
Transthyretin Amyloid Cardiomyopathy: Current Diagnostic Approach and Risk Stratification with Multimodality Imaging

 , ,
, ,  ,
,  , ,
, ,
Abstract
1. Introduction
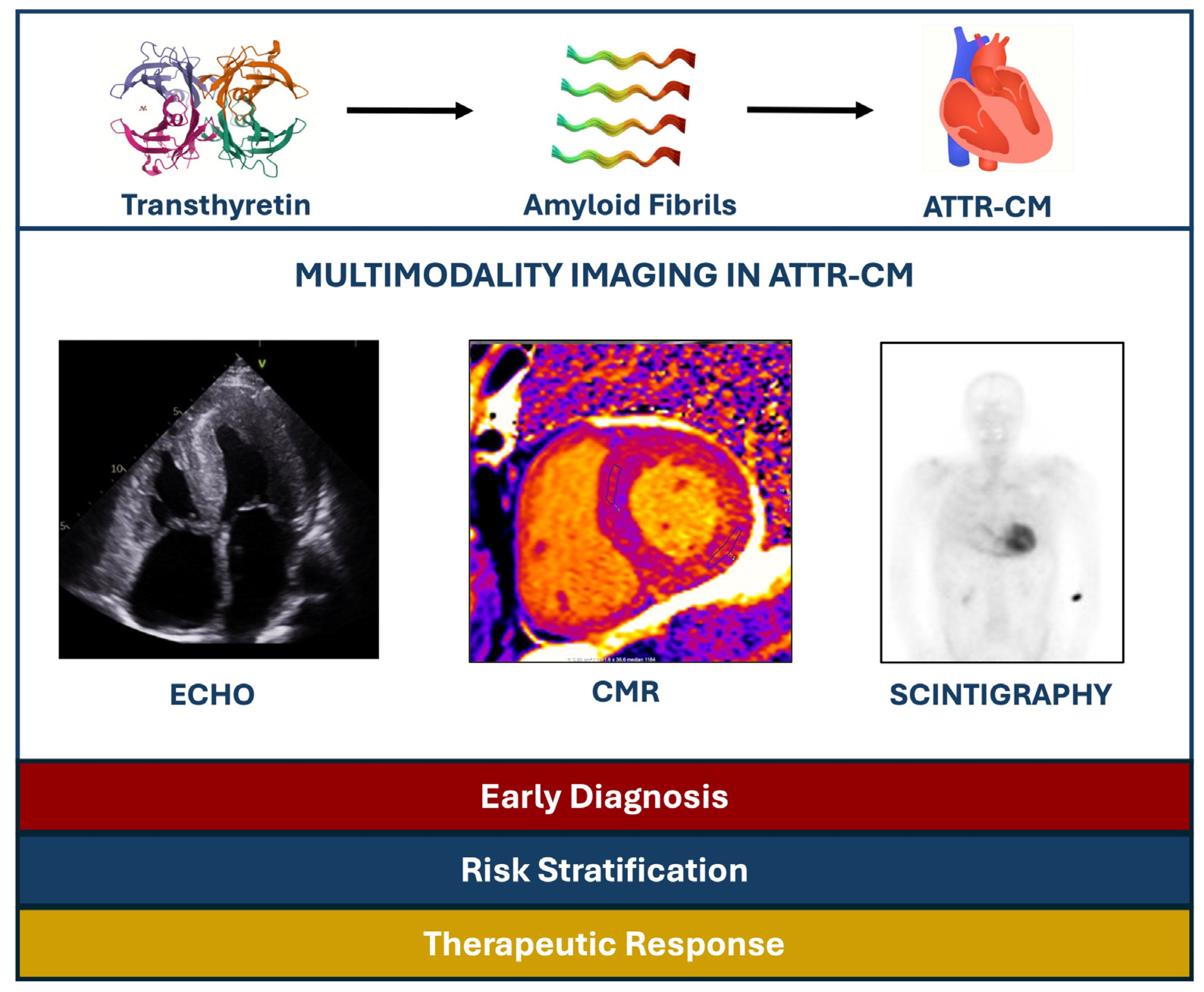
2. Pathophysiology of CA
- ATTRv is caused by autosomal dominant mutations in the transthyretin gene, located on chromosome 18, which encodes amyloidogenic variants with increased propensity to misfold.
3. Clinical Suspicion of ATTR-CM
- Unexplained HFpEF,
- ECG findings of low voltage despite left ventricular wall thickening,
- A ECG pseudo-infarction pattern, and
- Recurrent hospitalizations for HF despite optimized therapy [22].
- Autonomic or peripheral neuropathy;
- Carpal tunnel syndrome, especially if it is bilateral;
- Lumbar spine stenosis;
- Biceps tendon rupture.
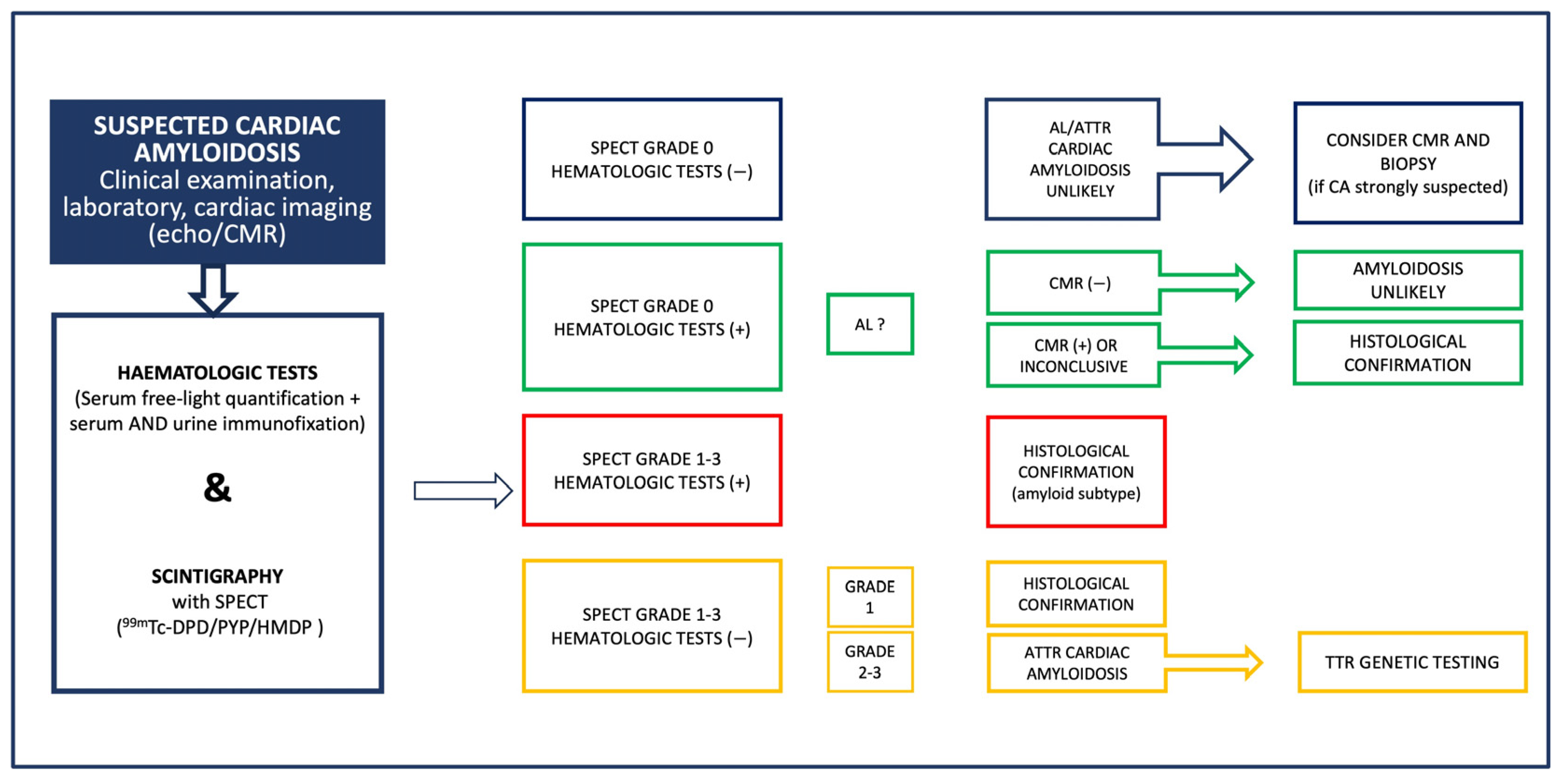
4. Diagnostic Algorithm of ATTR-CM
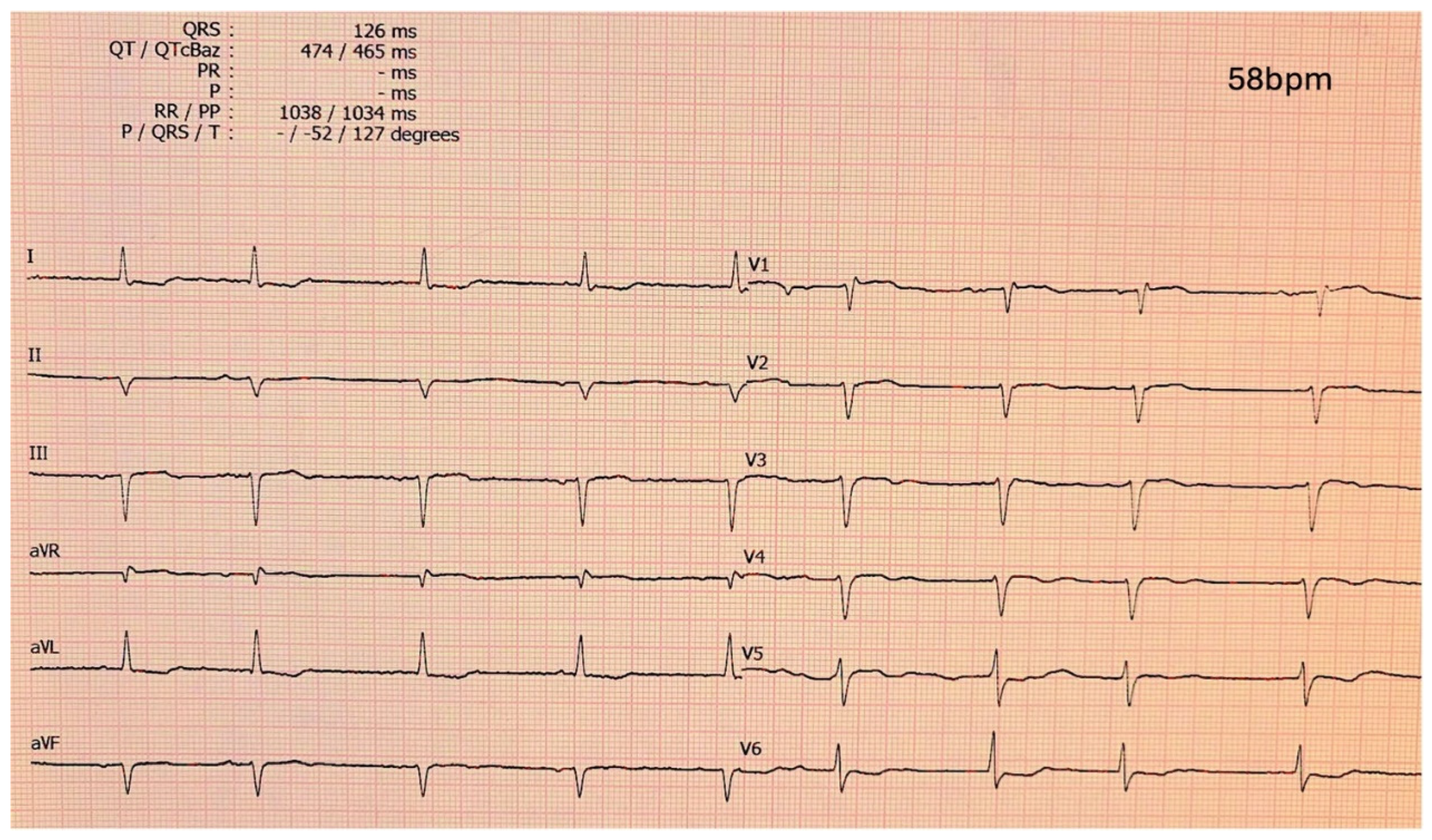
5. Electrocardiographic Features
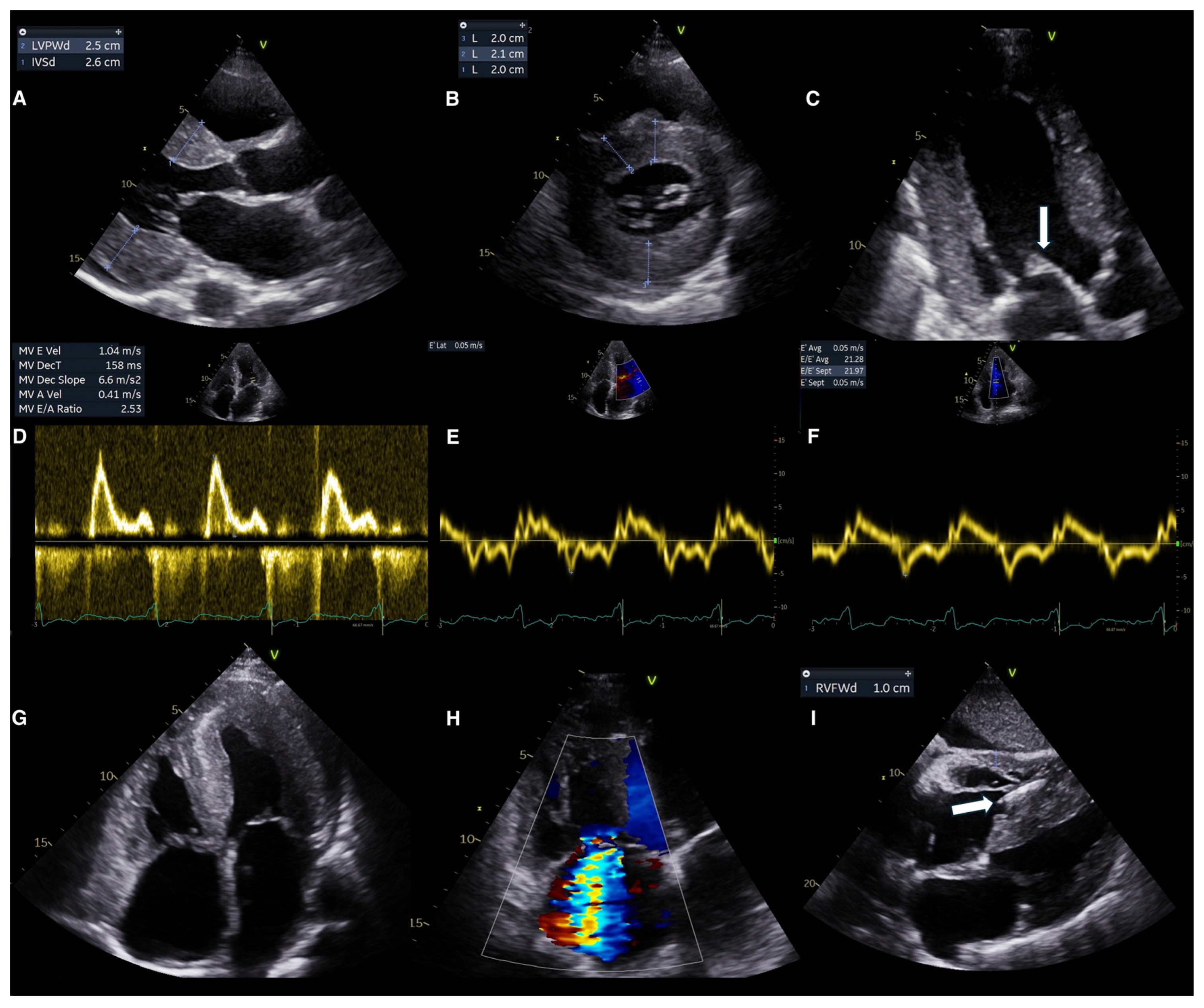
6. Echocardiography
6.1. Echocardiography for Diagnosis
Conventional Echocardiography
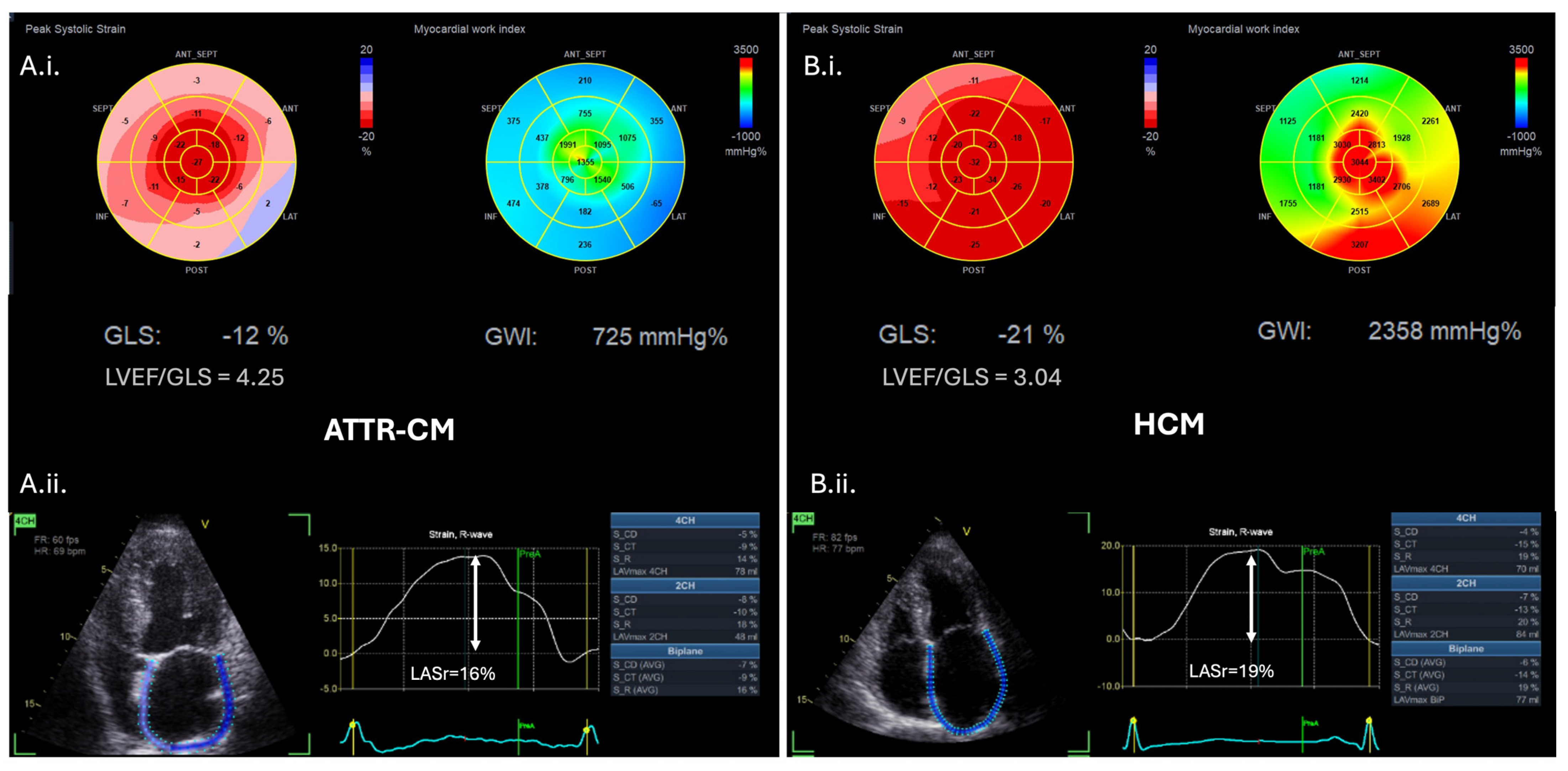
6.2. Advanced Echocardiography
6.3. Echocardiography for Prognosis
6.4. Echocardiography for Monitoring the Response to Treatment
7. Cardiac Magnetic Resonance
7.1. CMR for Diagnosis
7.2. CMR for Prognosis
7.3. CMR for Monitoring the Response to Treatment
8. Nuclear Medicine
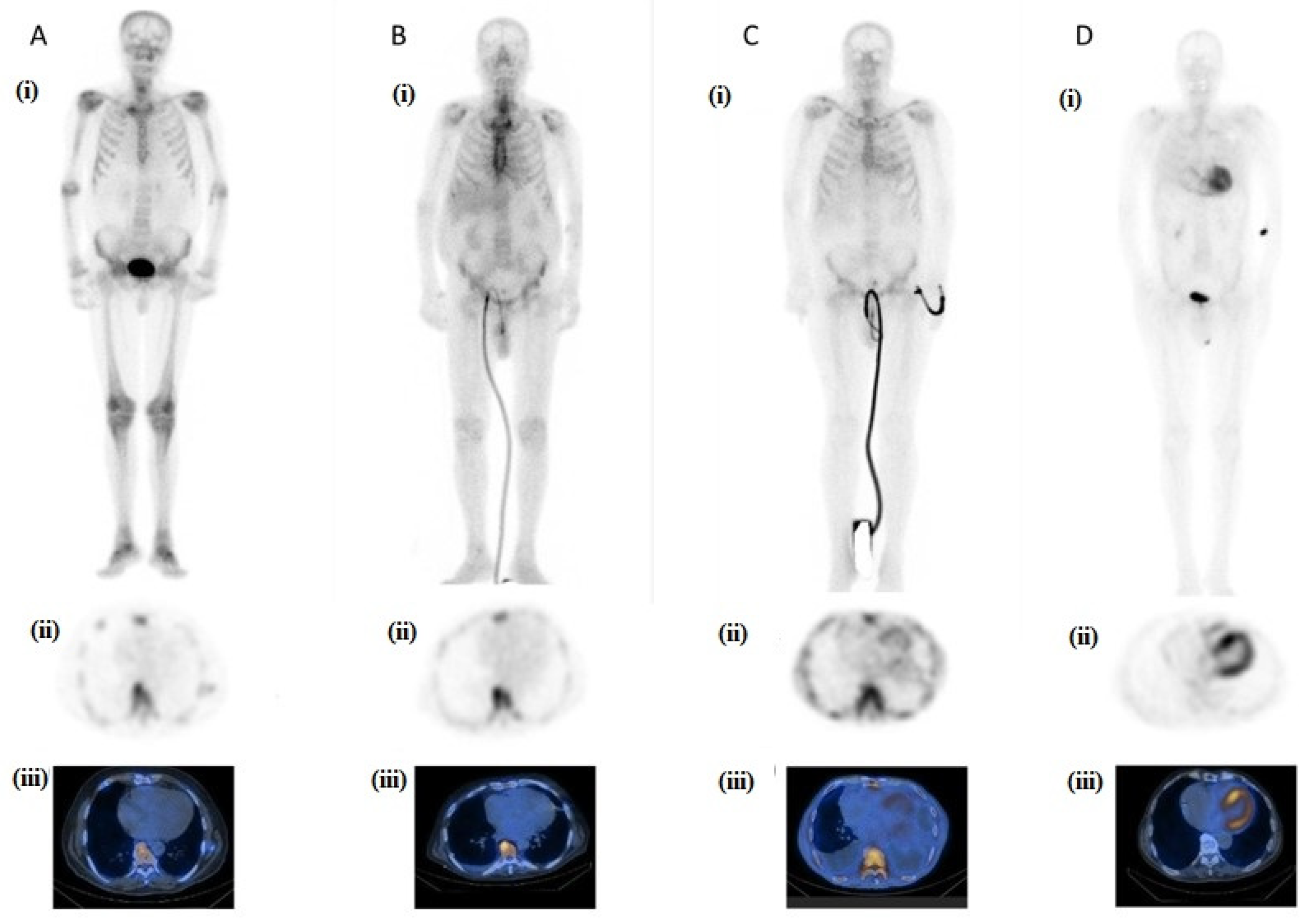
8.1. Nuclear Medicine for Diagnosis
8.2. Nuclear Medicine for Prognosis
8.3. Nuclear Medicine for Monitoring the Response to Treatment
9. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| AL | Light-chain amyloidosis |
| AL-CA | Light-chain cardiac amyloidosis |
| AS | Aortic stenosis |
| ATTR | Transthyretin amyloidosis |
| ATTR-CM | Transthyretin amyloid cardiomyopathy |
| ATTRv | Hereditary (variant) transthyretin amyloidosis |
| ATTRwt | Wild-type transthyretin amyloidosis |
| CA | Cardiac amyloidosis |
| CARI | Cardiac amyloidosis radionuclide imaging |
| CMR | Cardiac magnetic resonance |
| ECG | Electrocardiogram |
| ECV | Extracellular volume |
| GLS | Global longitudinal strain |
| GWI | Global myocardial work index |
| HCM | Hypertrophic cardiomyopathy |
| HF | Heart failure |
| HFpEF | Heart failure with preserved ejection fraction |
| H/CL | Heart to contralateral ratio |
| LA | Left atrium |
| LGE | Late gadolinium enhancement |
| LV | Left ventricle |
| LVEF | Left ventricular ejection fraction |
| LVH | Left ventricular hypertrophy |
| PET | Positron emission tomography |
| RV | Right ventricle |
| SPECT | Single-photon emission computed tomography |
| 99mTc-DPD | 99m Technetium 3,3-diphosphono-1,2-propanodicarboxylic acid |
| 99mTc-HMDP | 99m Technetium hydroxymethylene diphosphonate |
| 99mTc-PYP | 99m Technetium pyrophosphate |
References
- Wechalekar, A.D.; Gillmore, J.D.; Hawkins, P.N. Systemic Amyloidosis. Lancet 2016, 387, 2641–2654. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.P.; Damy, T.; Eriksson, U.; et al. Diagnosis and Treatment of Cardiac Amyloidosis: A Position Statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2021, 42, 1554–1568. [Google Scholar] [CrossRef] [PubMed]
- Gilstrap, L.G.; Dominici, F.; Wang, Y.; El-Sady, M.S.; Singh, A.; Di Carli, M.F.; Falk, R.H.; Dorbala, S. Epidemiology of Cardiac Amyloidosis–Associated Heart Failure Hospitalizations among Fee-for-Service Medicare Beneficiaries in the United States. Circ. Heart Fail. 2019, 12, e005407. [Google Scholar] [CrossRef] [PubMed]
- Buxbaum, J.N.; Dispenzieri, A.; Eisenberg, D.S.; Fändrich, M.; Merlini, G.; Saraiva, M.J.M.; Sekijima, Y.; Westermark, P. Amyloid Nomenclature 2022: Update, Novel Proteins, and Recommendations by the International Society of Amyloidosis (ISA) Nomenclature Committee. Amyloid 2022, 29, 213–219. [Google Scholar] [CrossRef]
- Ruberg, F.L.; Maurer, M.S. Cardiac Amyloidosis Due to Transthyretin Protein. JAMA 2024, 331, 778–791. [Google Scholar] [CrossRef]
- Gertz, M.A.; Dispenzieri, A.; Sher, T. Pathophysiology and Treatment of Cardiac Amyloidosis. Nat. Rev. Cardiol. 2014, 12, 91–102. [Google Scholar] [CrossRef]
- Gertz, M.A. Immunoglobulin Light Chain Amyloidosis: 2024 Update on Diagnosis, Prognosis, and Treatment. Am. J. Hematol. 2024, 99, 309–324. [Google Scholar] [CrossRef]
- Perfetti, V.; Palladini, G.; Casarini, S.; Navazza, V.; Rognoni, P.; Obici, L.; Invernizzi, R.; Perlini, S.; Klersy, C.; Merlini, G. The Repertoire of λ Light Chains Causing Predominant Amyloid Heart Involvement and Identification of a Preferentially Involved Germline Gene, IGLV1-44. Blood 2012, 119, 144–150. [Google Scholar] [CrossRef]
- Klabunde, T.; Petrassi, H.M.; Oza, V.B.; Raman, P.; Kelly, J.W.; Sacchettini, J.C. Rational Design of Potent Human Transthyretin Amyloid Disease Inhibitors. Nat. Struct. Biol. 2000, 7, 312–321. [Google Scholar] [CrossRef]
- Ruberg, F.L.; Grogan, M.; Hanna, M.; Kelly, J.W.; Maurer, M.S. Transthyretin Amyloid Cardiomyopathy: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 2872–2891. [Google Scholar] [CrossRef]
- Lauppe, R.; Liseth Hansen, J.; Fornwall, A.; Johansson, K.; Rozenbaum, M.H.; Strand, A.M.; Väkeväinen, M.; Kuusisto, J.; Gude, E.; Smith, J.G.; et al. Prevalence, Characteristics, and Mortality of Patients with Transthyretin Amyloid Cardiomyopathy in the Nordic Countries. ESC Heart Fail. 2022, 9, 2528–2537. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Naharro, A.; Hawkins, P.N.; Fontana, M. Cardiac Amyloidosis. Clin. Med. 2018, 18, s30. [Google Scholar] [CrossRef] [PubMed]
- Merlini, G.; Westermark, P. The Systemic Amyloidoses: Clearer Understanding of the Molecular Mechanisms Offers Hope for More Effective Therapies. J. Intern. Med. 2004, 255, 159–178. [Google Scholar] [CrossRef] [PubMed]
- Quarta, C.C.; Buxbaum, J.N.; Shah, A.M.; Falk, R.H.; Claggett, B.; Kitzman, D.W.; Mosley, T.H.; Butler, K.R.; Boerwinkle, E.; Solomon, S.D. The Amyloidogenic V122I Transthyretin Variant in Elderly Black Americans. N. Engl. J. Med. 2015, 372, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.S.; Hanna, M.; Grogan, M.; Dispenzieri, A.; Witteles, R.; Drachman, B.; Judge, D.P.; Lenihan, D.J.; Gottlieb, S.S.; Shah, S.J.; et al. Genotype and Phenotype of Transthyretin Cardiac Amyloidosis: THAOS (Transthyretin Amyloid Outcome Survey). J. Am. Coll. Cardiol. 2016, 68, 161–172. [Google Scholar] [CrossRef]
- Saito, Y.; Nakamura, K.; Ito, H. Molecular Mechanisms of Cardiac Amyloidosis. Int. J. Mol. Sci. 2022, 23, 25. [Google Scholar] [CrossRef]
- Laptseva, N.; Rossi, V.A.; Sudano, I.; Schwotzer, R.; Ruschitzka, F.; Flammer, A.J.; Duru, F. Arrhythmic Manifestations of Cardiac Amyloidosis: Challenges in Risk Stratification and Clinical Management. J. Clin. Med. 2023, 12, e005407. [Google Scholar] [CrossRef]
- Jung, M.H.; Chang, S.; Han, E.J.; Youn, J.C. Multimodal Imaging and Biomarkers in Cardiac Amyloidosis. Diagnostics 2022, 12, 627. [Google Scholar] [CrossRef]
- Maloberti, A.; Ciampi, C.; Politi, F.; Fabbri, S.; Musca, F.; Giannattasio, C. Cardiac Amyloidosis Red Flags: What All the Cardiologist Have to Know. Int. J. Cardiol. Cardiovasc. Risk Prev. 2024, 21, 200271. [Google Scholar] [CrossRef]
- Vergaro, G.; Aimo, A.; Barison, A.; Genovesi, D.; Buda, G.; Passino, C.; Emdin, M. Keys to Early Diagnosis of Cardiac Amyloidosis: Red Flags from Clinical, Laboratory and Imaging Findings. Eur. J. Prev. Cardiol. 2020, 27, 1806–1815. [Google Scholar] [CrossRef]
- aus dem Siepen, F.; Hansen, T. Diagnosing AL and ATTR Amyloid Cardiomyopathy: A Multidisciplinary Approach. J. Clin. Med. 2024, 13, 5873. [Google Scholar] [CrossRef]
- Merlo, M.; Porcari, A.; Pagura, L.; Cameli, M.; Vergaro, G.; Musumeci, B.; Biagini, E.; Canepa, M.; Crotti, L.; Imazio, M.; et al. A National Survey on Prevalence of Possible Echocardiographic Red Flags of Amyloid Cardiomyopathy in Consecutive Patients Undergoing Routine Echocardiography: Study Design and Patients Characterization—The First Insight from the AC-TIVE Study. Eur. J. Prev. Cardiol. 2022, 29, E173–E177. [Google Scholar] [CrossRef]
- aus dem Siepen, F.; Hein, S.; Prestel, S.; Baumgärtner, C.; Schönland, S.; Hegenbart, U.; Röcken, C.; Katus, H.A.; Kristen, A.V. Carpal Tunnel Syndrome and Spinal Canal Stenosis: Harbingers of Transthyretin Amyloid Cardiomyopathy? Clin. Res. Cardiol. 2019, 108, 1324–1330. [Google Scholar] [CrossRef]
- Tang, C.X.; Petersen, S.E.; Sanghvi, M.M.; Lu, G.M.; Zhang, L.J. Cardiovascular Magnetic Resonance Imaging for Amyloidosis: The State-of-the-Art. Trends Cardiovasc. Med. 2019, 29, 83–94. [Google Scholar] [CrossRef]
- Rauf, M.U.; Hawkins, P.N.; Cappelli, F.; Perfetto, F.; Zampieri, M.; Argiro, A.; Petrie, A.; Law, S.; Porcari, A.; Razvi, Y.; et al. Tc-99m Labelled Bone Scintigraphy in Suspected Cardiac Amyloidosis. Eur. Heart J. 2023, 44, 2187–2198. [Google Scholar] [CrossRef]
- Arno, S.; Cowger, J. The Genetics of Cardiac Amyloidosis. Heart Fail. Rev. 2022, 27, 1485–1492. [Google Scholar] [CrossRef]
- Arbelo, E.; Protonotarios, A.; Gimeno, J.R.; Arbustini, E.; Barriales-Villa, R.; Basso, C.; Bezzina, C.R.; Biagini, E.; Blom, N.A.; De Boer, R.A.; et al. 2023 ESC Guidelines for the Management of Cardiomyopathies. Eur. Heart J. 2023, 44, 3503–3626. [Google Scholar] [CrossRef]
- Martini, N.; Sinigiani, G.; De Michieli, L.; Mussinelli, R.; Perazzolo Marra, M.; Iliceto, S.; Zorzi, A.; Perlini, S.; Corrado, D.; Cipriani, A. Electrocardiographic Features and Rhythm Disorders in Cardiac Amyloidosis. Trends Cardiovasc. Med. 2024, 34, 257–264. [Google Scholar] [CrossRef]
- Cipriani, A.; De Michieli, L.; Porcari, A.; Licchelli, L.; Sinigiani, G.; Tini, G.; Zampieri, M.; Sessarego, E.; Argirò, A.; Fumagalli, C.; et al. Low QRS Voltages in Cardiac Amyloidosis: Clinical Correlates and Prognostic Value. JACC CardioOncol. 2022, 4, 458–470. [Google Scholar] [CrossRef]
- Teresi, L.; Trimarchi, G.; Liotta, P.; Restelli, D.; Licordari, R.; Carciotto, G.; Francesco, C.; Crea, P.; Dattilo, G.; Micari, A.; et al. Electrocardiographic Patterns and Arrhythmias in Cardiac Amyloidosis: From Diagnosis to Therapeutic Management-A Narrative Review. J. Clin. Med. 2024, 13, 5588. [Google Scholar] [CrossRef]
- Cuddy, S.A.M.; Chetrit, M.; Jankowski, M.; Desai, M.; Falk, R.H.; Weiner, R.B.; Klein, A.L.; Phelan, D.; Grogan, M. Practical Points for Echocardiography in Cardiac Amyloidosis. J. Am. Soc. Echocardiogr. 2022, 35, A31–A40. [Google Scholar] [CrossRef]
- Polo, J.M.; Barrenechea, A.R.U.; Martí, P.R.; Palacios, R.P.; Gutiérrez, A.G.; Juana, E.B.; Gracia, A.A.; Ayala, S.A.; Arregui, M.Á.A. Echocardiographic Markers of Cardiac Amyloidosis in Patients with Heart Failure and Left Ventricular Hypertrophy. Cardiol. J. 2023, 30, 266–275. [Google Scholar] [CrossRef]
- Lee, G.Y.; Kim, K.; Choi, J.O.; Kim, S.J.; Kim, J.S.; Choe, Y.H.; Grogan, M.A.; Jeon, E.S. Cardiac Amyloidosis without Increased Left Ventricular Wall Thickness. Mayo Clin. Proc. 2014, 89, 781–789. [Google Scholar] [CrossRef]
- Scheel, P.J.; Mukherjee, M.; Hays, A.G.; Vaishnav, J. Multimodality Imaging in the Evaluation and Prognostication of Cardiac Amyloidosis. Front. Cardiovasc. Med. 2022, 9, 787618. [Google Scholar] [CrossRef]
- Korosoglou, G.; Giusca, S.; André, F.; Siepen, F.A.D.; Nunninger, P.; Kristen, A.V.; Frey, N. Diagnostic Work-Up of Cardiac Amyloidosis Using Cardiovascular Imaging: Current Standards and Practical Algorithms. Vasc. Health Risk Manag. 2021, 17, 661–673. [Google Scholar] [CrossRef]
- Martinez-Naharro, A.; Baksi, A.J.; Hawkins, P.N.; Fontana, M. Diagnostic Imaging of Cardiac Amyloidosis. Nat. Rev. Cardiol. 2020, 17, 413–426. [Google Scholar] [CrossRef]
- Razvi, Y.; Patel, R.K.; Fontana, M.; Gillmore, J.D. Cardiac Amyloidosis: A Review of Current Imaging Techniques. Front. Cardiovasc. Med. 2021, 8, 751293. [Google Scholar] [CrossRef]
- Rigopoulos, A.G.; Ali, M.; Abate, E.; Torky, A.R.; Matiakis, M.; Mammadov, M.; Melnyk, H.; Vogt, A.; de Vecchis, R.; Bigalke, B.; et al. Advances in the Diagnosis and Treatment of Transthyretin Amyloidosis with Cardiac Involvement. Heart Fail. Rev. 2019, 24, 521–533. [Google Scholar] [CrossRef]
- Jurcuţ, R.; Onciul, S.; Adam, R.; Stan, C.; Coriu, D.; Rapezzi, C.; Popescu, B.A. Multimodality Imaging in Cardiac Amyloidosis: A Primer for Cardiologists. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 833–844. [Google Scholar] [CrossRef]
- Rimbas, R.C.; Balinisteanu, A.; Magda, S.L.; Visoiu, S.I.; Ciobanu, A.O.; Beganu, E.; Nicula, A.I.; Vinereanu, D. New Advanced Imaging Parameters and Biomarkers-A Step Forward in the Diagnosis and Prognosis of TTR Cardiomyopathy. J. Clin. Med. 2022, 11, 2360. [Google Scholar] [CrossRef]
- Liang, S.; Liu, Z.; Li, Q.; He, W.; Huang, H. Advance of Echocardiography in Cardiac Amyloidosis. Heart Fail. Rev 2023, 28, 1345–1356. [Google Scholar] [CrossRef]
- Galat, A.; Guellich, A.; Bodez, D.; Slama, M.; Dijos, M.; Zeitoun, D.M.; Milleron, O.; Attias, D.; Dubois-Randé, J.L.; Mohty, D.; et al. Aortic Stenosis and Transthyretin Cardiac Amyloidosis: The Chicken or the Egg? Eur. Heart J. 2016, 37, 3525–3531. [Google Scholar] [CrossRef]
- Giblin, G.T.; Cuddy, S.A.M. Multimodality Imaging in Cardiac Amyloidosis. Curr. Cardiol. Rep. 2021, 23, 833–844. [Google Scholar] [CrossRef]
- Russo, D.; Musumeci, M.B.; Volpe, M. The Neglected Issue of Cardiac Amyloidosis in Trials on Heart Failure with Preserved Ejection Fraction in the Elderly. Eur. J. Heart Fail. 2020, 22, 1740–1741. [Google Scholar] [CrossRef]
- González-López, E.; Gagliardi, C.; Dominguez, F.; Quarta, C.C.; De Haro-Del Moral, F.J.; Milandri, A.; Salas, C.; Cinelli, M.; Cobo-Marcos, M.; Lorenzini, M.; et al. Clinical Characteristics of Wild-Type Transthyretin Cardiac Amyloidosis: Disproving Myths. Eur. Heart J. 2017, 38, 1895–1904. [Google Scholar] [CrossRef]
- Licordari, R.; Minutoli, F.; Recupero, A.; Campisi, M.; Donato, R.; Mazzeo, A.; Dattilo, G.; Baldari, S.; Vita, G.; Zito, C.; et al. Early Impairment of Right Ventricular Morphology and Function in Transthyretin-Related Cardiac Amyloidosis. J. Cardiovasc. Echogr. 2021, 31, 17–22. [Google Scholar] [CrossRef]
- Bodez, D.; Ternacle, J.; Guellich, A.; Galat, A.; Lim, P.; Radu, C.; Guendouz, S.; Bergoend, E.; Couetil, J.P.; Hittinger, L.; et al. Prognostic Value of Right Ventricular Systolic Function in Cardiac Amyloidosis. Amyloid 2016, 23, 158–167. [Google Scholar] [CrossRef]
- Bellavia, D.; Pellikka, P.A.; Dispenzieri, A.; Scott, C.G.; Al-Zahrani, G.B.; Grogan, M.; Pitrolo, F.; Oh, J.K.; Miller, F.A. Comparison of Right Ventricular Longitudinal Strain Imaging, Tricuspid Annular Plane Systolic Excursion, and Cardiac Biomarkers for Early Diagnosis of Cardiac Involvement and Risk Stratification in Primary Systematic (AL) Amyloidosis: A 5-Year Cohort Study. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 680–689. [Google Scholar] [CrossRef]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.W.J.M.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI Expert Consensus Recommendations for Multimodality Imaging in Cardiac Amyloidosis: Part 2 of 2—Diagnostic Criteria and Appropriate Utilization. J. Card Fail. 2019, 25, 854–865. [Google Scholar] [CrossRef]
- Dorbala, S.; Cuddy, S.; Falk, R.H. How to Image Cardiac Amyloidosis: A Practical Approach. JACC Cardiovasc. Imaging 2020, 13, 1368–1383. [Google Scholar] [CrossRef]
- Rapezzi, C.; Aimo, A.; Barison, A.; Emdin, M.; Porcari, A.; Linhart, A.; Keren, A.; Merlo, M.; Sinagra, G. Restrictive Cardiomyopathy: Definition and Diagnosis. Eur. Heart J. 2022, 43, 4679–4693. [Google Scholar] [CrossRef]
- Habib, G.; Bucciarelli-Ducci, C.; Caforio, A.L.P.; Cardim, N.; Charron, P.; Cosyns, B.; Dehaene, A.; Derumeaux, G.; Donal, E.; Dweck, M.R.; et al. Multimodality Imaging in Restrictive Cardiomyopathies: An EACVI Expert Consensus Document in Collaboration with the “Working Group on Myocardial and Pericardial Diseases” of the European Society of Cardiology Endorsed by the Indian Academy of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1090–1091. [Google Scholar] [CrossRef]
- Bashir, Z.; Musharraf, M.; Azam, R.; Bukhari, S. Imaging Modalities in Cardiac Amyloidosis. Curr. Probl. Cardiol. 2024, 49, 102858. [Google Scholar] [CrossRef]
- Kyrouac, D.; Schiffer, W.; Lennep, B.; Fergestrom, N.; Zhang, K.W.; Gorcsan, J.; Lenihan, D.J.; Mitchell, J.D. Echocardiographic and Clinical Predictors of Cardiac Amyloidosis: Limitations of Apical Sparing. ESC Heart Fail. 2022, 9, 385–397. [Google Scholar] [CrossRef]
- Pagourelias, E.D.; Mirea, O.; Duchenne, J.; Van Cleemput, J.; Delforge, M.; Bogaert, J.; Kuznetsova, T.; Voigt, J.U. Echo Parameters for Differential Diagnosis in Cardiac Amyloidosis: A Head-to-Head Comparison of Deformation and Nondeformation Parameters. Circ. Cardiovasc. Imaging 2017, 10, e005588. [Google Scholar] [CrossRef]
- Liu, D.; Hu, K.; Niemann, M.; Herrmann, S.; Cikes, M.; Störk, S.; Gaudron, P.D.; Knop, S.; Ertl, G.; Bijnens, B.; et al. Effect of Combined Systolic and Diastolic Functional Parameter Assessment for Differentiation of Cardiac Amyloidosis from Other Causes of Concentric Left Ventricular Hypertrophy. Circ. Cardiovasc. Imaging 2013, 6, 1066–1072. [Google Scholar] [CrossRef]
- Moñivas Palomero, V.; Durante-Lopez, A.; Sanabria, M.T.; Cubero, J.S.; González-Mirelis, J.; Lopez-Ibor, J.V.; Navarro Rico, S.M.; Krsnik, I.; Dominguez, F.; Mingo, A.M.; et al. Role of Right Ventricular Strain Measured by Two-Dimensional Echocardiography in the Diagnosis of Cardiac Amyloidosis. J. Am. Soc. Echocardiogr. 2019, 32, 845–853.e1. [Google Scholar] [CrossRef]
- Timóteo, A.T.; Rosa, S.A.; Brás, P.G.; Ferreira, M.J.V.; Bettencourt, N. Multimodality Imaging in Cardiac Amyloidosis: State-of-the-Art Review. J. Clin. Ultrasound. 2022, 50, 1084–1096. [Google Scholar] [CrossRef]
- Agrawal, T.; Nagueh, S.F. Echocardiographic Assessment of Cardiac Amyloidosis. Heart Fail. Rev. 2022, 27, 1505–1513. [Google Scholar] [CrossRef]
- Monte, I.P.; Faro, D.C.; Trimarchi, G.; de Gaetano, F.; Campisi, M.; Losi, V.; Teresi, L.; Di Bella, G.; Tamburino, C.; de Gregorio, C. Left Atrial Strain Imaging by Speckle Tracking Echocardiography: The Supportive Diagnostic Value in Cardiac Amyloidosis and Hypertrophic Cardiomyopathy. J. Cardiovasc. Dev. Dis. 2023, 10, 261. [Google Scholar] [CrossRef]
- Nochioka, K.; Quarta, C.C.; Claggett, B.; Roca, G.Q.; Rapezzi, C.; Falk, R.H.; Solomon, S.D. Left Atrial Structure and Function in Cardiac Amyloidosis. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1128–1137. [Google Scholar] [CrossRef]
- Ferkh, A.; Geenty, P.; Stefani, L.; Emerson, P.; Pham, J.; Byth, K.; Boyd, A.C.; Richards, D.; Taylor, M.S.; Kwok, F.; et al. Diagnostic and Prognostic Value of the Left Atrial Myopathy Evaluation in Cardiac Amyloidosis Using Echocardiography. ESC Heart Fail. 2024, 11, 4139–4147. [Google Scholar] [CrossRef]
- Marzlin, N.; Hays, A.G.; Peters, M.; Kaminski, A.; Roemer, S.; O’Leary, P.; Kroboth, S.; Harland, D.R.; Khandheria, B.K.; Tajik, A.J.; et al. Myocardial Work in Echocardiography. Circ. Cardiovasc. Imaging 2023, 16, E014419. [Google Scholar] [CrossRef]
- Trimarchi, G.; Carerj, S.; Di Bella, G.; Manganaro, R.; Pizzino, F.; Restelli, D.; Pelaggi, G.; Lofrumento, F.; Licordari, R.; Taverna, G.; et al. Clinical Applications of Myocardial Work in Echocardiography: A Comprehensive Review. J. Cardiovasc. Echogr. 2024, 34, 99–113. [Google Scholar] [CrossRef]
- de Gregorio, C.; Trimarchi, G.; Faro, D.C.; De Gaetano, F.; Campisi, M.; Losi, V.; Zito, C.; Tamburino, C.; Di Bella, G.; Monte, I.P. Myocardial Work Appraisal in Transthyretin Cardiac Amyloidosis and Nonobstructive Hypertrophic Cardiomyopathy. Am. J. Cardiol. 2023, 208, 173–179. [Google Scholar] [CrossRef]
- de Gregorio, C.; Trimarchi, G.; Faro, D.C.; Poleggi, C.; Teresi, L.; De Gaetano, F.; Zito, C.; Lofrumento, F.; Koniari, I.; Licordari, R.; et al. Systemic Vascular Resistance and Myocardial Work Analysis in Hypertrophic Cardiomyopathy and Transthyretin Cardiac Amyloidosis with Preserved Left Ventricular Ejection Fraction. J. Clin. Med. 2024, 13, 1671. [Google Scholar] [CrossRef]
- Palmiero, G.; Rubino, M.; Monda, E.; Caiazza, M.; D’urso, L.; Carlomagno, G.; Verrillo, F.; Ascione, R.; Manganelli, F.; Cerciello, G.; et al. Global Left Ventricular Myocardial Work Efficiency in Heart Failure Patients with Cardiac Amyloidosis: Pathophysiological Implications and Role in Differential Diagnosis. J. Cardiovasc. Echogr. 2021, 31, 157–164. [Google Scholar] [CrossRef]
- Ladefoged, B.; Pedersen, A.L.D.; Clemmensen, T.S.; Poulsen, S.H. Strain-Derived Myocardial Work in Wild-Type Transthyretin Cardiac Amyloidosis with Aortic Stenosis-Diagnosis and Prognosis. Echocardiography 2023, 40, 1079–1087. [Google Scholar] [CrossRef]
- Klein, A.; Hatle, L.; Taliercio, C.; Jae, O.; Kyle, R.; Gertz, M.; Bailey, K.; Seward, J.; Tajik, J. Prognostic Significance of Doppler Measures of Diastolic Function in Cardiac Amyloidosis. A Doppler Echocardiography Study. Circulation 1991, 83, 808–816. [Google Scholar] [CrossRef]
- Tana, M.; Tana, C.; Palmiero, G.; Mantini, C.; Coppola, M.G.; Limongelli, G.; Schiavone, C.; Porreca, E. Imaging Findings of Right Cardiac Amyloidosis: Impact on Prognosis and Clinical Course. J. Ultrasound 2023, 26, 605–614. [Google Scholar] [CrossRef]
- Patel, A.R.; Dubrey, S.W.; Mendes, L.A.; Skinner, M.; Cupples, A.; Falk, R.H.; Davidoff, R. Right Ventricular Dilation in Primary Amyloidosis: An Independent Predictor of Survival. Am. J. Cardiol. 1997, 80, 486–492. [Google Scholar] [CrossRef]
- Damy, T.; Jaccard, A.; Guellich, A.; Lavergne, D.; Galat, A.; Deux, J.F.; Hittinger, L.; Dupuis, J.; Frenkel, V.; Rigaud, C.; et al. Identification of Prognostic Markers in Transthyretin and AL Cardiac Amyloidosis. Amyloid 2016, 23, 194–202. [Google Scholar] [CrossRef]
- Chacko, L.; Karia, N.; Venneri, L.; Bandera, F.; Passo, B.D.; Buonamici, L.; Lazari, J.; Ioannou, A.; Porcari, A.; Patel, R.; et al. Progression of Echocardiographic Parameters and Prognosis in Transthyretin Cardiac Amyloidosis. Eur. J. Heart Fail. 2022, 24, 1700–1712. [Google Scholar] [CrossRef]
- Tanaka, H. Efficacy of Echocardiography for Differential Diagnosis of Left Ventricular Hypertrophy: Special Focus on Speckle-Tracking Longitudinal Strain. J. Echocardiogr. 2021, 19, 71–79. [Google Scholar] [CrossRef]
- Ternacle, J.; Bodez, D.; Guellich, A.; Audureau, E.; Rappeneau, S.; Lim, P.; Radu, C.; Guendouz, S.; Couetil, J.P.; Benhaiem, N.; et al. Causes and Consequences of Longitudinal LV Dysfunction Assessed by 2D Strain Echocardiography in Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2016, 9, 126–138. [Google Scholar] [CrossRef]
- Fine, N.M.; White, J.A.; Jimenez-Zepeda, V.; Howlett, J.G. Determinants and Prognostic Significance of Serial Right Heart Function Changes in Patients with Cardiac Amyloidosis. Can. J. Cardiol. 2020, 36, 432–440. [Google Scholar] [CrossRef]
- Tjahjadi, C.; Fortuni, F.; Stassen, J.; Debonnaire, P.; Lustosa, R.P.; Marsan, N.A.; Delgado, V.; Bax, J.J. Prognostic Implications of Right Ventricular Systolic Dysfunction in Cardiac Amyloidosis. Am. J. Cardiol. 2022, 173, 120–127. [Google Scholar] [CrossRef]
- Huntjens, P.R.; Zhang, K.W.; Soyama, Y.; Karmpalioti, M.; Lenihan, D.J.; Gorcsan, J. Prognostic Utility of Echocardiographic Atrial and Ventricular Strain Imaging in Patients with Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2021, 14, 1508–1519. [Google Scholar] [CrossRef]
- Antonelli, J.; Neveu, A.; Kosmala, W.; L’Official, G.; Curtis, E.; Oger, E.; Donal, E. Evolution and Prognostic Value of Left Ventricular Deformation and Myocardial Work Parameters in Transthyretin Amyloid Cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2024, 25, 469–479. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Baumbach, A.; Böhm, M.; Burri, H.; Čelutkiene, J.; Chioncel, O.; Cleland, J.G.F.; Coats, A.J.S.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Maurer, M.S.; Schwartz, J.H.; Gundapaneni, B.; Elliott, P.M.; Merlini, G.; Waddington-Cruz, M.; Kristen, A.V.; Grogan, M.; Witteles, R.; Damy, T.; et al. Tafamidis Treatment for Patients with Transthyretin Amyloid Cardiomyopathy. N. Engl. J. Med. 2018, 379, 1007–1016. [Google Scholar] [CrossRef]
- Pugliatti, P.; Trimarchi, G.; Barocelli, F.; Pizzino, F.; Di Spigno, F.; Tedeschi, A.; Piccione, M.C.; Irrera, P.; Aschieri, D.; Niccoli, G.; et al. Advancing Cardiac Amyloidosis Care Through Insights from Cardiopulmonary Exercise Testing. J. Clin. Med. 2024, 13, 7285. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Bengel, F.; Brito, D.; Damy, T.; Duca, F.; Dorbala, S.; Nativi-Nicolau, J.; Obici, L.; Rapezzi, C.; Sekijima, Y.; et al. Expert Consensus on the Monitoring of Transthyretin Amyloid Cardiomyopathy. Eur. J. Heart Fail. 2021, 23, 895–905. [Google Scholar] [CrossRef]
- Shah, S.J.; Fine, N.; Garcia-Pavia, P.; Klein, A.L.; Fernandes, F.; Weissman, N.J.; Maurer, M.S.; Boman, K.; Gundapaneni, B.; Sultan, M.B.; et al. Effect of Tafamidis on Cardiac Function in Patients with Transthyretin Amyloid Cardiomyopathy: A Post Hoc Analysis of the ATTR-ACT Randomized Clinical Trial. JAMA Cardiol. 2024, 9, 25–34. [Google Scholar] [CrossRef]
- Ichikawa, Y.; Oota, E.; Odajima, S.; Kintsu, M.; Todo, S.; Takeuchi, K.; Yamauchi, Y.; Shiraki, H.; Yamashita, K.; Fukuda, T.; et al. Impact of Tafamidis on Echocardiographic Cardiac Function of Patients with Transthyretin Cardiac Amyloidosis. Circ. J. 2023, 87, 508–516. [Google Scholar] [CrossRef]
- Giblin, G.T.; Cuddy, S.A.M.; González-López, E.; Sewell, A.; Murphy, A.; Dorbala, S.; Falk, R.H. Effect of Tafamidis on Global Longitudinal Strain and Myocardial Work in Transthyretin Cardiac Amyloidosis. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 1029–1039. [Google Scholar] [CrossRef]
- Rettl, R.; Duca, F.; Binder, C.; Dachs, T.M.; Cherouny, B.; Camuz Ligios, L.; Mann, C.; Schrutka, L.; Dalos, D.; Charwat-Resl, S.; et al. Impact of Tafamidis on Myocardial Strain in Transthyretin Amyloid Cardiomyopathy. Amyloid 2023, 30, 127–137. [Google Scholar] [CrossRef]
- Kao, T.W.; Hung, Y.H.; Yu, A.L.; Cheng, M.F.; Su, M.Y.; Chao, C.C.; Tsai, C.H.; Lin, Y.H. Effect of Tafamidis on Clinical and Functional Parameters in Transthyretin Amyloid Cardiomyopathy. JACC Adv. 2025, 4, 101511. [Google Scholar] [CrossRef]
- Burrage, M.K.; Ferreira, V.M. Cardiovascular Magnetic Resonance for the Differentiation of Left Ventricular Hypertrophy. Curr. Heart Fail. Rep. 2020, 17, 192–204. [Google Scholar] [CrossRef]
- Licordari, R.; Trimarchi, G.; Teresi, L.; Restelli, D.; Lofrumento, F.; Perna, A.; Campisi, M.; de Gregorio, C.; Grimaldi, P.; Calabrò, D.; et al. Cardiac Magnetic Resonance in HCM Phenocopies: From Diagnosis to Risk Stratification and Therapeutic Management. J. Clin. Med. 2023, 12, 3481. [Google Scholar] [CrossRef]
- Maceira, A.M.; Joshi, J.; Prasad, S.K.; Moon, J.C.; Perugini, E.; Harding, I.; Sheppard, M.N.; Poole-Wilson, P.A.; Hawkins, P.N.; Pennell, D.J. Cardiovascular Magnetic Resonance in Cardiac Amyloidosis. Circulation 2005, 111, 186–193. [Google Scholar] [CrossRef]
- Syed, I.S.; Glockner, J.F.; Feng, D.L.; Araoz, P.A.; Martinez, M.W.; Edwards, W.D.; Gertz, M.A.; Dispenzieri, A.; Oh, J.K.; Bellavia, D.; et al. Role of Cardiac Magnetic Resonance Imaging in the Detection of Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2010, 3, 155–164. [Google Scholar] [CrossRef]
- Zhao, L.; Tian, Z.; Fang, Q. Diagnostic Accuracy of Cardiovascular Magnetic Resonance for Patients with Suspected Cardiac Amyloidosis: A Systematic Review and Meta-Analysis. BMC Cardiovasc. Disord. 2016, 16, 129. [Google Scholar] [CrossRef]
- Taylor, R.S.; Walker, S.; Ciani, O.; Warren, F.; Smart, N.A.; Piepoli, M.; Davos, C.H. Exercise-Based Cardiac Rehabilitation for Chronic Heart Failure: The EXTRAMATCH II Individual Participant Data Meta-Analysis. Health Technol Assess 2019, 23, 1–97. [Google Scholar] [CrossRef]
- Karamitsos, T.D.; Piechnik, S.K.; Banypersad, S.M.; Fontana, M.; Ntusi, N.B.; Ferreira, V.M.; Whelan, C.J.; Myerson, S.G.; Robson, M.D.; Hawkins, P.N.; et al. Noncontrast T1 Mapping for the Diagnosis of Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2013, 6, 488–497. [Google Scholar] [CrossRef]
- Baggiano, A.; Boldrini, M.; Martinez-Naharro, A.; Kotecha, T.; Petrie, A.; Rezk, T.; Gritti, M.; Quarta, C.; Knight, D.S.; Wechalekar, A.D.; et al. Noncontrast Magnetic Resonance for the Diagnosis of Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2020, 13, 69–80. [Google Scholar] [CrossRef]
- Brooks, J.; Kramer, C.M.; Salerno, M. Markedly Increased Volume of Distribution of Gadolinium in Cardiac Amyloidosis Demonstrated by T1 Mapping. J. Magn. Reason. Imaging 2013, 38, 1591–1595. [Google Scholar] [CrossRef]
- Martinez-Naharro, A.; Kotecha, T.; Norrington, K.; Boldrini, M.; Rezk, T.; Quarta, C.; Treibel, T.A.; Whelan, C.J.; Knight, D.S.; Kellman, P.; et al. Native T1 and Extracellular Volume in Transthyretin Amyloidosis. JACC Cardiovasc. Imaging 2019, 12, 810–819. [Google Scholar] [CrossRef]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.W.J.M.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI Expert Consensus Recommendations for Multimodality Imaging in Cardiac Amyloidosis: Part 1 of 2-Evidence Base and Standardized Methods of Imaging. J. Nucl. Cardiol. 2019, 26, 2065–2123. [Google Scholar] [CrossRef]
- Pan, J.A.; Kerwin, M.J.; Salerno, M. Native T1 Mapping, Extracellular Volume Mapping, and Late Gadolinium Enhancement in Cardiac Amyloidosis: A Meta-Analysis. JACC Cardiovasc. Imaging 2020, 13, 1299–1310. [Google Scholar] [CrossRef]
- Martinez-Naharro, A.; Abdel-Gadir, A.; Treibel, T.A.; Zumbo, G.; Knight, D.S.; Rosmini, S.; Lane, T.; Mahmood, S.; Sachchithanantham, S.; Whelan, C.J.; et al. CMR-Verified Regression of Cardiac AL Amyloid After Chemotherapy. JACC Cardiovasc. Imaging 2018, 11, 152–154. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M.; Pica, S.; Reant, P.; Abdel-Gadir, A.; Treibel, T.A.; Banypersad, S.M.; Maestrini, V.; Barcella, W.; Rosmini, S.; Bulluck, H.; et al. Prognostic Value of Late Gadolinium Enhancement Cardiovascular Magnetic Resonance in Cardiac Amyloidosis. Circulation 2015, 132, 1570–1579. [Google Scholar] [CrossRef] [PubMed]
- Dungu, J.N.; Valencia, O.; Pinney, J.H.; Gibbs, S.D.J.; Rowczenio, D.; Gilbertson, J.A.; Lachmann, H.J.; Wechalekar, A.; Gillmore, J.D.; Whelan, C.J.; et al. CMR-Based Differentiation of AL and ATTR Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2014, 7, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Azuma, M.; Horita, N.; Utsunomiya, D. Monitoring the Efficacy of Tafamidis in ATTR Cardiac Amyloidosis by MRI-ECV: A Systematic Review and Meta-Analysis. Tomography 2024, 10, 1303–1311. [Google Scholar] [CrossRef]
- Gillmore, J.D.; Maurer, M.S.; Falk, R.H.; Merlini, G.; Damy, T.; Dispenzieri, A.; Wechalekar, A.D.; Berk, J.L.; Quarta, C.C.; Grogan, M.; et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation 2016, 133, 2404–2412. [Google Scholar] [CrossRef]
- Brito, D.; Albrecht, F.C.; De Arenaza, D.P.; Bart, N.; Better, N.; Carvajal-Juarez, I.; Conceição, I.; Damy, T.; Dorbala, S.; Fidalgo, J.C.; et al. World Heart Federation Consensus on Transthyretin Amyloidosis Cardiomyopathy (ATTR-CM). Glob. Heart 2023, 18, 59. [Google Scholar] [CrossRef]
- Hanna, M.; Ruberg, F.L.; Maurer, M.S.; Dispenzieri, A.; Dorbala, S.; Falk, R.H.; Hoffman, J.; Jaber, W.; Soman, P.; Witteles, R.M.; et al. Cardiac Scintigraphy with Technetium-99m-Labeled Bone-Seeking Tracers for Suspected Amyloidosis: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2020, 75, 2851–2862. [Google Scholar] [CrossRef]
- Porcari, A.; Hutt, D.F.; Grigore, S.F.; Quigley, A.M.; Rowczenio, D.; Gilbertson, J.; Patel, R.; Razvi, Y.; Ioannou, A.; Rauf, M.U.; et al. Comparison of Different Technetium-99m-Labelled Bone Tracers for Imaging Cardiac Amyloidosis. Eur. J. Prev. Cardiol. 2023, 30, E4–E6. [Google Scholar] [CrossRef]
- Hutt, D.F.; Quigley, A.M.; Page, J.; Hall, M.L.; Burniston, M.; Gopaul, D.; Lane, T.; Whelan, C.J.; Lachmann, H.J.; Gillmore, J.D.; et al. Utility and Limitations of 3,3-Diphosphono-1,2-Propanodicarboxylic Acid Scintigraphy in Systemic Amyloidosis. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 1289–1298. [Google Scholar] [CrossRef]
- Hage, F.G.; Bourque, J.M.; Pandey, S.; Shah, N.R.; Soman, P.; Abbott, B.G.; Abidov, A.; Aggarwal, N.R.; AlJaroudi, W.; Bhambhvani, P.G.; et al. American Society of Nuclear Cardiology Quality Metrics for Cardiac Amyloid Radionuclide Imaging. J. Nucl. Cardiol. 2024, 40, 102041. [Google Scholar] [CrossRef]
- Perugini, E.; Guidalotti, P.L.; Salvi, F.; Cooke, R.M.T.; Pettinato, C.; Riva, L.; Leone, O.; Farsad, M.; Ciliberti, P.; Bacchi-Reggiani, L.; et al. Noninvasive Etiologic Diagnosis of Cardiac Amyloidosis Using 99mTc-3,3-Diphosphono-1,2-Propanodicarboxylic Acid Scintigraphy. J. Am. Coll. Cardiol. 2005, 46, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Clerc, O.F.; Vijayakumar, S.; Dorbala, S. Radionuclide Imaging of Cardiac Amyloidosis: An Update and Future Aspects. Semin. Nucl. Med. 2024, 54, 717–732. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, Y.S.; Kim, S.J. Diagnostic Performance of PET for Detection of Cardiac Amyloidosis: A Systematic Review and Meta-Analysis. J. Cardiol. 2020, 76, 618–625. [Google Scholar] [CrossRef]
- Hutt, D.F.; Fontana, M.; Burniston, M.; Quigley, A.M.; Petrie, A.; Ross, J.C.; Page, J.; Martinez-Naharro, A.; Wechalekar, A.D.; Lachmann, H.J.; et al. Prognostic Utility of the Perugini Grading of 99mTc-DPD Scintigraphy in Transthyretin (ATTR) Amyloidosis and Its Relationship with Skeletal Muscle and Soft Tissue Amyloid. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1344–1350. [Google Scholar] [CrossRef] [PubMed]
- Castano, A.; Haq, M.; Narotsky, D.L.; Goldsmith, J.; Weinberg, R.L.; Morgenstern, R.; Pozniakoff, T.; Ruberg, F.L.; Miller, E.J.; Berk, J.L.; et al. Multicenter Study of Planar Technetium 99m Pyrophosphate Cardiac Imaging: Predicting Survival for Patients with ATTR Cardiac Amyloidosis. JAMA Cardiol. 2016, 1, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Rettl, R.; Duca, F.; Kronberger, C.; Binder, C.; Willixhofer, R.; Ermolaev, N.; Poledniczek, M.; Hofer, F.; Nitsche, C.; Hengstenberg, C.; et al. Prognostic Implication of DPD Quantification in Transthyretin Cardiac Amyloidosis. Eur. Heart J. Cardiovasc. Imaging 2025, 26, 251–260. [Google Scholar] [CrossRef]
- Castaño, A.; DeLuca, A.; Weinberg, R.; Pozniakoff, T.; Blaner, W.S.; Pirmohamed, A.; Bettencourt, B.; Gollob, J.; Karsten, V.; Vest, J.A.; et al. Serial Scanning with Technetium Pyrophosphate (99mTc-PYP) in Advanced ATTR Cardiac Amyloidosis. J. Nucl. Cardiol. 2016, 23, 1355–1363. [Google Scholar] [CrossRef]
- Papathanasiou, M.; Kessler, L.; Bengel, F.M.; Jakstaite, A.M.; Kersting, D.; Varasteh, Z.; Luedike, P.; Carpinteiro, A.; Herrmann, K.; Rassaf, T.; et al. Regression of Myocardial 99mTc-DPD Uptake After Tafamidis Treatment of Cardiac Transthyretin Amyloidosis. J. Nucl. Med. 2023, 64, 1083–1086. [Google Scholar] [CrossRef]
- Vijayakumar, S.; Pabon, A.R.; Clerc, O.F.; Cuddy, S.A.M.; Gu, Y.; Watts, C.; Sullivan, K.; Auer, B.; Kijewski, M.F.; DiCarli, M.F.; et al. Quantitative 99mTc-Pyrophosphate Myocardial Uptake: Changes on Transthyretin Stabilization Therapy. J. Nucl. Cardiol. 2024, 39, 102019. [Google Scholar] [CrossRef]
- Doumas, A.; Zegkos, T.; Parcharidou, D.; Gossios, T.; Ntelios, D.; Chatzileontiadou, S.; Papanastasiou, E.; Hatjiharissi, E.; Iakovou, I.; Efthimiadis, G.K. A Novel Quantitative Method for Assessing the Therapeutic Response to Tafamidis Therapy in Patients with Cardiac TTR Amyloidosis. A Preliminary Report. Hell. J. Nucl. Med. 2022, 25, 216–219. [Google Scholar]
- Zhao, M.; Calabretta, R.; Yu, J.; Binder, P.; Hu, S.; Hacker, M.; Li, X. Nuclear Molecular Imaging of Disease Burden and Response to Treatment for Cardiac Amyloidosis. Biology 2022, 11, 1395. [Google Scholar] [CrossRef] [PubMed]
- Bellevre, D.; Bailliez, A.; Maréchaux, S.; Manrique, A.; Mouquet, F. First Follow-Up of Cardiac Amyloidosis Treated by Tafamidis, Evaluated by Absolute Quantification in Bone Scintigraphy. JACC Case Rep. 2021, 3, 133–135. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ECG | Echocardiography | CMR |
|---|---|---|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tziomalos, G.; Zegkos, T.; Baltagianni, E.; Bazmpani, M.-A.; Exadaktylou, P.; Parcharidou, D.; Gossios, T.; Doumas, A.; Karamitsos, T.; Vassilikos, V.; et al. Transthyretin Amyloid Cardiomyopathy: Current Diagnostic Approach and Risk Stratification with Multimodality Imaging. J. Clin. Med. 2025, 14, 2014. https://doi.org/10.3390/jcm14062014
Tziomalos G, Zegkos T, Baltagianni E, Bazmpani M-A, Exadaktylou P, Parcharidou D, Gossios T, Doumas A, Karamitsos T, Vassilikos V, et al. Transthyretin Amyloid Cardiomyopathy: Current Diagnostic Approach and Risk Stratification with Multimodality Imaging. Journal of Clinical Medicine. 2025; 14(6):2014. https://doi.org/10.3390/jcm14062014
Chicago/Turabian StyleTziomalos, Georgios, Thomas Zegkos, Eleftheria Baltagianni, Maria-Anna Bazmpani, Paraskevi Exadaktylou, Despoina Parcharidou, Thomas Gossios, Argyrios Doumas, Theodoros Karamitsos, Vassilios Vassilikos, and et al. 2025. "Transthyretin Amyloid Cardiomyopathy: Current Diagnostic Approach and Risk Stratification with Multimodality Imaging" Journal of Clinical Medicine 14, no. 6: 2014. https://doi.org/10.3390/jcm14062014
APA StyleTziomalos, G., Zegkos, T., Baltagianni, E., Bazmpani, M.-A., Exadaktylou, P., Parcharidou, D., Gossios, T., Doumas, A., Karamitsos, T., Vassilikos, V., Efthimiadis, G., Ziakas, A., & Kamperidis, V. (2025). Transthyretin Amyloid Cardiomyopathy: Current Diagnostic Approach and Risk Stratification with Multimodality Imaging. Journal of Clinical Medicine, 14(6), 2014. https://doi.org/10.3390/jcm14062014