
Advances in Current Treatment Paradigms for Metastatic Hormone-Sensitive Prostate Cancer


 ,
,
Abstract
1. Introduction
2. Classification and Diagnosis of mHSPCa
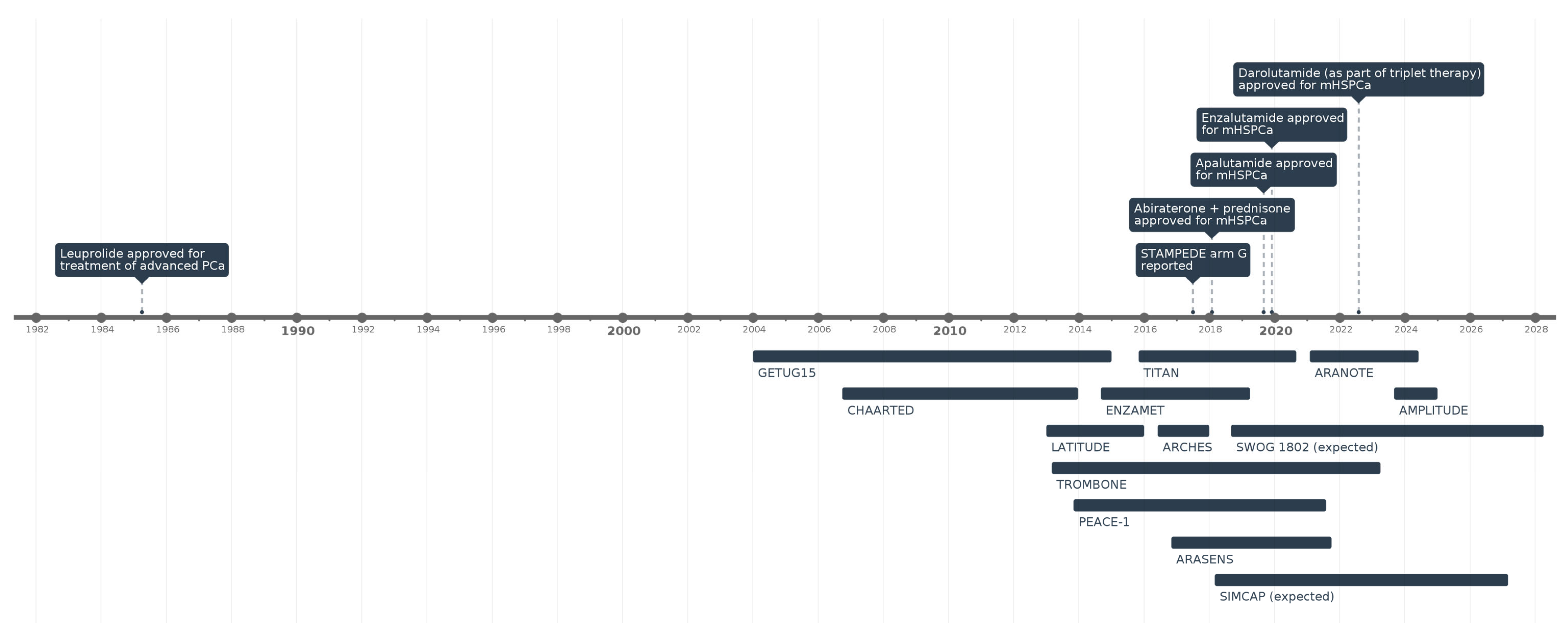
3. Key Clinical Trials and Treatment Strategies
3.1. Doublet Therapy
3.2. Abiraterone
3.3. Enzalutamide
3.4. Apalutamide
3.5. Triplet Therapy
3.6. Radiation Therapy

{kind=link}
| Therapy | Trial | Mechanism of Action | N | Inclusion Criteria | HR for Death | Progression-Free Survival HR | Adverse Events |
|---|---|---|---|---|---|---|---|
| Docetaxel + ADT vs. ADT alone [32] | CHAARTED | Chemohormonal therapy | 790 | Radiologic evidence of metastatic disease | Overall cohort: 0.72 (0.59–0.89) | *C: 0.62 (0.51–0.75) | Neutropenia, febrile neutropenia |
| Docetaxel + ADT vs. ADT alone [37] | STAMPEDE ARM C | Chemohormonal therapy | 2962 | mPCa patients initiating hormone therapy | Overall cohort: 0.78 (0.66–0.93) | *C: 0.61 (0.53–0.71) | Neutropenia, febrile neutropenia |
| Docetaxel + ADT vs. ADT alone [38] | GETUG-15 | Chemohormonal therapy | 385 | Patients with metastatic disease | Overall cohort: ** 1.01 (0.75–1.36) | *R: 0.75 (0.58–0.97) | Neutropenia |
| Abiraterone + prednisone + ADT vs. ADT alone [42,54] | LATITUDE | Androgen biosynthesis inhibitor | 1199 | High-risk mHSPCa | Overall cohort: 0.66 (0.56–0.78) | *R: 0.45 (0.40–0.51) | Hypertension, hypokalemia |
| Abiraterone + ADT vs. ADT alone [44] | STAMPEDE ARM G | Androgen biosynthesis inhibitor | 1917 | mPCa patients initiating hormone therapy | Overall cohort: 0.63 (0.52–0.76) | *C: 0.29 (0.25–0.34) | Hypertension, respiratory disorders |
| Enzalutamide + ADT vs. NSAA SOC [46] | ENZAMET | Androgen receptor signaling inhibitor | 1125 | Patients with metastatic disease | Overall cohort: 0.70 (0.58–0.84) | *B: 0.39 (0.33–0.47) | Fatigue, seizures |
| Enzalutamide + ADT vs. ADT alone [47] | ARCHES | Androgen receptor signaling inhibitor | 1150 | Patients with metastatic disease | Overall cohort: 0.66 (0.53–0.81) | *R: 0.39 (0.30–0.50) | Fatigue, hypertension |
| Apalutamide + ADT vs. ADT alone [48] | TITAN | Androgen receptor signaling inhibitor | 1052 | Patients with metastatic disease | Overall cohort: 0.52 (0.42–0.64) | *R: 0.48 (0.39–0.60) | Rash, hypothyroidism |
| Darolutamide + Docetaxel + ADT vs. docetaxel + ADT [35,49] | ARASENS | Multimodal | 1306 | Candidates for doublet therapy | High-volume cohort: 0.69 (0.57–0.82) | *C: 0.36 (0.30–0.42) | Neutropenia |
| Darolutamide + ADT vs. ADT [50] | ARANOTE | Androgen receptor signaling inhibitor | 669 | Patients with metastatic disease | Overall cohort: ** 0.81 (0.59–1.12) | *R: 0.54 (0.41–0.71) | Fatigue |
| Abiraterone + docetaxel + ADT vs. docetaxel + ADT [51] | PEACE-1 | Multimodal | 1173 | De novo mHSPCa with high metastatic burden | Overall cohort: 0.82 (0.69–0.98) | *R: 0.54 (0.41–0.71) | Neutropenia, hypertension |
| EBRT + ADT + docetaxel vs. ADT + docetaxel [40] | STAMPEDE ARM H | Radiation therapy | 2061 | mPCa patients initiating hormone therapy | Overall cohort: ** 0.92 (0.80–1.06) | ** 0.96 (0.85–1.08) | Urinary incontinence |
| EBRT + ADT vs. ADT alone | HORRAD | Radiation therapy | 432 | Newly diagnosed mHSPCa with PSA > 20 | Overall cohort: ** 0.9 (0.70–1.14) | B: 0.78 (0.63–0.97) | Bowel and urinary symptoms |
| EBRT + ADT | STOPCAP | Radiation therapy | N/A | N/A | Overall cohort: ** 0.92 (0.81–1.04) | B: 0.74 (0.67–0.82) | N/A |
4. Personalized Treatment Considerations and Patient Selection
5. Emerging Therapies and Future Research in mHSPCa
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| mHSPCa | Metastatic Hormone-Sensitive Prostate Cancer |
| CRPC | Castration-Resistant Prostate Cancer |
| PCa | Prostate Cancer |
| ADT | Androgen Deprivation Therapy |
| ARSI | Androgen Receptor Signaling Inhibitor |
| OS | Overall Survival |
| rPFS | Radiographic Progression-Free Survival |
| PFS | Progression-Free Survival |
| PSA | Prostate-Specific Antigen |
| USPSTF | United States Preventive Services Task Force |
| AUA | American Urological Association |
| NCCN | National Comprehensive Cancer Network |
| CT | Computer Tomography |
| MRI | Magnetic Resonance Imaging |
| PSMA PET-CT | Prostate-Specific Membrane Antigen Positron Emission Tomography-Compute Tomography |
| EBRT | External Beam Radiotherapy |
| SNP | Single Nucleotide Polymorphism |
| HR | Hazard Ratio |
| FDA | Food and Drug Administration |
| PD-1 | Programmed Cell Death Protein 1 |
| PARPi | Poly (ADP-ribose) Polymerase Inhibitor |
| HRR | Homologous Recombination Repair |
| SMART | Sequential Multiple Assignment Randomized Trial |
| cRP | Cytoreductive radical prostatectomy |
References
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA Cancer J. Clin. 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA Cancer J. Clin. 2025, 75, 10–45. [Google Scholar] [CrossRef] [PubMed]
- Borregales, L.D.; DeMeo, G.; Gu, X.; Cheng, E.; Dudley, V.; Schaeffer, E.M.; Nagar, H.; Carlsson, S.; Vickers, A.; Hu, J.C. Grade Migration of Prostate Cancer in the United States During the Last Decade. JNCI J. Natl. Cancer Inst. 2022, 114, 1012–1019. [Google Scholar] [CrossRef]
- Jemal, A.; Culp, M.B.; Ma, J.; Islami, F.; A Fedewa, S. Prostate Cancer Incidence 5 Years After US Preventive Services Task Force Recommendations Against Screening. JNCI J. Natl. Cancer Inst. 2021, 113, 64–71. [Google Scholar] [CrossRef]
- Zhang, A.C.; Rasul, R.; Golden, A.; Feuerstein, M.A. Incidence and mortality trends of metastatic prostate cancer: Surveillance, Epidemiology, and End Results database analysis. Can. Urol. Assoc. J. 2021, 15, E637–E643. [Google Scholar] [CrossRef]
- Schafer, E.J.; Jemal, A.; Wiese, D.; Sung, H.; Kratzer, T.B.; Islami, F.; Dahut, W.L.; Knudsen, K.E. Disparities and Trends in Genitourinary Cancer Incidence and Mortality in the USA. Eur. Urol. 2023, 84, 117–126. [Google Scholar] [CrossRef]
- Kelly, S.P.; Anderson, W.F.; Rosenberg, P.S.; Cook, M.B. Past, Current, and Future Incidence Rates and Burden of Metastatic Prostate Cancer in the United States. Eur. Urol. Focus 2018, 4, 121–127. [Google Scholar] [CrossRef]
- Moyer, V.A.; US Preventive Services Task Force. Screening for prostate cancer: US Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2012, 157, 120–134. [Google Scholar] [CrossRef] [PubMed]
- Leapman, M.S.; Wang, R.; Park, H.; Yu, J.B.; Sprenkle, P.C.; Cooperberg, M.R.; Gross, C.P.; Ma, X. Changes in Prostate-Specific Antigen Testing Relative to the Revised US Preventive Services Task Force Recommendation on Prostate Cancer Screening. JAMA Oncol. 2022, 8, 41–47. [Google Scholar] [CrossRef]
- Siegel, D.A.; Elizabeth, O.M.; Richards, T.B.; Dowling, N.F.; Weir, H.K. Prostate cancer incidence and survival, by stage and race/ethnicity—United States, 2001–2017. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1473–1480. [Google Scholar] [CrossRef]
- Wenzel, M.; Preisser, F.; Hoeh, B.; Schroeder, M.; Würnschimmel, C.; Steuber, T.; Heinzer, H.; Banek, S.; Ahrens, M.; Becker, A.; et al. Impact of Time to Castration Resistance on Survival in Metastatic Hormone Sensitive Prostate Cancer Patients in the Era of Combination Therapies. Front. Oncol. 2021, 11, 659135. [Google Scholar]
- Freedland, S.J.; Davis, M.; Epstein, A.J.; Arondekar, B.; Ivanova, J.I. Real-world treatment patterns and overall survival among men with Metastatic Castration-Resistant Prostate Cancer (mCRPC) in the US Medicare population. Prostate Cancer Prostatic Dis. 2024, 27, 327–333. [Google Scholar] [PubMed]
- Djavan, B.; Eastham, J.; Gomella, L.; Tombal, B.; Taneja, S.; Dianat, S.S.; Kazzazi, A.; Shore, N.; Abrahamsson, P.; Cheetham, P.; et al. Testosterone in prostate cancer: The Bethesda consensus. BJU Int. 2012, 110, 344–352. [Google Scholar] [CrossRef]
- Klotz, L.; Breau, R.H.; Collins, L.L.; Gleave, M.E.; Pickles, T.; Pouliot, F.; Saad, F. Maximal testosterone suppression in the management of recurrent and metastatic prostate cancer. Can. Urol. Assoc. J. 2017, 11, 16–23. [Google Scholar]
- Pernar, C.H.; Ebot, E.M.; Wilson, K.M.; Mucci, L.A. The epidemiology of prostate cancer. Cold Spring Harb. Perspect. Medicine. 2018, 8, a030361. [Google Scholar]
- Na, R.; Zheng, S.L.; Han, M.; Yu, H.; Jiang, D.; Shah, S.; Ewing, C.M.; Zhang, L.; Novakovic, K.; Petkewicz, J.; et al. Germline mutations in ATM and BRCA1/2 distinguish risk for lethal and indolent prostate cancer and are associated with early age at death. Eur. Urol. 2017, 71, 740–747. [Google Scholar] [PubMed]
- Ewing, C.M.; Ray, A.M.; Lange, E.M.; Zuhlke, K.A.; Robbins, C.M.; Tembe, W.D.; Wiley, K.E.; Isaacs, S.D.; Johng, D.; Wang, Y.; et al. Germline Mutations in HOXB13 and Prostate-Cancer Risk. N. Engl. J. Med. 2012, 366, 141–149. [Google Scholar]
- Bergengren, O.; Pekala, K.R.; Matsoukas, K.; Fainberg, J.; Mungovan, S.F.; Bratt, O.; Bray, F.; Brawley, O.; Luckenbaugh, A.N.; Mucci, L.; et al. 2022 Update on Prostate Cancer Epidemiology and Risk Factors—A Systematic Review. Eur. Urol. 2023, 84, 191–206. [Google Scholar]
- Shiota, M.; Nemoto, S.; Ikegami, R.; Tatarano, S.; Kamoto, T.; Kobayashi, K.; Sakai, H.; Igawa, T.; Kamba, T.; Fujimoto, N.; et al. Predictive model of castration resistance in advanced prostate cancer by machine learning using genetic and clinical data: KYUCOG-1401-A study. BJC Rep. 2024, 2, 1–8. [Google Scholar]
- Finelli, A.; Beer, T.M.; Chowdhury, S.; Evans, C.P.; Fizazi, K.; Higano, C.S.; Kim, J.; Martin, L.; Saad, F.; Saarela, O. Comparison of joint and landmark modeling for predicting cancer progression in men with castration-resistant prostate cancer: A secondary post hoc analysis of the PREVAIL randomized clinical trial. JAMA Netw. Open 2021, 4, e2112426. [Google Scholar]
- Lowrance, W.; Dreicer, R.; Jarrard, D.F.; Scarpato, K.R.; Kim, S.K.; Kirkby, E.; Buckley, D.I.; Griffin, J.C.; Cookson, M.S. Updates to Advanced Prostate Cancer: AUA/SUO Guideline (2023). J. Urol. 2023, 209, 1082–1090. [Google Scholar] [CrossRef]
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; An, Y.; Bitting, R.; Chapin, B.; Cheng, H.H.; D’Amico, A.V.; Desai, N.; Dorff, T.; et al. NCCN Guidelines® Insights: Prostate Cancer, Version 3.2024: Featured Updates to the NCCN Guidelines. J. Natl. Compr. Cancer Netw. 2024, 22, 140–150. [Google Scholar]
- Lowrance, W.T.; Breau, R.H.; Chou, R.; Chapin, B.F.; Crispino, T.; Dreicer, R.; Jarrard, D.F.; Kibel, A.S.; Morgan, T.M.; Morgans, A.K.; et al. Advanced Prostate Cancer: AUA/ASTRO/SUO Guideline PART I. J. Urol. 2021, 205, 14–21. [Google Scholar]
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; An, Y.; Barocas, D.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; D’Amico, A.V.; et al. Prostate Cancer, Version 4.2023, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN 2023, 21, 1067–1096. [Google Scholar]
- Dyrberg, E.; Hendel, H.W.; Huynh, T.H.V.; Klausen, T.W.; Løgager, V.B.; Madsen, C.; Pedersen, E.M.; Pedersen, M.; Thomsen, H.S. 68Ga-PSMA-PET/CT in comparison with 18F-fluoride-PET/CT and whole-body MRI for the detection of bone metastases in patients with prostate cancer: A prospective diagnostic accuracy study. Eur. Radiol. 2018, 29, 1221–1230. [Google Scholar] [CrossRef]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar]
- Zhou, J.; Gou, Z.; Wu, R.; Yuan, Y.; Yu, G.; Zhao, Y. Comparison of PSMA-PET/CT, choline-PET/CT, NaF-PET/CT, MRI, and bone scintigraphy in the diagnosis of bone metastases in patients with prostate cancer: A systematic review and meta-analysis. Skelet. Radiol. 2019, 48, 1915–1924. [Google Scholar]
- Sonni, I.; Felker, E.R.; Lenis, A.T.; Sisk, A.E.; Bahri, S.; Allen-Auerbach, M.S.; Armstrong, W.R.; Suvannarerg, V.; Tubtawee, T.; Grogan, T.; et al. Head-to-Head Comparison of 68Ga-PSMA-11 PET/CT and mpMRI with a Histopathology Gold Standard in the Detection, Intraprostatic Localization, and Determination of Local Extension of Primary Prostate Cancer: Results from a Prospective Single-Center Imaging Trial. J. Nucl. Med. 2022, 63, 847–854. [Google Scholar]
- Liu, F.; Dong, J.; Shen, Y.; Yun, C.; Wang, R.; Wang, G.; Tan, J.; Wang, T.; Yao, Q.; Wang, B.; et al. Comparison of PET/CT and MRI in the Diagnosis of Bone Metastasis in Prostate Cancer Patients: A Network Analysis of Diagnostic Studies. Front. Oncol. 2021, 11, 736654. [Google Scholar] [CrossRef]
- Lokeshwar, S.D.; Choksi, A.U.; Haltstuch, D.; Rahman, S.N.; Press, B.H.; Syed, J.; Hurwitz, M.E.; Kim, I.Y.; Leapman, M.S. Personalizing approaches to the management of metastatic hormone sensitive prostate cancer: Role of advanced imaging, genetics and therapeutics. World J. Urol. 2023, 41, 2007–2019. [Google Scholar]
- Van Den Bergh, L.; Lerut, E.; Haustermans, K.; Deroose, C.M.; Oyen, R.; Isebaert, S.; Budiharto, T.; Ameye, F.; Mottaghy, F.M.; Bogaerts, K.; et al. Final analysis of a prospective trial on functional imaging for nodal staging in patients with prostate cancer at high risk for lymph node involvement. Urol. Oncol. Semin. Orig. Investig. 2015, 33, 109.e23–109.e31. [Google Scholar] [CrossRef]
- Kyriakopoulos, C.E.; Chen, Y.-H.; Carducci, M.A.; Liu, G.; Jarrard, D.F.; Hahn, N.M.; Shevrin, D.H.; Dreicer, R.; Hussain, M.; Eisenberger, M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J. Clin. Oncol. 2018, 36, 1080–1087. [Google Scholar] [CrossRef]
- Ranasinghe, W.; Chapin, B.F.; Kim, I.Y.; Sooriakumaran, P.; Lawrentschuk, N. The cytoreductive prostatectomy in metastatic prostate cancer: What the individual trials are hoping to answer. BJU Int. 2020, 125, 792–800. [Google Scholar] [CrossRef]
- Sooriakumaran, P.; Wilson, C.; Rombach, I.; Hassanali, N.; Aning, J.; Lamb, A.D.; Cathcart, P.; Eden, C.; Ahmad, I.; Rajan, P.; et al. Feasibility and safety of radical prostatectomy for oligo-metastatic prostate cancer: The Testing Radical prostatectomy in men with prostate cancer and oligo-Metastases to the bone (TRoMbone) trial. BJU Int. 2022, 130, 43–53. [Google Scholar] [CrossRef]
- Hussain, M.; Tombal, B.; Saad, F.; Fizazi, K.; Sternberg, C.N.; Crawford, E.D.; Shore, N.; Kopyltsov, E.; Kalebasty, A.R.; Bögemann, M.; et al. Darolutamide Plus Androgen-Deprivation Therapy and Docetaxel in Metastatic Hormone-Sensitive Prostate Cancer by Disease Volume and Risk Subgroups in the Phase III ARASENS Trial. J. Clin. Oncol. 2023, 41, 3595–3607. [Google Scholar] [CrossRef]
- Tannock, I.F.; De Wit, R.; Berry, W.R.; Horti, J.; Pluzanska, A.; Chi, K.N.; Oudard, S.; Théodore, C.; James, N.D.; Turesson, I.; et al. Docetaxel plus Prednisone or Mitoxantrone plus Prednisone for Advanced Prostate Cancer. N. Engl. J. Med. 2004, 351, 1502–1512. [Google Scholar] [CrossRef]
- James, N.D.; Sydes, M.R.; Clarke, N.W.; Mason, M.D.; Dearnaley, D.P.; Spears, M.R.; Ritchie, A.W.S.; Parker, C.C.; Russell, J.M.; Attard, G.; et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): Survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet 2016, 387, 1163–1177. [Google Scholar] [CrossRef]
- Gravis, G.; Fizazi, K.; Joly, F.; Oudard, S.; Priou, F.; Esterni, B.; Latorzeff, I.; Delva, R.; Krakowski, I.; Laguerre, B.; et al. Androgen-deprivation therapy alone or with docetaxel in non-castrate metastatic prostate cancer (GETUG-AFU 15): A randomised, open-label, phase 3 trial. Lancet Oncol. 2013, 14, 149–158. [Google Scholar] [CrossRef]
- Gravis, G.; Boher, J.-M.; Chen, Y.-H.; Liu, G.; Fizazi, K.; Carducci, M.A.; Oudard, S.; Joly, F.; Jarrard, D.M.; Soulie, M.; et al. Burden of Metastatic Castrate Naive Prostate Cancer Patients, to Identify Men More Likely to Benefit from Early Docetaxel: Further Analyses of CHAARTED and GETUG-AFU15 Studies. Eur. Urol. 2018, 73, 847–855. [Google Scholar] [CrossRef]
- Parker, C.C.; James, N.D.; Brawley, C.D.; Clarke, N.W.; Hoyle, A.P.; Ali, A.; Ritchie, A.W.S.; Attard, G.; Chowdhury, S.; Cross, W.; et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomised controlled phase 3 trial. Lancet 2018, 392, 2353–2366. [Google Scholar] [CrossRef]
- De Bono, J.S.; Logothetis, C.J.; Molina, A.; Fizazi, K.; North, S.; Chu, L.; Chi, K.N.; Jones, R.J.; Goodman, O.B.; Saad, F.; et al. Abiraterone and Increased Survival in Metastatic Prostate Cancer. N. Engl. J. Med. 2011, 364, 1995–2005. [Google Scholar] [CrossRef]
- Fizazi, K.; Tran, N.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Özgüroğlu, M.; Ye, D.; Feyerabend, S.; Protheroe, A.; et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2017, 377, 352–360. [Google Scholar] [CrossRef]
- Fizazi, K.; Shore, N.; Tammela, T.L.; Ulys, A.; Vjaters, E.; Polyakov, S.; Jievaltas, M.; Luz, M.; Alekseev, B.; Kuss, I.; et al. Darolutamide in nonmetastatic, castration-resistant prostate cancer. N. Engl. J. Med. 2019, 380, 1235–1246. [Google Scholar] [CrossRef]
- James, N.D.; De Bono, J.S.; Spears, M.R.; Clarke, N.W.; Mason, M.D.; Dearnaley, D.P.; Ritchie, A.W.S.; Amos, C.L.; Gilson, C.; Jones, R.J.; et al. Abiraterone for Prostate Cancer Not Previously Treated with Hormone Therapy. N. Engl. J. Med. 2017, 377, 338–351. [Google Scholar] [CrossRef]
- Rush, H.L.; Murphy, L.; Morgans, A.K.; Clarke, N.W.; Cook, A.D.; Attard, G.; Macnair, A.; Dearnaley, D.P.; Parker, C.C.; Russell, J.M.; et al. Quality of Life in Men with Prostate Cancer Randomly Allocated to Receive Docetaxel or Abiraterone in the STAMPEDE Trial. J. Clin. Oncol. 2022, 40, 825–836. [Google Scholar] [CrossRef]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.G.; et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef]
- Armstrong, A.J.; Szmulewitz, R.Z.; Petrylak, D.P.; Holzbeierlein, J.; Villers, A.; Azad, A.; Alcaraz, A.; Alekseev, B.; Iguchi, T.; Shore, N.D.; et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy with Enzalutamide or Placebo in Men with Metastatic Hormone-Sensitive Prostate Cancer. J. Clin. Oncol. 2019, 37, 2974–2986. [Google Scholar]
- Chi, K.N.; Agarwal, N.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, R.; Juárez Soto, Á.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H. Apalutamide for metastatic, castration-sensitive prostate cancer. N. Engl. J. Med. 2019, 381, 13–24. [Google Scholar]
- Smith, M.R.; Hussain, M.; Saad, F.; Fizazi, K.; Sternberg, C.N.; Crawford, E.D.; Kopyltsov, E.; Park, C.H.; Alekseev, B.; Montesa-Pino, Á.; et al. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N. Engl. J. Med. 2022, 386, 1132–1142. [Google Scholar]
- Saad, F.; Vjaters, E.; Shore, N.; Olmos, D.; Xing, N.; Gomes, A.J.P.d.S.; Mota, A.C.d.A.; Salman, P.; Jievaltas, M.; Ulys, A.; et al. Darolutamide in Combination with Androgen-Deprivation Therapy in Patients with Metastatic Hormone-Sensitive Prostate Cancer From the Phase III ARANOTE Trial. J. Clin. Oncol. 2024, 42, 4271–4281. [Google Scholar]
- Fizazi, K.; Foulon, S.; Carles, J.; Roubaud, G.; McDermott, R.; Fléchon, A.; Tombal, B.; Supiot, S.; Berthold, D.; Ronchin, P.; et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet 2022, 399, 1695–1707. [Google Scholar] [CrossRef]
- Boevé, L.M.; Hulshof, M.C.; Vis, A.N.; Zwinderman, A.H.; Twisk, J.W.; Witjes, W.P.; Delaere, K.P.; van Moorselaar, R.J.A.; Verhagen, P.C.; van Andel, G. Effect on Survival of Androgen Deprivation Therapy Alone Compared to Androgen Deprivation Therapy Combined with Concurrent Radiation Therapy to the Prostate in Patients with Primary Bone Metastatic Prostate Cancer in a Prospective Randomised Clinical Trial: Data from the HORRAD Trial. Eur. Urol. 2019, 75, 410–418. [Google Scholar]
- Burdett, S.; Boevé, L.M.; Ingleby, F.C.; Fisher, D.J.; Rydzewska, L.H.; Vale, C.L.; van Andel, G.; Clarke, N.W.; Hulshof, M.C.; James, N.D.; et al. Prostate Radiotherapy for Metastatic Hormone-sensitive Prostate Cancer: A STOPCAP Systematic Review and Meta-analysis. Eur. Urol. 2019, 76, 115–124. [Google Scholar]
- Rydzewska, L.H.; Burdett, S.; Vale, C.L.; Clarke, N.W.; Fizazi, K.; Kheoh, T.; Mason, M.D.; Miladinovic, B.; James, N.D.; Parmar, M.K.; et al. Adding abiraterone to androgen deprivation therapy in men with metastatic hormone-sensitive prostate cancer: A systematic review and meta-analysis. Eur. J. Cancer 2017, 84, 88–101. [Google Scholar] [CrossRef]
- Sweeney, C.J.; Chen, Y.-H.; Carducci, M.; Liu, G.; Jarrard, D.F.; Eisenberger, M.; Wong, Y.-N.; Hahn, N.; Kohli, M.; Cooney, M.M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N. Engl. J. Med. 2015, 373, 737–746. [Google Scholar]
- Tucci, M.; Bertaglia, V.; Vignani, F.; Buttigliero, C.; Fiori, C.; Porpiglia, F.; Scagliotti, G.V.; Di Maio, M. Addition of Docetaxel to Androgen Deprivation Therapy for Patients with Hormone-sensitive Metastatic Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. 2016, 69, 563–573. [Google Scholar] [CrossRef]
- Yin, L.; Hu, Q. CYP17 inhibitors—Abiraterone, C17,20-lyase inhibitors and multi-targeting agents. Nat. Rev. Urol. 2014, 11, 32–42. [Google Scholar]
- Cao, B.; Kim, M.; Reizine, N.M.; Moreira, D.M. Adverse Events and Androgen Receptor Signaling Inhibitors in the Treatment of Prostate Cancer: A Systematic Review and Multivariate Network Meta-analysis. Eur. Urol. Oncol. 2023, 6, 237–250. [Google Scholar] [CrossRef]
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.E.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Bhattacharya, S.; Carles, J.; Chowdhury, S.; et al. Enzalutamide in Metastatic Prostate Cancer before Chemotherapy. N. Engl. J. Med. 2014, 371, 424–433. [Google Scholar] [CrossRef]
- Nadal, R.; Taplin, M.-E.; Bellmunt, J. Enzalutamide for the Treatment of Prostate Cancer: Results and Implications of the AFFIRM Trial. Futur. Oncol. 2014, 10, 351–362. [Google Scholar] [CrossRef]
- Omer, D.M.; Shah, F.; Luthra, A.; Chen, C.-T.; Lee, C.I.; Williams, H.; Walch, H.; Verheij, F.S.; Rosen, R.; Alvarez, J.; et al. Clinical and Genomic Characterization of Secondary Rectal Cancer After Radiotherapy for Prostate Cancer. JAMA Netw. Open 2025, 8, e251039. [Google Scholar] [CrossRef]
- Monda, S.; Pratsinis, M.; Lui, H.; Noel, O.; Chandrasekar, T.; Evans, C.P.; Dall’Era, M.A. Secondary Bladder Cancer After Prostate Cancer Treatment: An Age-matched Comparison Between Radiation and Surgery. Eur. Urol. Focus 2024, 10, 448–453. [Google Scholar] [CrossRef]
- Demus, T.; Getzenberg, R.H.; Nieder, A.M. Understanding Prescribing Differences Between Urologists and Medical Oncologists in the Management of Advanced Prostate Cancer. Urol. Pr. 2023, 10, 90–97. [Google Scholar] [CrossRef]
- Caram, M.E.; Kaufman, S.R.; Modi, P.K.; Herrel, L.; Oerline, M.; Ross, R.; Skolarus, T.A.; Hollenbeck, B.K.; Shahinian, V. Adoption of Abiraterone and Enzalutamide by Urologists. Urology 2019, 131, 176–183. [Google Scholar] [CrossRef]
- Heath, E.I.; Dyson, G.E.; Cackowski, F.C.; Hafron, J.; Powell, I. Treatment Intensification Patterns and Utilization in Patients with Metastatic Castration-Sensitive Prostate Cancer. Clin. Genitourin. Cancer 2022, 20, 524–532. [Google Scholar] [CrossRef]
- Liao, Y.; Grobholz, R.; Abel, U.; Trojan, L.; Michel, M.S.; Angel, P.; Mayer, D. Increase of AKT/PKB expression correlates with gleason pattern in human prostate cancer. Int. J. Cancer 2003, 107, 676–680. [Google Scholar] [CrossRef]
- McMenamin, M.E.; Soung, P.; Perera, S.; Kaplan, I.; Loda, M.; Sellers, W.R. Loss of PTEN expression in paraffin-embedded primary prostate cancer correlates with high Gleason score and advanced stage. Cancer Res. 1999, 59, 4291–4296. [Google Scholar]
- Bitting, R.L.; Armstrong, A.J. Targeting the PI3K/Akt/mTOR pathway in castration-resistant prostate cancer. Endocr. Relat. Cancer 2013, 20, R83–R99. [Google Scholar] [CrossRef]
- Fizazi, K.; George, D.J.; De Santis, M.; Clarke, N.; Fay, A.P.; Uemura, H.; Grinsted, L.; Rooney, C.; Verheijen, R.; Anjum, R.; et al. A phase III trial of capivasertib and abiraterone versus placebo and abiraterone in patients with de novo metastatic hormone-sensitive prostate cancer characterized by PTEN deficiency (CAPItello-281). J. Clin. Oncol. 2021, 39, TPS178. [Google Scholar] [CrossRef]
- Chi, K.N.; Agarwal, N.; Armstrong, A.J.; Hellmis, E.; Schlürmann, F.; Sugimoto, M.; Ürün, Y.; Xing, N.; Aregay, M.; Lima, J.; et al. Phase III, double-blind, placebo-controlled, 2-cohort, randomized study of saruparib (AZD5305) in combination with new hormonal agents in patients with metastatic castration-sensitive prostate cancer with and without homologous recombination repair mutation (EvoPAR-Prostate01). J. Clin. Oncol. 2024, 42, TPS5123. [Google Scholar]
- Rathkopf, D.E.; Chi, K.N.; Olmos, D.; Cheng, H.H.; Agarwal, N.; Graff, J.N.; Sandhu, S.K.; Hayreh, V.; Lopez-Gitlitz, A.; Francis, P.S.J.; et al. AMPLITUDE: A study of niraparib in combination with abiraterone acetate plus prednisone (AAP) versus AAP for the treatment of patients with deleterious germline or somatic homologous recombination repair (HRR) gene-altered metastatic castration-sensitive prostate cancer (mCSPC). J. Clin. Oncol. 2021, 39, TPS176. [Google Scholar]
- Gu, W.; Han, W.; Luo, H.; Zhou, F.; He, D.; Ma, L.; Guo, H.; Liang, C.; Chong, T.; Jiang, J.; et al. Rezvilutamide versus bicalutamide in combination with androgen-deprivation therapy in patients with high-volume, metastatic, hormone-sensitive prostate cancer (CHART): A randomised, open-label, phase 3 trial. Lancet Oncol. 2022, 23, 1249–1260. [Google Scholar]
- Comparing a 6-month vs. Long-term Course of Rezvilutamide With ADT Plus Chemotherapy in mHSPC. Available online: https://clinicaltrials.gov/study/NCT05956639?term=Comparing%20a%206-month%20vs%20Long-term%20Course%20of%20Rezvilutamide%20With%20ADT%20Plus%20Chemotherapy%20in%20mHSPC.&rank=1 (accessed on 14 February 2025).
- Abello, A.; Kenney, P.A. Unified Approaches to Surgery and Systemic Therapy for Renal Cell Carcinoma. In Renal Cancer: Contemporary Management; Libertino, J.A., Gee, J.R., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 411–435. [Google Scholar]
- Fan, J.; Xu, K.; Jiang, Z.; Gan, C.; Song, H.; Gao, G.; Wang, G.; Kang, Q.; Luo, L.; Wang, Z.; et al. Role of 18F-PSMA-1007 PET/CT-derived quantitative volumetric tumor parameters in cytoreductive radical prostatectomy selection for patients with low-volume metastatic hormone-sensitive prostate cancer: A retrospective study. BMC Cancer 2025, 25, 1–11. [Google Scholar]
- Heidenreich, A.; Pfister, D.; Porres, D. Cytoreductive Radical Prostatectomy in Patients with Prostate Cancer and Low Volume Skeletal Metastases: Results of a Feasibility and Case-Control Study. J. Urol. 2015, 193, 832–838. [Google Scholar]
- Culp, S.H.; Schellhammer, P.F.; Williams, M.B. Might Men Diagnosed with Metastatic Prostate Cancer Benefit from Definitive Treatment of the Primary Tumor? A SEER-Based Study. Eur. Urol. 2014, 65, 1058–1066. [Google Scholar] [CrossRef]
- Antwi, S.; Everson, T.M. Prognostic impact of definitive local therapy of the primary tumor in men with metastatic prostate cancer at diagnosis: A population-based, propensity score analysis. Cancer Epidemiol. 2014, 38, 435–441. [Google Scholar]
- Cytoreductive Prostatectomy Combined With Triple or Dual Systemic Therapy in mHSPC Patients. Available online: https://clinicaltrials.gov/study/NCT06350825?term=Cytoreductive%20Prostatectomy%20Combined%20With%20Triple%20or%20Dual%20Systemic%20Therapy%20in%20mHSPC%20Patients.&rank=1 (accessed on 14 February 2025).
- Fang, A.M.; MacDonald, L.P.; Gregg, J.R.; Siddiqui, B.A.; Tang, C.; Chapin, B.F. Prostatectomy and other local treatments for oligometastatic prostate cancer: Recent and ongoing trials. Curr. Opin. Urol. 2025, 35, 171–177. [Google Scholar] [CrossRef]
- A Trial of Immunotherapy Strategies in Metastatic Hormone-sensitive Prostate Cancer. Available online: https://clinicaltrials.gov/study/NCT03879122?term=A%20Trial%20of%20Immunotherapy%20Strategies%20in%20Metastatic%20Hormone-sensitive%20Prostate%20Cancer.&rank=1 (accessed on 14 February 2025).
- Trujillo, B.; Wu, A.; Wetterskog, D.; Attard, G. Blood-based liquid biopsies for prostate cancer: Clinical opportunities and challenges. Br. J. Cancer 2022, 127, 1394–1402. [Google Scholar]
- Crocetto, F.; Russo, G.; Di Zazzo, E.; Pisapia, P.; Mirto, B.F.; Palmieri, A.; Pepe, F.; Bellevicine, C.; Russo, A.; La Civita, E.; et al. Liquid Biopsy in Prostate Cancer Management—Current Challenges and Future Perspectives. Cancers 2022, 14, 3272. [Google Scholar] [CrossRef]
- ProBio: A Biomarker Driven Study in Patients With Metastatic Prostate Cancer (ProBio). Available online: https://clinicaltrials.gov/study/NCT03903835?term=ProBio&rank=1 (accessed on 14 February 2025).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smani, S.; DuBois, J.; Ajjawi, I.; Sohoni, N.; Choksi, A.U.; Lokeshwar, S.D.; Kim, I.Y.; Renzulli, J.F., II. Advances in Current Treatment Paradigms for Metastatic Hormone-Sensitive Prostate Cancer. J. Clin. Med. 2025, 14, 2565. https://doi.org/10.3390/jcm14082565
Smani S, DuBois J, Ajjawi I, Sohoni N, Choksi AU, Lokeshwar SD, Kim IY, Renzulli JF II. Advances in Current Treatment Paradigms for Metastatic Hormone-Sensitive Prostate Cancer. Journal of Clinical Medicine. 2025; 14(8):2565. https://doi.org/10.3390/jcm14082565
Chicago/Turabian StyleSmani, Shayan, Julien DuBois, Ismail Ajjawi, Nishan Sohoni, Ankur U. Choksi, Soum D. Lokeshwar, Isaac Y. Kim, and Joseph F. Renzulli, II. 2025. "Advances in Current Treatment Paradigms for Metastatic Hormone-Sensitive Prostate Cancer" Journal of Clinical Medicine 14, no. 8: 2565. https://doi.org/10.3390/jcm14082565
APA StyleSmani, S., DuBois, J., Ajjawi, I., Sohoni, N., Choksi, A. U., Lokeshwar, S. D., Kim, I. Y., & Renzulli, J. F., II. (2025). Advances in Current Treatment Paradigms for Metastatic Hormone-Sensitive Prostate Cancer. Journal of Clinical Medicine, 14(8), 2565. https://doi.org/10.3390/jcm14082565