

Clinical Outcomes of Transradial Versus Transfemoral Approach in Rotational Atherectomy: Results from the Rotational Atherectomy in Calcified Lesions in Korea (ROCK) Registry
 , , , , , , , , , ,
, , , , , , , , , ,
Abstract
1. Introduction
2. Methods
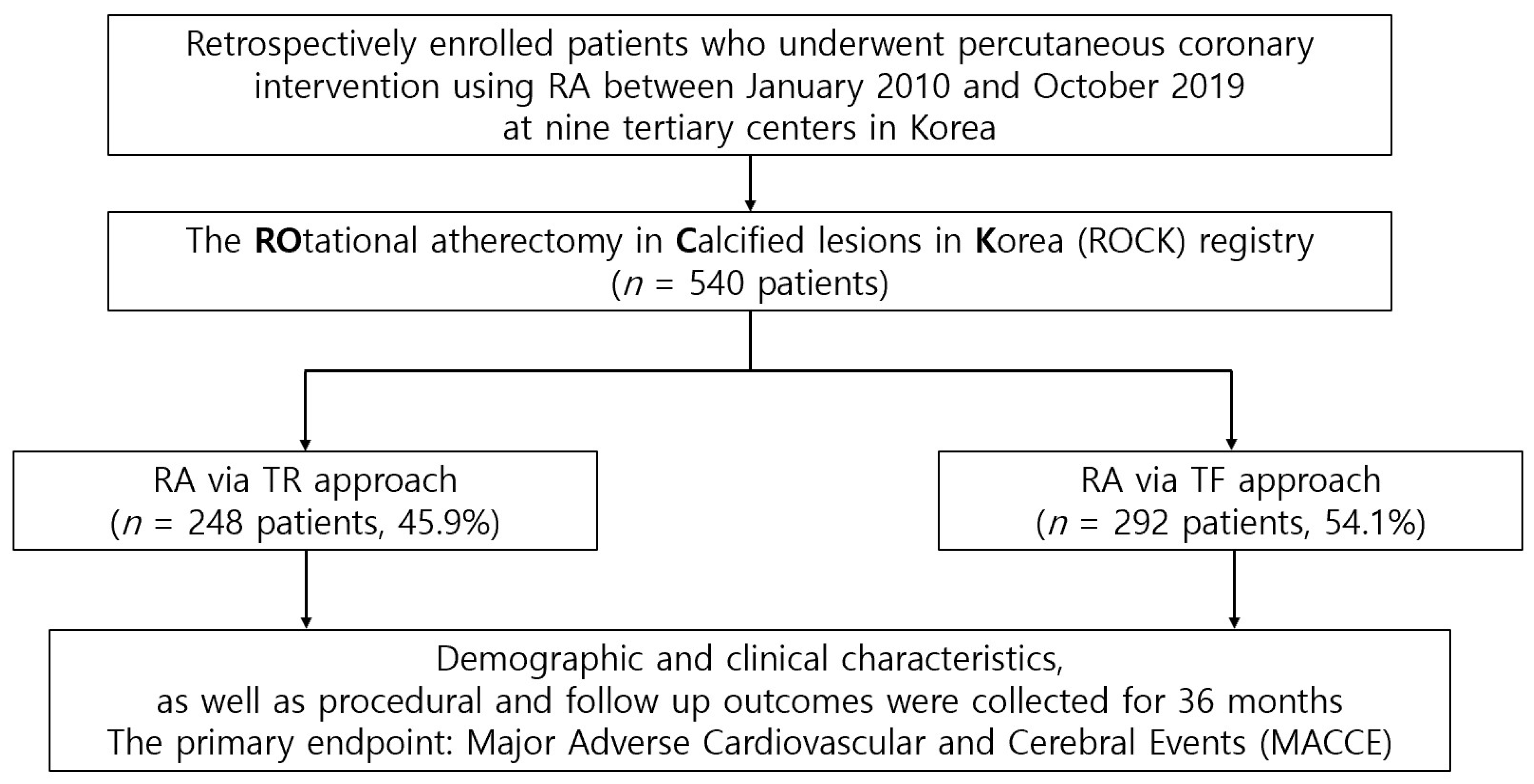
2.1. Study Design and Population
2.2. RA Procedure
2.3. Clinical Outcomes and Definition
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. In-Hospital Events and Procedural Outcomes
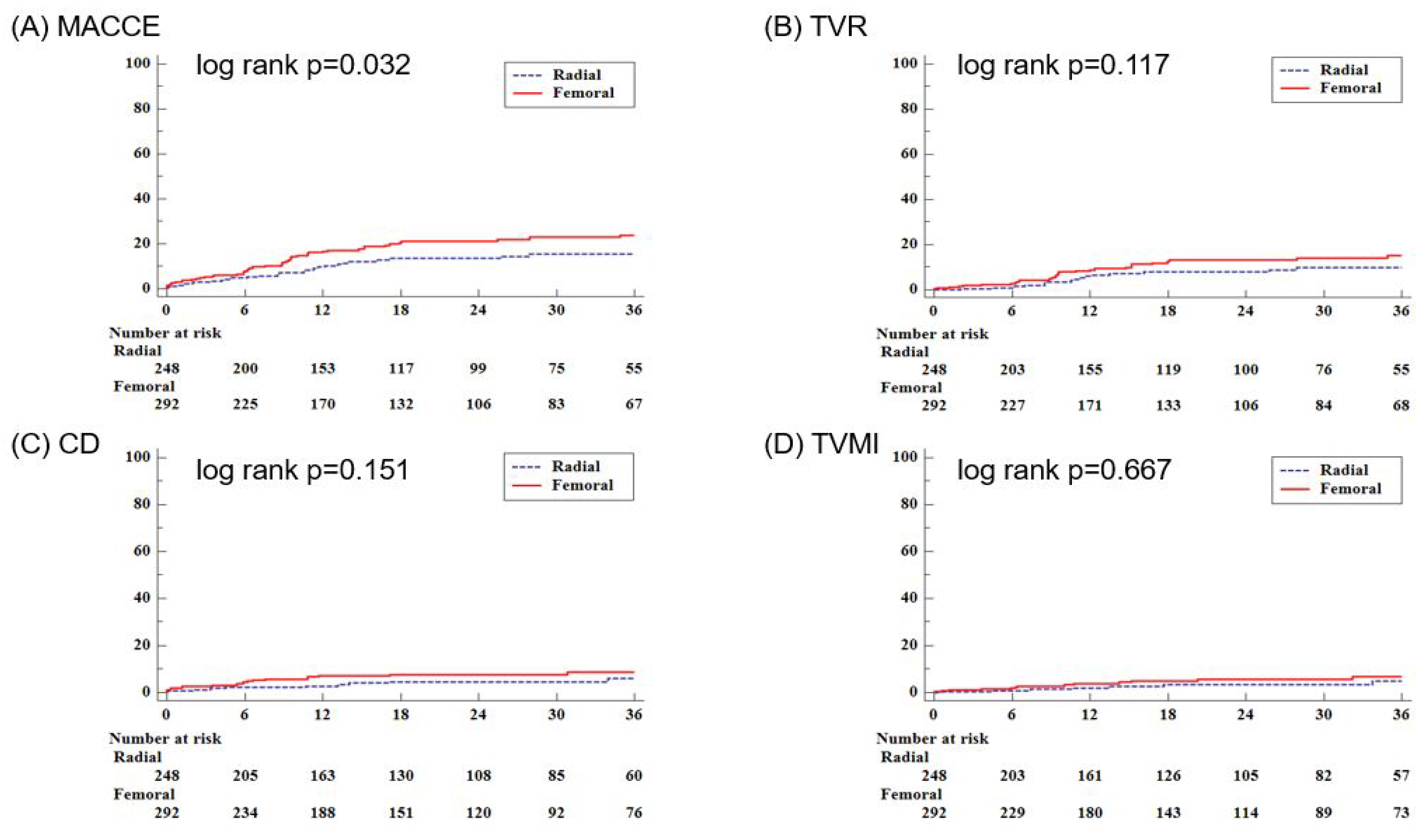
3.3. Clinical Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Madhavan, M.V.; Tarigopula, M.; Mintz, G.S.; Maehara, A.; Stone, G.W.; Genereux, P. Coronary artery calcification: Pathogenesis and prognostic implications. J. Am. Coll. Cardiol. 2014, 63, 1703–1714. [Google Scholar] [CrossRef] [PubMed]
- Vavuranakis, M.; Toutouzas, K.; Stefanadis, C.; Chrisohou, C.; Markou, D.; Toutouzas, P. Stent deployment in calcified lesions: Can we overcome calcific restraint with high-pressure balloon inflations? Catheter. Cardiovasc. Interv. 2001, 52, 164–172. [Google Scholar] [CrossRef]
- Barbato, E.; Carrie, D.; Dardas, P.; Fajadet, J.; Gaul, G.; Haude, M.; Khashaba, A.; Koch, K.; Meyer-Gessner, M.; Palazuelos, J.; et al. European expert consensus on rotational atherectomy. EuroIntervention 2015, 11, 30–36. [Google Scholar] [CrossRef]
- Cavusoglu, E.; Kini, A.S.; Marmur, J.D.; Sharma, S.K. Current status of rotational atherectomy. Catheter. Cardiovasc. Interv. 2004, 62, 485–498. [Google Scholar] [CrossRef] [PubMed]
- Jolly, S.S.; Yusuf, S.; Cairns, J.; Niemela, K.; Xavier, D.; Widimsky, P.; Budaj, A.; Niemela, M.; Valentin, V.; Lewis, B.S.; et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): A randomised, parallel group, multicentre trial. Lancet 2011, 377, 1409–1420. [Google Scholar] [CrossRef]
- Valgimigli, M.; Gagnor, A.; Calabro, P.; Frigoli, E.; Leonardi, S.; Zaro, T.; Rubartelli, P.; Briguori, C.; Ando, G.; Repetto, A.; et al. Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: A randomised multicentre trial. Lancet 2015, 385, 2465–2476. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Sharma, S.K.; Tomey, M.I.; Teirstein, P.S.; Kini, A.S.; Reitman, A.B.; Lee, A.C.; Genereux, P.; Chambers, J.W.; Grines, C.L.; Himmelstein, S.I.; et al. North American Expert Review of Rotational Atherectomy. Circ. Cardiovasc. Interv. 2019, 12, e007448. [Google Scholar] [CrossRef]
- Mota, P.; de Belder, A.; Leitao-Marques, A. Rotational atherectomy: Technical update. Rev. Port. Cardiol. 2015, 34, 271–278. [Google Scholar] [CrossRef]
- Kotowycz, M.A.; Khan, S.Q.; Freixa, X.; Ivanov, J.; Seidelin, P.H.; Overgaard, C.B.; Dzavik, V. Rotational atherectomy through the radial artery is associated with similar procedural success when compared with the transfemoral route. Coron. Artery Dis. 2015, 26, 254–258. [Google Scholar] [CrossRef]
- Watt, J.; Austin, D.; Mackay, D.; Nolan, J.; Oldroyd, K.G. Radial Versus Femoral Access for Rotational Atherectomy: A UK Observational Study of 8622 Patients. Circ. Cardiovasc. Interv. 2017, 10, e005311. [Google Scholar] [CrossRef]
- Watt, J.; Oldroyd, K.G. Radial versus femoral approach for high-speed rotational atherectomy. Catheter. Cardiovasc. Interv. 2009, 74, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Iijima, R. Implications and characteristics of high bleeding risk in East Asian patients undergoing percutaneous coronary intervention: Start with what is right rather than what is acceptable. J. Cardiol. 2021, 78, 91–98. [Google Scholar] [CrossRef]
- Lee, K.; Jung, J.H.; Lee, M.; Kim, D.W.; Park, M.W.; Choi, I.J.; Lee, J.H.; Lee, J.H.; Lee, S.R.; Lee, P.H.; et al. Clinical Outcome of Rotational Atherectomy in Calcified Lesions in Korea-ROCK Registry. Medicina 2021, 57, 694. [Google Scholar] [CrossRef] [PubMed]
- Camnitz, W.M.; Keeley, E.C. Heavily calcified coronary arteries: The bane of an interventionalist’s existence. J. Interv. Cardiol. 2010, 23, 254–255. [Google Scholar] [CrossRef]
- Kinnaird, T.; Cockburn, J.; Gallagher, S.; Choudhury, A.; Sirker, A.; Ludman, P.; de Belder, M.; Copt, S.; Mamas, M.; de Belder, A. Temporal changes in radial access use, associates and outcomes in patients undergoing PCI using rotational atherectomy between 2007 and 2014: Results from the British Cardiovascular Intervention Society national database. Am. Heart J. 2018, 198, 46–54. [Google Scholar] [CrossRef]
- Ramsdale, D.R.; Morris, J.L. If Rotablator is useful, why don’t we use it? Heart 1997, 78 (Suppl. 2), 36–37. [Google Scholar] [CrossRef] [PubMed]
- Genereux, P.; Madhavan, M.V.; Mintz, G.S.; Maehara, A.; Kirtane, A.J.; Palmerini, T.; Tarigopula, M.; McAndrew, T.; Lansky, A.J.; Mehran, R.; et al. Relation between coronary calcium and major bleeding after percutaneous coronary intervention in acute coronary syndromes (from the Acute Catheterization and Urgent Intervention Triage Strategy and Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction Trials). Am. J. Cardiol. 2014, 113, 930–935. [Google Scholar]
- Achim, A.; Kakonyi, K.; Jambrik, Z.; Olajos, D.; Nemes, A.; Bertrand, O.F.; Ruzsa, Z. Distal Radial Artery Access for Recanalization of Radial Artery Occlusion and Repeat Intervention: A Single Center Experience. J. Clin. Med. 2022, 11, 6916. [Google Scholar] [CrossRef]
- Khan, A.A.; Panchal, H.B.; Zaidi, S.I.M.; Papireddy, M.R.; Mukherjee, D.; Cohen, M.G.; Banerjee, S.; Rao, S.V.; Pancholy, S.; Paul, T.K. Safety and efficacy of radial versus femoral access for rotational Atherectomy: A systematic review and meta-analysis. Cardiovasc. Revasc. Med. 2019, 20, 241–247. [Google Scholar] [CrossRef]
- Desta, L.; Jurga, J.; Volz, S.; Omerovic, E.; Ulvenstam, A.; Zwackman, S.; Pagonis, C.; Calle, F.; Olivecrona, G.K.; Persson, J.; et al. Transradial versus trans-femoral access site in high-speed rotational atherectomy in Sweden. Int. J. Cardiol. 2022, 352, 45–51. [Google Scholar] [CrossRef]
- Kubler, P.; Zimoch, W.; Kosowski, M.; Tomasiewicz, B.; Telichowski, A.; Reczuch, K. In patients undergoing percutaneous coronary intervention with rotational atherectomy radial access is safer and as efficient as femoral access. J. Interv. Cardiol. 2018, 31, 471–477. [Google Scholar] [CrossRef] [PubMed]
- You, W.; Wu, X.Q.; Ye, F.; Chen, S.L. Advantages of Transradial Rotational Atherectomy versus Transfemoral Approach in Elderly Patients with Hard-Handling Calcified Coronary Lesions—A Single Center Experience. Acta Cardiol. Sin. 2018, 34, 464–471. [Google Scholar] [PubMed]
- Kim, J.Y.; Yoon, J. Transradial approach as a default route in coronary artery interventions. Korean Circ. J. 2011, 41, 1–8. [Google Scholar] [CrossRef]
- Whitlow, P.L.; Bass, T.A.; Kipperman, R.M.; Sharaf, B.L.; Ho, K.K.; Cutlip, D.E.; Zhang, Y.; Kuntz, R.E.; Williams, D.O.; Lasorda, D.M.; et al. Results of the study to determine rotablator and transluminal angioplasty strategy (STRATAS). Am. J. Cardiol. 2001, 87, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Safian, R.D.; Feldman, T.; Muller, D.W.; Mason, D.; Schreiber, T.; Haik, B.; Mooney, M.; O’Neill, W.W. Coronary angioplasty and Rotablator atherectomy trial (CARAT): Immediate and late results of a prospective multicenter randomized trial. Catheter. Cardiovasc. Interv. 2001, 53, 213–220. [Google Scholar] [CrossRef]
- Allali, A.; Abdel-Wahab, M.; Elbasha, K.; Mankerious, N.; Traboulsi, H.; Kastrati, A.; El-Mawardy, M.; Hemetsberger, R.; Sulimov, D.S.; Neumann, F.J.; et al. Rotational atherectomy of calcified coronary lesions: Current practice and insights from two randomized trials. Clin. Res. Cardiol. 2023, 112, 1143–1163. [Google Scholar] [CrossRef]
- Kassimis, G.; Patel, N.; Kharbanda, R.K.; Channon, K.M.; Banning, A.P. High-speed rotational atherectomy using the radial artery approach and a sheathless guide: A single-centre comparison with the “conventional” femoral approach. EuroIntervention 2014, 10, 694–699. [Google Scholar] [CrossRef]
- Achim, A.; Peter, O.A.; Cocoi, M.; Serban, A.; Mot, S.; Dadarlat-Pop, A.; Nemes, A.; Ruzsa, Z. Correlation between Coronary Artery Disease with Other Arterial Systems: Similar, Albeit Separate, Underlying Pathophysiologic Mechanisms. J. Cardiovasc. Dev. Dis. 2023, 10, 210. [Google Scholar] [CrossRef]
- Yin, W.H.; Tseng, C.K.; Tsao, T.P.; Jen, H.L.; Huang, W.P.; Huang, C.L.; Wang, J.J.; Young, M.S. Transradial versus transfemoral rotablation for heavily calcified coronary lesions in contemporary drug-eluting stent era. J. Geriatr. Cardiol. 2015, 12, 489–496. [Google Scholar]
- Sheth, R.A.; Walker, T.G.; Saad, W.E.; Dariushnia, S.R.; Ganguli, S.; Hogan, M.J.; Hohenwalter, E.J.; Kalva, S.P.; Rajan, D.K.; Stokes, L.S.; et al. Quality improvement guidelines for vascular access and closure device use. J. Vasc. Interv. Radiol. 2014, 25, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Armillotta, M.; Bergamaschi, L.; Paolisso, P.; Belmonte, M.; Angeli, F.; Sansonetti, A.; Stefanizzi, A.; Bertolini, D.; Bodega, F.; Amicone, S.; et al. Prognostic Relevance of Type 4a Myocardial Infarction and Periprocedural Myocardial Injury in Patients with Non-ST-Segment-Elevation Myocardial Infarction. Circulation 2025, 151, 760–772. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, R.A.; Townsend, J.C.; Bonnema, D.D.; Patel, C.A.; Gibbons, M.T.; Todoran, T.M.; Nielsen, C.D.; Powers, E.R.; Steinberg, D.H. Comparison of percutaneous coronary intervention safety before and during the establishment of a transradial program at a teaching hospital. Am. J. Cardiol. 2012, 109, 1154–1159. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| TR Approach (n = 248) | TF Approach (n = 292) | p-Value | |
|---|---|---|---|
| Age, years | 72.5 ± 9.4 | 70.5 ± 10.6 | 0.024 |
| Sex | 0.069 | ||
| Male | 138 (55.7) | 185 (63.4) | |
| Female | 110 (44.3) | 107 (36.6) | |
| BMI | 24.6 ± 3.8 | 24.0 ± 4.0 | 0.073 |
| Smoking | 39 (15.7) | 64 (21.9) | 0.068 |
| HTN | 184 (74.2) | 231 (79.1) | 0.177 |
| DM | 132 (53.2) | 173 (59.3)) | 0.160 |
| Dyslipidemia | 110 (44.4) | 125 (42.8) | 0.718 |
| Family history of CAD | 5 (2.0) | 6 (2.1) | 0.975 |
| CKD | 28 (11.3) | 68 (23.3) | <0.001 |
| Dialysis | 4 (1.6) | 45 (15.4) | <0.001 |
| Previous PCI | 54 (21.8) | 85 (29.1) | 0.052 |
| Previous CABG | 4 (1.6) | 20 (6.9) | 0.003 |
| Previous MI | 24 (9.7) | 42 (14.4)) | 0.096 |
| CVA | 36 (14.5) | 39 (13.4) | 0.698 |
| PVD | 10 (4.0) | 29 (9.9) | 0.008 |
| Heart failure | 22(8.9) | 55(18.8) | 0.001 |
| Atrial fibrillation | 25 (10.1) | 24 (8.2) | 0.453 |
| Clinical diagnosis | 0.558 | ||
| Stable angina | 80 (32.3) | 94 (32.2) | |
| Unstable angina | 87 (35.1) | 88 (30.1) | |
| NSTEMI | 60 (24.2) | 74 (25.3) | |
| STEMI | 6 (2.4) | 13 (4.5) | |
| Silent ischemia | 15 (6.1) | 22 (7.5) | |
| Triglyceride | 120.4 ± 69.8 | 119.0 ± 77.7 | 0.838 |
| Total cholesterol | 147.2 ± 35.9 | 140.4 ± 40.8 | 0.047 |
| LDL cholesterol | 88.6 ± 44.6 | 81.3 ± 34.1 | 0.048 |
| HDL cholesterol | 46.7 ± 14.7 | 45.5 ± 14.4 | 0.350 |
| hsCRP | 2.0 ± 4.8 | 3.9 ± 12.5 | 0.107 |
| HbA1c | 6.8 ± 1.4 | 6.6 ± 1.4 | 0.240 |
| Hemoglobin | 12.6 ± 2.9 | 12.1 ± 1.9 | 0.014 |
| Platelet count | 225.3 ± 67.8 | 214.0 ± 73.3 | 0.065 |
| Drug | |||
| DOAC | 12 (4.8) | 4 (1.4) | 0.018 |
| DAPT | 241 (97.2) | 278 (95.2) | 0.238 |
| Aspirin | 241 (97.2) | 288 (98.6) | 0.234 |
| P2Y12 inhibitor | 244 (98.4) | 286 (98.0) | 0.760 |
| Statin | 231 (93.2) | 271(92.8) | 0.879 |
| TR Approach (n = 248) | TF Approach (n = 292) | p-Value | |
|---|---|---|---|
| Lesion classification | 0.823 | ||
| A, n (%) | 1 (0.4) | 2 (0.7) | |
| B1, n (%) | 20 (8.1) | 20 (6.9) | |
| B2, n (%) | 26 (10.5) | 26 (8.9) | |
| C, n (%) | 201 (81.1) | 244(83.6) | |
| Vessel diseases | 0.815 | ||
| 1VD, n (%) | 56 (22.6) | 60 (20.6) | |
| 2VD, n (%) | 76 (30.7) | 95 (32.5) | |
| 3VD, n (%) | 116 (46.8) | 137 (46.9) | |
| MVD, n (%) | 192 (77.4) | 232 (79.5) | 0.567 |
| LM disease | 31 (12.5) | 43 (14.7) | 0.454 |
| pre EF | 55.5 ± 12.2 | 50.9 ± 14.0 | <0.001 |
| Use of IVUS | 120 (48.4) | 129 (44.2) | 0.328 |
| Mean stent diameter, mm | 3.0 ± 0.4 | 3.0 ± 0.4 | 0.270 |
| Total number of stent, mm | 2.2 ± 1.1 | 2.5 ± 1.2 | 0.001 |
| Total stent length, mm | 61.8 ± 32.4 | 70.7 ± 35.2 | 0.004 |
| Max burr size, mm | 1.50 ± 0.20 | 1.50 ± 0.20 | 0.367 |
| Procedure time, min | 72.4 ± 38.1 | 85.1 ± 58.7 | 0.004 |
| Procedure success, n (%) | 242 (97.6) | 278 (95.2) | 0.145 |
| TR Approach (n = 248) | TF Approach (n = 292) | p-Value | |
|---|---|---|---|
| In-hospital events | |||
| In-hospital MACCE, n (%) | 28 (11.3) | 32 (11.0) | 0.903 |
| In-hospital death, n (%) | 5 (2.0) | 6 (2.1) | 0.975 |
| Urgent CABG/PCI, n (%) | 2 (0.8) | 7 (2.4) | 0.189 |
| Peri-procedural MI, n (%) | 21 (8.5) | 24 (8.2) | 0.917 |
| In-hospital CVA, n (%) | 1 (0.4) | 1 (0.3) | >0.999 |
| Procedural outcomes | |||
| Coronary dissection, n (%) | 20 (8.0) | 26 (9.0) | 0.680 |
| Temporary pacemaker during procedure, n (%) | 2 (0.8) | 14 (4.8) | 0.007 |
| Coronary perforation, n (%) | 4 (1.6) | 6 (2.1) | 0.760 |
| In-hospital bleeding, n (%) | 8 (3.2) | 19 (6.5) | 0.081 |
| TR Approach (n = 248) | TF Approach (n = 292) | p-Value | Univariate HR (95% CI) | p-Value | Multivariate HR ** (95% CI) | p-Value | |
|---|---|---|---|---|---|---|---|
| MACCE | 28 (11.3) | 52 (17.8) | 0.034 | 1.643 (1.038–2.601) | 0.034 | 1.520 (0.889–2.600) | 0.126 |
| All cause of death | 20 (8.1) | 26 (8.9) | 0.728 | 1.124 (0.627–2.013) | 0.695 | 1.230 (0.610–2.482) | 0.562 |
| Cardiac death | 10 (4.0) | 20 (6.9) | 0.154 | 1.732 (0.811–3.700) | 0.156 | 1.699 (0.686–4.205) | 0.252 |
| MI | 7 (2.8) | 13 (4.5) | 0.318 | 1.639 (0.654–4.108) | 0.292 | 1.601 (0.536–4.786) | 0.400 |
| RR | 21 (8.5) | 33 (11.3) | 0.274 | 1.399 (0.809–2.417) | 0.230 | 1.140 (0.615–2.114) | 0.676 |
| TVR | 16 (6.5) | 29 (9.9) | 0.145 | 1.622 (0.881–2.986) | 0.121 | 1.212 (0.606–2.424) | 0.587 |
| TLR | 13 (5.2) | 25 (8.6) | 0.133 | 1.706 (0.873–3.334) | 0.118 | 1.245 (0.582–2.663) | 0.572 |
| CVA | 4 (1.6) | 6 (2.1) | 0.760 | 1.301 (0.367–4.610) | 0.684 | 1.479 (0.230–9.512) | 0.681 |
| ST | 2 (0.8) | 5 (1.7) | 0.461 | 2.163 (0.420–11.151) | 0.356 | 2.224 (0.343–14.414) | 0.402 |
| Total bleeding | 13 (5.2) | 19 (6.5) | 0.535 | 1.280 (0.632–2.592) | 0.493 | 1.214 (0.526–2.802) | 0.649 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.; Jung, J.; Her, S.-H.; Lee, K.; Jung, J.-H.; Yoo, K.-D.; Moon, K.-W.; Moon, D.; Lee, S.-N.; Jang, W.-Y.; et al. Clinical Outcomes of Transradial Versus Transfemoral Approach in Rotational Atherectomy: Results from the Rotational Atherectomy in Calcified Lesions in Korea (ROCK) Registry. J. Clin. Med. 2025, 14, 3066. https://doi.org/10.3390/jcm14093066
Kim K, Jung J, Her S-H, Lee K, Jung J-H, Yoo K-D, Moon K-W, Moon D, Lee S-N, Jang W-Y, et al. Clinical Outcomes of Transradial Versus Transfemoral Approach in Rotational Atherectomy: Results from the Rotational Atherectomy in Calcified Lesions in Korea (ROCK) Registry. Journal of Clinical Medicine. 2025; 14(9):3066. https://doi.org/10.3390/jcm14093066
Chicago/Turabian StyleKim, Kyunyeon, Jin Jung, Sung-Ho Her, Kyusup Lee, Ji-Hoon Jung, Ki-Dong Yoo, Keon-Woong Moon, Donggyu Moon, Su-Nam Lee, Won-Young Jang, and et al. 2025. "Clinical Outcomes of Transradial Versus Transfemoral Approach in Rotational Atherectomy: Results from the Rotational Atherectomy in Calcified Lesions in Korea (ROCK) Registry" Journal of Clinical Medicine 14, no. 9: 3066. https://doi.org/10.3390/jcm14093066
APA StyleKim, K., Jung, J., Her, S.-H., Lee, K., Jung, J.-H., Yoo, K.-D., Moon, K.-W., Moon, D., Lee, S.-N., Jang, W.-Y., Choi, I.-J., Lee, J.-H., Lee, J.-H., Lee, S.-R., Lee, S.-W., Yun, K.-H., & Lee, H.-J. (2025). Clinical Outcomes of Transradial Versus Transfemoral Approach in Rotational Atherectomy: Results from the Rotational Atherectomy in Calcified Lesions in Korea (ROCK) Registry. Journal of Clinical Medicine, 14(9), 3066. https://doi.org/10.3390/jcm14093066