

Deterioration of Myocardial Global Longitudinal Strain and Its Relationship with Arterial Stiffness in Patients with Cardiac Amyloidosis: A Six-Month Follow-Up

 , ,
, ,  , , ,
, , ,  , , , , add
Show full author list
, , , , add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Echocardiographic Study
2.3. Measurement of PWV
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| LV | left ventricle |
| c-f PWV | carotid–femoral pulse wave velocity |
| c-r PWV | carotid–radial pulse wave velocity |
| GLS | global longitudinal strain |
References
- Merlini, G.; Bellotti, V. Molecular mechanisms of amyloidosis. N. Engl. J. Med. 2003, 349, 583–596. [Google Scholar] [CrossRef] [PubMed]
- Pinney, J.H.; Hawkins, P.N. Amyloidosis. Ann. Clin. Biochem. 2012, 49, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Yokochi, T. Transthyretin cardiac amyloidosis: An update on diagnosis and treatment. ESC Heart Fail. 2019, 6, 1128–1139. [Google Scholar] [CrossRef]
- Wechalekar, A.D.; Gillmore, J.D.; Hawkins, P.N. Systemic amyloidosis. Lancet 2016, 387, 2641–2654. [Google Scholar] [CrossRef]
- Falk, R.H. Diagnosis and management of the cardiac amyloidoses. Circulation 2005, 112, 2047–2060. [Google Scholar] [CrossRef]
- Martinez-Naharro, A.; Hawkins, P.N.; Fontana, M. Cardiac amyloidosis. Clin. Med. 2018, 18, s30–s35. [Google Scholar] [CrossRef]
- Smith, R.R.; Hutchins, G.M. Ischemic heart disease secondary to amyloidosis of intramyocardial arteries. Am. J. Cardiol. 1979, 44, 413–417. [Google Scholar] [CrossRef]
- Gasparović, H.; Petričević, M.; Durić, E.; Brida, V.; Jelasić, D.; Biočina, B. Amyloidosis of the aortic root in a patient with polyarteritis nodosa. Coll. Antropol. 2014, 38, 1051–1053. [Google Scholar]
- Bruno, G.; Bringhen, S.; Maffei, I.; Iannaccone, A.; Crea, T.; Ravera, A.; Astarita, A.; Vallelonga, F.; Salvini, M.; Gay, F.; et al. Cardiovascular organ damage and blood pressure levels predict adverse events in multiple myeloma patients undergoing carfilzomib therapy. Cancers 2019, 11, 622. [Google Scholar] [CrossRef]
- Belz, G.G. Elastic properties and Windkessel function of the human aorta. Cardiovasc. Drugs Ther. 1995, 9, 73–83. [Google Scholar] [CrossRef]
- Trimarchi, G.; Carerj, S.; Di Bella, G.; Manganaro, R.; Pizzino, F.; Restelli, D.; Pelaggi, G.; Lofrumento, F.; Licordari, R.; Taverna, G.; et al. Clinical applications of myocardial work in echocardiography: A comprehensive review. J. Cardiovasc. Echogr. 2024, 34, 99–113. [Google Scholar] [CrossRef] [PubMed]
- de Gregorio, C.; Trimarchi, G.; Faro, D.C.; De Gaetano, F.; Campisi, M.; Losi, V.; Zito, C.; Tamburino, C.; Di Bella, G.; Monte, I.P. Myocardial work appraisal in transthyretin cardiac amyloidosis and nonobstructive hypertrophic cardiomyopathy. Am. J. Cardiol. 2023, 208, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Georgiopoulos, G.; Makris, N.; Laina, A.; Theodorakakou, F.; Briasoulis, A.; Trougakos, I.P.; Dimopoulos, M.; Kastritis, E.; Stamatelopoulos, K. Cardiovascular toxicity of proteasome inhibitors: Underlying mechanisms and management strategies. J. Am. Coll. Cardiol. CardioOnc 2023, 5, 1–21. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart. J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- Galderisi, M.; Cosyns, B.; Edvardsen, T.; Cardim, M.; Delgado, V.; Di Salvo, G.; Donal, E.; Sade, L.E.; Ernande, L.; Garbi, M.; et al. 2016–2018 EACVI Scientific Documents Committee; 2016–2018 EACVI Scientific Documents Committee Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: An expert consensus document of the European Association of Cardiovascular Imaging. Eur. Heart. J. Cardiovasc. Imaging 2017, 18, 1301–1310. [Google Scholar]
- Adams, D.; Kolke, H.; Slama, M.; Coelho, T. Hereditary transthyretin amyloidosis: A model of medical progress for a fatal disease. Nat. Rev. Neurol. 2019, 15, 387–404. [Google Scholar] [CrossRef]
- Mohty, D.; Pibarot, P.; Damy, T. Aortic stenosis and amyloid heart disease: ‘The 2A dangerous liaisons’. Eur. Heart J. 2020, 41, 2815. [Google Scholar] [CrossRef]
- Cuddy, S.R.; Jacob, S. Cardiovascular Implications of Amyloidosis. J. Am. Coll. Cardiol. 2021, 77, 2067–2077. [Google Scholar]
- Hoteit, A.; Casimero, F.V.C.; Stone, J.R.; Cameron, D.; Isselbacher, E.M.; Seyedsadjadi, R.; Gaggin, H.K. Wild-type Transthyretin Amyloid deposition in an ascending aortic aneurysm. JACC Case Rep. 2024, 29, 102311. [Google Scholar] [CrossRef]
- Huntjens, P.R.; Zhang, K.W.; Soyama, Y.; Karmpalioti, M.; Gorcsan, J., 3rd. Prognostic Utility of Echocardiographic Atrial and Ventricular Strain Imaging in Patients With Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2021, 14, 1508–1519. [Google Scholar] [CrossRef]
- Griffin, J.M.; Rosenblum, H.; Mauer, M.S. Pathophysiology and therapeutic approaches to cardiac amyloidosis. Circ. Res. 2021, 128, 1554–1575. [Google Scholar] [CrossRef] [PubMed]
- Hou, W.; Wang, Z.; Huang, J.; Fan, F.; Yang, F.; Qiu, L.; Zhao, K.; Qiu, J.; Yang, Y.; Ma, W.; et al. Early diagnostic and prognostic value of myocardial strain derived from cardiovascular magnetic resonance in patients with cardiac amyloidosis. Cardiovasc. Diagn. Ther. 2023, 13, 979–983. [Google Scholar] [CrossRef] [PubMed]
- de Gregorio, C.; Trimarchi, G.; Faro, D.C.; Poleggi, C.; Teresi, L.; De Gaetano, F.; Zito, C.; Lofrumento, F.; Koniari, I.; Licordari, R.; et al. Systemic vascular resistance and myocardial work analysis in hypertrophic cardiomyopathy and transthyretin cardiac amyloidosis with preserved left ventricular ejection fraction. J. Clin. Med. 2024, 13, 1671. [Google Scholar] [CrossRef]
- Petrescu, A.; Santos, P.; Orlowska, M.; Pedrosa, J.; Bézy, S.; Chakraborty, B.; Cvijic, M.; Dobrovie, M.; Delforge, M.; D’hooge, J.; et al. Velocities of naturally occurring myocardial shear waves increase with age and in cardiac amyloidosis. J. Am. Coll. Cardiol. Imaging 2019, 12, 2389–2398. [Google Scholar] [CrossRef]
- Yoshida, Y.; Nakanishi, K.; Jin, Z.; Daimon, M.; Ishiwata, J.; Sawada, N.; Hirokawa, M.; Kaneko, H.; Nakao, T.; Mizuno, Y.; et al. Association between progression of arterial stiffness and left ventricular remodeling in a community-based cohort. JACC Adv. 2023, 2, 100409. [Google Scholar] [CrossRef]
- Monte, I.P.; Faro, D.C.; Trimarchi, G.; de Gaetano, F.; Campisi, M.; Losi, V.; Teresi, L.; Di Bella, G.; Tamburino, C.; de Gregorio, C. Left atrial strain imaging by speckle tracking echocardiography: The supportive diagnostic value in cardiac amyloidosis and hypertrophic cardiomyopathy. J. Cardiovasc. Dev. Dis. 2023, 10, 261. [Google Scholar] [CrossRef]
- Nemes, A.; Földeák, D.; Domsik, P.; Kalapos, A.; Kormányos, Á.; Borbényi, Z.; Forster, T. Cardiac amyloidosis is associated with increased aortic stiffness. J. Clin. Ultrasound 2018, 46, 183–187. [Google Scholar] [CrossRef]
- Wang, Y.; Feng, X.; Shen, B.; Ma, J.; Zhao, W. Is vascular amyloidosis intertwined with arterial aging, hypertension and atherosclerosis? Front. Genet. 2017, 8, 126. [Google Scholar] [CrossRef]
- Cooper, L.L.; O’Donnell, A.; Beiser, A.S.; Thibault, E.G.; Sanchez, J.S.; Benjamin, E.J.; Hamburg, N.M.; Vasan, R.S.; Larson, M.G.; Johnsosn, K.A.; et al. Association of aortic stiffness and pressure pulsatility with global amyloid-β and regional Tau burden among Framingham Heart Study participants without dementia. JAMA Neurol. 2022, 79, 710–719. [Google Scholar] [CrossRef]
- Trimarchi, G.; Pizzino, F.; Paradossi, U.; Gueli, I.A.; Palazzini, M.; Gentile, P.; Di Spigno, F.; Ammirati, E.; Garascia, A.; Tedeschi, A.; et al. Charting the Unseen: How non-invasive imaging could redefine cardiovascular prevention. J. Cardiovasc. Dev. Dis. 2024, 9, 245. [Google Scholar] [CrossRef]
- Byer, S.H.; Sivamurugan, A.; Grewal, U.S.; Fradley, M.G.; Dominic, P. Impact of sodium-glucose cotransporter-2 inhibitors on cardiovascular outcomes in transthyretin amyloid cardiomyopathy. Am. J. Cardiol. 2025, 243, 15–18. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Patients with CA n = 31 | Control Group n = 31 | p | |
|---|---|---|---|
| BMI (kg/m2) | 25.9 ± 4.3 | 27.4 ± 2.8 | 0.24 |
| HR (bpm) | 72 ± 7 | 69 ± 12 | 0.43 |
| SBP (mmHg) | 116 ± 18 | 130 ± 6 | 0.001 |
| DBP (mmHg) | 73 ± 12 | 74± 8 | 0.64 |
| LVEF (%) | 50 ± 12 | 61 ± 6 | <0.001 |
| LVMI (g/m2) | 119.4 ± 52.1 | 90.4 ± 19.8 | 0.04 |
| GLS (%) | −14.02 ± 4.4 | −17.3 ± 2.4 | 0.005 |
| c-f PWV (m/s) | 11.8 ± 2.7 | 10.2 ± 2.6 | 0.007 |
| c-r PWV (m/s) | 10.3 ± 2.3 | 9.3 ± 1.3 | 0.01 |
| Hemoglobin (g/dL) | 13.2 ± 1.9 | 13.3 ± 1.2 | 0.12 |
| Glucose (mg/dL) | 106 ± 24 | 100 ± 24 | 0.1 |
| Creatinine (mg/dL) | 1.1 ± 0.5 | 1 ± 0.4 | 0.8 |
| Cholesterol (mg/dL) | 176 ± 51 | 172 ± 37 | 0.8 |
| nt-proBNP (pg/mL) | 2244 ± 2852 | 49 ± 28.2 | <0.001 |
| Patients with CA n = 31 | Control Group n = 31 | |||||
|---|---|---|---|---|---|---|
| Baseline | 6 Months | p | Baseline | 6 Months | p | |
| BMI (kg/m2) | 27.4 ± 2.8 | 27 ± 5.1 | 0.5 | 25.9 ± 4.3 | 25.6 ± 4.3 | 0.6 |
| Troponine I (ng/mL) | 268 ± 435 | 324 ± 488 | 0.7 | 4.5 ± 6.5 | 5.1 ± 6.8 | 0.8 |
| LVEF (%) | 61 ± 6 | 61.6 ± 5.3 | 0.9 | 50 ± 12 | 48.8 ± 4.7 | 0.057 |
| LVMI (g/m2) | 90.4 ± 19.8 | 90.5 ± 19.9 | 0.9 | 119.4 ± 52.1 | 124 ± 53.2 | 0.02 |
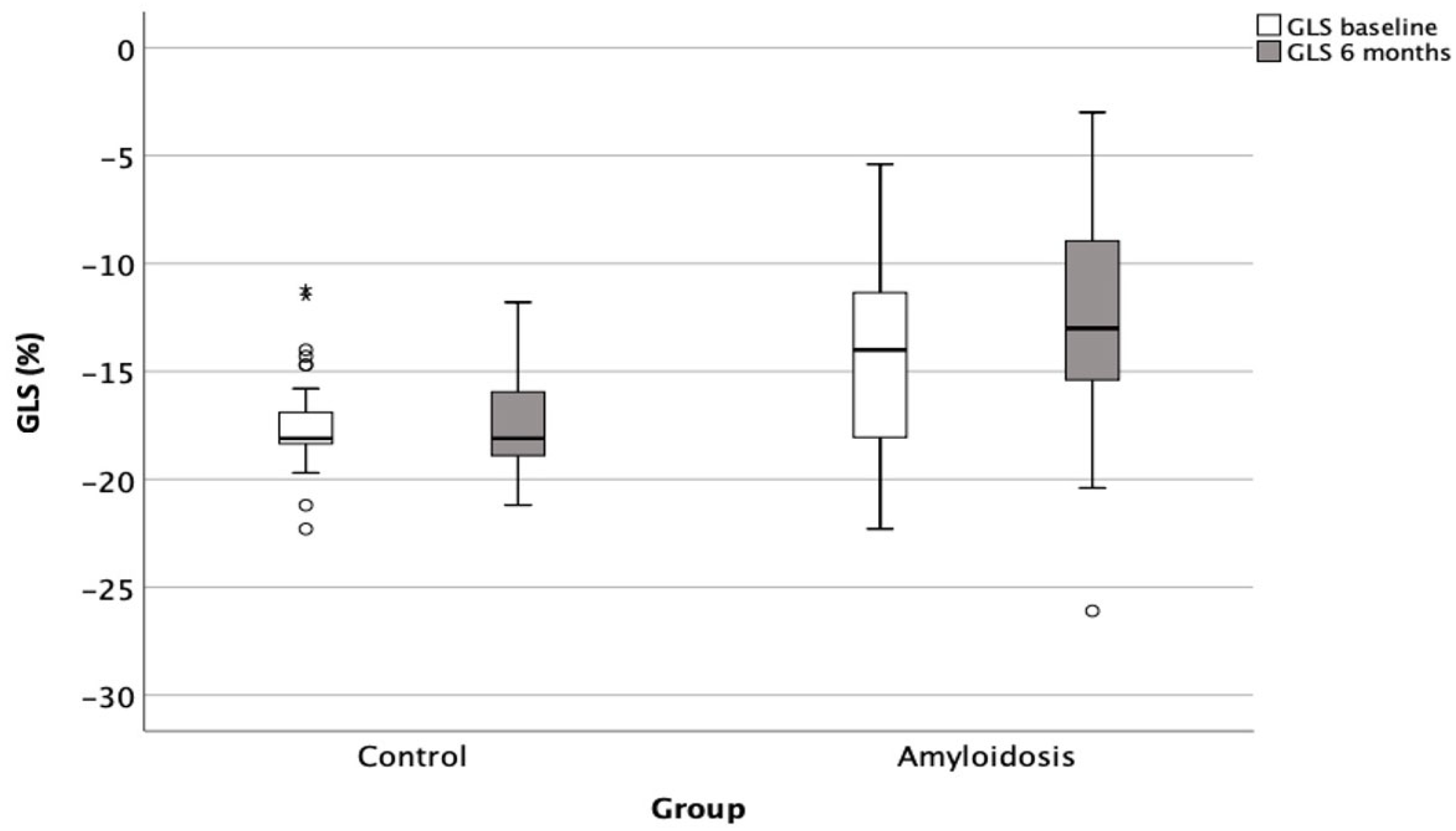
| GLS (%) | −17.3 ± 2.4 | −17.2 ± 2.2 | 0.9 | −14.02 ± 4.4 | −12.8 ± 4.9 | 0.018 |
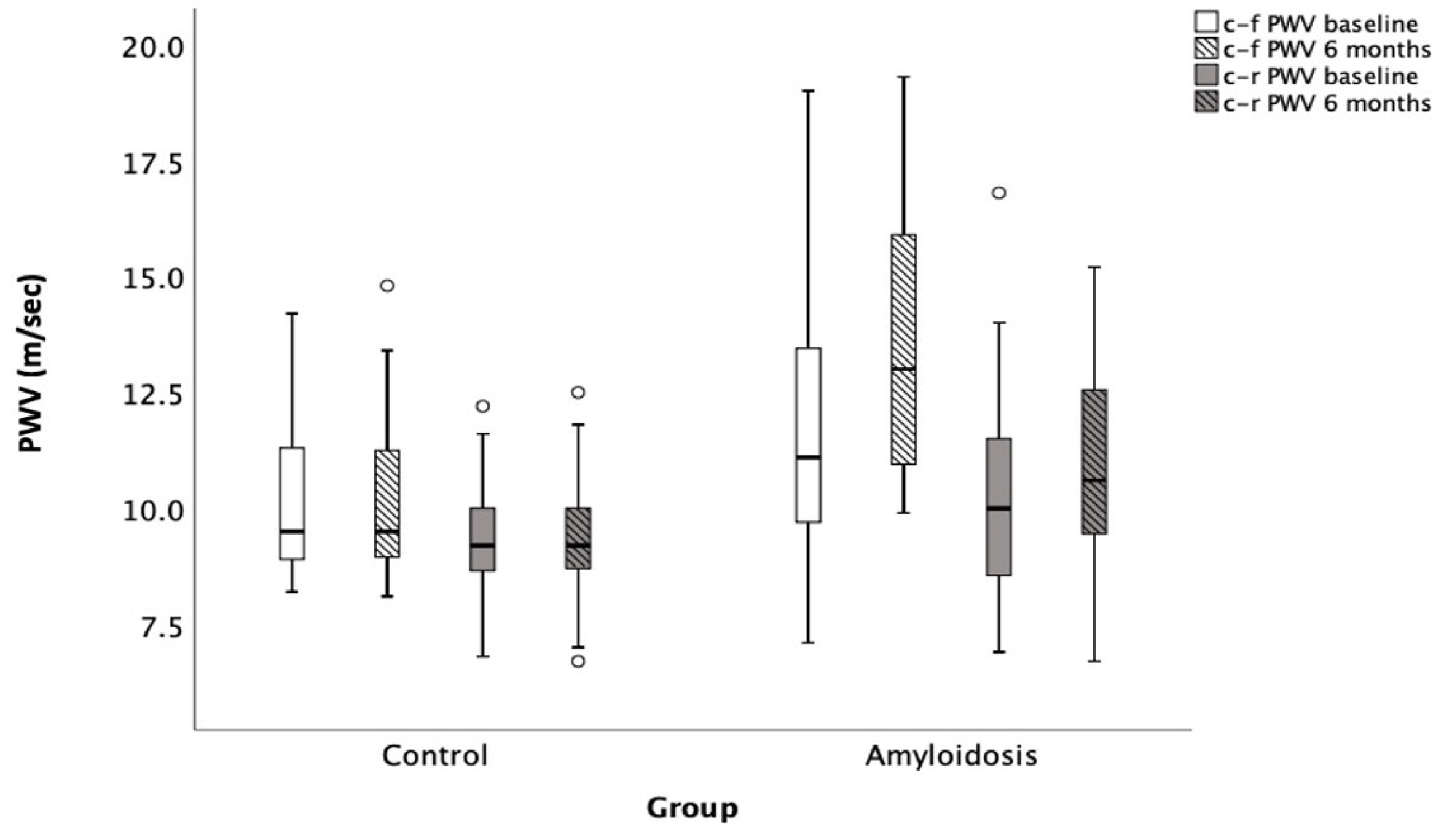
| c-f PWV (m/s) | 10.2 ± 2.6 | 10.1 ± 2.4 | 0.8 | 11.8 ± 2.7 | 13.4 ± 2.9 | 0.03 |
| c-r PWV (m/s) | 9.3 ± 1.3 | 9.4 ± 1.2 | 0.8 | 10.3 ± 2.3 | 10.8 ± 2.5 | 0.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korela, D.; Foukarakis, E.; Plevritaki, A.; Maragkoudakis, S.; Anastasiou, I.; Patrianakos, A.; Kapsoritakis, N.; Koukouraki, S.; Bourogianni, O.; Pontikoglou, C.; et al. Deterioration of Myocardial Global Longitudinal Strain and Its Relationship with Arterial Stiffness in Patients with Cardiac Amyloidosis: A Six-Month Follow-Up. J. Clin. Med. 2025, 14, 2078. https://doi.org/10.3390/jcm14062078
Korela D, Foukarakis E, Plevritaki A, Maragkoudakis S, Anastasiou I, Patrianakos A, Kapsoritakis N, Koukouraki S, Bourogianni O, Pontikoglou C, et al. Deterioration of Myocardial Global Longitudinal Strain and Its Relationship with Arterial Stiffness in Patients with Cardiac Amyloidosis: A Six-Month Follow-Up. Journal of Clinical Medicine. 2025; 14(6):2078. https://doi.org/10.3390/jcm14062078
Chicago/Turabian StyleKorela, Dafni, Emmanouil Foukarakis, Anthοula Plevritaki, Spyros Maragkoudakis, Ioannis Anastasiou, Alexandros Patrianakos, Nikolaos Kapsoritakis, Sophia Koukouraki, Olga Bourogianni, Charalampos Pontikoglou, and et al. 2025. "Deterioration of Myocardial Global Longitudinal Strain and Its Relationship with Arterial Stiffness in Patients with Cardiac Amyloidosis: A Six-Month Follow-Up" Journal of Clinical Medicine 14, no. 6: 2078. https://doi.org/10.3390/jcm14062078
APA StyleKorela, D., Foukarakis, E., Plevritaki, A., Maragkoudakis, S., Anastasiou, I., Patrianakos, A., Kapsoritakis, N., Koukouraki, S., Bourogianni, O., Pontikoglou, C., Psillaki, M., Padadaki, H. A., Zaganas, I., Samonakis, D., Detorakis, E., Petrakis, I., Stylianou, K., Chlouverakis, G., Giannakoudakis, E., ... Marketou, M. (2025). Deterioration of Myocardial Global Longitudinal Strain and Its Relationship with Arterial Stiffness in Patients with Cardiac Amyloidosis: A Six-Month Follow-Up. Journal of Clinical Medicine, 14(6), 2078. https://doi.org/10.3390/jcm14062078