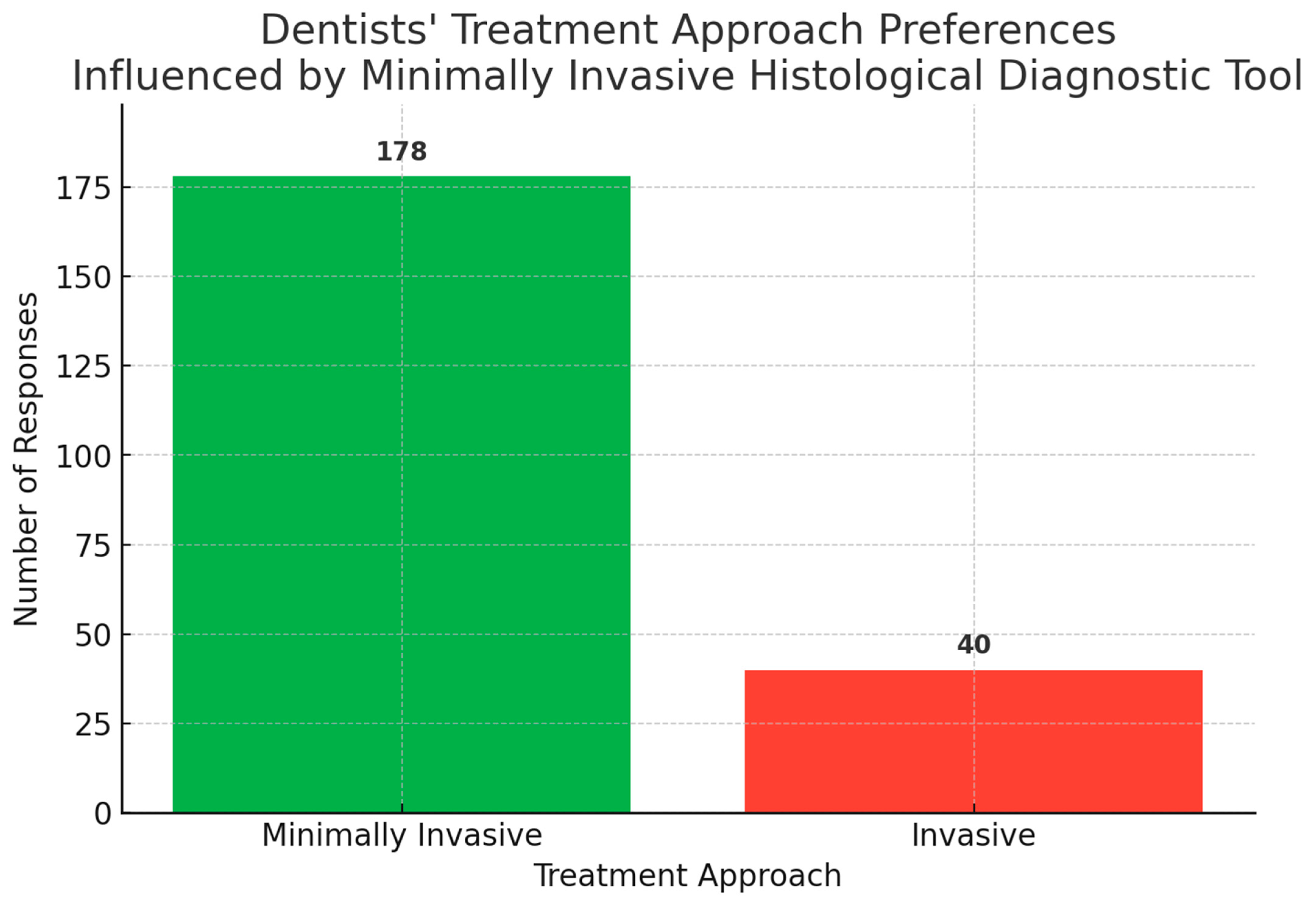
3.4. Clinical Decisions Influenced by a Hypothetical Availability of a Minimally Invasive Histological Diagnostic Tool
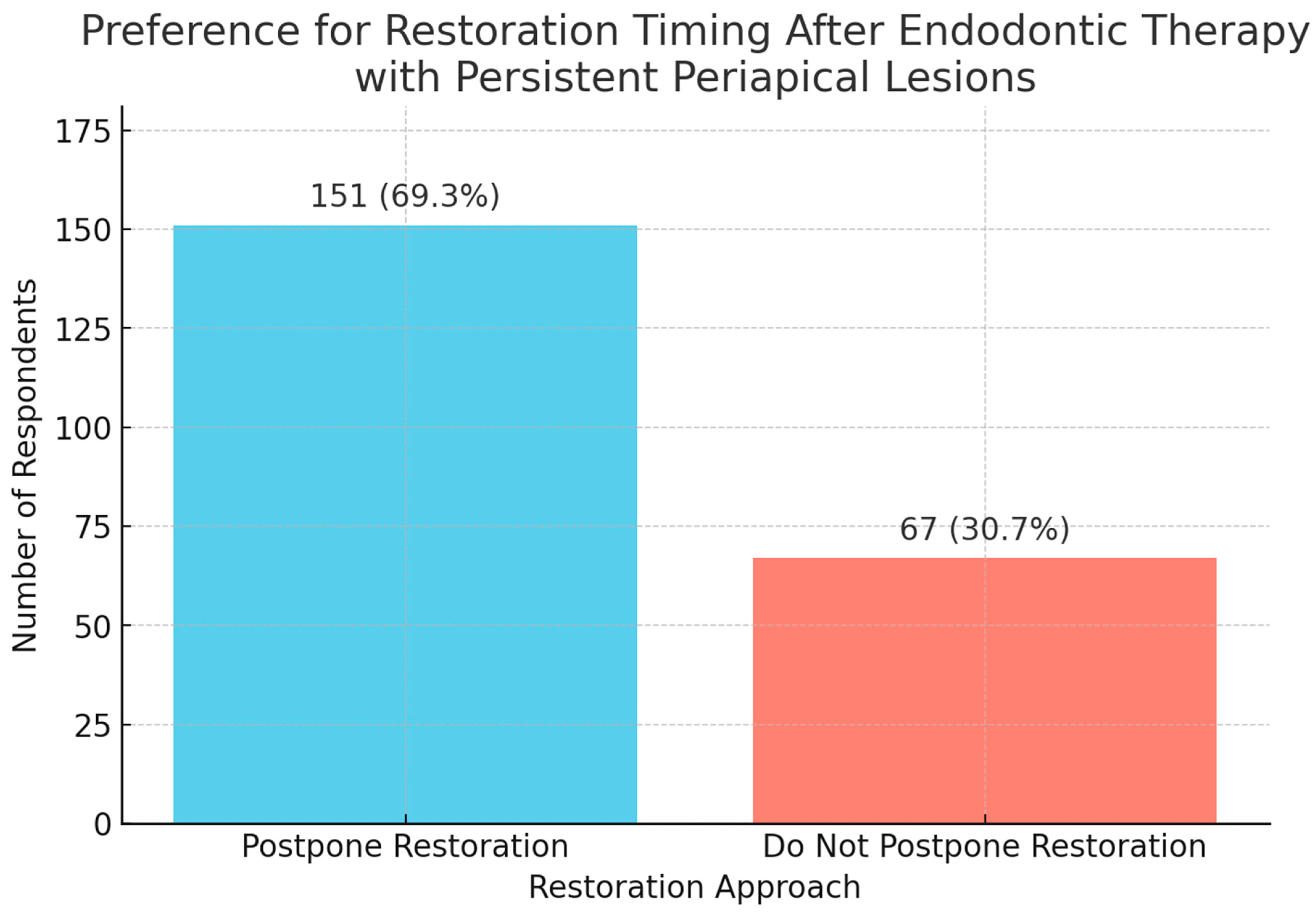
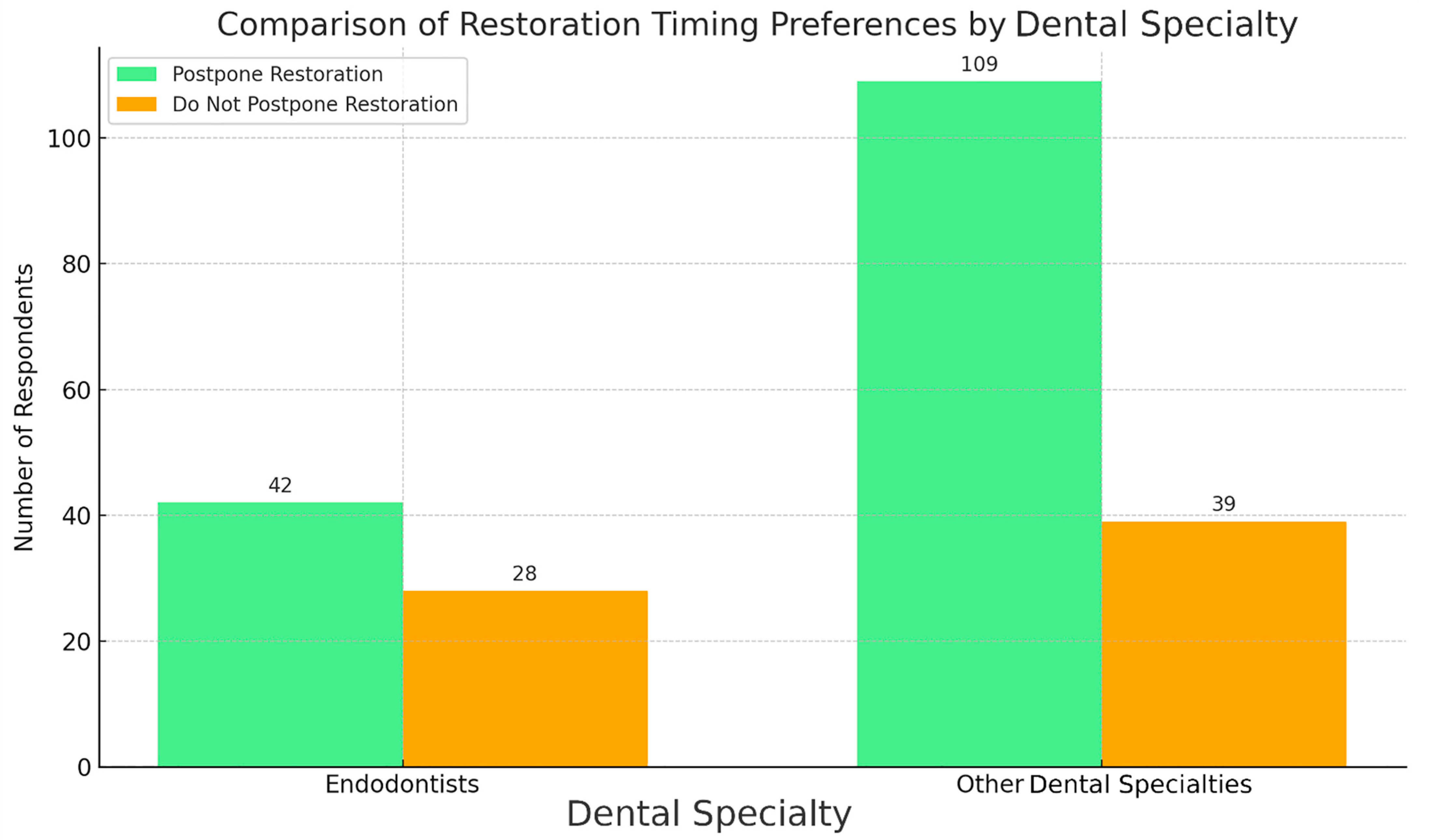
3.5. Rationale and Time Span for Final Crown Restoration in Cases with Ongoing Periapical Healing
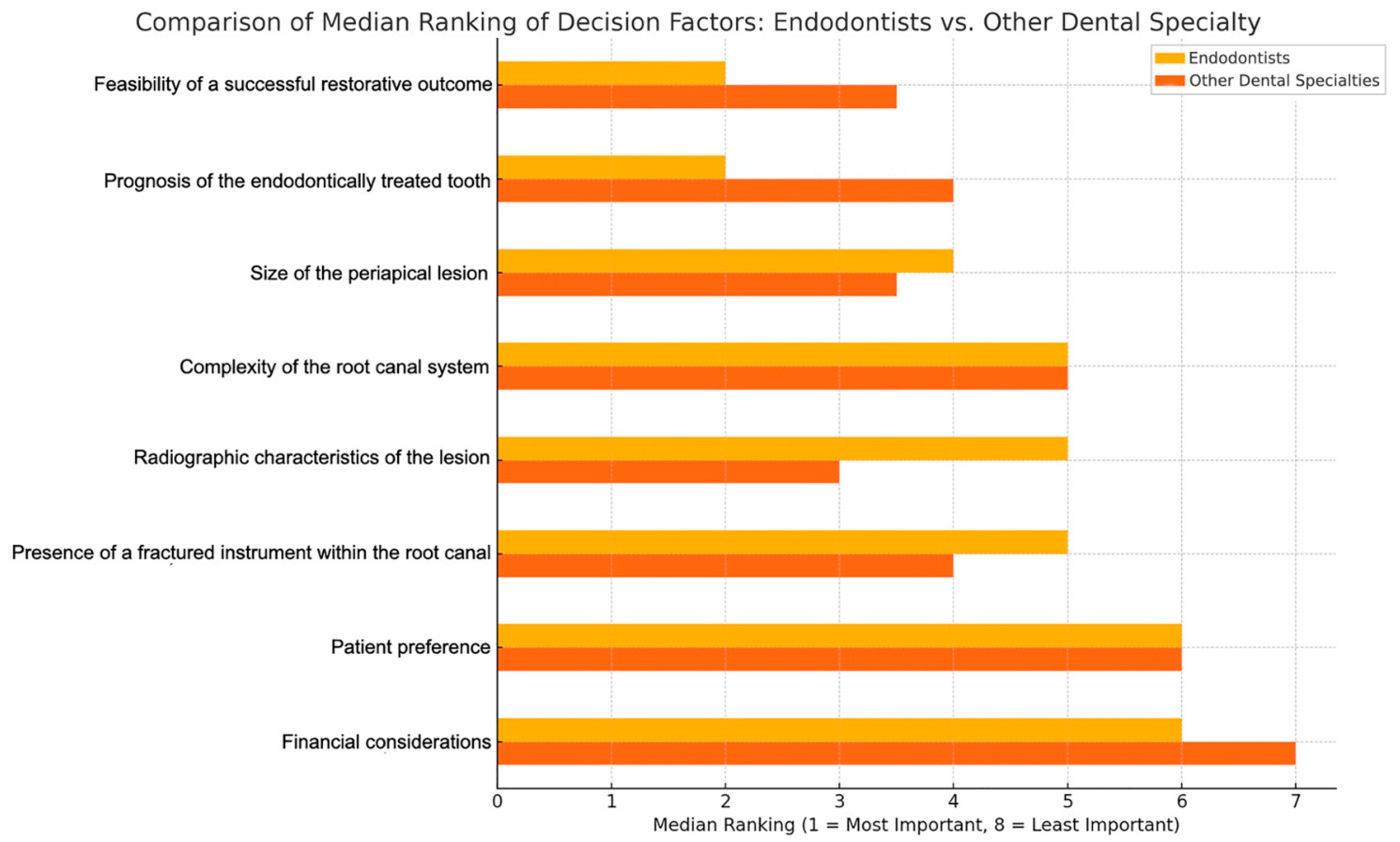
3.6. Factors Influencing Decision-Making for Final Restoration and Treatment Options
3.6.1. Restorative Approach for Endodontically Treated Teeth
3.6.2. To Preserve or to Extract?
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abbott, P.V.; Yu, C. A clinical classification of the status of the pulp and the root canal system. Aust. Dent. J. 2007, 52, S17–S31. [Google Scholar] [CrossRef] [PubMed]
- Mannocci, F.; Bitter, K.; Sauro, S.; Ferrari, P.; Austin, R.; Bhuva, B. Present status and future directions: The restoration of root filled teeth. Int. Endod. J. 2022, 55, 1059–1084. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.S.; Robbins, J.W. Post Placement and Restoration of Endodontically Treated Teeth: A Literature Review. J. Endod. 2004, 30, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Naumann, M.; Schmitter, M.; Frankenberger, R.; Krastl, G. “Ferrule Comes First. Post Is Second!” Fake News and Alternative Facts? A Systematic Review. J. Endod. 2018, 44, 212–219. [Google Scholar] [CrossRef]
- McGuigan, M.B.; Louca, C.; Duncan, H.F. The impact of fractured endodontic instruments on treatment outcome. Br. Dent. J. 2013, 214, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Gorni, F.G.M.; Gagliani, M.M. The Outcome of Endodontic Retreatment: A 2-yr Follow-up. J. Endod. 2004, 30, 1–4. [Google Scholar] [CrossRef]
- Gliga, A.; Imre, M.; Grandini, S.; Marruganti, C.; Gaeta, C.; Bodnar, D.; Dimitriu, B.A.; Foschi, F. The Limitations of Periapical X-ray Assessment in Endodontic Diagnosis—A Systematic Review. J. Clin. Med. 2023, 12, 4647. [Google Scholar] [CrossRef]
- Estrela, C.; Bueno, M.R.; Leles, C.R.; Azevedo, B.; Azevedo, J.R. Accuracy of Cone Beam Computed Tomography and Panoramic and Periapical Radiography for Detection of Apical Periodontitis. J. Endod. 2008, 34, 273–279. [Google Scholar] [CrossRef]
- Patel, S.; Durack, C.; Abella, F.; Shemesh, H.; Roig, M.; Lemberg, K. Cone beam computed tomography in Endodontics—A review. Int. Endod. J. 2015, 48, 3–15. [Google Scholar] [CrossRef]
- Kruse, C.; Spin-Neto, R.; Reibel, J.; Wenzel, A.; Kirkevang, L. Diagnostic validity of periapical radiography and CBCT for assessing periapical lesions that persist after endodontic surgery. Dentomaxillofacial Radiol. 2017, 46, 20170210. [Google Scholar] [CrossRef]
- Ferrari, M.; Vichi, A.; Fadda, G.M.; Cagidiaco, M.C.; Tay, F.R.; Breschi, L.; Polimeni, A.; Goracci, C. A Randomized Controlled Trial of Endodontically Treated and Restored Premolars. J. Dent. Res. 2012, 91, 72. [Google Scholar] [CrossRef] [PubMed]
- Mannocci, F.; Bertelli, E.; Sherriff, M.; Watson, T.F.; Pitt Ford, T.R. Three-year clinical comparison of survival of endodontically treated teeth restored with either full cast coverage or with direct composite restoration. Int. Endod. J. 2009, 42, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Alani, A.; Bishop, K.; Djemal, S. The influence of specialty training, experience, discussion and reflection on decision making in modern restorative treatment planning. Br. Dent. J. 2011, 210, 4. [Google Scholar] [CrossRef] [PubMed]
- Kimble, P.; Stuhr, S.; McDonald, N.; Venugopalan, A.; Campos, M.S.; Cavalcanti, B. Decision Making in the Restoration of Endodontically Treated Teeth: Effect of Biomimetic Dentistry Training. Dent. J. 2023, 11, 159. [Google Scholar] [CrossRef]
- Naumann, M.; Kiessling, S.; Seemann, R. Treatment concepts for restoration of endodontically treated teeth: A nationwide survey of dentists in Germany. J. Prosthet. Dent. 2006, 96, 332–338. [Google Scholar] [CrossRef]
- Morgano, S.M.; Hashem, A.F.; Fotoohi, K.; Rose, L. A nationwide survey of contemporary philosophies and techniques of restoring endodontically treated teeth. J. Prosthet. Dent. 1994, 72, 259–267. [Google Scholar] [CrossRef]
- Pratt, I.; Aminoshariae, A.; Montagnese, T.A.; Williams, K.A.; Khalighinejad, N.; Mickel, A. Eight-Year Retrospective Study of the Critical Time Lapse between Root Canal Completion and Crown Placement: Its Influence on the Survival of Endodontically Treated Teeth. J. Endod. 2016, 42, 1598–1603. [Google Scholar] [CrossRef]
- Slavicek, G.; Makarevich, A.; Makarevich, I.; Bulatova, K. Concepts, aims, and drawbacks in interdisciplinary dentistry: Results of an international questionnaire. J. Interdiscip. Dent. 2013, 3, 91. [Google Scholar] [CrossRef]
- Analiză de Situație Sănătatea orală. Available online: https://insp.gov.ro/wp-content/uploads/2024/03/SO-1-Analiza-de-situatie-f.pdf (accessed on 3 February 2025).
- Ricucci, D.; Mannocci, F.; Pitt Ford, T.R. A study of periapical lesions correlating the presence of a radiopaque lamina with histological findings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2006, 101, 389–394. [Google Scholar] [CrossRef]
- Çalışkan, M.K.; Kaval, M.E.; Tekin, U.; Ünal, T. Radiographic and histological evaluation of persistent periapical lesions associated with endodontic failures after apical microsurgery. Int. Endod. J. 2016, 49, 1011–1019. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Bingisser, A.C.; Reichart, P.A.; Sendi, P.; Bosshardt, D.D.; von Arx, T. Comparison between Radiographic (2-dimensional and 3-dimensional) and Histologic Findings of Periapical Lesions Treated with Apical Surgery. J. Endod. 2015, 41, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Faggion, C.M., Jr. Is the Evidence Supporting Dental Procedures Strong? A Survey of Cochrane Systematic Reviews in Oral Health. J. Evid.-Based Dent. Pract. 2012, 12, 131–134.e14. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, A.I.K.; Blum, J.; Chen, J.; Baziotis-Kalfas, D.; Dao, A.; Bai, K.; Bekheet, M.; Atwal, N.; Cho, S.S.H.; Ganhewa, M.; et al. Determinants of Clinical Decision Making under Uncertainty in Dentistry: A Scoping Review. Diagnostics 2023, 13, 1076. [Google Scholar] [CrossRef]
- Corsentino, G.; Pedullà, E.; Castelli, L.; Liguori, M.; Spicciarelli, V.; Martignoni, M.; Ferrari, M.; Grandini, S. Influence of Access Cavity Preparation and Remaining Tooth Substance on Fracture Strength of Endodontically Treated Teeth. J. Endod. 2018, 44, 1416–1421. [Google Scholar] [CrossRef] [PubMed]
- Ploumaki, A.; Bilkhair, A.; Tuna, T.; Stampf, S.; Strub, J.R. Success rates of prosthetic restorations on endodontically treated teeth; a systematic review after 6 years. J. Oral Rehabil. 2013, 40, 618–630. [Google Scholar] [CrossRef]
- Sartoretto, S.C.; Shibli, J.A.; Javid, K.; Cotrim, K.; Canabarro, A.; Louro, R.S.; Lowenstein, A.; Mourão, C.F.; Moraschini, V. Comparing the Long-Term Success Rates of Tooth Preservation and Dental Implants: A Critical Review. J. Funct. Biomater. 2023, 14, 142. [Google Scholar] [CrossRef]
- Fransson, H.; Dawson, V. Tooth survival after endodontic treatment. Int. Endod. J. 2023, 56, 140–153. [Google Scholar] [CrossRef]
- Gliga, A.; Gaeta, C.; Salvati, G.; Foschi, F.; Azaripour, A. The Platformless Technique (PFLT): A Minimally Invasive Technique for Removing Separated Instruments: Case Report Study. Ann. Case Rep. 2025, 10, 2175. [Google Scholar] [CrossRef]
- Gillen, B.M.; Looney, S.W.; Gu, L.-S.; Loushine, B.A.; Weller, R.N.; Loushine, R.J.; Pashley, D.H.; Tay, F.R. Impact of the Quality of Coronal Restoration versus the Quality of Root Canal Fillings on Success of Root Canal Treatment: A Systematic Review and Meta-analysis. J. Endod. 2011, 37, 895–902. [Google Scholar] [CrossRef]
- Bhuva, B.; Giovarruscio, M.; Rahim, N.; Bitter, K.; Mannocci, F. The restoration of root filled teeth: A review of the clinical literature. Int. Endod. J. 2021, 54, 509–535. [Google Scholar] [CrossRef]
- Goodacre, C.J.; Spolnik, K.J. The Prosthodontic Management of Endodontically Treated Teeth: A Literature Review. Part I. Success and Failure Data, Treatment Concepts. J. Prosthodont. 1994, 3, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, C.J.; Spolnik, K.J. The Prosthodontic Management of Endodontically Treated Teeth: A Literature Review. Part III. Tooth Preparation Considerations. J. Prosthodont. 1995, 4, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Hancocks, S. Defensive dentistry. Br. Dent. J. 2014, 217, 327. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, C.J.; Spolnik, K.J. The Prosthodontic Management of Endodontically Treated Teeth: A Literature Review. Part II. Maintaining the Apical Seal. J. Prosthodont. 1995, 4, 51–53. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor 1 | Factor 2 | Statistic | p-Value | Significant (Bonferroni Corrected) | |
|---|---|---|---|---|---|
| 1 | Size of the lesion | Radiographic appearance of the lesion | 3875.0 | 1.0 | FALSE |
| 2 | Size of the lesion | Risk of tooth fracture | 4544.5 | 0.00026579870299298943 | TRUE |
| 3 | Size of the lesion | Patient’s financial situation | 3998.0 | 2.5333148609749084 × 10−7 | TRUE |
| 4 | Size of the lesion | Patient’s age | 3362.5 | 5.054794611413946 × 10−9 | TRUE |
| 5 | Size of the lesion | Presence of parafunctional habits | 6825.0 | 1.0 | FALSE |
| 6 | Radiographic appearance of the lesion | Risk of tooth fracture | 3755.0 | 1.5845899673177555 × 10−6 | TRUE |
| 7 | Radiographic appearance of the lesion | Patient’s financial situation | 4405.0 | 4.067956797586387 × 10−7 | TRUE |
| 8 | Radiographic appearance of the lesion | Patient’s age | 3606.5 | 8.554452406846989 × 10−10 | TRUE |
| 9 | Radiographic appearance of the lesion | Presence of parafunctional habits | 6491.5 | 1.0 | FALSE |
| 10 | Risk of tooth fracture | Patient’s financial situation | 2111.5 | 3.74610556252516 × 10−17 | TRUE |
| 11 | Risk of tooth fracture | Patient’s age | 2195.0 | 1.0288567882695264 × 10−18 | TRUE |
| 12 | Risk of tooth fracture | Presence of parafunctional habits | 2321.5 | 2.9566901945733574 × 10−9 | TRUE |
| 13 | Patient’s financial situation | Patient’s age | 6646.0 | 1.0 | FALSE |
| 14 | Patient’s financial situation | Presence of parafunctional habits | 3955.0 | 7.713597598065507 × 10−9 | TRUE |
| 15 | Patient’s age | Presence of parafunctional habits | 2728.5 | 2.3366778678366123 × 10−12 | TRUE |
| Factor 1 | Factor 2 | Statistic | p-Value | Significant (Bonferroni Corrected) | |
|---|---|---|---|---|---|
| 1 | Complexity of the root canal system | Size of the periapical lesion | 3055.5 | 0.00942309800732801 | FALSE |
| 2 | Complexity of the root canal system | Radiographic characteristics of the lesion | 3426.0 | 0.09090837381321469 | FALSE |
| 3 | Complexity of the root canal system | Presence of a fractured instrument within the root canal | 3535.0 | 0.15406392799101443 | FALSE |
| 4 | Complexity of the root canal system | Feasibility of a successful restorative outcome | 2441.5 | 5.68631249962933 × 10−5 | TRUE |
| 5 | Complexity of the root canal system | Patient preference | 3204.0 | 0.027403705329801967 | FALSE |
| 6 | Complexity of the root canal system | Prognosis of the endodontically treated tooth | 3366.5 | 0.06915552397079221 | FALSE |
| 7 | Complexity of the root canal system | Financial considerations | 2481.0 | 8.565811606481425 × 10−5 | TRUE |
| 8 | Size of the periapical lesion | Radiographic characteristics of the lesion | 3627.5 | 0.21991907946614342 | FALSE |
| 9 | Size of the periapical lesion | Presence of a fractured instrument within the root canal | 2585.0 | 0.0002052044869450844 | TRUE |
| 10 | Size of the periapical lesion | Feasibility of a successful restorative outcome | 3048.0 | 0.009710989800152451 | FALSE |
| 11 | Size of the periapical lesion | Patient preference | 2344.0 | 2.0237440865496785 × 10−5 | TRUE |
| 12 | Size of the periapical lesion | Prognosis of the endodontically treated tooth | 4004.0 | 0.7672471076754539 | FALSE |
| 13 | Size of the periapical lesion | Financial considerations | 1775.0 | 1.9902665000139928 × 10−8 | TRUE |
| 14 | Radiographic characteristics of the lesion | Presence of a fractured instrument within the root canal | 2832.0 | 0.0017001905490849063 | TRUE |
| 15 | Radiographic characteristics of the lesion | Feasibility of a successful restorative outcome | 2658.0 | 0.0004160384080060211 | TRUE |
| 16 | Radiographic characteristics of the lesion | Patient preference | 2569.5 | 0.00019124779035497368 | TRUE |
| 17 | Radiographic characteristics of the lesion | Prognosis of the endodontically treated tooth | 3632.5 | 0.23595436286445182 | FALSE |
| 18 | Radiographic characteristics of the lesion | Financial considerations | 1956.5 | 2.1317018227860162 × 10−7 | TRUE |
| 19 | Presence of a fractured instrument within the root canal | Feasibility of a successful restorative outcome | 1684.0 | 4.735348646975183 × 10−9 | TRUE |
| 20 | Presence of a fractured instrument within the root canal | Patient preference | 3323.5 | 0.05375150498927233 | FALSE |
| 21 | Presence of a fractured instrument within the root canal | Prognosis of the endodontically treated tooth | 2720.0 | 0.00075594097039443 | TRUE |
| 22 | Presence of a fractured instrument within the root canal | Financial considerations | 2346.5 | 2.0581099499104012 × 10−5 | TRUE |
| 23 | Feasibility of a successful restorative outcome | Patient preference | 1235.5 | 4.6189821806569014 × 10−12 | TRUE |
| 24 | Feasibility of a successful restorative outcome | Prognosis of the endodontically treated tooth | 2875.5 | 0.0024075203911395108 | FALSE |
| 25 | Feasibility of a successful restorative outcome | Financial considerations | 834.5 | 3.451978225000826 × 10−15 | TRUE |
| 26 | Patient preference | Prognosis of the endodontically treated tooth | 1969.0 | 2.182473830534536 × 10−7 | TRUE |
| 27 | Patient preference | Financial considerations | 2629.0 | 0.0002795080718228816 | TRUE |
| 28 | Prognosis of the endodontically treated tooth | Financial considerations | 1182.5 | 1.823849199508511 × 10−12 | TRUE |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gliga, A.; Gaeta, C.; Foschi, F.; Grandini, S.; Aranguren, J.; Ruiz, X.-F.; Azaripour, A.; Săndulescu, M.; Diaconu, C.T.; Bodnar, D.; et al. A Cross-Sectional Survey Assessing the Factors Influencing Dentists’ Decisions on Post-Endodontic Prosthetic Crown Restoration. J. Clin. Med. 2025, 14, 3632. https://doi.org/10.3390/jcm14113632
Gliga A, Gaeta C, Foschi F, Grandini S, Aranguren J, Ruiz X-F, Azaripour A, Săndulescu M, Diaconu CT, Bodnar D, et al. A Cross-Sectional Survey Assessing the Factors Influencing Dentists’ Decisions on Post-Endodontic Prosthetic Crown Restoration. Journal of Clinical Medicine. 2025; 14(11):3632. https://doi.org/10.3390/jcm14113632
Chicago/Turabian StyleGliga, Alexandru, Carlo Gaeta, Federico Foschi, Simone Grandini, Jose Aranguren, Xavier-Fructuos Ruiz, Adriano Azaripour, Mihai Săndulescu, Cezar Tiberiu Diaconu, Dana Bodnar, and et al. 2025. "A Cross-Sectional Survey Assessing the Factors Influencing Dentists’ Decisions on Post-Endodontic Prosthetic Crown Restoration" Journal of Clinical Medicine 14, no. 11: 3632. https://doi.org/10.3390/jcm14113632
APA StyleGliga, A., Gaeta, C., Foschi, F., Grandini, S., Aranguren, J., Ruiz, X.-F., Azaripour, A., Săndulescu, M., Diaconu, C. T., Bodnar, D., & Imre, M. (2025). A Cross-Sectional Survey Assessing the Factors Influencing Dentists’ Decisions on Post-Endodontic Prosthetic Crown Restoration. Journal of Clinical Medicine, 14(11), 3632. https://doi.org/10.3390/jcm14113632